
Women and Babies: Management of Patent Ductus Arteriosus ...content/pdf/guidelines... · Compliance...
19
Compliance with this Guideline is recommended Page 1 of 19 Guideline Women and Babies: Management of Patent Ductus Arteriosus in Preterm Infants Document No: RPAH_GL2016_002 Functional Sub-Group: Clinical Governance Corporate Governance Summary: Describes the pathophysiology diagnosis and management of patent ductus arteriosus in preterm babies National Standard: Standard 1 Governance for Safety and Quality in Health Service Organisations Standard 9 Recognising and responding to the derioriating patient. Author: A/Prof Nick Evans, Senior Staff Specialist Approved by: RPA Newborn Care Guideline Development Committee General Manager Publication (Issue) Date: January 2016 Next Review Date: January 2017 Replaces Existing Guideline: RPAH_GL2014_024 Previous Review Dates: March 2014
-
Upload
nguyenkhue -
Category
Documents
-
view
215 -
download
0
Transcript of Women and Babies: Management of Patent Ductus Arteriosus ...content/pdf/guidelines... · Compliance...
Compliance with this Guideline is recommended Page 1 of 19
Guideline
Women and Babies: Management of Patent Ductus Arteriosus in Preterm Infants
Document No: RPAH_GL2016_002 Functional Sub-Group: Clinical Governance
Corporate Governance Summary: Describes the pathophysiology diagnosis and management of patent ductus arteriosus in preterm babies
National Standard: Standard 1 Governance for Safety and Quality in Health Service Organisations
Standard 9 Recognising and responding to the derioriating patient. Author: A/Prof Nick Evans, Senior Staff Specialist Approved by: RPA Newborn Care Guideline Development Committee General Manager Publication (Issue) Date: January 2016 Next Review Date: January 2017 Replaces Existing Guideline: RPAH_GL2014_024 Previous Review Dates: March 2014
Compliance with this Guideline is recommended Page 2 of 19
Management of Patent Ductus Arteriosus in Preterm Infants
CONTENTS 1. Introduction ........................................................................................................... 3
2. Policy Statement .................................................................................................. 3
3. Principles / Guidelines .......................................................................................... 3
3.1. Summary of Guideline (for quick reference). .................................................. 3
3.2. Which drug to close PDA and at what dosage regimen? ................................ 3
3.3. When to treat? ................................................................................................ 4
4. Key Points ............................................................................................................ 5
DETAILED GUIDELINE (FOR FURTHER READING). ............. Error! Bookmark not defined. 4.1. Introduction ..................................................................................................... 6
4.2. Incidence and Risk Factors: ........................................................................... 6
5. Diagnosis .............................................................................................................. 6
5.1. Clinical diagnosis. ........................................................................................... 7
5.2. Ultrasound diagnosis.9 .................................................................................... 7
6. The natural history of preterm ductal constriction. ................................................ 9
Duct flow patterns and prediction of closure: ......................................................... 10
6.1. The natural history of preterm ductal shunting. ............................................ 10
7. Treatment ........................................................................................................... 11
7.1. When to treat the patent ductus arteriosus? ................................................. 11
7.2. Treating clinically apparent patent ducts. ..................................................... 11
7.3. Pre-symptomatic treatment. ......................................................................... 11
7.4. Prophylactic treatment. ................................................................................. 12
8. How to close the preterm patent ductus? ........................................................... 12
9. Performance Measures ...................................................................................... 15
10. References and links ....................................................................................... 15
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 3 of 19
Management of Patent Ductus Arteriosus in Preterm Infants 1. INTRODUCTION
The risks addressed by this guideline: Clinical risk of persisting patency of the Ductus Arteriosus in the preterm infant.
The aims / expected outcome of this guideline: Babies with PDA will be identified and appropriately managed by neonatal medical staff.
2. POLICY STATEMENT The goal of this guideline is to familiarise staff with current evidence in relation to pathophysiology, diagnosis and treatment of PDA in the preterm infant and to delineate the RPA Newborn Care approach to management of this problem. 3. PRINCIPLES / GUIDELINES SUMMARY GUIDELINE FOR QUICK REFERENCE.
3.1. Which drug to close PDA and at what dosage regimen?
For early ultrasound targeted treatment (in babies born before 28 weeks), consider indomethacin as first line. For later symptomatic treatment, either indomethacin or ibuprofen are acceptable for treatment. The evidence slightly favours ibuprofen in this situation due to less side effects.
Consider paracetamol for second line medical treatment when either ibuprofen or indomethacin have failed to close a significant PDA.
Indomethacin : To be used first line for early ultrasound targeted treatment before 24 hours of age in babies born before 28 weeks. We use the regimen described by Tammela et al47 and used in the DETECT trial27 of 0.2mg/kg, further doses of 0.1mg/kg, 0.1mg/kg at 24 hours intervals to give only if ductal diameter >1.6mm 24 hours after the first dose.
Ibuprofen: To be used for later symptomatic treatment after 48 hrs. The standard dosage regimen of 10mg/kg, 5mg/kg, 5 mg/kg at 24 hour intervals will be the usual starting dosage.
The higher dosage regimen of 20mg/kg, 10mg/kg, 10mg/kg at 24 hours intervals should be considered in babies older than day 5, particularly if there has been failure to close with the 10mg/kg, 5 mg/kg, 5 mg/kg regimen and consider giving orally after 48 hours depending on feed tolerance.
Paracetamol: This cannot yet be considered a first line treatment as the evidence on this drug is still evolving. There has not yet been a placebo comparison or longer term follow up. Three trials have shown comparable closure rates to indomethacin and ibuprofen with no difference in side effects so paracetamol can be considered as second line treatment for PDAs unresponsive to ibuprofen or indomethacin. Dosage regimen is 15mg/kg orally 6 hourly for 3 days. With consideration to continuing for up to 7 days where the PDA fails to close after 3 days.
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 4 of 19
3.2. When to treat?
In babies born before 28 weeks, consider early ultrasound targeted treatment:
The pathophysiological observations of the early haemodynamic impact of poorly constricting preterm PDAs are consistent with the improvements in short term outcomes seen with early prophylactic or targeted treatment, particularly with respect to peri/intraventricular haemorrhage (P/IVH) and pulmonary haemorrhage. There is reasonable evidence of no harm with early treatment from the prophylactic treatment trials. There is also merit in limiting dose exposure and attempting to target treatment at those most likely to benefit, on the basis of early ductal constriction and early clinical risk factors.
• Babies born before 28 weeks should have a neonatologist clinician performed cardiac ultrasound, ideally between 3 and 6 hours of age, but before 12 hours.
• Consider treatment with 0.2 mg/kg of indomethacin if all the following ultrasound criteria are met:
o The heart is structurally normal with particular reference to the aortic arch. o The duct is more than or equal to 2.0 mm in diameter at its narrowest point (usually the
pulmonary end). o That significant pulmonary hypertension is excluded on the basis that any right to left
shunting occupies less than 30% of the cardiac cycle. If there is significant pulmonary hypertension in a duct 2.0 mm or above, then consider repeat neonatal clinician performed ultrasound in 6 hours and treatment at this time if the duct remains large and the shunt has become more left to right.
• Babies should have a repeat cardiac ultrasound 24 hours after the first dose and if the PDA has constricted to ≤1.6mm then no further doses should be given. If the diameter is >1.6 mm, two further doses of 0.1 mg/kg of indomethacin should be given at 24 hr intervals.
In babies born from 28 weeks onwards, consider symptomatic treatment.
These babies should be monitored for presence of a PDA by routine clinical examination with neonatal clinician performed cardiac ultrasound if clinically indicated. Medical treatment should be considered if all three of the conditions below are fulfilled:
1. The baby has a clinically apparent PDA on the basis of physical signs
2. Ultrasound findings confirming large PDA with significant shunt defined by: • Diameter at narrowest point of more than or equal to 2.0mm together with one or more
of the following: 1. Reversed diastolic flow in the post ductal descending aorta 2. Increased velocities in the left pulmonary artery (diastolic >0.2m/sec, mean
>0.45m/sec) 3. Dilation of the left atrium and or left ventricle.
3. Symptoms that may be related to the ductal shunt including: • Pulmonary haemorrhage • Inability to wean from the ventilator beyond 72 hrs of age. • Respiratory instability including increasing apnoea and rising oxygen requirements. • Later symptoms, there are a range of non-specific symptoms that should be ascribed
to a PDA with caution based on ultrasound findings and whether the symptoms are out of keeping with what might be expected, including:
1. Persistent oxygen requirements 2. Feed intolerance
3. Fluid retention or other renal signs
There is some evidence that ibuprofen treatment of symptomatic PDA carries less subsequent risk of NEC than indomethacin and prolonged courses of indomethacin are associated with NEC. While
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 5 of 19
treatment with either drug is acceptable, consideration should be given to using ibuprofen first line with consideration to giving it orally at the same dose as intravenously, (10mg/kg, 5mg/kg, 5mg/kg at 24 hour intervals) if it is decided to treat a symptomatic PDA after 48 hours of life.
Duration of treatment:
• Shortening duration of treatment:
• Side effects: If side effects develop that might relate to medical treatment, consideration should be given to not giving further doses. Such side effects might include: gastrointestinal bleeding, rising creatinine, thrombocytopaenia.
• Good early constriction: A neonatologist performed cardiac ultrasound can be repeated prior to the second dose of ibuprofen and, if the duct is constricted to ≤1.6 mm diameter on colour Doppler, consideration should be given to not giving further doses. If the ductus is closed prior to the second dose, further doses are probably not needed.
• Prolonging duration of treatment: If the ductus is still patent 24 hours after the 3rd dose, then consideration should be given to giving further doses up to a maximum of 6 doses of 5mg/kg of Ibuprofen or 0.1mg/kg of Indomethacin. Lower gestational age and a larger diameter ductus make it more likely that the PDA will continue to be a problem.
Medical re-treatment:
Babies who fail to respond to a first course of medical treatment, usually do not respond to further courses so consider paracetamol in babies who have failed to respond to first line treatment and in whom the PDA remains symptomatic and haemodynamically significant.
Surgical Ligation:
Consideration for ligation should be confined to babies who remain on substantial respiratory support and have unequivocal ultrasound features of haemodynamic significance and medical treatment has failed (usually after two courses) or medical treatment is contraindicated.
4. KEY POINTS Key Points
Level of Evidence
Risk of PDA increases with lower gestation, lack of antenatal steroids and hyaline membrane disease.
Level of Evidence III3,4
Early diagnosis requires cardiac ultrasound Level of Evidence II5,6 Larger ductal diameter is associated with lower systemic blood flow in the first 12 hours after birth.
Level of Evidence II15
Indomethacin or Ibuprofen are the first line treatment. Consider surgery only if medical treatment has failed or is contraindicated and there are persisting cardiopulmonary symptoms that are probably due to ductal shunting.
Level of Evidence I33 Grade of Recommendation A
Prophylactic indomethacin reduces incidence of IVH but does not improve neurodevelopmental outcomes.
Level of Evidence I39
Early prophylactic or targeted treatment of ducts with indomethacin may reduce the risk of early pulmonary haemorrhage.
Level of Evidence II27,28 Grade of Recommendation B
If the duct has significantly constricted 24 hrs after the first dose, consideration should be given to not giving further doses.
Level of Evidence II30 Grade of Recommendation B
Oral ibuprofen appears to be as effective and may be more effective than intravenous ibuprofen in babies treated after 48 hrs of age.
Level of Evidence II42,43 Grade of Recommendation B
The evidence for oral paracetamol is limited but the trials to Level of Evidence II58,59,Dash
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 6 of 19
date have suggest it is as effective as oral ibuprofen and intravenous indomethacin in the closure of PDA.
5. DETAILED GUIDELINE FOR FURTHER READING
5.1. Introduction
The traditional view of preterm ductal shunting has been that the duct of the premature infant doesn’t constrict in the early postnatal period but, because of raised pulmonary artery pressure, the haemodynamic effect of this is either a negligible or a right to left shunt with resultant worsening hypoxia.1,2 The development of Doppler ultrasound has given us a window on the natural history of the preterm ductus that questions the current relevance of this thinking.
5.2. Incidence and Risk Factors:
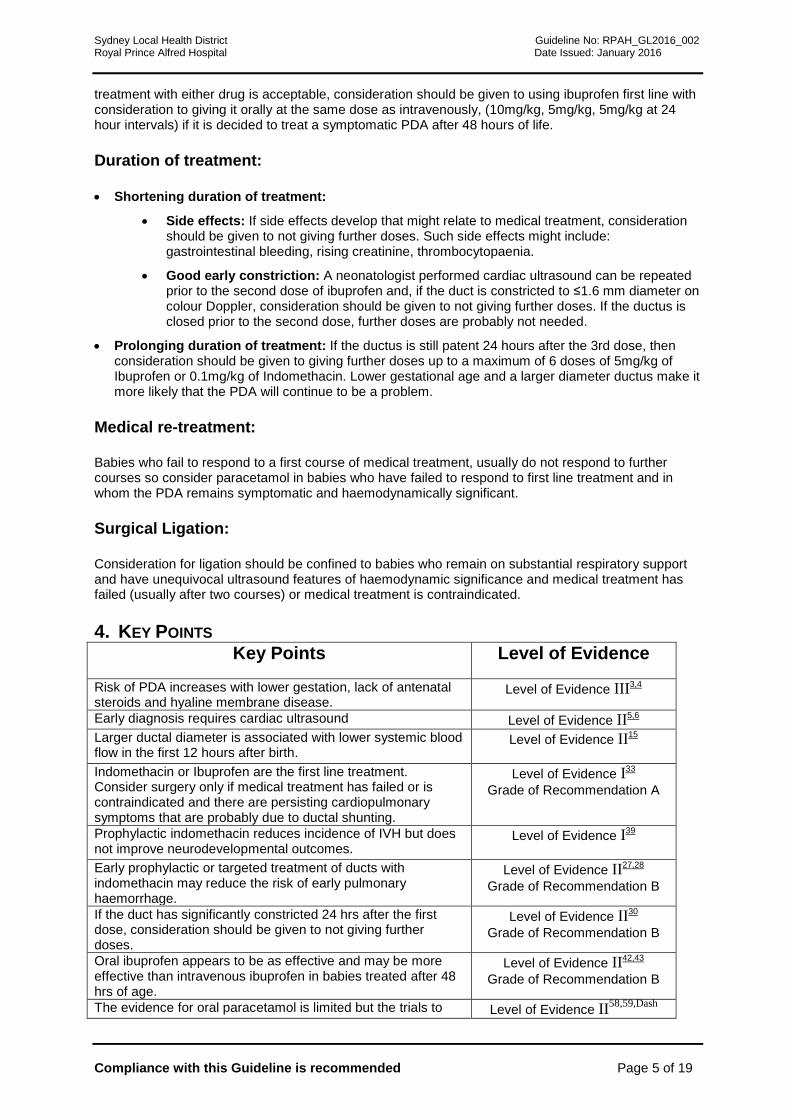
The most important determinant of incidence of persistent patency of the ductus arteriosus (PDA) is low gestation. Lack of antenatal steroids and need for ventilation are also risk factors for PDA 3,4. The graph below shows the incidence of medical and surgical treatment for PDA according to gestation at birth within the New South Wales and Australian Capital Territory network of 10 tertiary NICUs for the years 2007 to 2011.
6. DIAGNOSIS The literature on diagnosis of PDA is confused by poorly defined terminology with terms such as ‘symptomatic’, ‘clinically apparent’ and ‘haemodynamically significant’ often used interchangeably. There are no standard definitions but below would be our interpretation of the meaning of these terms:
‘Clinically apparent PDA’ refers to presence of physical signs consistent with a PDA such as murmur, active praecordium or full pulses, preferably confirmed by cardiac ultrasound.
‘Symptomatic PDA’ implies that the PDA may be having a clinical impact on the baby’s condition. This is really hard to define as most ‘clinical symptoms’ of a PDA are non-specific and may or may not relate to a concurrent PDA. Probably the respiratory and circulatory effects of a PDA are easiest to define and may include persistent ventilator dependence, deteriorating respiratory status, increasing recurrent apnoea, pulmonary haemorrhage and hypotension. Probably the most specific of these would be pulmonary haemorrhage,8 particularly if it occurs within the first week of life and is associated with a respiratory deterioration.
‘Haemodynamically significant PDA’ refers to ultrasound findings that are consistent with a large shunt volume. Again there are no standard definitions but this will often be based on ductal diameter together with a range of indirect markers of shunt size as discussed below.
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 7 of 19
6.1. Clinical diagnosis. Reliance on clinical signs, such as an active praecordium, full pulses or a systolic murmur, will eventually make the diagnosis of a PDA but only after the left to right shunt through the duct has been significant for some days. Blinded comparison of these clinical signs to cardiac ultrasound criteria of ductal haemodynamic significance (discussed below) 5, have shown it is normal for haemodynamically significant ducts to be clinically silent for the first 2 to 3 days of life. From day 4 onwards, physical signs, particularly the murmur, become more accurate but some inaccuracy persists up to day 7 of life 6. Wide pulse pressure also does not accurately diagnose patent ducts in the first week of life.7
Thus a ‘haemodynamically significant” PDA and/or ‘symptomatic’ PDA may not be ‘clinically apparent’ particularly in the first few postnatal days. Accurate and early diagnosis of significant ductal shunting depends on cardiac ultrasound.
6.2. Ultrasound diagnosis.9
Accurate diagnosis relies on cardiac ultrasound.
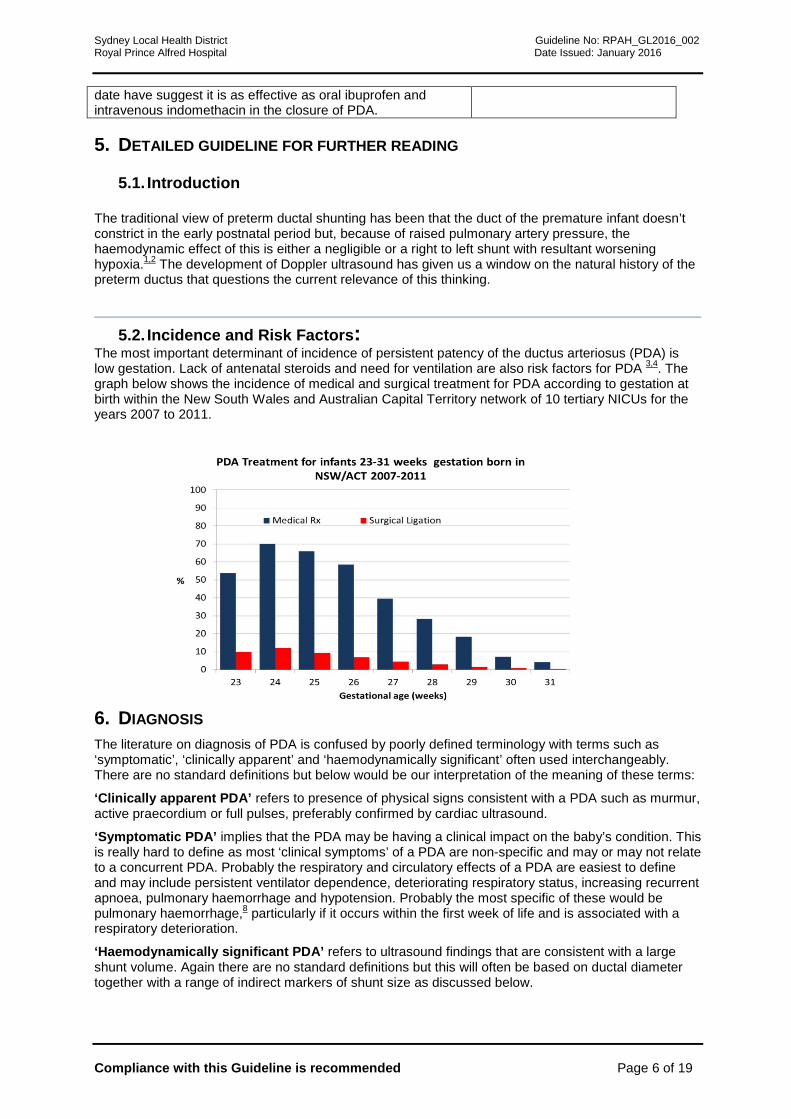
• Patency can be confirmed by diastolic turbulence on Doppler in the pulmonary artery. The picture below shows the diastolic turbulence seen with a patent duct. This is a reasonably accurate method for diagnosing ductal patency with left to right shunting but tells you little about the haemodynamic significance.
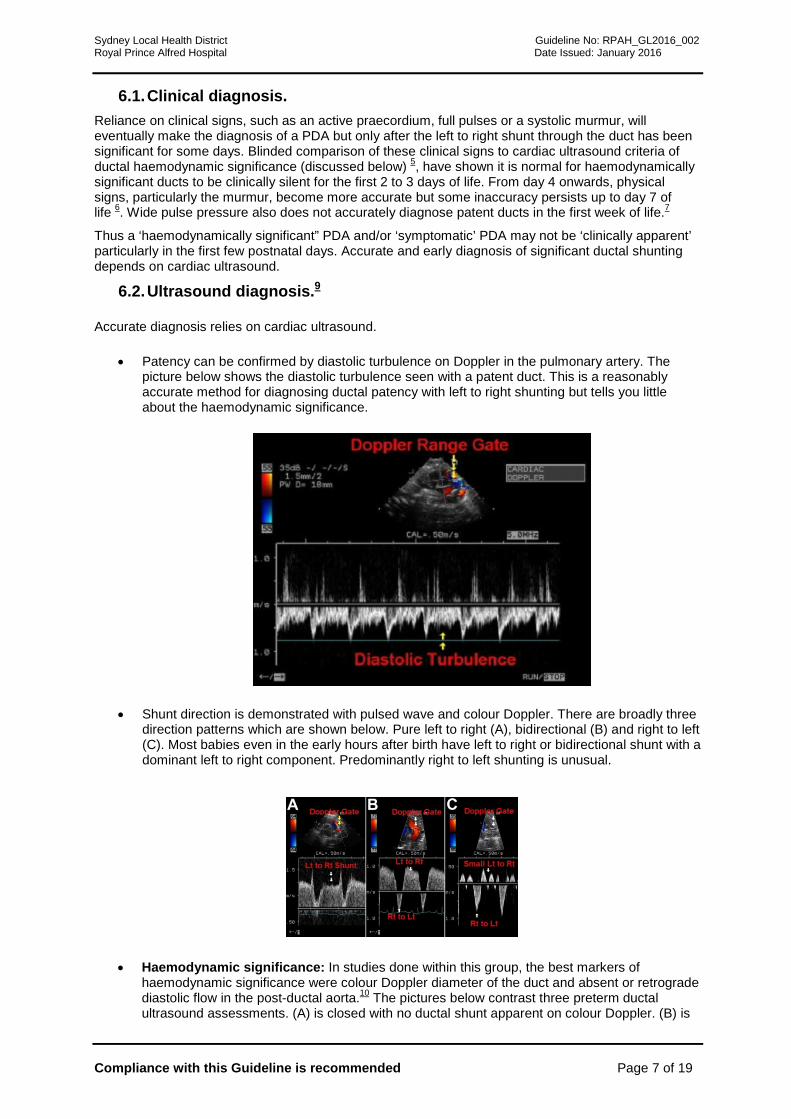
• Shunt direction is demonstrated with pulsed wave and colour Doppler. There are broadly three direction patterns which are shown below. Pure left to right (A), bidirectional (B) and right to left (C). Most babies even in the early hours after birth have left to right or bidirectional shunt with a dominant left to right component. Predominantly right to left shunting is unusual.
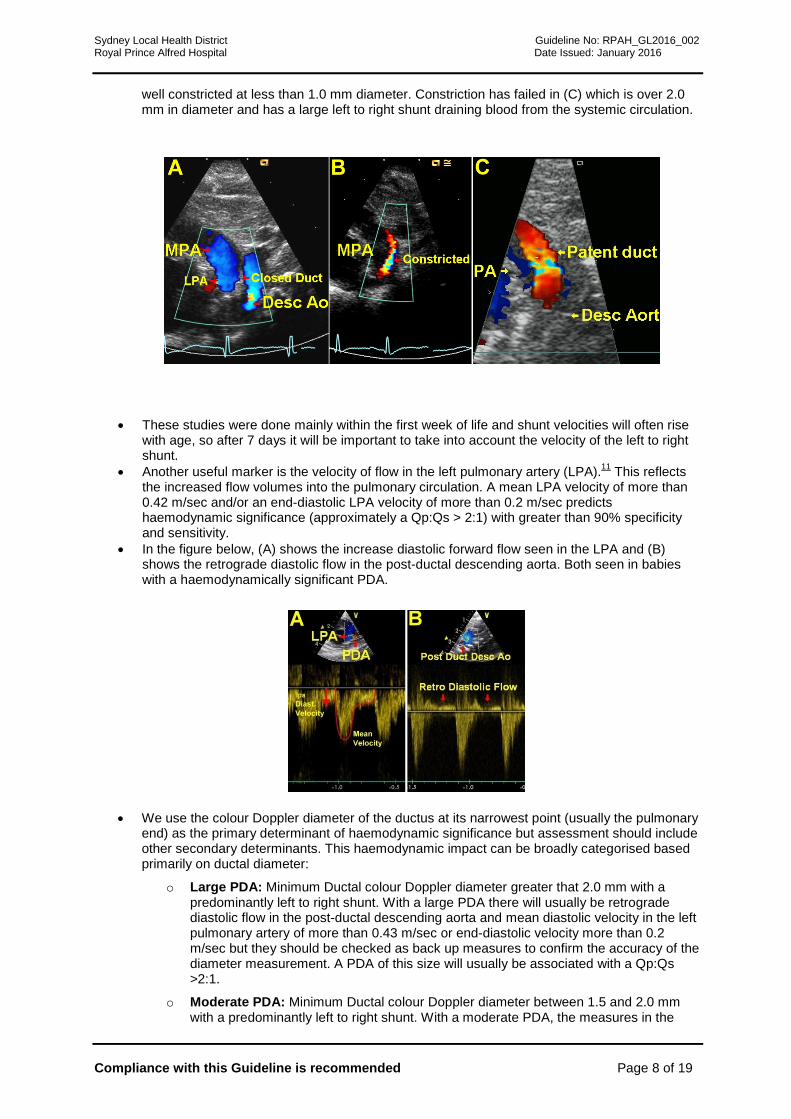
• Haemodynamic significance: In studies done within this group, the best markers of haemodynamic significance were colour Doppler diameter of the duct and absent or retrograde diastolic flow in the post-ductal aorta.10 The pictures below contrast three preterm ductal ultrasound assessments. (A) is closed with no ductal shunt apparent on colour Doppler. (B) is
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 8 of 19
well constricted at less than 1.0 mm diameter. Constriction has failed in (C) which is over 2.0 mm in diameter and has a large left to right shunt draining blood from the systemic circulation.
• These studies were done mainly within the first week of life and shunt velocities will often rise with age, so after 7 days it will be important to take into account the velocity of the left to right shunt.
• Another useful marker is the velocity of flow in the left pulmonary artery (LPA).11 This reflects the increased flow volumes into the pulmonary circulation. A mean LPA velocity of more than 0.42 m/sec and/or an end-diastolic LPA velocity of more than 0.2 m/sec predicts haemodynamic significance (approximately a Qp:Qs > 2:1) with greater than 90% specificity and sensitivity.
• In the figure below, (A) shows the increase diastolic forward flow seen in the LPA and (B) shows the retrograde diastolic flow in the post-ductal descending aorta. Both seen in babies with a haemodynamically significant PDA.
• We use the colour Doppler diameter of the ductus at its narrowest point (usually the pulmonary end) as the primary determinant of haemodynamic significance but assessment should include other secondary determinants. This haemodynamic impact can be broadly categorised based primarily on ductal diameter:
o Large PDA: Minimum Ductal colour Doppler diameter greater that 2.0 mm with a predominantly left to right shunt. With a large PDA there will usually be retrograde diastolic flow in the post-ductal descending aorta and mean diastolic velocity in the left pulmonary artery of more than 0.43 m/sec or end-diastolic velocity more than 0.2 m/sec but they should be checked as back up measures to confirm the accuracy of the diameter measurement. A PDA of this size will usually be associated with a Qp:Qs >2:1.
o Moderate PDA: Minimum Ductal colour Doppler diameter between 1.5 and 2.0 mm with a predominantly left to right shunt. With a moderate PDA, the measures in the
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 9 of 19
descending aorta and left pulmonary artery will be more variable but should be assessed. A PDA of this size will usually be associated with a Qp:Qs >1.5:1.
o Small PDA: Minimum Ductal colour Doppler diameter less than 1.5 mm with a predominantly left to right shunt. With a small PDA, the diastolic flow in the descending aorta will usually be antegrade and left pulmonary artery velocities will be below the thresholds defined above. If this is not the case, the accuracy of the diameter measurement should be reviewed.
o Closed PDA: There is no shunt within the ductus that is apparent on colour Doppler.
• At RPAH, the Doppler ultrasound characteristics of a haemodynamically significant PDA will usually fulfil the criteria above for a large PDA.
7. THE NATURAL HISTORY OF PRETERM DUCTAL CONSTRICTION.
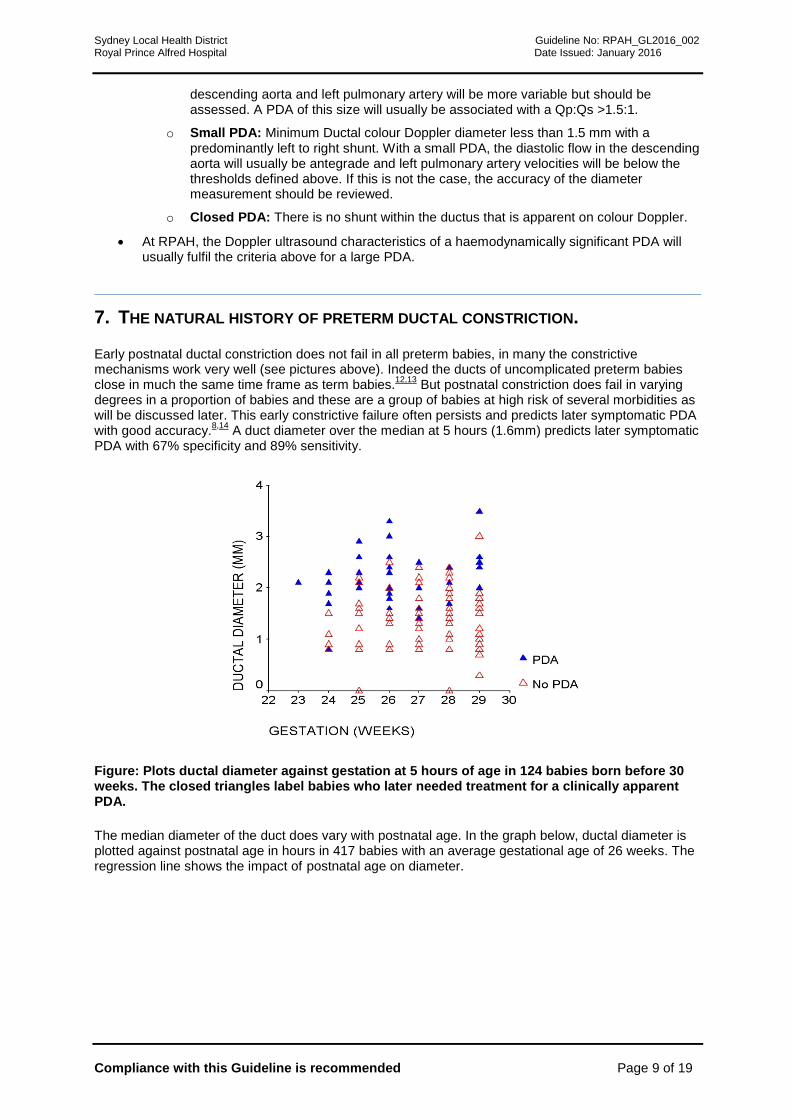
Early postnatal ductal constriction does not fail in all preterm babies, in many the constrictive mechanisms work very well (see pictures above). Indeed the ducts of uncomplicated preterm babies close in much the same time frame as term babies.12,13 But postnatal constriction does fail in varying degrees in a proportion of babies and these are a group of babies at high risk of several morbidities as will be discussed later. This early constrictive failure often persists and predicts later symptomatic PDA with good accuracy.8,14 A duct diameter over the median at 5 hours (1.6mm) predicts later symptomatic PDA with 67% specificity and 89% sensitivity.
Figure: Plots ductal diameter against gestation at 5 hours of age in 124 babies born before 30 weeks. The closed triangles label babies who later needed treatment for a clinically apparent PDA.
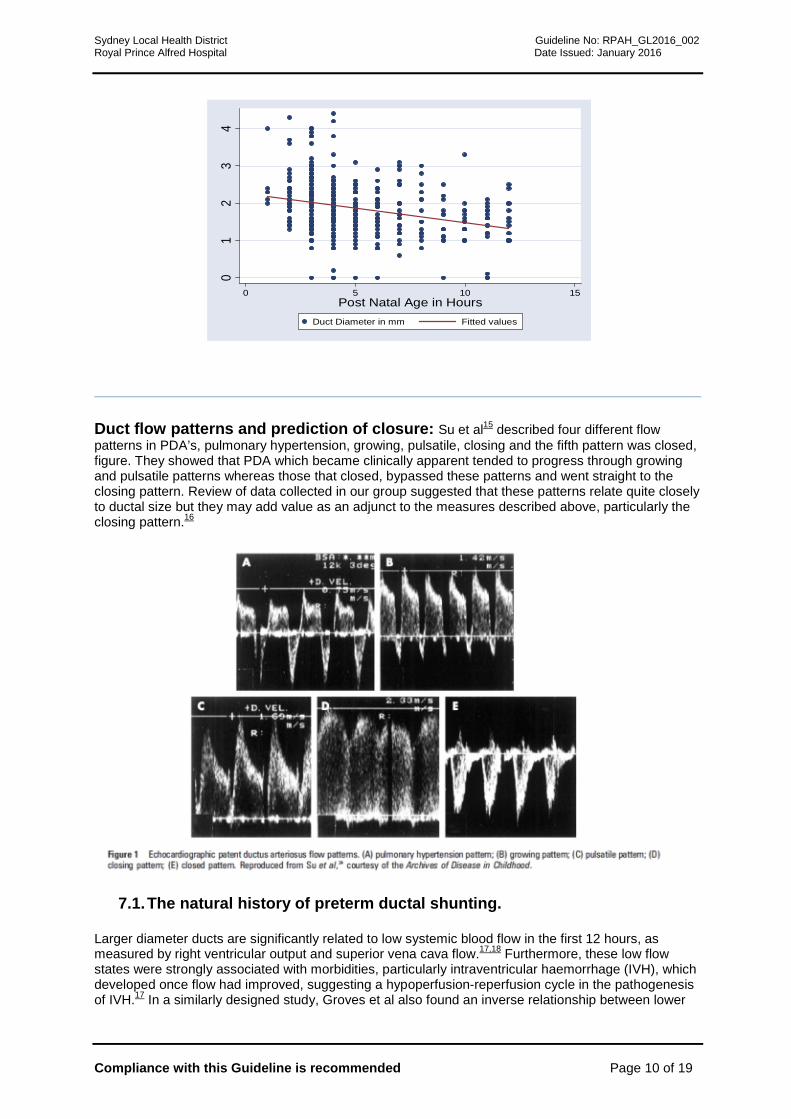
The median diameter of the duct does vary with postnatal age. In the graph below, ductal diameter is plotted against postnatal age in hours in 417 babies with an average gestational age of 26 weeks. The regression line shows the impact of postnatal age on diameter.
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 10 of 19
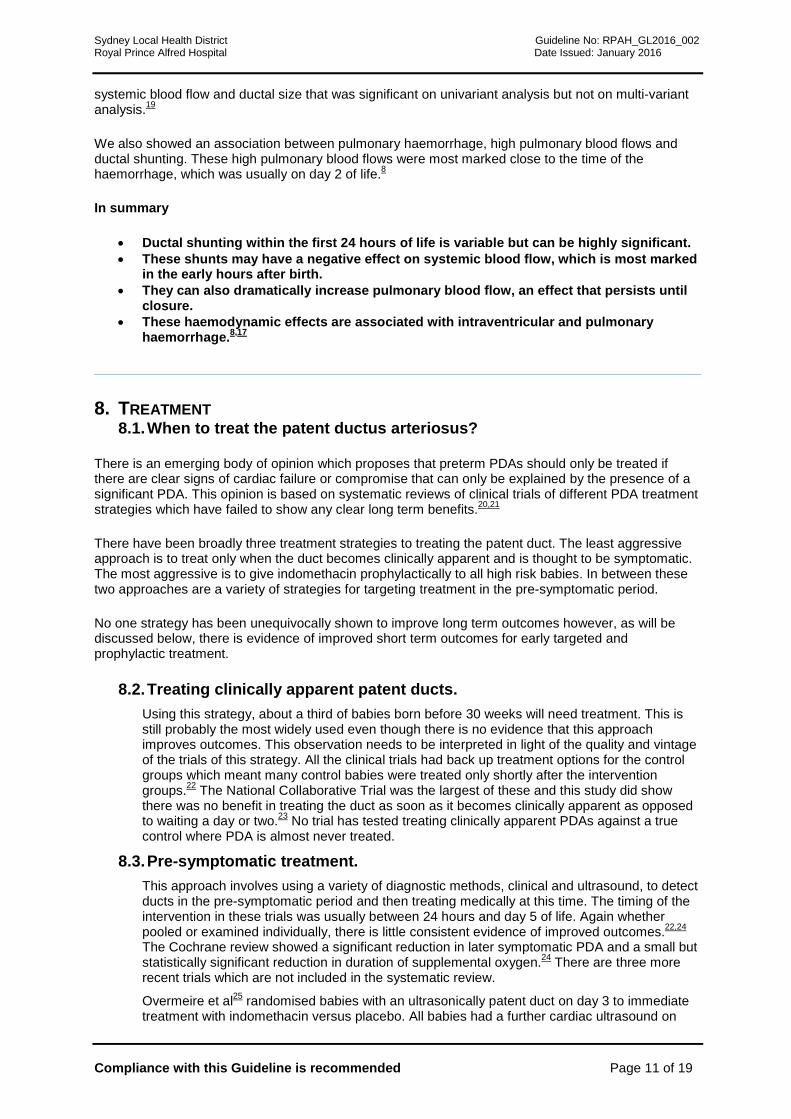
Duct flow patterns and prediction of closure: Su et al15 described four different flow patterns in PDA’s, pulmonary hypertension, growing, pulsatile, closing and the fifth pattern was closed, figure. They showed that PDA which became clinically apparent tended to progress through growing and pulsatile patterns whereas those that closed, bypassed these patterns and went straight to the closing pattern. Review of data collected in our group suggested that these patterns relate quite closely to ductal size but they may add value as an adjunct to the measures described above, particularly the closing pattern.16
7.1. The natural history of preterm ductal shunting.
Larger diameter ducts are significantly related to low systemic blood flow in the first 12 hours, as measured by right ventricular output and superior vena cava flow.17,18 Furthermore, these low flow states were strongly associated with morbidities, particularly intraventricular haemorrhage (IVH), which developed once flow had improved, suggesting a hypoperfusion-reperfusion cycle in the pathogenesis of IVH.17 In a similarly designed study, Groves et al also found an inverse relationship between lower
01
23
4
0 5 10 15Post Natal Age in Hours
Duct Diameter in mm Fitted values
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 11 of 19
systemic blood flow and ductal size that was significant on univariant analysis but not on multi-variant analysis.19
We also showed an association between pulmonary haemorrhage, high pulmonary blood flows and ductal shunting. These high pulmonary blood flows were most marked close to the time of the haemorrhage, which was usually on day 2 of life.8
In summary
• Ductal shunting within the first 24 hours of life is variable but can be highly significant. • These shunts may have a negative effect on systemic blood flow, which is most marked
in the early hours after birth. • They can also dramatically increase pulmonary blood flow, an effect that persists until
closure. • These haemodynamic effects are associated with intraventricular and pulmonary
haemorrhage.8,17
8. TREATMENT 8.1. When to treat the patent ductus arteriosus?
There is an emerging body of opinion which proposes that preterm PDAs should only be treated if there are clear signs of cardiac failure or compromise that can only be explained by the presence of a significant PDA. This opinion is based on systematic reviews of clinical trials of different PDA treatment strategies which have failed to show any clear long term benefits.20,21
There have been broadly three treatment strategies to treating the patent duct. The least aggressive approach is to treat only when the duct becomes clinically apparent and is thought to be symptomatic. The most aggressive is to give indomethacin prophylactically to all high risk babies. In between these two approaches are a variety of strategies for targeting treatment in the pre-symptomatic period.
No one strategy has been unequivocally shown to improve long term outcomes however, as will be discussed below, there is evidence of improved short term outcomes for early targeted and prophylactic treatment.
8.2. Treating clinically apparent patent ducts. Using this strategy, about a third of babies born before 30 weeks will need treatment. This is still probably the most widely used even though there is no evidence that this approach improves outcomes. This observation needs to be interpreted in light of the quality and vintage of the trials of this strategy. All the clinical trials had back up treatment options for the control groups which meant many control babies were treated only shortly after the intervention groups.22 The National Collaborative Trial was the largest of these and this study did show there was no benefit in treating the duct as soon as it becomes clinically apparent as opposed to waiting a day or two.23 No trial has tested treating clinically apparent PDAs against a true control where PDA is almost never treated.
8.3. Pre-symptomatic treatment. This approach involves using a variety of diagnostic methods, clinical and ultrasound, to detect ducts in the pre-symptomatic period and then treating medically at this time. The timing of the intervention in these trials was usually between 24 hours and day 5 of life. Again whether pooled or examined individually, there is little consistent evidence of improved outcomes.22,24 The Cochrane review showed a significant reduction in later symptomatic PDA and a small but statistically significant reduction in duration of supplemental oxygen.24 There are three more recent trials which are not included in the systematic review.
Overmeire et al25 randomised babies with an ultrasonically patent duct on day 3 to immediate treatment with indomethacin versus placebo. All babies had a further cardiac ultrasound on
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 12 of 19
day 7 and the duct was treated again if still patent. There was no difference in individual clinical outcomes but a combination of adverse short term outcomes was higher in those treated on day 3.
Aranda et al26 randomised 136 babies (<1kg and <30 weeks) to ibuprofen or placebo if they had an ultrasonically significant PDA within 72 hours of birth. Babies were treated at an average of 1.5 days of age. Babies who received ibuprofen had a significantly better composite primary outcome of need for PDA rescue treatment, death or dropped (out from the trial), 31% vs 53%, p<0.005. There were no significant differences in the individual outcomes but a trend to lower rates of PVL with early ibuprofen (0% vs 6%, p=0.057).
The DETECT trial,27 conducted at this hospital and Royal North Shore Hospital in Sydney and King Edward Memorial Hospital in Perth, had to be stopped early due to withdrawal of indomethacin from the Australian market. In this trial, babies born before 29 weeks had a neonatologist performed cardiac ultrasound within the first 12 hours of life and were randomised to indomethacin or placebo if the ductal diameter was above the median for that age. Babies below the median were not treated. Forty two babies were randomised to indomethacin and 44 to placebo. There was no difference in the primary outcome of death or major P/IVH or PVL. Babies randomised to indomethacin had significantly less need for further treatment for PDA (20% vs 40%, p=0.04) and clinically interesting trend to less major pulmonary haemorrhage (9% vs 23%, p=0.06), which was significantly different for major pulmonary haemorrhage occurring during the first 72 hours.
8.4. Prophylactic treatment. This strategy involves the administration of treatment to all high-risk infants on the first day, usually within the first 6 hours. The meta-analysis of 2872 preterm babies randomised prophylactic indomethacin trials shows significant reductions after indomethacin in intraventricular haemorrhage, later symptomatic PDA and reduced PDA ligation rates but little effect on other morbidities particularly respiratory outcomes.28 Despite this evidence, this approach has not gained widespread acceptance mainly due to concerns about the effect of indomethacin in reducing cerebral blood flow29,30 and that follow up studies from two of the largest trials have not shown any significant improvement on developmental outcomes.31,32
Meta-analysis of 931 babies randomised into prophylactic ibuprofen trials showed reduced rate of later symptomatic PDA and reduced PDA ligation but no difference in any other clinical outcomes including major IVH.33 Neurodevelopmental outcomes from these studies have not been published.
With the evidence of some benefit from an early targeted treatment together with the lack of apparent harms from early prophylactic treatment, at RPAH, we consider using the early targeted indomethacin approach in the babies at highest risk, those born before 28 weeks and will use the approach of treating clinically apparent and symptomatic PDA in babies born after this time (see guideline essentials).
9. HOW TO CLOSE THE PRETERM PATENT DUCTUS? Indomethacin or Ibuprofen?: Ductal patency is maintained by circulating prostaglandins and both these drugs work by a general inhibition of prostaglandin synthesis. Indomethacin has been used for many years and will close the duct in most cases but at the expense of some side effects including transient reduced cerebral blood flow,29 oliguria, hyponatraemia and gastro-intestinal complications. Most of these side effects are transient and self-limiting. Infusing the dose over 20 to 30 minutes may reduce but does not eliminate the effect on cerebral blood flow.30
Ibuprofen has less side effects and has become established as an alternative to indomethacin. Randomised trials have shown it to have similar efficacy in closing the duct with a lower rate of renal side effects.34-36 In clinical trials, both indomethacin and ibuprofen have about a 75% success rate for ductal closure. Blood flow studies have shown that ibuprofen has less negative effects on cerebral blood flow.37 One trial of prophylactic ibuprofen was stopped early because three babies seemed to have pulmonary hypertensive crises shortly after being given ibuprofen.38 It is still not really known whether this was an effect of ibuprofen but there are other case reports of this reaction appearing in the literature.61 There is a small risk reduction in NEC rates after ibuprofen compared to indomethacin but no significant differences in any longer term clinical outcomes between indomethacin and ibuprofen.36
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 13 of 19
While either indomethacin or ibuprofen would be acceptable treatment for either early or later treatment, the evidence would suggest that indomethacin should be considered first for early treatment and ibuprofen for later treatment. The evidence for improvement in short term outcomes with early treatment (either prophylactic or early targeted) is based on treatment with indomethacin. These improved outcomes have not been shown with prophylactic ibuprofen. On the other hand, the reduced rate of NEC with ibuprofen compared to indomethacin was based on studies using later treatment.
In our post-implementation audit of changing to ibuprofen in 2010, we have not been to duplicate the 75% closure rate of the clinical trials. Just 51% of 90 PDAs closed in response to ibuprofen treatment.
What dosage regimen for Ibuprofen? The usual regimen for Ibuprofen has been 10 mg/kg as a loading dose followed by two doses of 5 mg/kg at 24 hour intervals. Much of the current trial evidence for ibuprofen was based on the use of Lysine ibuprofen whereas the commercial preparation for newborns is Sodium ibuprofen and there is also a much cheaper Arginine Ibuprofen preparation available. It is not known whether the compounding of Ibuprofen makes a difference to efficacy although De Carolis et al described a ‘before and after’ changing from Lysine Ibuprofen to Sodium Ibuprofen study, in which they reported a significant reduction in successful medical closure from 73% to 50%, p<0.002 after changing to sodium ibuprofen.39
Two recent studies have suggested that higher doses of ibuprofen may improve closure efficacy. Hirt et al40 performed a pharmacokinetic study which suggested an optimised regimen based on postnatal age: 10, 5, 5 mg/kg for neonates younger than 70 hours, 14, 7, 7 mg/kg for neonates between 70 and 108 h and 18, 9, 9 mg/kg for neonates between 108 and 180 h. Dani et al41 took a simpler approach of randomising 70 babies born before 29 weeks, with RDS and an ultrasound significant PDA between 12 and 24 hrs to Ibuprofen 10,5,5 mg/kg vs 20,10,10 mg/kg. The latter regimen achieved significantly better closure (63 vs 86%%, p = 0.03) with no significant difference in adverse effects.
The data on safety of the higher dose is limited but it seems reasonable to consider a higher dosage regimen (20, 10,10 mg/kg) in babies after day 5, particularly if they haven't responded to the usual dose regimen. Prior to that time, we will use the standard 10mg/kg, 5 mg/kg, 5 mg/kg at 24 hours intervals.
Oral or Intravenous Ibuprofen? Intravenous Ibuprofen is expensive while oral Ibuprofen is cheap. This has led to studies, mainly is less well-resourced health systems, into the use of oral Ibuprofen for preterm PDA closure. Early studies suggest oral Ibuprofen was as effective as intravenous but two recent RCTs from the same Turkish group suggest it may be better than intravenous.
Gokmen et al42 randomised 102 babies born before 32 weeks and BW <1500g to oral or intravenous ibuprofen at 10,5,5 mg/kg. The oral group had significantly better closure rate of 85% vs 62% with no difference in side effects or other outcomes. They repeated this study in a more immature cohort of 80 babies born before 28 weeks and BW <1000g and got similar results with 83% closure with oral vs 63% with intravenous.43 Both these studies randomised babies between 48 and 96 hrs of age so the findings may not be generalisable to treatment before 48 hrs of age.
At RPAH, consideration should be made to giving ibuprofen orally where a PDA is being treated after 48 hours of age. The dosage is the same as given intravenously (10mg/kg, 5 mg/kg, 5 mg/kg at 24 hours intervals).
What regimen for Indomethacin? Infusing the dose over 20 to 30 minutes may reduce but does not eliminate the effect on cerebral blood flow.30 Three randomised trials have shown that a dose of 0.1mg/kg daily for 6 days is as effective as the traditional 0.2mg/kg 12hrly for three doses but causes less side effects.44-46 However, a more recent trial using 0.2mg/kg followed by two lower doses at 0.1mg.kg showed no advantage to a longer course.47 As indomethacin has a long half life in the preterm newborn, there is pharmacokinetic logic to a higher initial loading dose.
Meta-analysis of trials comparing short (3 doses) vs long (6 doses) course indomethacin confirms similar efficacy with less side effects but does show a higher risk of NEC with longer courses. As a result, the authors of this review caution against the routine use of longer courses.48 At RPAH, we use the regimen of Tamella et al,47 also used in the DETECT trial27 of 0.2mg/kg, 0.1 mg/kg, 0.1mg/kg at 24 hours intervals.
How long to continue indomethacin or ibuprofen? Babies will often close their ducts very quickly after one or two doses of indomethacin. In these babies, the question arises of whether
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 14 of 19
the full course needs to be given. The randomised data suggests the longer 6 day course is associated with less re-opening in the short term but at a cost of a possibly higher NEC rate. However there is good evidence from ultrasound surveillance, that ducts that were thought to have 're-opened' clinically, in fact, had never closed.49 In a recently published RCT, we randomised babies, 24 hours after the first dose, to either continue the full course of 3 doses or to continue the full course only if the ductus was still more than 1.6 mm in diameter on ultrasound prior to the second dose. The latter group received significantly less indomethacin and the eventual closure rate and surgical ligation rate was not significantly different between the two groups.50 Most of the babies with ultrasonically guided treatment duration only needed one dose of indomethacin and there was no difference in side effect or successful PDA closure. This approach has not been tested with Ibuprofen but at RPA, we would consider not giving further doses if there has been significant constriction of the duct apparent on ultrasound 24 hours after the first dose.
Non-responders and Ductal re-opening? There is no clinical trial evidence to guide the management of this problem. There are two clinical situations here; firstly the ductus that closes with the first course and then re-opens and, secondly, the ductus that fails to close with the first course. Unless followed with ultrasound, these two scenarios can appear very similar as the murmur will often disappear and then reappear in both scenarios. The observational studies of this were with indomethacin treatment. In the study of Sangem et al,51 which did not use ultrasound, closure was achieved in 42% of those who received a second course. Keller and Clyman52 did use ultrasound and showed that a second course closed 39% (n=23) of those whose duct had re-opened after ultrasound confirmed closure whereas 0 out of 9, where the duct had never completely closed previously, achieved closure with a second course. Consideration should be using paracetamol in non-responders (see below).
Paracetamol: The interest in paracetamol as a duct closure agent stems from a small observational series from Hammerman et al.57 They made a chance observation of closure of a duct that had been resistant to medical treatment in a baby who had been given paracetamol for other reasons. They tried it on four further babies with resistant PDA and they all closed with a short time frame. Several subsequent observational studies confirmed that paracetamol might be closing PDA
Now clinical trial data is emerging on this. Dang et al58 randomised 160 babies born before 34 weeks to oral ibuprofen vs oral paracetamol in a non-blinded trial. Overall closure rates were similar at 79% vs 81% respectively with less GI bleeding and less jaundice in the paracetamol group. Oncel et al59 randomised 90 babies born before 30 weeks aged 48 to 96 hrs to oral ibuprofen or paracetamol. Closure rates were also similar at 77 vs 72% respectively. Dash et al60 randomised 77 babies <1500g to oral paracetamol or intravenous indomethacin. PDA closure rates were similar (100% vs 95%) with no difference in complications and no evidence of hepatotoxicity from paracetamol.
It is too early to recommend paracetamol as a first line treatment as there has been no placebo control or long term follow up but the above three trials have now randomised 327 babies and are consistent in the findings of similar efficacy to oral ibuprofen and intravenous indomethacin with no difference in side effects. It seems reasonable to consider paracetamol as a second line treatment for babies that have failed to respond to ibuprofen and/or indomethacin.
What dosage for paracetamol? The above trials have all used 15mg/kg 6 hourly in all babies with the course duration of 3 days59,60 and 7 days.58
Medical or surgical closure? The National Collaborative Trial is the only randomised trial to have addressed this issue.23 In this trial, babies randomised to surgical ligation had a higher incidence of pneumothoraces and retinopathy but other outcomes were not different. Cassady et al randomised preterm babies to prophylactic surgical ligation within the first 24 hours. There were no differences in outcomes between the two groups except the babies with prophylactic ligation had a lower incidence of NEC.53 This approach has been considered too invasive to gain any penetration into routine clinical care and there is little evidence to support surgery as first line treatment.
More recently concerns have been raised about duct ligation precipitating a state of cardiac afterload compromise in the early post-operative period. This probably accounts for the cardiorespiratory instability that often occurs for 24-48 hrs after ligation.54,55 There is also observational data showing a range of worse medium and long term outcomes, including neurosensory impairment, in babies that have ligation.56 This is an intervention that we should use judiciously and would usually only consider at RPAH in babies who are ventilator dependent with a clearly haemodynamically significant ductus.
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 15 of 19
Primary Author: A/Prof Nick Evans, November 2015
10. PERFORMANCE MEASURES
NSW NICUS and ANZNN database audit of treatment and complications from preterm patent ductus arteriosus.
11. REFERENCES AND LINKS
4. References and links
1. Chu J, Clements JA, Cotton EK, Klaus MH, Sweet AY, Tooley WH,. Neonatal pulmonary ischemia. Pediatrics 1967;40:709-766.
2. Walther FJ, Benders MJ, Leighton JO. Persistent pulmonary hypertension in premature infants with severe respiratory distress syndrome. Pediatrics 1992;90:899-904.
3. Morales WJ, Angel JL, O'Brien WF, Knuppel RA. Use of ampicillin and corticosteroids in premature rupture of membranes: a randomized study. Obstet Gynecol 1989;73:721-6.
4. Evans N, Archer LNJ. Postnatal circulatory adaptation in healthy term and preterm neonates. Arch Dis Child 1990;65:24-6.
5. Skelton R, Evans N, Smythe J. A blinded comparison of clinical and echocardiographic evaluation of the preterm infant for patent ductus arteriosus. J Paeds Child Health 1994;30:406-11.
6. Davis P, Turner-Gomes S, Cunningham K, Way C, Roberts R, Schmidt B. Precision and accuracy of clinical and radiological signs in premature infants at risk of patent ductus arteriosus. Arch Pediatr Adolesc Med 1995 Oct; 149(10): 1136-41.
7. Evans N, Moorcraft J. Effect of patency of the ductus arteriosus on blood pressure in very preterm infants. Arch Dis Child 1992;67:1169-1173.
8. Kluckow M, Evans N. High pulmonary blood flow, the duct and pulmonary hemorrhage. J Pediatr 2000;137:68-72
9. Evans N. Diagnosis of patent ductus arteriosus in the preterm newborn. Arch Dis Child 1993;68:58-61.
10. Evans NJ, Iyer P. Assessment of ductus arteriosus shunting in preterm infants requiring ventilation: Effect of inter-atrial shunting. Journal of Pediatrics 1994;125:778-785.
11. M El Hajjar, G Vaksmann, T Rakza, G Kongolo, L Storme. Severity of the ductal shunt: a comparison of different markers. Arch Dis Child Fetal Neonatal Ed 2005;90:F419-F422
12. Evans N, Archer LNJ. Postnatal circulatory adaptation in term and healthy preterm newborns. Arch Dis Child1990;65:24-26.
13. Reller MD, Ziegler ML, Rice MJ, Solin RC, McDonald RW. Duration of ductal shunting in healthy preterm infants: An echocardiographic study. J Pediatr 1988:112:441-446.
14. Kluckow M, Evans N. Early echocardiographic prediction of symptomatic patent ductus arteriosus in preterm infants requiring mechanical ventilation. J Pediatr 1995;127:774-779.
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 16 of 19
15. Su BH, Watanabe T, Shimizu M, Yanagisawa M Echocardiographic assessment of patent ductus arteriosus shunt flow pattern in premature infants. Arch Dis Child Fetal Neonatal Ed 1997;77:F36-F40
16. Condo M. Evans N. Bellu R. Kluckow M. Echocardiographic assessment of ductal significance: retrospective comparison of two methods. Archives of Disease in Childhood Fetal & Neonatal Edition. 2012;97(1):F35-8,
17. Kluckow M, Evans N. Low superior vena cava flow and intraventricular haemorrhage in preterm infants. Arch Dis Child 2000;82:F188-F194
18. Evans N, Kluckow M. Early determinants of right and left ventricular outputs in ventilated preterm infants. Arch Dis Child 1996;74:F88-F94.
19. Groves AM. Kuschel CA. Knight DB. Skinner JR. Does retrograde diastolic flow in the descending aorta signify impaired systemic perfusion in preterm infants? Pediatric Research. 2008;63(1):89-94,
20. Benitz WE. Treatment of persistent patent ductus arteriosus in preterm infants: time to accept the null hypothesis? Journal of Perinatology. 2010;30(4):241-52
21. Bose CL. Laughon MM. Patent ductus arteriosus: lack of evidence for common treatments. Archives of Disease in Childhood Fetal & Neonatal Edition. 2007;92(6):F498-502
22. Knight DB. The treatment of patent ductus arteriosus in preterm infants. A review and overview of randomised trials. Seminars in Neonatology 2000;6:63-74
23. Gersony WM, Peckham GJ, Ellison RC, Miettinen OS, Nada AS. Effects of indomethacin in premature infant with patent ductus arteriosus: results of a national collaborative trial. J Pediatr 1983;102:895-906.
24. Cooke L, Steer PA, Woodgate PG. Indomethacin for asymptomatic patent ductus arteriosus in preterm infants. Cochrane Database of Systematic Reviews 2003, Issue 1. Art. No.: CD003745. DOI: 10.1002/14651858.CD003745.
25. Van Overmeire B, Van de Broek H, Van LAer P, Weyler J, Vanbaesebrouck P. Early versus late indomethacin treatment for patent ductus arteriosus in premature babies with respiratory distress syndrome. Journal of Pediatrics 2001;138:205-11
26. Aranda JV. Clyman R. Cox B. Van Overmeire B. Wozniak P. Sosenko I. Carlo WA. Ward RM. Shalwitz R. Baggs G. Seth A. Darko L. A randomized, double-blind, placebo-controlled trial on intravenous ibuprofen L-lysine for the early closure of nonsymptomatic patent ductus arteriosus within 72 hours of birth in extremely low-birth-weight infants. American Journal of Perinatology. 2009; 26(3):235-45
27. Kluckow, Jeffery M, Gill A, Evans N. A randomised placebo-controlled trial of early treatment of the patent ductus arteriosus Arch Dis Child Fetal Neonatal Ed 2014;99:2 F99-F104
28. Fowlie PW, Davis PG, McGuire W. Prophylactic intravenous indomethacin for preventing mortality and morbidity in preterm infants. Cochrane Database of Systematic Reviews 2010, Issue 7. Art. No.: CD000174. DOI: 10.1002/14651858.CD000174.pub2.
29. Edwards AD, Wyatt JS, Richardson C, Potter A, Cope M, Delpy DT, Reynolds EOR. Effects of indomethacin on cerebral haemodynamics in very preterm infants. Lancet 1990;335:1491-5.
30. Colditz P, Murphy D, Rolfe P, Wilkinson AR. Effect of infusion rate of indomethacin on cerebrovascular responses in preterm neonates. Arch Dis Child. 1989; 64: 8-12.
31. Schmidt B. Davis P. Moddemann D. Ohlsson A. Roberts RS. Saigal S. Solimano A. Vincer M. Wright LL. Trial of Indomethacin Prophylaxis in Preterms Investigators. Long-
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 17 of 19
term effects of indomethacin prophylaxis in extremely-low-birth-weight infants. New England Journal of Medicine 2001;344:1966-72
32. Ment LR, Vohr B, Oh W, Scott DT, Allan WC, Westerveld M, Duncan CC; Ehrenkranz RA, Katz KH, Schneider KC, Makuch RW. Neurodevelopmental outcome at 36 months' corrected age of preterm infants in the Multicenter Indomethacin Intraventricular Hemorrhage Prevention Trial. Pediatrics 1996;98: 714-8
33. Ohlsson A, Walia R, Shah SS. Ibuprofen for the treatment of patent ductus arteriosus in preterm and/or low birth weight infants. Cochrane Database of Systematic Reviews 2013, Issue 4. Art. No.: CD003481. DOI: 10.1002/14651858.CD003481.pub5.
34. Van Overmeire B, Follens I, Hartmann S, Creten WL, Van Acker KJ. Treatment of patent ductus arteriosus with Ibuprofen. Arch Dis Child 1997;76:179-84.
35. Varvarigou A, Bardin CL, Beharry K, Chemtob S, Papageorgiou A, Aranda JV. Early Ibuprofen administration to prevent patent ductus arteriosus in premature newborn infants. JAMA 1996;275:539-44
36. Ohlsson A, Walia R, Shah SS. Ibuprofen for the treatment of patent ductus arteriosus in preterm and/or low birth weight infants. Cochrane Database of Systematic Reviews 2010, Issue 4. Art. No.: CD003481. DOI: 10.1002/14651858.CD003481.pub4.
37. Mosca F, Bray M, Lattanzio M, Fumagalli M, Tosetto C. Comparative evaluation of the effects of indomethacin and ibuprofen on cerebral perfusion and oxygenation in preterm infants with patent ductus arteriosus. J Pediatr 1997;131:549-54
38. Gournay V, Savagner C, Thiriez G, Kuster A, Roze JC. Pulmonary hypertension after ibuprofen prophylaxis in very preterm infants. Lancet 2002:359:1486-8
39. De Carolis MP. Bersani I. De Rosa G. Cota F. Romagnoli C. Ibuprofen lysinate and sodium ibuprofen for prophylaxis of patent ductus arteriosus in preterm neonates. Indian Pediatrics. 2012;49(1):47-9
40. Hirt D, Van Overmeire B, Treluyer JM, Langhendries JP, Marguglio A, Eisinger MJ, Schepens P, Urien S. An optimized ibuprofen dosing scheme for preterm neonates with patent ductus arteriosus, based on a population pharmacokinetic and pharmacodynamic study. British Journal of Clinical Pharmacology. 2008; 65(5):629-36
41. Dani C. Vangi V. Bertini G. Pratesi S. Lori I. Favelli F. Ciuti R. Bandinelli A. Martano C. Murru P. Messner H. Schena F. Mosca F. High-dose ibuprofen for patent ductus arteriosus in extremely preterm infants: a randomized controlled study. Clinical Pharmacology & Therapeutics. 2012:91(4):590-6.
42. Gokmen T. Erdeve O. Altug N. Oguz SS. Uras N. Dilmen U. Efficacy and safety of oral versus intravenous ibuprofen in very low birth weight preterm infants with patent ductus arteriosus.
Journal of Pediatrics. 2011;158(4):549-554.e1.
43. Erdeve O. Yurttutan S. Altug N. Ozdemir R. Gokmen T. Dilmen U. Oguz SS. Uras N. Oral versus intravenous ibuprofen for patent ductus arteriosus closure: a randomised controlled trial in extremely low birthweight infants. Archives of Disease in Childhood Fetal & Neonatal Edition. 2012;97(4):F279-83.
44. Hammerman C, Aramburo MJ. Prolonged indomethacin therapy for the prevention of recurrences of patent ductus arteriosus. J Pediatr 1990;117:771-6.
45. Rennie JM, Cooke RWI. Prolonged low dose indomethacin for persistent ductus arteriosus of prematurity. Arch Dis Child 1991;66:55-58.
Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 18 of 19
46. Lee J, Rajadurai VS, Tan KW, Wong KY, Wong EH, Leong JY. Randomized trial of prolonged low-dose versus conventional-dose indomethacin for treating patent ductus arteriosus in very low birth weight infants. Pediatrics 2003;112:345-50
47. Tammela O, Ojala R, Iivainen T et al. Short vs Prolonged indomethacin therapy for patent ductus arteriosus in preterm infants. J Pediatr 1999;134:552-557.
48. Herrera CM, Holberton JR, Davis PG. Prolonged versus short course of indomethacin for the treatment of patent ductus arteriosus in preterm infants. Cochrane Database of Systematic Reviews 2007, Issue 2. Art. No.: CD003480. DOI: 10.1002/14651858.CD003480.pub3.
49. Weiss H. Cooper B. Brook M. Schlueter M. Clyman R. Factors determining reopening of the ductus arteriosus after successful clinical closure with indomethacin Journal of Pediatrics 1995; 127(3):466-71
50. Browning-Carmo K, Evans N, Paradisis M. Duration of Indomethacin Treatment of the Preterm Patent Ductus Arteriosus as Directed by Echocardiography. Journal of Pediatrics 2009;155:819-822
51. Sangem M. Asthana S. Amin S. Multiple courses of indomethacin and neonatal outcomes in premature infants.Pediatric Cardiology. 2008;29(5):878-84
52. Keller RL. Clyman RI. Persistent Doppler flow predicts lack of response to multiple courses of indomethacin in premature infants with recurrent patent ductus arteriosus. Pediatrics. 2003;112(3 Pt 1):583-7
53. Cassady G, Crouse DT, Kirklin JW, Strange MJ, Joiner CH, Godoy G, et al. A randomized, controlled trial of very early prophylactic ligation of the ductus arteriosus in babies who weighed 1000 g or less at birth. New England Journal of Medicine 1989;320:1511-6
54. McNamara PJ. Stewart L. Shivananda SP. Stephens D. Sehgal A. Patent ductus arteriosus ligation is associated with impaired left ventricular systolic performance in premature infants weighing less than 1000 g. Journal of Thoracic & Cardiovascular Surgery. 2010;140(1):150-7
55. Noori S. Friedlich P. Seri I. Wong P. Changes in myocardial function and hemodynamics after ligation of the ductus arteriosus in preterm infants. J Pediatr 2007;150(6):597-602
56. Kabra NS. Schmidt B. Roberts RS. Doyle LW. Papile L. Fanaroff A. Trial of Indomethacin Prophylaxis in Preterms Investigators. Neurosensory impairment after surgical closure of patent ductus arteriosus in extremely low birth weight infants: results from the Trial of Indomethacin Prophylaxis in Preterms. J Pediatr 2007;150(3):229-34, 234.e1
57. Hammerman C. Bin-Nun A. Markovitch E. Schimmel MS. Kaplan M. Fink D. Ductal closure with paracetamol: a surprising new approach to patent ductus arteriosus treatment. Pediatrics. 2011;128(6):e1618-21
58. Dang D, Wang D, Zhang C, Zhou W, Wu H. Comparison of oral paracetamol vs ibuprofen in premature infants with patent ductus arteriosus: A Randomised controlled trial. PLoS ONE 8(11): e77888. doi:10.1371/journal.pone.0077888
59. Oncel MY, Yurttuta S, Erdeve O, et al. Oral paracetamol vs oral ibuprofen in the management of patent ductus arteriosus in preterm infants: A randomised controlled trial. J Pediatr 2014;64:510-4
60. Dash SK, Kabra NS, Avasthi BS, Sharma SR, Padhi P, Ahmed J. Enteral Paracetamol or intravenous indomethacin for closure of patent ductus arteriosus in preterm neonates. Indian Pediatrics 2015;52:573-578

Sydney Local Health District Guideline No: RPAH_GL2016_002 Royal Prince Alfred Hospital Date Issued: January 2016
Compliance with this Guideline is recommended Page 19 of 19
61. Bellini C. Campone F. Serra G. Pulmonary hypertension following L-lysine ibuprofen therapy in a preterm infant with patent ductus arteriosus. CMAJ Canadian Medical Association Journal. 2006;174(13):1843-4,


















