Genitourinary Manifestations of Von Hippel-Lindau Disease
31
Genitourinary Manifestations of Von Hippel - Lindau Disease Alejandro Sanchez, MD
Transcript of Genitourinary Manifestations of Von Hippel-Lindau Disease

Genitourinary Manifestations of Von Hippel-Lindau Disease
Alejandro Sanchez, MD
Presenter
Presentation Notes
20 minutes + 10 minutes of questions Studies to look up Linehan & rickets Cancer Biol 2013 JCO AS cohort from NIH Duffey and Colleagues 2004, 3 cm rule �Joly, 2011 TA for VHL Schuch et al. 2012b �

Disclosures
• None
Presenter
Presentation Notes
Llooked at 2019 talk. Look up Carlo, Eur Urol, 2019. Need more pictures. Talk about risk factors and differences in sporadic RCC. Surgery - enucleation…3 cm rule updated in 2018 (AUA, ball) - low metastatic risk. Tumor growth rates of tumors. Surgical goals -> why preserve kidney function? CKD -> higher risk of CVD, hospitalization, etc. ESRD/transplant survival (Go et al., 2004 NEJM). PN vs RN…Thank you slide with Samantha, Kristen, and... Incidence: Kidney ccRCC 24-70% / cysts 22-59%; Adrenal gland 18%, Epididymis 10-26%

Talk Overview
• Renal masses • Epidemiology• Surveillance• Treatment
• Pheochromocytoma/paraganglioma• Epidemiology• Surveillance• Treatment
• Epididymal / broad ligament cystadenomas
Presenter
Presentation Notes
Llooked at 2019 talk. Look up Carlo, Eur Urol, 2019. Need more pictures. Talk about risk factors and differences in sporadic RCC. Surgery - enucleation…3 cm rule updated in 2018 (AUA, ball) - low metastatic risk. Tumor growth rates of tumors. Surgical goals -> why preserve kidney function? CKD -> higher risk of CVD, hospitalization, etc. ESRD/transplant survival (Go et al., 2004 NEJM). PN vs RN…Thank you slide with Samantha, Kristen, and... Incidence: Kidney ccRCC 24-70% / cysts 22-59%; Adrenal gland 18%, Epididymis 10-26%

What genitourinary organs are affected by VHL?
Presenter
Presentation Notes
Llooked at 2019 talk. Look up Carlo, Eur Urol, 2019. Need more pictures. Talk about risk factors and differences in sporadic RCC. Surgery - enucleation…3 cm rule updated in 2018 (AUA, ball) - low metastatic risk. Tumor growth rates of tumors. Surgical goals -> why preserve kidney function? CKD -> higher risk of CVD, hospitalization, etc. ESRD/transplant survival (Go et al., 2004 NEJM). PN vs RN…Thank you slide with Samantha, Kristen, and... Incidence: Kidney ccRCC 24-70% / cysts 22-59%; Adrenal gland 18%, Epididymis 10-26%

Epidemiology of sporadic renal cancer vs VHL
Sporadic RCC VHL
Siegel RL, et al. CA Cancer J Clin, 2020
• Autosomal Dominant• 1 in 36,0000
Presenter
Presentation Notes
All RCC including TCC 80-85% are renal cancer (most common histology is ccRCC) 8% TCC Rest are benign lesions, sarcoma, wilms tumors, RMC, collecting duct sarcoma

Epidemiology of sporadic renal cancer vs VHL
Ball MW, et al. J Clin Oncol, 2020
Sporadic RCC VHLDemographics
Age at presentation 60-70 yr 40-45 yrSex (M:F) 2:1 1:1Race/ethnicity Lowest among Asian
Americans and Pacific Islanders
Risk factors Obesity, diabetes, hypertension, smoking
Autosomal dominant inheritance
Masses at presentation Unilateral, unifocal Bilateral, multifocal

What is the incidence of VHL in de novo advanced ccRCC?
Carlo Manuscript
Carlo M, et al. JAMA Oncology, 2018
• N=254 patients germline tested• Median age 56 (range 13-79)• 211 (83.1%) Male • 177 (69.7%) with ccRCC• 1 patient with VHL mutation
Presenter
Presentation Notes
10% of those diagnosed do not have any family history

What is the risk of RCC among VHL patients?
Maher ER, et al. Q J Med, 1990Chahoud J, et al. W Journal of Urology, 2020Linehan, Genome Research, 2012
Presenter
Presentation Notes
Overall cysts and RCC occur in about 2/3 of VHL patients, lifetime risk All are ccRCC, can have clear cell papillary (Rao P, et al. Hum Pathol, 2014 and Williamson SR, Am J Surg Pathol, 2013). Symptoms: flank pain, hematuria The mean age at onset in one large series was 44 years and it was estimated that 69 percent of patients surviving to age 60 would develop RCC [Maher ER, et al, 1990].

RCC risk among VHL patients differs by mutation type
• VHL type is broken down by risk of pheochromocytoma:• Type 1: LOW risk of pheochromocytoma• Type 2: HIGH risk of pheochromocytoma
VHL type Pheochromocytoma RCC Hemangioblastomas1A Low High High1B Low Low High2A High Low High2B High High High2C High No No
*
*
*Highest risk of RCC
Presenter
Presentation Notes
Type 1 is low risk of Pheo vs type 2 which is high pheo but variable penetrance of RCC and hemangioblastomas These subclassifications should be used as a guide and are not absolute. Continued surveillance for other VHL-related lesions should continue, for example, in individuals who present with type 2C characteristics

Details of screening for RCC
• Imaging:• Start at age 15 yr• Imaging every 2 years if no tumor found• MRI should be done consecutively with neuroaxis protocol• Can alternate with renal ultrasound if no concerning lesions and MRI concerns• If contraindications present: MRI (+/- contrast) > MRI (w/o contrast) > CT (w/ contrast)
> CT (w/o contrast) > ultrasound (kidneys, adrenals, and pancreas only)
• Physical exam/labs:• Adenopathy, varicocele, stigmata of chronic kidney disease or paraneoplastic
syndromes• Renal function, liver function, LDH, calcium, neutrophil-to-lymphocyte ratio
Chahoud J, et al. W Journal of Urology, 2020
Presenter
Presentation Notes
Low incidence of RCC before 20 yo but can happen RCCs are often multicentric and bilateral, and can arise either in conjunction with cysts or de novo from noncystic renal parenchyma. Although renal cysts may be benign, they are thought to represent a premalignant lesion; solid components within otherwise benign-appearing renal cysts almost always contain RCC Renal manifestations in patients with VHL syndrome histologically range from simple cysts lined by bland, one to two layers of clear cells, atypical cysts with more complex epithelial proliferations, and scattered aggregates of clear cell proliferation in renal parenchyma to ccRCC arising either within cysts or de novo from noncystic renal parenchyma The ccRCCs in VHL patients typically exhibit low nuclear grade and stage, as they are often closely monitored and removed early.

How does surveillance change by mass size?
• Masses < 3 cm -> assess growth kinetics with MRI every 3-6 months for one year
• If ≥ 3 cm recommend nephron-sparing technique at academic center with VHL expertise• Thermal ablative techniques (RFA/Cryo), should be used in patients with small tumors
and high-operative risk
• What about pregnancy/family planning?• Surveillance should be performed before planning conception if possible• MRI without contrast can be done during pregnancy• AS for renal masses < 4 cm is preferred during pregnancy and treatment delayed until
after delivery
Chahoud J, et al. W Journal of Urology, 2020

What are the growth characteristics of renal masses in VHL?
• If growing 2-4 mm (expected) per year -> repeat imaging every 6 months for first year and every year for subsequent two years
• If growing > or equal to 5 mm per year -> imaging every 3-6 months until treated or stable growth rate
• If stable renal mass for 3 years, consider imaging every 2 years
Chahoud J, et al. W Journal of Urology, 2020

Ball MW, et al. J Clin Oncol, 2020
n=286 tumorsn=192 patients
What are the growth characteristics of renal masses in VHL?
Presenter
Presentation Notes
Growth Kinetics of VHL lesions No difference by sex, BMI, baseline size, smoking status, or mutation type or location for mets?

What is the role of renal mass biopsy in VHL?
• Rarely indicated
• Avoid for cystic lesions
• Specific situations:• Prior thermal ablation or suspected
recurrence• Atypical radiographic appearance suggestive
of alternate diagnosis to primary renal malignancy (e.g., inflammation)
• Concurrent or prior extra-renal malignancy that could confound diagnosis
Chahoud J, et al. W Journal of Urology, 2020

VHL ccRCC treatment: “3 cm rule”
Walther MM, et al. J Urol, 1999
Presenter
Presentation Notes
“3-cm rule / guideline” – updated in a more contemporary cohort and noted to confirm These results Solid renal tumors <3 cm in diameter generally have very low metastatic potential and can be safely monitored as long as they remain stable. In one study, for example, serial imaging studies were performed in 96 patients with VHL disease and small renal tumors [37]. Surgery was performed in 52 when a tumor reached a threshold size of 3 cm in diameter. Only two patients required nephrectomy, and none developed metastatic disease at a median follow-up of 60 months. In the other 44 patients, this size threshold was not used as an indication for immediate surgery. In this group, 12 patients required nephrectomy, and 11 developed metastatic disease with a median follow-up of 66 months. **25% will develop metastases

What are the goals of ccRCC treatment in VHL?
• “Reset the clock”
• Minimize the risk of metastases
• Minimize the risk of chronic kidney disease through nephron-sparing techniques
Walther MM, et al. J Urol, 1999
Bindroup MLM, et al. Journal of Medical Genetics, 2017
Presenter
Presentation Notes
Risk of death from RCC has decreased and CNS hemangioblastomas remain the main cause of death for VHL patients Up to 20 tumors resected in the literature w/ preservation of renal fun ction

VHL ccRCC treatment: surgical approach
Open
Russo P and Mano R, Korean J Urol, 2014
Robotic
Presenter
Presentation Notes
MIS vs open: surgeon/center experience matters most Continued close surveillance is required after treatment of RCC in VHL patients. New renal tumors are detected in approximately 30 percent of patients by five years and 85 percent by 10 years. The risk of metastatic disease appears to be low as long as the patient is carefully monitored. Chauveau D, et al. Kid Int, 1996 Genomic analyses of germline VHL-associated tumours have shed light on tumour evolution, and inter- and intrapatient heterogeneity. Aside from the common loss of 3p, intrapatient tumours are clonally independent, showing different molecular trajectories following the VHL/ 3p founding event. Mitchell TJ, et al. Cell, 2018 and Fei SS, et al. Nat Commun 2016.

VHL ccRCC treatment: enucleation vs wide resection
Blackwell RH, et al. Urology, 2017
Standard partial nephrectomy Tumor enucleation
Pseudocapsule Pseudocapsule
Presenter
Presentation Notes
MIS vs open: surgeon/center experience matters most Continued close surveillance is required after treatment of RCC in VHL patients. New renal tumors are detected in approximately 30 percent of patients by five years and 85 percent by 10 years. The risk of metastatic disease appears to be low as long as the patient is carefully monitored. Chauveau D, et al. Kid Int, 1996 Genomic analyses of germline VHL-associated tumours have shed light on tumour evolution, and inter- and intrapatient heterogeneity. Aside from the common loss of 3p, intrapatient tumours are clonally independent, showing different molecular trajectories following the VHL/ 3p founding event. Mitchell TJ, et al. Cell, 2018 and Fei SS, et al. Nat Commun 2016.
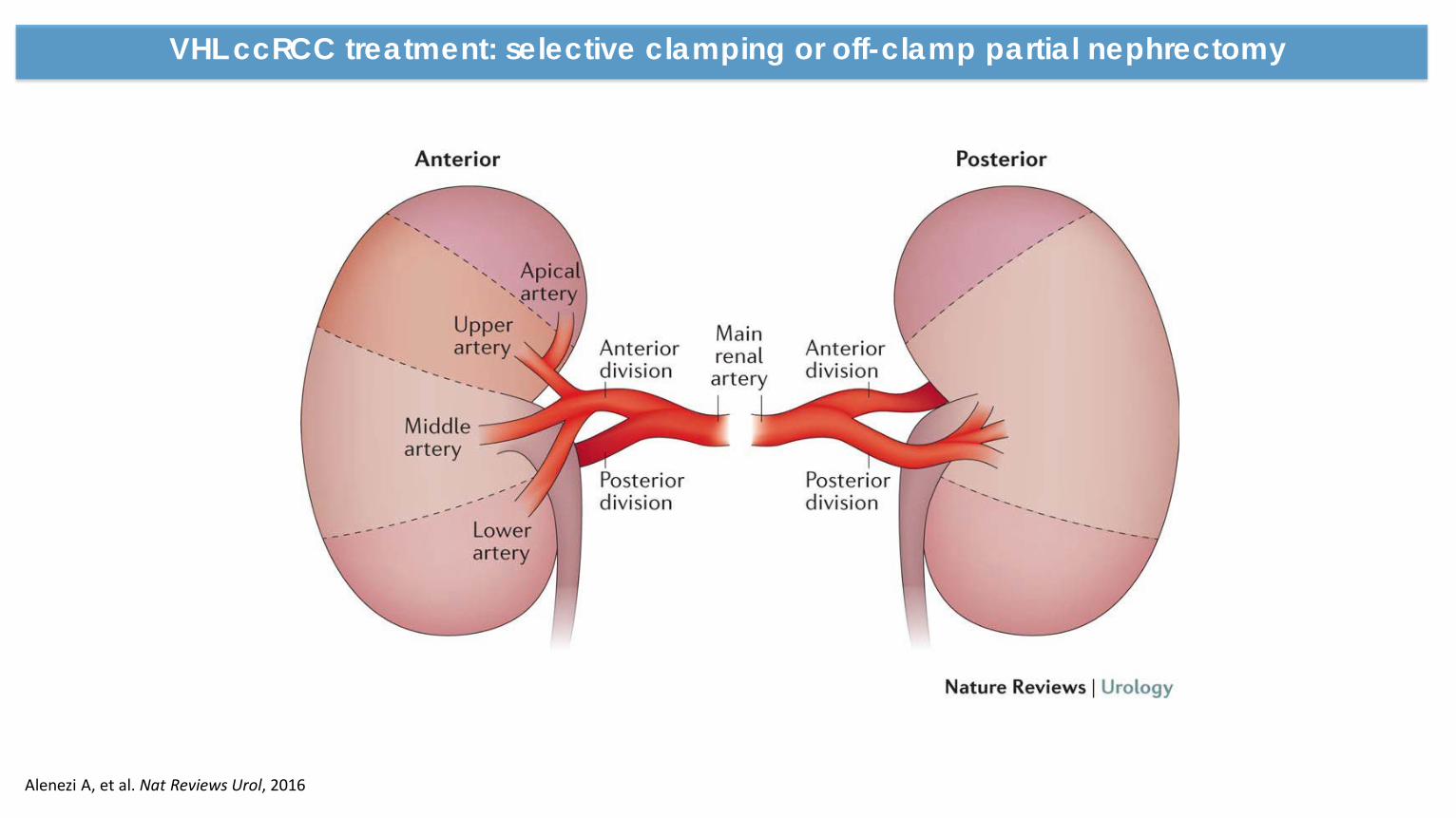
VHL ccRCC treatment: selective clamping or off-clamp partial nephrectomy
Alenezi A, et al. Nat Reviews Urol, 2016

VHL ccRCC treatment: ablation
• Limited VHL-specific data
• Extrapolating from sporadic ccRCC data (usually solitary lesions)
• Size • Location• Risk of local recurrence higher
• Case selection is key
• May complicate subsequent surgeries and possibly affect tumor progression
Shuch B and Linehan, Nat Reviews Urol, 2012
Presenter
Presentation Notes
Small series with short-tern follow-up and renal function data AUA recommends consideration of TA in patients with tumors < 3 cm (T1a), alternative approach to minimize treatment morbidity

VHL ccRCC treatment: renal dysfunction
Lane B, et al. Eur Urol, 2015
• Chronic kidney disease (CKD) is a risk factor for cardiovascular morbidity
• Surgical CKD differs from medical CKD

Important patient counseling regarding management of renal masses
• Urologist should lead the counseling process (+/- nephrology), consider all management strategies, and review the most common and serious urologic and non-urologic morbidities of each treatment pathway
• Provide perspectives on tumor biology, risk assessment including tumor size and imaging characteristics
• Renal function recovery related to diagnosis and management of renal masses
• Referral to nephrology for management of CKD if high risk or GFR is < 45 in patient with pre-existing CKD, or those in whom eGFR < 30 after intervention
Chahoud J, et al. W Journal of Urology, 2020

What are the genitourinary organs affect by VHL?
Presenter
Presentation Notes
Incidence: Kidney ccRCC 24-70% / cysts 22-59%; Adrenal gland 18%, Epididymis 10-26%

What is the pheochromocytoma and paraganglioma?
• Up to 20% can be extra-adrenal (skull base to bladder), aka paragangliomas
Presenter
Presentation Notes
Extra-adrenal 20% skull base to bladder Large pheochromocytomas can become cancer (what %)? Only large, undiagnosed pheos become malignant. Small ones are usually not treated. Not immediate need for treatment. Symptomatic vs asymptomatic. Get an idea of growth. Decide at the right point for treatment.

Pheochromocytomas present in VHL type 2
VHL type Pheochromocytoma RCC Hemangioblastomas2A High Low High2B High High High2C High No No
Presenter
Presentation Notes
Also found in multiple endocrine neoplasia type 2, SDH A, B, C, neurofibromatosis type 1 and other rare conditions. Defines type 2A-C Sporadic pheochromocytoma (no other tumors or family history of disease) – out of 271 tested for VHL, RET, SDHB and SDHD 11% (n=30) had germline mutation. 42% presented at age less than 18 yr. 2 large series NIH (N=64 pts w/ VHL), 106 pheos. 12% outside the adrenal. 35% asymptomatmic w/o evidence of HTN or increased catecholamine production (Walther, J Urol, 1999) Mayo Clinic (n=109 pts w/ VHL), 18% (n=20) had a pheo at median 30 yr and 3 of these were outside the adrenal gland. 1/3 had no catecholamine production. (Baghai M, et al., Arch Surg, 2002)

Pheochromocytoma presentation
• About 1/3 will be symptomatic
• VHL-associated vs sporadic:• Younger age• Often multiple• Can be extra-adrenal• Less likely to be symptomatic
• Symptoms of catecholamine production: hypertension, diaphoresis, tachycardia, and apparent mood changes
Walther, J Urol, 1999Baghai M, et al. Arch Surg, 2002
Presenter
Presentation Notes
Also found in multiple endocrine neoplasia type 2, SDH A, B, C, neurofibromatosis type 1 and other rare conditions. Defines type 2A-C Children may be predominantly have sweating Sporadic pheochromocytoma (no other tumors or family history of disease) – out of 271 tested for VHL, RET, SDHB and SDHD 11% (n=30) had germline mutation. 42% presented at age less than 18 yr. 2 large series NIH (N=64 pts w/ VHL), 106 pheos. 12% outside the adrenal. 35% asymptomatmic w/o evidence of HTN or increased catecholamine production (Walther, J Urol, 1999) Mayo Clinic (n=109 pts w/ VHL), 18% (n=20) had a pheo at median 30 yr and 3 of these were outside the adrenal gland. 1/3 had no catecholamine production. (Baghai M, et al., Arch Surg, 2002)

Pheochromocytoma in VHL: screening
• Radiographic imaging via plasma fractionated metanephrines or 24-hour urine fractionated metanephrines and catecholamines
• Conventional imaging (CT or MRI) is adequate for adrenal lesions
• Conventional imaging is not adequate for extra-adrenal lesions, consider:• Iobenguane I-123 scan• Whole body MRI• FDG or 68-Ga Dotatate PET CTs
Neumann HPH, et al. NEJM, 2019
Presenter
Presentation Notes
Conventional imaging may not be sufficient because of the potential for extra-adrenal lesions, referred to as paragangliomas. Studies with 18F-DOPA PET provide some context and suggest that iobenguane (also known as metaiodobenzylguanidine [MIBG]) scanning is not effective at detecting pheochromocytomas in patients with VHL: ●A pilot study of 18F-DOPA PET in seven patients with VHL indicated a high detection rate (7 out of 7), as did computed tomography (CT) scan. On the other hand [(123/131)I]-MIBG scintigraphy failed to detect 4 of the 7 lesions [50]. ●These data were confirmed in an independent study of 48 patients with hereditary and nonhereditary cases [51]. ●In a prospective study assessing adrenal imaging of 52 patients with VHL disease, 390 lesions were identified by CT (n = 139), magnetic resonance imaging (MRI; n = 117), 18F-FDG PET (n = 94), and 18F-DOPA PET (n = 40). 18F-DOPA PET identified 20 pancreatic and 20 extrapancreatic tumors, including lesions in the adrenal gland (n = 11), kidney (n = 3), liver (n = 4), lung (n = 1), and cervical paraganglioma (n = 1). These tumor sites were not seen by conventional imaging studies in 9.6 percent of patients and 4.4 percent of lesions [52]. ●In a prospective study of 197 patients with VHL-associated pancreatic lesions, clinical and imaging characteristics were analyzed to study the associations between 18F-FDG PET uptake, tumor growth, and the development of metastatic disease [53]. PET imaging detected metastatic disease in three patients in whom it was not detected by CT scan and suggested non-neoplastic disease in three more patients. Measurement of plasma metanephrines and normetanephrines provides important diagnostic information. In a study of patients with VHL disease and multiple endocrine neoplasia type 2 (MEN-2), measurements of plasma normetanephrines and metanephrines provided a sensitivity of 97 percent and a specificity of 96 percent [49]. A high normetanephrine to metanephrine ratio is expected because patients with VHL disease almost exclusively produce normetanephrines (indicating norepinephrine production).

Pheochromocytoma in VHL: management
• Symptomatic pheochromocytomas should be surgically removed
• Partial adrenalectomy if possible (minimize the risk of adrenal insufficiency)
• Alpha-adrenergic blockade and other supportive measures needed

What are the genitourinary organs affect by VHL?
Glasker S, et al. OncoTargets and Therapy, 2020Zanotelli D, et al. Archives of Gynecology and Obstetrics, 2010

CONCLUSIONS
• Surveillance and early detection is key
• Treatment of genitourinary manifestations in VHL requires a multidisciplinary approach
• Organ-preservation is key in the management of renal and adrenal masses

Thank you
VHL and High-Risk Renal Cancer Clinic Team







![Von Hippel Lindau Disease [VHL]: Magnetic Resonance Imaging ...](https://static.fdocuments.net/doc/165x107/587759fb1a28ab13448b6a8e/von-hippel-lindau-disease-vhl-magnetic-resonance-imaging-.jpg)