
Guideline Women and Babies: Management of Pneumothorax in ...
16
Compliance with this Guideline is recommended Page 1 of 16 Guideline Women and Babies: Management of Pneumothorax in Newborn Infants Document No: RPAH_GL2017_ Number (sequential akin to DOH) Functional Sub-Group: Clinical Governance Summary: Describes the management of pneumothorax in newborn infants including the procedure of intercostal catheter insertion National Standard: Standard 1: Governance for safety and quality in Health service organisations Standard 9: Recognising and responding to clinical deterioration in acute health care Policy Author: Rowena McMullan, Neonatal Staff Specialist Approved by: RPA Newborn Care Guideline Development Committee Publication (Issue) Date: June 2017 Next Review Date: June 2020 Replaces Existing Policy: Management of Pneumothorax Previous Review Dates: Note: Sydney Local Health District (LHD) and South Western Sydney LHD were established on 1 July 2011, with the dissolution of the former Sydney South West Area Health Service (SSWAHS) in January 2011. The former SSWAHS was established on 1 January 2005 with the amalgamation of the former Central Sydney Area Health Service (CSAHS) and the former South Western Sydney Area Health Service (SWSAHS). In the interim period between 1 January 2011 and the release of specific LHN policies (dated after 1 January 2011) and SLHD (dated after July 2011), the former SSWAHS, CSAHS and SWSAHS policies are applicable to the LHDs as follows: Where there is a relevant SSWAHS policy, that policy will apply Where there is no relevant SSWAHS policy, relevant CSAHS policies will apply to Sydney LHD; and relevant SWSAHS policies will apply to South Western Sydney LHD.
Transcript of Guideline Women and Babies: Management of Pneumothorax in ...

Compliance with this Guideline is recommended Page 1 of 16
Guideline
Women and Babies: Management of Pneumothorax in Newborn Infants
Document No: RPAH_GL2017_ Number (sequential akin to DOH) Functional Sub-Group: Clinical Governance
Summary: Describes the management of pneumothorax in newborn
infants including the procedure of intercostal catheter insertion
National Standard: Standard 1: Governance for safety and quality in Health service organisations Standard 9: Recognising and responding to clinical deterioration in acute health care Policy Author: Rowena McMullan, Neonatal Staff Specialist Approved by: RPA Newborn Care Guideline Development Committee Publication (Issue) Date: June 2017 Next Review Date: June 2020 Replaces Existing Policy: Management of Pneumothorax Previous Review Dates:
Note: Sydney Local Health District (LHD) and South Western Sydney LHD were established on 1 July 2011, with the dissolution of the former Sydney South West Area Health Service (SSWAHS) in January 2011. The former SSWAHS was established on 1 January 2005 with the amalgamation of the former Central Sydney Area Health Service (CSAHS) and the former South Western Sydney Area Health Service (SWSAHS).
In the interim period between 1 January 2011 and the release of specific LHN policies (dated after 1 January 2011) and SLHD (dated after July 2011), the former SSWAHS, CSAHS and SWSAHS policies are applicable to the LHDs as follows:
Where there is a relevant SSWAHS policy, that policy will apply
Where there is no relevant SSWAHS policy, relevant CSAHS policies will apply to Sydney LHD; and relevant SWSAHS policies will apply to South Western Sydney LHD.

Compliance with this Guideline is recommended Page 2 of 16
Women and Babies: Management of Pneumothorax in Newborn
Infants
Procedural Guidelines
1. Introduction 2. Policy Statement 3. Principles/Guidelines
3.1 Background 3.2 Diagnosis
3.2.1 Transillumination 3.2.2 Chest X-ray 3.2.3 Ultrasound
3.3 Management of pneumothorax 3.3.1 Choice of catheter 3.3.2 Procedure to perform thoracocentesis 3.3.3 Procedure to insert intercostal catheter 3.3.4 Procedure to set up the Atrium Oasis Dry Suction Water Seal System
3.4 Risks and complications 4. Key points 5. References
Note:
• This is an evidence based guideline. The aim is to ensure best and consistent practice within RPA Newborn Care
• A further and secondary aim is to provide brief background information on common neonatal problems to trainees who may have limited prior content knowledge.
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 3 of 16
Women and Babies: Management of Pneumothorax in Newborn Infants
1. Introduction
The risks addressed by this policy:
Clinical risk of pneumothorax Clinical risk of intercostal catheter placement
The aims / expected outcome of this policy
To assist staff to recognise and appropriately manage pneumothorax in newborn infants To facilitate the appropriate and safe insertion and maintenance of intercostal catheters
2. Policy Statement
The goal of this guideline is to recognise and manage pneumothorax in newborn infants, and facilitate the safe and appropriate insertion of intercostal catheters.
3.1 Background Pneumothorax is defined as air in the pleural space, and is relatively common in newborn care. Pneumothoraces are seen in 1-2% of normal term babies,1 and the majority of these are asymptomatic. However, pneumothoraces are more likely to occur in those with underlying lung disease, and may be life-threatening. Air enters the pleural space after rupture of overdistended alveoli, air then tracking along the perihilar connective tissue. If air continues to accumulate, intrathoracic pressure increases, venous return to the heart is reduced, and cardiac output becomes compromised. This is a tension pneumothorax, results in a hypoxic and shocked infant, and is a neonatal emergency. Pneumothoraces occur in up to 10%2 of preterm infants; local data shows a rate of 4.9% of infants less than 30 weeks in Australia and New Zealand had a pneumothorax requiring drainage.3 Pneumothorax is associated with increased intraventricular haemorrhage4 and increased mortality in preterm infants.5 Risk factors for pneumothorax include:
• mechanical ventilation, • respiratory distress syndrome, • meconium aspiration syndrome, • pulmonary hypoplasia.6-8
Strategies proven in meta-analysis to affect incidence of pneumothorax are summarised in Table 1.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 4 of 16
Strategies that REDUCE risk of air leak: Typical risk ratio ( 95% confidence intervals)
Surfactant in neonatal respiratory distress syndrome: Early surfactant vs delayed surfactant 0.69 (0.59 to 0.82)9 Multiple doses vs single doses 0.51 (0.30 to 0.88)10 Animal derived surfactant vs protein-free synthetic surfactant 0.65 (0.55 to 0.77)11 Prophylactic surfactant 0.67 (0.5 to 0.9)12 Early surfactant with brief ventilation vs. selective surfactant and continued mechanical ventilation
0.52 (0.28 to 0.96)13
Ventilation strategies: Synchronised vs non-synchronised ventilation for respiratory support 0.69 (0.51 to 0.93)14 Volume-targeted vs pressure-limited ventilation 0.46 (0.25 to 0.84)15 Strategies that INCREASE risk of air leak: Typical risk ratio ( 95%
confidence intervals) CPAP vs no respiratory support in preterm infants with respiratory distress syndrome
2.64 (1.39 to 5.04)16
Long vs short inspiratory times if ventilated 1.56 (1.25 to 1.94)17 Elective high frequency oscillatory ventilation vs conventional ventilation 1.19 (1.05 to 1.34)18
Table 1. Strategies affecting incidence of pneumothorax
3.2 Diagnosis Symptomatic infants present with increased work of breathing. Examination findings may include chest asymmetry, decreased air entry on the affected sign, and shift in the position of the apex. Hypoxia is a late sign. There should be a high index of suspicion of pneumothorax if a ventilated newborn has a sudden increase in oxygen or ventilatory requirements, or has cardiovascular compromise. Pneumothorax may be detected with transillumination, chest xray or ultrasound. If there is time to delay, a chest X-ray usually confirms diagnosis, and is the investigation of choice at present. 3.2.1 Transillumination Placement of a cold fibreoptic light source next to the infant’s skin should transilluminate the whole hemithorax in the presence of a large pneumothorax. It should be compared to the other side of the chest for reference. In a negative result a halo of light appears around the light source only. Transillumination is most useful in small babies. Large infants require a bright source and a very dark room for transillumination to be visible, therefore is only useful is positive. False positive results may occur with other air accumulations such as pulmonary interstitial emphysema or pneumomediastinum. False negatives may be seen with a large or oedematous infant, small air leaks, a weak light source or a bright room. Reported sensitivity is 87-100% and specificity 95-100%.19-21

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 5 of 16
3.2.2 X-ray
A chest X-ray usually provides definitive diagnosis if there is time to obtain one. In a large pneumothorax under tension, air may be seen in the pleural space, with flattening of the diaphragm and displacement of the mediastinum. The lung edge is clearly visible.
Smaller pneumothoraces may be more difficult to appreciate. A generalised increase in lucency may be noted on the affected side (on the right on the film opposite). If there is uncertainty, a lateral decubitus film with the affected side up should aid diagnosis. Be aware of false positives – shadows of skin folds, bed sheets, and the latissimus dorsi mimicking a lung edge have all caused diagnostic dilemmas. Follow the shadows along and look for lung markings.
Also note the Mach sign - it is an optical illusion which exaggerates the contrast along differing shades of grey where they come into contact with each other, and may mimic pneumothorax on X-ray. Diagnostic accuracy for chest xray is reported as sensitivity 40-87% and specificity 96-99%.19,22

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 6 of 16
3.2.3 Ultrasound For those with skill in the use of ultrasound, this technique may be a useful bedside adjunct for diagnosis. Sensitivity is reported as 79-100% and specificity 98-100%.19,22-24 Use the linear L18-5 transducer and set to the preset ‘Neonatal Lung’. Place the transducer anteriorly (mid-clavicular line, 5-8th intercostal space). Using B-mode, in a normal lung you should be able to see the pleura, visible as a hyperechoic line beneath subcutaneous tissue, sliding up and down. This will be absent in pneumothorax as air separates the pleura. It is possible to identify the edge of the collection of air with ultrasound (the lung point) where the pleura stop sliding. Using M-mode, the normal lung is seen beneath pleura (the waves) as a granular pattern (the gravelly beach) as a ‘seashore’. In pneumothorax, this pattern is replaced by the ‘stratosphere’ or ‘barcode’ sign, where lung sliding is abolished, and the lung is no longer visible and instead reverberation artefact (A-lines) is seen.
Ultrasound lung scan in B mode. The left side of the image shows the granular pattern of the normal lung. The downward pointing vertical arrow is the lung point – the point denoting the edge of the pneumothorax. It shows the the transition from the granular appearing normal lung to a hypoechoic area with horizontal reverberation artefact of the pleura in the lung fields on the right side. From Raimondi et al24.
‘Seashore’ sign of a normal lung on M-mode (left) and 2D (right). Taken from Blank et al.23
‘Stratosphere’ or ‘barcode’ sign of a pneumothorax on M-mode (left) and 2D (right).

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 7 of 16
3.3 Management of pneumothorax
There is a paucity of high quality evidence for management of pneumothorax in newborns. There are a number of strategies available:
1. Careful observation only. In a retrospective cohort study of 136 ventilated infants with pneumothorax, 35 (26%) were managed without need for an intercostal catheter. 14 of the 35 infants had needle thoracocentesis and 21 of 35 had careful observation only. 57% of those managed with needle aspiration and 90% of those managed expectantly resolved without any subsequent need for intervention.25
2. Needle thoracocentesis (simple aspiration of air) may be performed to rapidly stabilise a compromised infant, or may be the only measure required in an otherwise stable patient.25
3. Intercostal catheter insertion.
There is currently insufficient evidence to recommend an initial strategy.26 At RPA Newborn Care our preference is:
• An asymptomatic or stable infant on minimal respiratory support may be managed conservatively with careful observation • An infant with a large symptomatic pneumothorax or a tension pneumothorax should have an intercostal catheter placed • If there is insufficient time to place an intercostal catheter in an acutely compromised infant, needle thoracocentesis should be performed, followed by consideration of placement of an intercostal catheter.
3.3.1 Choice of catheter
Rigid large-bore chest drains have been used traditionally, which require blunt dissection of the chest wall. Small-bore, flexible pigtail catheters inserted via the Seldinger technique or directly over an introducer are now recommended as primary choice of intercostal catheter in adults due to ease and speed of insertion, reduced pain both during insertion and while in situ, lower complication rates and equal success rates for most pleural pathologies.27
In newborn patients, small-bore flexible catheters have been shown to be equally safe and effective in draining air compared to large-bore catheters,28-31 and associated with a shorter time to insertion, by a mean of 10 minutes.29,30
Published complication rates of small-bore flexible catheters in comparison to large-bore rigid tubes in infants are summarised below, although noting the level of evidence is III to IV. Risks and complications of intercostal catheters are detailed in 3.4.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 8 of 16
Small-bore flexible tubes (%) Large-bore rigid tubes (%) Major: Perforation of a viscus 0-128-30,32 0-329,30,33 Minor: Bleeding at site 0-329,30,32 0-329,30 Accidental dislodgement 4-2528,30,32 1530 Failure to drain/blockage/kinking 2-1528-30 629 Breakage 629 029 Pain 029 1129
First choice of catheter in our nursery for drainage of pneumothorax is a 6Fr or 8Fr flexible pigtail catheter. Placement of a rigid large-bore tube should be considered if drainage of a complicated effusion is expected or if flexible pigtail catheter is unsuccessful.
3.3.2 Procedure to perform thoracocentesis
Clean equipment Sterile equipment 0.015% chlorhexidine solution Dressing pack Gloves Three-way tap 20-22G cannula or 21-23G butterfly
needle 10ml syringe
• Collect equipment as detailed above. • This is usually an emergency procedure in a compromised infant. However, if time available
consider the use of appropriate analgesia, such as sucrose. • Prepare the insertion site using appropriate antiseptic solution. Insertion site should be the 2nd-3rd
intercostal space in the mid-clavicular line. Infants should be supine. • Attach the butterfly or cannula to a 3-way tap and a 10ml syringe. • Insert the butterfly or cannula at the chosen site, just above the rib below, aspirating as you go. You
may feel a pop as you enter the pleural space. The needle should be inserted until air is easily aspirated into the syringe.
• If using a cannula, withdraw the needle while gently advancing the cannula into position.
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 9 of 16
• The pneumothorax is removed by pulling back on the syringe, and then turning the three way tap off to the baby and expelling the syringe to the air. This should be done until air can no longer be aspirated. The three-way tap is maintained closed to ensure further air is not introduced into the pleural space, and preparation for insertion of an intercostal catheter should be commenced.
• If using a cannula, it may be left in situ for a short time. If using a butterfly, it must be removed. Secure the cannula with tape and tegaderm.
• An alternative method of performing emergency thoracocentesis is to follow the above procedure, but instead of a syringe and 3-way tap, you may use a butterfly with the other end of the tubing placed underwater in a Gallipot of sterile water. This may facilitate insertion as you get immeadiate feedback (bubbles in the water) when the pneumothorax has been entered.
• Please note that needle thoracocentesis is often temporary, and placement of an intercostal catheter should be considered.
3.3.3 Procedure to insert intercostal catheter
Preparation
Clean equipment Sterile equipment Clean dressing trolley and allow to dry Sterile drapes 0.015% chlorhexidine solution unopened Dressing pack Leukoplast Intercostal catheter – 6Fr or 8Fr 1% lignocaine unopened Surgical instruments Atrium underwater drain 1ml syringe and orange needle Drawing up needle Cook® Plastic multipurpose tubing
adapter Steristrips, Tegaderm (2 frame style and
multiple IV style (‘teddy bears’), Comfeel
Collect the required equipment as above.
Analgesia should be provided. Consider:
• Oral sucrose 24% • Subcutaneous 1% lignocaine. Maximum dose is 3mg/kg, or 0.3ml/kg of 1% lignocaine. The
maximum volume should be less than 1ml. • Morphine or fentanyl. Dose should be individualised to the patient, but consider 50-100
micrograms/kg morphine IV.
The area for insertion should be identified, and the infant placed supine, or rolled slightly with the affected side up to facilitate insertion. The area for insertion is in the 4th or 5th intercostal space, between the mid and anterior axillary line. This usually corresponds to a point 1-2cm lateral to and 0.5-1cm below the nipple in newborn infants.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 10 of 16
Figure 1. The safe triangle for insertion of intercostal catheters. From Strutt et al.34
Maximal sterile precautions should be taken. The bedspace should be isolated with screens. The proceduralist should wear mask and hat, gown and double gloves after the WHO surgical hand scrub.
Preparation of the catheter
• Set up the trolley. • Draw up the required lignocaine dose. • Remove the plastic sleeve from the introducer. • Insert the introducer into the catheter via the white self-sealing valve.
• Place a bung onto the 3-way tap, and close the tap to the catheter. • Clean the area with 0.015% chlorhexidine for 30 seconds and allow to air dry. Remove the first set of gloves. • Place sterile drapes over the infant. • Infiltrate the area with local anaesthetic.
Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 11 of 16
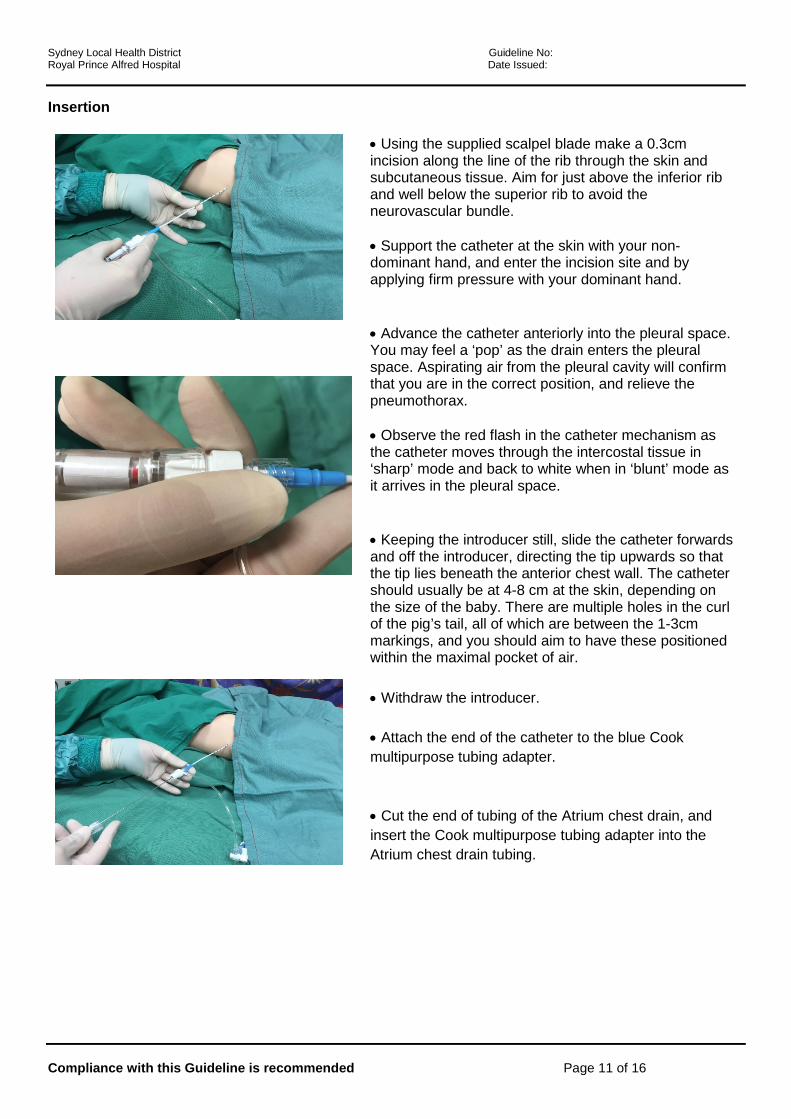
Insertion
• Using the supplied scalpel blade make a 0.3cm incision along the line of the rib through the skin and subcutaneous tissue. Aim for just above the inferior rib and well below the superior rib to avoid the neurovascular bundle. • Support the catheter at the skin with your non-dominant hand, and enter the incision site and by applying firm pressure with your dominant hand.
• Advance the catheter anteriorly into the pleural space. You may feel a ‘pop’ as the drain enters the pleural space. Aspirating air from the pleural cavity will confirm that you are in the correct position, and relieve the pneumothorax. • Observe the red flash in the catheter mechanism as the catheter moves through the intercostal tissue in ‘sharp’ mode and back to white when in ‘blunt’ mode as it arrives in the pleural space.
• Keeping the introducer still, slide the catheter forwards and off the introducer, directing the tip upwards so that the tip lies beneath the anterior chest wall. The catheter should usually be at 4-8 cm at the skin, depending on the size of the baby. There are multiple holes in the curl of the pig’s tail, all of which are between the 1-3cm markings, and you should aim to have these positioned within the maximal pocket of air.
• Withdraw the introducer. • Attach the end of the catheter to the blue Cook multipurpose tubing adapter.
• Cut the end of tubing of the Atrium chest drain, and insert the Cook multipurpose tubing adapter into the Atrium chest drain tubing.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 12 of 16
• Open the 3-way tap to the chest drain tubing.
Securing the catheter
• Ensure the skin is clean and dry prior to applying the dressing • Secure the pigtail catheter at the point of entry to the baby using 2-3 sterile surgical strips crossed over. • Please note that these drains do not require suturing in place.
• Apply two Tegaderms® on opposite sides of the catheter to ‘sandwich’ the catheter.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 13 of 16
• Reinforce the edge of the Tegaderm with the white strips from a Tegaderm IV. • Place a rectangle of Comfeel onto the skin by the hip, and anchor the catheter by forming a mesentery with Leukoplast. Secure the tubing to the infant’s bedding to ensure no traction on the drain. • Post-procedure, ensure you have ordered a chest x-ray and documented the procedure correctly in the infant’s notes. The ‘neonatal intercostal catheter insertion record’ form should be completed and placed in the notes.
3.3.4 Procedure to set up the Atrium Oasis Dry Suction Water Seal System
• Fill water seal to 2 cm line. Remove the sterile water ampoule from the rear of the drain and twist off the top. Squeeze the water into chamber B via the port on the top left hand side of the drain. Fill until the water fills chamber C to the 2 cm line. The water will turn blue.
• Connect chest drain to patient. Connect chest drain to patient prior to initiating suction.
• Connect chest drain to suction. Connect suction tubing from suction port to wall suction unit and adjust negative pressure until the bellows expand to mark E (-20 cm H2O). The bellows will not expand until suction is applied. The wall suction unit will need to be set at -80 mmHg/-5kpa or higher for -20 cm H2O to be reached.35
3.4 Risks and Complications
Minor complications of the flexible small-bore intercostal catheters are seen in up to 25% of preterm infants,30 and include failure to drain, kinking at the insertion site, blockage and accidental dislodgement. These can usually be remedied with careful attention to securing the catheter, and cautious handling of the infant once in situ. Serious complications are unusual, but may be life-threatening. They include haemothorax from laceration of intercostal or other large vessels, and perforation of underlying structures such as liver, lung, diaphragm or heart.28,36 These can be reduced with attention to anatomy and using the minimally required pressure during insertion.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 14 of 16
3. Key Points
Many pneumothoraces can be managed with careful observation only Level IV
An intercostal catheter should be inserted for pneumothoraces that are large and symptomatic or under tension
Level IV
A small-bore flexible pigtail catheter is the preferred first choice of catheter for pneumothorax in newborn infants
Level III
4. References 1. Davis CH, Stevens GW. Value of routine radiographic examination of the newborn, based on a study of 702 consecutive babies. Am J Obstet Gynecol 1930;20:73. 2. Walker MW, Shoemaker M, Riddle K, Crane MM, Clark R. Clinical process improvement: reduction of pneumothorax and mortality in high-risk preterm infants. J Perinatol 2002;22:641-5. 3. Chow SSW, Le Marsney R, Hossain S, Haslam R, Lui K. Report of the Australia and New Zealand Neonatal Network 2013. Sydney: Australia and New Zealand Neonatal Network; 2015. 4. Hill A, Perlman JM, Volpe JJ. Relationship of pneumothorax to occurrence of intraventricular hemorrhage in the premature newborn. Pediatrics 1982;69:144-9. 5. Bhatia R, Davis PG, Doyle LW, Wong C, Morley CJ. Identification of pneumothorax in very preterm infants. J Pediatr 2011;159:115-20 e1. 6. Wiswell TE, Tuggle JM, Turner BS. Meconium aspiration syndrome: have we made a difference? Pediatrics 1990;85:715-21. 7. Madansky DL, Lawson EE, Chernick V, Taeusch HW, Jr. Pneumothorax and other forms of pulmonary air leak in newborns. Am Rev Respir Dis 1979;120:729-37. 8. Yu VY, Liew SW, Robertson NR. Pneumothorax in the newborn. Changing pattern. Arch Dis Child 1975;50:449-53. 9. Bahadue FL, Soll R. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. The Cochrane database of systematic reviews 2012;11:CD001456. 10. Soll R, Ozek E. Multiple versus single doses of exogenous surfactant for the prevention or treatment of neonatal respiratory distress syndrome. The Cochrane database of systematic reviews 2009:CD000141. 11. Ardell S, Pfister RH, Soll R. Animal derived surfactant extract versus protein free synthetic surfactant for the prevention and treatment of respiratory distress syndrome. The Cochrane database of systematic reviews 2015;8:CD000144. 12. Soll R, Ozek E. Prophylactic protein free synthetic surfactant for preventing morbidity and mortality in preterm infants. The Cochrane database of systematic reviews 2010:CD001079. 13. Stevens TP, Harrington EW, Blennow M, Soll RF. Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. The Cochrane database of systematic reviews 2007:CD003063. 14. Greenough A, Rossor TE, Sundaresan A, Murthy V, Milner AD. Synchronized mechanical ventilation for respiratory support in newborn infants. The Cochrane database of systematic reviews 2016;9:CD000456.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 15 of 16
15. Wheeler K, Klingenberg C, McCallion N, Morley CJ, Davis PG. Volume-targeted versus pressure-limited ventilation in the neonate. The Cochrane database of systematic reviews 2010:CD003666. 16. Ho JJ, Subramaniam P, Davis PG. Continuous distending pressure for respiratory distress in preterm infants. The Cochrane database of systematic reviews 2015:CD002271. 17. Kamlin C, Davis PG. Long versus short inspiratory times in neonates receiving mechanical ventilation. The Cochrane database of systematic reviews 2004:CD004503. 18. Cools F, Offringa M, Askie LM. Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants. The Cochrane database of systematic reviews 2015:CD000104. 19. Cattarossi L, Copetti R, Brusa G, Pintaldi S. Lung Ultrasound Diagnostic Accuracy in Neonatal Pneumothorax. Can Respir J 2016;2016:6515069. 20. Kuhns LR, Bednarek FJ, Wyman ML, Roloff DW, Borer RC. Diagnosis of pneumothorax or pneumomediastinum in the neonate by transillumination. Pediatrics 1975;56:355-60. 21. Wyman ML, Kuhns LR. Accuracy of transillumination in the recognition of pneumothorax and pneumomediastinum in the neonate. Clin Pediatr (Phila) 1977;16:323-4. 22. Alrajab S, Youssef AM, Akkus NI, Caldito G. Pleural ultrasonography versus chest radiography for the diagnosis of pneumothorax: review of the literature and meta-analysis. Crit Care 2013;17:R208. 23. Blank DA, Hooper SB, Binder-Heschl C, et al. Lung ultrasound accurately detects pneumothorax in a preterm newborn lamb model. Journal of paediatrics and child health 2016;52:643-8. 24. Raimondi F, Rodriguez Fanjul J, Aversa S, et al. Lung Ultrasound for Diagnosing Pneumothorax in the Critically Ill Neonate. J Pediatr 2016;175:74-8 e1. 25. Litmanovitz I, Carlo WA. Expectant management of pneumothorax in ventilated neonates. Pediatrics 2008;122:e975-9. 26. Bruschettini M, Romantsik O, Ramenghi LA, Zappettini S, O'Donnell CP, Calevo MG. Needle aspiration versus intercostal tube drainage for pneumothorax in the newborn. The Cochrane database of systematic reviews 2016;1:CD011724. 27. Havelock T, Teoh R, Laws D, Gleeson F, Group BTSPDG. Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010;65 Suppl 2:ii61-76. 28. Roberts JS, Bratton SL, Brogan TV. Efficacy and complications of percutaneous pigtail catheters for thoracostomy in pediatric patients. Chest 1998;114:1116-21. 29. Arda IS, Gurakan B, Aliefendioglu D, Tuzun M. Treatment of pneumothorax in newborns: use of venous catheter versus chest tube. Pediatr Int 2002;44:78-82. 30. Wei YH, Lee CH, Cheng HN, Tsao LT, Hsiao CC. Pigtail catheters versus traditional chest tubes for pneumothoraces in premature infants treated in a neonatal intensive care unit. Pediatr Neonatol 2014;55:376-80. 31. Wood B, Dubik M. A new device for pleural drainage in newborn infants. Pediatrics 1995;96:955-6. 32. Martin K, Emil S, Zavalkoff S, et al. Transitioning from stiff chest tubes to soft pleural catheters: prospective assessment of a practice change. Eur J Pediatr Surg 2013;23:389-93. 33. Moessinger AC, Driscoll JM, Jr., Wigger HJ. High incidence of lung perforation by chest tube in neonatal pneumothorax. J Pediatr 1978;92:635-7. 34. Strutt J, Kharbanda A. Pediatric Chest Tubes And Pigtails: An Evidence-Based Approach To The Management Of Pleural Space Diseases. Pediatr Emerg Med Pract 2015;12:1-24; quiz 0-1.

Sydney Local Health District Guideline No: Royal Prince Alfred Hospital Date Issued:
Compliance with this Guideline is recommended Page 16 of 16
35. Atrium Oasis dry suction chest drains, Instructions for use. . (Accessed 17th May, 2016, at http://www.atriummed.com/en/chest_drainage/Documents/OasisWallChart-010395-Letter-Size.pdf.) 36. Reed RC, Waters BL, Siebert JR. Complications of percutaneous thoracostomy in neonates and infants. J Perinatol 2016;36:296-9.







![Management of Jaundice in Babies Less than 28 Days of Age€¦ · This guideline was developed in line with the NICE Neonatal Jaundice guideline [1], ... Phototherapy for babies near](https://static.fdocuments.net/doc/165x107/606332aed233223ce601f020/management-of-jaundice-in-babies-less-than-28-days-of-age-this-guideline-was-developed.jpg)










