X-linked myotubular myopathy in Rottweiler dogs is caused by a ...

Am. J. Hum. Genet. 57:120-126, 199S
Genetic Linkage Heterogeneity in Myotubular MyopathyF. Samson,' L. Mesnard,' M. Heimburger,' A. Hanauer72 M. Chevallay,6 J. J. Mercadier,'J. F. Pelissier,3 N. Feingold,4 C. Junien,5 J.-L. Mandel,2 and M. Fardeau6
'CNRS URA 1159, Le Plessis Robinson; 2INSERM U184, Strasbourg; 3Hopital de la Timone, Marseille; and 4INSERM U155, 5U73, and 6UI53, Paris
Summary
Myotubular myopathy is a severe congenital disease in-herited as an X-linked trait (MTM1; McKusick 31040).It has been mapped to the long arm of chromosome X,to the Xq27-28 region. Significant linkage has subse-quently been established for the linkage group com-prised of DXS304, DXS15, DXS52, and F8C in severalstudies. To date, published linkage studies have pro-vided no evidence of genetic heterogeneity in severe neo-natal myotubular myopathy (XLMTM). We have inves-tigated a family with typical XLMTM in which no link-age to these markers was found. Our findings stronglysuggest genetic heterogeneity in myotubular myopathyand indicate that great care should be taken when usingXq28 markers in linkage studies for prenatal diagnosisand genetic counseling.
Introduction
Severe neonatal myotubular myopathy (XLMTM;McKusick 31040), first described by Van Wijngaarden(Van Wijngaarden et al. 1969) and Barth (Barth et al.1975), is a congenital disease usually inherited as an X-linked trait. This condition, which was originally called"myotubular" myopathy because of the striking resem-blance between affected muscle fibers and fetal myo-tubes, only affects males and is most often lethal. Prena-tal onset, attested to by polyhydramnios and reducedfetal movements, occurs in nearly all cases. Clinical fea-tures include severe generalized hypotonia and muscleweakness associated with respiratory failure. Character-istic histopathological features include the presence of acentral area devoid of myofibrils and centrally posi-tioned nuclei in most muscle fibers, a situation similarto that seen in primitive embryonic myotubes involvingboth type I and II muscle fibers.Myotubular myopathy appears to be a distinct disease
entity differing from centronuclear myopathies, despite
Received March 16, 1994; accepted for publication April 7, 1995.Address for correspondence and reprints: Dr. Franqoise Samson,
CNRS URA 1159, H6pital Marie Lannelongue, 133 Avenue de laResistance, F92350 Le Plessis Robinson, France.© 1995 by The American Society of Human Genetics. All rights reserved.0002-9297/95/5701-0015$02.00
initial confusion. Some studies have suggested that, un-like centronuclear myopathies, this disorder results froman arrest in the normal development of muscle fibers(Sarnat 1990; Sawchak et al. 1991). In addition, theabnormal persistence of a fetal myosin isoform observedin the severe neonatal X-linked form of the disease (Saw-chak et al. 1991; Soussi-Yanicostas et al. 1991) does notoccur in centronuclear myopathies.Myotubular myopathy is a rare disease, and sibships
are usually small, mainly owing to neonatal lethality.Linkage analysis has only been performed in 12 familiesbut has provided evidence of linkage between XLMTMand four markers (loci DXS52, DXS134, DXS15, andF8C) located within the Xq28 region (Thomas et al.1987, 1990; Darnfors et al. 1990; Lehesjoki et al. 1990;Starr et al. 1990; Liechti-Gallati et al. 1991). This locushas been designated MTM1. On the basis of a singlerecombination between the disease gene and these mark-ers in a XLMTM family and on the absence of recombi-nation with DXS304 in the same meiotic event (Lehes-joki et al. 1990), the following order of loci has beensuggested: cen-DXS42-DXS105-(DXS304, MTM1)-(DXS52, DXS134, DXS15, F8C)-tel. More recently,the MTM1 gene has been mapped to a 600-kb intervalin a region flanked by DXS1113 and DXS305 (Dahl etal. 1995). The use of these Xq28 markers for prenataldiagnosis of XLMTM has been advocated. However, aslightly different histochemical pattern has been ob-served in a few families with neonates affected by an X-linked myotubular myopathy, raising the possibility ofgenetic heterogeneity. In these families, virtually all typeI fibers are affected, whereas only a minority of type IIfibers show the characteristic features of myotubularmyopathy (Engel et al. 1968). However, the coexistenceof cases with and without selective fiber I atrophy withina given family (Zimmerman and Weber 1979) madesuch heterogeneity unlikely. The possibility of twoXLMTM alleles on chromosome X has also been raisedby Barth et al. (1975), given the varied severity of thedisease.We report on the first family with typical XLMTM
in which the disease is not genetically linked to Xq28markers. We examined 28 markers on the X chromo-some and carried out linkage analysis of 11 markersof the Xq27-q28 region: DXS105, DXS98, DXS548,FRAXAC2, DXS296, DXS1113, DXS304 (U6.2 and
120

Samson et al.: X-Linked Myotubular Myopathy
U6.2-20E), DXS305, DXS52, and F8C. We observedmultiple recombination events between the disease locusand six informative markers located in Xq27-q28. Thesefindings suggest that locus heterogeneity is a potentialsource of error in prenatal diagnosis based on Xq28markers.
Subjects, Material, and Methods
Family ZThe proband, a male born after 35 wk of gestation
with severe hypotonia, was admitted to a neonatal inten-sive care unit because of respiratory failure and died at29 d of age. Gestation was complicated by polyhydram-nios, and the mother noticed a reduction in fetal move-ments toward the end of the pregnancy. Diagnosis ofXLMTM was based on characteristic abnormalitiesfound on muscle biopsy. Light and electron microscopyshowed that most of the muscle fibers were much smallerthan those of control age-matched infants; muscle nu-clei were located in the central position, and there wasa central area devoid of myofibrils (figs. 1 and 2). Histo-chemical staining for oxidative enzymes showed a sub-sarcolemmal ring devoid of enzyme activity, sur-rounding a central zone of high activity (not shown).Apparently healthy female members of the family under-went muscle biopsy, and four were found to have severalsmall fibers with centrally located nuclei scatteredamong normal fibers (fig. 3). A muscle biopsy of thefather was normal.
DNA AnalysisAll individuals except the proband were sampled
twice to check the haplotypes. DNA extracted fromleukocytes was completely digested with restrictionenzymes in the conditions recommended by the manu-facturer (Biolabs). A total of 11 DNA markers locatedin the Xq27-q28 region, including eight RFLPs andthree microsatellites, were studied (table 1). An addi-tional 17 RFLP markers spanning the long and shortarms of chromosome X were also studied (table 2).For RFLP analysis, 15 jig of DNA was electropho-resed in 0.8% agarose gel and transferred to Hybondmembranes (Amersham) by Southern blotting. Geno-typing of the family with the VNTR probe DXYS20was performed in hybridization conditions describedelsewhere (Page et al. 1987). The DNA probes werelabeled using a[32P]-dCTP (3000 Ci/mmol) (Amer-sham) and the Klenow random labeling kit (Boeh-ringer) to a specific activity of 109 counts per min/jg. Hybridization was carried out at 650C for 3 h inAmersham Rapid Hybridization Buffer. The mem-branes were washed three times in 2 x SSC (SSC is0.15 M NaCl + 1.5 X 10'2 M sodium citrate), andonce in 2 X SSC, 0.1% SDS at 600 C for 10 min, then
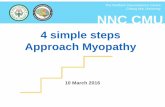
Figure I Cryostat sections of muscle biopsies, stained for myo-fibrillar ATPase after acid preincubation (pH 4.35) x 320. a, CaseII16, numerous small rounded fibers, with a central area devoid ofactivity, corresponding to nuclei or internuclear spaces (myotube-likefibers). b, Normal control on a 6-wk-old child. Note the absence ofmyotubular aspect, normal mosaic pattern of the different muscularfiber types, and presence of some TIc muscle fibers.
rinsed briefly in 2 x SSC and exposed to x-ray film(Cronex, Dupont) with intensifying screens for 2 d at-70°C. Because of its histological similarities withXLMTM and the possibility of complete lack of pene-trance in some individuals carrying the myotonic dys-trophy gene, congenital myotonic dystrophy (CMyD)had to be ruled out by means other than histologicalstudies (i.e., DNA analysis); this was especially im-portant in our XLMTM family with no apparent link-age to the Xq28 region. DNA analysis of the CTGrepeat which is abnormally expanded in myotonicdystrophy (MD) (Brook et al. 1992) was done by us-ing a Southern blot of BglI-digested genomic DNAfrom four unrelated neonates with the congenitalform of myotonic dystrophy, and from three unre-lated neonates with XLMTM, including the propos-itus of the family studied here. The blot was hybrid-
121

Am. J. Hum. Genet. 57:120-126, 199S
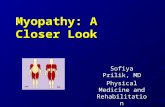
Figure 2 Electron micrograph of case III6. Round muscle fiber with centrally located nucleus. The central part of the fiber is devoid ofmyofibrils but contains collection of mitochondria and glycogen, x 7,000.
ized with a (CTG)7 oligonucleotide labeled with T4polynucleotide kinase using y[32P]-ATP (6000 Ci!mmol). Membranes were washed in 4 x SSC at roomtemperature three times for 15 min, then in 1 x SSCat 500C for 20 min, and exposed to x-ray film over-night.Length polymorphism of the microsatellites
DXS548, FRAXAC2, and DXS1113 was typed bymeans of PCR, using reaction conditions and a step-cycle file described elsewhere (Oudet et al. 1993; We-ber et al. 1993). Five microliters of each reaction mixwas added to 15 gl of formamide-loading buffer.
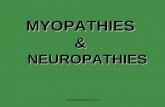
Figure 3 Muscle histology of case 115 (healthy female carrier).Hematin-Eosine staining, x 160. Several atrophic fibers (arrows),some with central nuclei, are scattered among normal fibers.
After denaturation at 90'C for 2 min, 2 g1 of eachreaction mix was subjected to electrophoresis in a 6%polyacrylamide denaturing (7 M urea) gel, and thegel was submitted to autoradiography.
Linkage AnalysisThe MLINK subprogram of the LINKAGE software
package (Lathrop et al. 1984) was used for two-pointanalysis. Allele frequencies of published DNA markerswere used in the analyses. Since no published data onthe frequency of the disease allele were available, it wasestimated by comparing the frequency of XLMTM inour laboratory and that of other neonatal neuromuscu-lar disorders in which the gene frequency is known (spi-nal muscular atrophy and the congenital form of myo-tonic dystrophy). Assumptions used in the linkage analy-ses were a recessive X-linked mode of inheritance with80% penetrance in females typed by muscle biopsy anda frequency of the disease allele of .00001.
Results
The family pedigree is shown in figure 4. Six of the11 markers studied in Xq27-q28 were informative. Mul-tiple crossovers involving these markers were detected(fig. 4). In particular, the affected male had the samehaplotype as his unaffected brother and grandfather.This virtually ruled out a disease locus in the Xq27-q28 region. The family was therefore screened with 17additional RFLPs distributed elsewhere throughout theX chromosome. The results are summarized in table 2.
122

123Samson et al.: X-Linked Myotubular Myopathy
Table I
DNA Markers Covering the Region Xq22-q28 of the X Chromosome Studied in Family Z
Map Location Locus Symbol Probe Enzyme Reference
Xq27.1-q27.2 ........... DXS 105 cX55.7 TaqI Williamson et al. 1991Xq27.2 .............. DXS 98 4D8 MspI Williamson et al. 1991Xq27.3 .............. DXS 548 CA repeat Riggins et al. 1992Xq27.3 .............. FRAXAC2 CA repeat Richards et al. 1991Xq27.3-q28 .............. DXS 296 VK21C MspI Williamson et al. 1991Xq28 .............. DXS 1113 CA repeat Weber et al. 1993
Xq28 DXS 304 U6.2 TaqI Williamson et al. 1991U6.2-20E BanHI Williamson et al. 1991
Xq28 .............. DXS 305 St35-691 TaqI Williamson et al. 1991Xq28 .............. DXS 52 St14-1 TaqL/BclI Williamson et al. 1991Xq28 .............. F8C F814 BclI Williamson et al. 1991
Recombinations were seen with 8 markers, excludingfour additional regions for linkage (Xp22.1-p21.1;Xpl1.3; Xq2l.3-q22; Xq26.2-q26.3). Probable recom-binants were observed with two other markers. Theother seven markers were uninformative.No inconsistencies with any of the 17 informative mark-
ers were detected within the family, even with the highlypolymorphic probes St14 and DXYS20, strongly sug-gesting that false paternities and/or sample mix-up couldnot explain these results. To rule out errors, the familywas resampled. The genotypes in the second DNA analysis
Table 2
DNA Markers Spanning the X Chromosome,with the Exception of the Xq27-28 Region
Locus Lod Score atMap Location Symbol Probe 0 = .00
Xp22.3 .............. DXS 143 Dic 56 NIXp22.3-p22.2 ........... DXS 9 RC8 NIXp22.1 .............. DXS 41 p99-6 -2.776Xp21.2 .............. DXS 164 pERT 87-8 -2.769Xp21.2 .............. DXS 164 pERT 87-15 -0.085Xp2l.2-p21.1 ........... DXS 206 XJ2-3 -2.769Xp21.1 .............. DXS 84 L 754 -2.769Xpll.3 .............. DXS 7 L1-28 -2.772Xql2-ql3 .............. DXS 159 cpX 73 NIXql3-q21 .............. DXYS 1 pdP 231 NIXq2l.3-q22 .............. DXS 3 p 19-2 -6.029Xq2l.3-q22 .............. DXS 17 S 21 -2.605Xq22 .............. DXS 94 pXG 12 NIXq24-q26 .............. DXS 11 p22-33 NIXq26 .............. DXS 107 cpX234 NIXq26 .............. DXS 144 C11 -1.085Xq26.2-q26.3 ........... DXS 51 52 A -5.967
NOTE.-Characteristics of probes and RFLPs are indicated in Wil-liamson et al (1991). NI = probe not informative.
confirmed our initial results. Finally, to exclude the slightpossibility of misdiagnosis of a neonatal form of myotonicdystrophy, Southern blot DNA studies of the CTG repeatabnormally expanded in myotonic dystrophy were per-formed: while varying degrees of allelic expansion rangingfrom 5 kb to 6.5 kb (up to 2,166 repeats) were detectedin all four CMyD cases studied, no expansion was detected
XcenDXS105DXS98FRAXAC2DXS1113DXS305DXS52F8C
Xtel
12
1 123 1 1
3 2 3
1 2 2
7 5 4
1 2 2
12 2 1 2
12 2 1 2
31 2 3 1
33 2 3 3
12 1 1 2
7 6 7 7 4
12 2 1 2
~~45 7 91
2 2 1 2 I.~1 2 ~1 2 1 1 2 1
3 1 .3 3 2 3
23 3 2 3 3 2 3
2 2 I.~ 1 I. 1 1 1
5S 5 7*- 7 7 7 7 7
2 2 *1 1 2 1
III
22113133126422
Figure 4 Informative loci in family Z. The vertical ar-rangement of alleles indicates the most likely haplotype. The paternalhaplotype is indicated on the left for the females. Genotypes formarkers DXS105, DXS98, FRAXAC2, DXS1113, DXS305, DXS52,and F8C are indicated for each individual from top to bottom in thelocus order Xq27 to Xq28. Alleles are numbered under each subjectstudied. Arrows indicate recombinations between the disease locusand the markers. Brackets indicate localization of recombinationevents between markers in individual II1 and II3. % indicates deadand affected male. ( indicates carrier ascertained by muscle biopsy.® indicates an obligate carrier female. * indicates spontaneousmiscarriage without determination of sex.

Am. J. Hum. Genet. 57:120-126, 199S
CMyD XLMTM
1 2 3 4 5 6 7
9 kb .,.
8.2kb
Figure 5 Detection of the CTG expansion usin:nucleotide to probe several digests of genomic DNAlated newborns with severe congenital myotonic dys4), and from three unrelated newborns with myotu(XLMTM) (lanes 5-7). While varying degrees of;ranging from 5 kb to 6.5 kb are detected in CMy]was detected in the three XLMTM probands, incluc(case III6) of family Z (lane 5). The variation of the-100 bp (2.5-2.6 kb, using Bg1I digests), correspormum amplification of -33 repeats.
in the XLMTM probands, including that of t
reported here (fig. 5).
Discussion
The gene responsible for XLMTM wa
the Xq27-28 region in a previous geneticfamilies, and the peak two-point LOD sco
recombination fraction of 0 = .00 was athe DXS15 locus (Thomas et al. 1987, 1
evidence of linkage between the disease locMTM1 and the Xq28 markers DXS52,F8C has been reported by several laboratoof 10 additional families (Darnfors et al. 19et al. 1990; Starr et al. 1990; Liechti-GallatNo evidence of genetic heterogeneity has I
these families.We report the first XLMTM family in wh
conflict with previous linkage data. This foclinical and histological criteria for XLMTMnotypically indistinguishable from theXLMTM families. In this family, recombinalin several "phase-known" meioses. The r
events indicated in figure 4 rule out a disease ISince this family was initially uninformative ipedigree structure itself, female carriers weremeans of muscle biopsies, as previously rep(
et al. 1984; Oldfors et al. 1989). Specimens from the fourfemales (111, 113, 115, and III4) showed characteristic abnor-malities, namely, several small muscle fibers scatteredamong normal fibers (fig. 3). These females were thereforedesignated as carriers. Given the X-linked inheritance ofthe disease and the fact that virtually all affected males die
7.4kb in the neonatal period, grandmother I2 was designatedas an obligate carrier, although muscle biopsy was notperformed, since, unfortunately, nonspecific abnormalitiesare often observed on muscle biopsy of older individuals.The first evidence of absence of linkage to the Xq28 regioncame from the haplotype of markers from DXS98 to F8Cin the affected and unaffected brothers (1116 and 119),which were the same and corresponded to that inherited
2.6 kb from the grandfather (Il) without recombination. On the~-2.5 kb basis of minimum recombination events, it is particularly
striking that recombinations with six informative probesg a (CTG)7 oligo- occurred in the meioses giving rise to individuals I114 andfrom four unre- M6. We can rule out that a single recombination telomerictrophy (lanes 1- to F8C could render this family consistent with the otherbular myopathy ones. In fact, the XLMTM gene has been recently mappedallelic expansion to a 600-kb interval in proximal Xq28, in a region flankedD) no expansion by DXS1113 and DXS305 (Dahl et al. 1995), almost 10ngormal allele is cM proximal to F8C. This locus was designated MTM1.
nding to a maxi- To be consistent with this localization of the XLMTMgene, one would have to assume both germinal mosaicismin I1 and a double recombination in the intervalFRAXAC2-DXS305 (<10 cM), which is very unlikely
Lhe new family (probability being estimated very conservatively at 1/10 formosaicism x 1/100 for double recombination, equivalent toa lod score of -3). No recombination between DXS1 113 (amicrosatellite very close to the IDS gene) and the XLMTMlocus was detected in the two "phase-known" meioses
s assigned to available from generation II of this pedigree, but DXS1 113study of two was uninformative for the meioses giving rise to individuals)re of 3.7 at a 1114 and 1116. Recent results indicate that the MTM1 locus)btained with lies between DXS304 and DXS305, just distal to IDS/990). Further DXS1113 (Dahl et al. 1994).:us designated Grandmother 12 was not formally proved to be aDXS15, and carrier by means of muscle biopsy abnormalities butries in a total was nonetheless designated an obligate carrier. Since90; Lehesjoki the affected male had the same haplotype as histi et al. 1991). healthy grandfather, we initially raised the possibilitybeen found in of grandparental germ-line mosaicism to explain the
discrepancy between our results and those of previousich the results studies. Cases of germ-line mosaicism, based on theamily met the possibility of transmission by a phenotypically normaland was phe- grandfather, have been identified in several X-linkedXq28-linked diseases, including Duchenne muscular dystrophy
tions occurred (Bakker et al. 1987), ornithine transcarbamylase defi-recombination ciency (Maddalena et al. 1988), and Wiskott-Aldrichlocus in Xq28. syndrome (Arveiler et al. 1990). In the latter disease,in terms of the this phenomenon was shown to simulate genetic heter-e identified by ogeneity. However, DNA analysis of a healthy brotherorted (Ambler recently born to this family (III9), allowed us to rule
124

Samson et al.: X-Linked Myotubular Myopathy 125
out this hypothesis, since this normal boy had thesame haplotype as his maternal grandfather.
Because of histological similarities betweenXLMTM and congenital myotonic dystrophy, and thepossibility of complete lack of penetrance in someindividuals carrying the myotonic dystrophy gene, weinvestigated the unlikely possibility that the linkageheterogeneity demonstrated here was due to misdiag-nosis. This was ruled out by the absence of the CTGexpansion that occurs in myotonic dystrophy (Brooket al. 1992).
Given the pedigree structure and the existence of threeclinically asymptomatic carrier sisters, the mode of in-heritance in this family is likely to be X-linked recessive.Cases of severe centronuclear myopathies with prenatalonset, thus showing clinical similarities with XLMTM,have been described (Torres et al. 1985). However, inthis family in which two male neonates were severelyaffected, the mother had clinical manifestations sug-gesting autosomal dominant inheritance, which was notthe case in our family. Furthermore, in the family re-ported by Torres et al. (1985) there is a possibility thatthe mother was in fact a symptomatic carrier ofXLMTM. Although autosomal recessive inheritance hasbeen suggested in centronuclear myopathies, it has notbeen convincingly demonstrated. If the mode of inheri-tance is indeed X-linked recessive in this family, severalregions of the X chromosome that have not been ex-cluded because of the lack of informativeness of RFLPmarkers remain candidates for this new myotubular my-opathy locus. This warrants analysis of microsatellitemarkers in these regions. However, the maximum lodscore expected from this family (taking into accountresults of muscle biopsy in females) is <2 and will thusfall short of significance.
In conclusion, the results of this study stronglypoint to genetic heterogeneity in myotubular myopa-thies. The mapping of the disease locus in the Xq28-unlinked family is of importance for genetic counsel-ing, prenatal diagnosis, gene isolation, and the etiol-ogy of myotubular myopathy. This lack of linkage tothe Xq28 region emphasizes that great care is re-quired in prenatal diagnosis based on linkage analy-sis. Indeed, since neither clinical nor histological cri-teria can help to discriminate between genetic typesof myotubular myopathies, our findings suggest thatprenatal diagnosis should only be offered when Xq28marker linkage has been demonstrated in the individ-ual family. Our data further indicate that myotubularmyopathy may result from mutations at two differentloci on the X chromosome. Since a lod score of >3cannot be generated by this family, additional Xq28-unlinked families need to be identified to locate thisnew locus for myotubular myopathy.
AcknowledgmentsWe are very grateful to the family members who allowed
us to take blood and muscle samples. We also thank Dr. D.Hillaire (Genethon) for her assistance in DNA banking andC. Oudet for help in microsatellite typing. Funding was pro-vided by a Research Fellowship from the Association Franqaisecontre les Myopathies (F.S.), a grant from the AssociationFrancaise contre les Myopathies (F.S. and J.J.M.), and by theCentre National de la Recherche Scientifique).
ReferencesAmbler MW, Neave C, Tutschka BG, Pueschel SM, OrsonJM, Singer DB (1984) X-linked recessive myotubular myop-athy. I. Clinical and pathologic findings in a family. HumPathol 15:566-574
Arveiler B, de Saint-Basile G, Fischer A, Griscelli C, MandelJL (1990) Germ-line mosaicism simulates genetic heteroge-neity in Wiskott-Aldrich syndrome. Am J Hum Genet46:906-911
Bakker E, Van Broeckhoven C, Bonten EJ, Van de VoorenMJ, Van Hull W, Van Ommen GJB (1987) Germline mosa-icism and Duchenne muscular dystrophy mutations. Nature329:554-556
Barth PG, Van Wijngaarden GK, Bethlem J (1975) X-linkedmyotubular myopathy with fatal neonatal asphyxia. Neu-rology 25:531-536
Brook JD, McCurrach ME, Harley HG, Buckler AJ, ChurchD, Aburatani H, Hunter K, et al (1992) Molecular basis ofmyotonic dystrophy: expansion of a trinucleotide (CTG)repeat at the 3' end of a transcript encoding a protein kinasefamily member. Cell. 68:799-808
Dahl N, Hu LJ, Chery M, Fardeau M, Gilgenkrantz S, Ni-velon-Chevalier A, Sidaner-Noisette I, et al (1995) Myotu-bular myopathy in a girl with a deletion at Xq27-q28 andunbalanced X inactivation assigns the MTM1 gene to a 600-kb region. Am J Hum Genet 56:1108-1115
Dahl N, Samson F, Thomas NST, Hu LJ, Gong W, HermanG, Laporte J, et al (1994) X-linked myotubular myopathyMTM1 mapped between DXS304 and DXS305 closelylinked to the DXS455 VNTR and a new, highly informativemicrosatellite marker (DXS1684). J Med Genet 31:922-924
Darnfors C, Larsson HEB, Oldfors A, Kyllerman M, Gus-tavson KH, Bjursell G, WahlstromJ (1990) X-linked myotu-bular myopathy: a linkage study. Clin Genet 37:335-340
Engel KW, Gold GN, Karpati G (1968) Type I fiber hypotro-phy and central nuclei: a rare congenital muscle abnormalitywith a possible experimental model. Arch Neurol 18:435-444
Lathrop GM, Lalouel JM, Julier C, Ott J (1984) Strategies formultilocus linkage analysis in humans. Proc Natl Acad SciUSA 81:3443-3446
Lehesjoki AE, Sankila EM, Miao J, Somer M, Salonen R,Rapola J, de la Chapelle A (1990) X-linked neonatal myotu-bular myopathy: one recombination detected with fourpolymorphic DNA markers from Xq28. J Med Genet27:288-291
Liechti-Gallati S, Moller B, Grimm T, Kress W, Moller C,

126 Am. J. Hum. Genet. 57:120-126, 1995
Boltshauser E, Moser H, et al (1991) X-linked centronuclearmyopathy: mapping the gene to Xq28. Neuromuscul Disord1:239-245
Maddalena A, Sosnoski DM, Berry GT, Nussbaum RL (1988)Mosaicism for an intragenic deletion in a boy with mildornithine transcarbamylase deficiency. New Engl J Med319:999-1003
Oldfors A, Kyllerman M, Wahlstrom J, Darnfors C, Henriks-son KG (1989) X-linked myotubular myopathy: clinical andpathological findings in a family. Clin Genet 36:5-14
Oudet C, Mornet E, Serre JL, Thomas F, Lentes-Zengerlin S,Kretz C, Deluchat C, et al (1993) Linkage disequilibriumbetween the fragile X mutation and two closely linked CArepeats suggests that fragile X chromosome are derived froma small number of founder chromosomes. Am J Med Genet52:297-304
Page DC, Bieker K, Brown LG, Hinton S, Leppert M, LalouelJM, Lathrop M, et al (1987) Linkage, physical mappingand DNA sequence analysis of pseudoautosomal loci on thehuman X and Y chromosomes. Genomics 1:243-256
Richards RI, Holman K, Kremer E, Lynch M, Pritchard M,Yu S, Mulley J, et al (1991) Fragile X syndrome: geneticlocalisation by linkage mapping of two microsatellite re-peats FRAXAC1 and FRAXAC2 which immediately flankthe fragile site. J Med Genet 28:818-823
Riggins GJ, Sherman SL, Oostra BA, Sutcliffe JS, Feitell D,Nelson D, Van Oost BA, et al (1992) Characterization of ahighly polymorphic dinucleotide repeat 150 kb proximal tothe fragile X site. Am J Med Genet 43:237-243
Sarnat HB (1990) Myotubular myopathy: arrest of morpho-genesis of myofibres associated with persistence of fetal vi-mentin and desmin: four cases compared with fetal andneonatal muscle. Can J Neurol Sci 17:109-123
Sawchak JA, Sher JH, Norman MG, Kula RW, Shafiq SA
(1991) Centronuclear myopathy heterogeneity: distinctionof clinical types by myosin isoform patterns. Neurology41:135-140
Soussi-Yanicostas N, Chevallay M, Lurent-Winter C, TomeFMS, Fardeau M, Butler-Browne GS (1991) Distinct con-tractile protein profile in congenital myotonic dystrophy andX-linked myotubular myopathy. Neuromuscul Disord1:103-111
Starr J, Lamont M, Iselius L, Harvey J, Heckmatt J (1990) Alinkage study of a large pedigree with X-linked centronu-clear myopathy. J Med Genet 27:281-283
Thomas NST, Sarfarazi M, Roberts K, William H, Cole G,Liechti-Gallati S, Harper PS (1987) X-linked myotubularmyopathy (XLMTM): evidence for linkage to Xq28 DNAmarkers. Cytogenet Cell Genet 46:314
Thomas NST, Williams H, Cole G, Roberts K, Clarke A,Liechti-Gallati S, Braga S, et al (1990) X-linked neonatalcentronuclear/myotubular myopathy: evidence for linkageto Xq28 DNA marker loci. J Med Genet 27:284-287
Torres CF, Griggs RC, Goetz JP (1985) Severe neonatalcentronuclear myopathy with autosomal dominant inheri-tance. Arch Neurol 42:1011-1014
Van Wijngaarden GK, Fleury P, Bethlem J, Meijer H (1969)Familial "myotubular" myopathy. Neurology 19:901-908
Weber C, Oudet C, Johnson S, Pilia G, Schlessinger D, Ha-nauer A (1993) Dinucleotide repeat polymorphism close toIDS gene in Xq27.3-q28 (DXS1 113). Hum Mol Genet 2:612
Williamson R, Bowcock A, Kidd K, Pearson P, Schmidtke J,Ceverha P, Chipperfield M, et al (1991) Report of the DNAcommittee and catalogues of cloned and mapped genes,markers formatted for PCR and DNA polymorphisms. Cy-togenet Cell Genet 58:1190-1832
Zimmerman P, Weber U (1979) Familial centronuclear myop-athy: a haploid DNA disease. Acta Neuropathol (Berl)46:209-214