
General physiology - Blood
141
BLOOD PHYSIOLOGY Dr.Lara Owies
-
Upload
hamzeh-albattikhi -
Category
Education
-
view
243 -
download
5
Transcript of General physiology - Blood
BLOOD PHYSIOLOGY
Dr.Lara Owies
• Plasma volume• Blood volume• plasma composition & function• blood composition & cell count• White blood cell types & function• Platelets count & function• Hemostasis, mechanism &
disorders
Lecture Outline
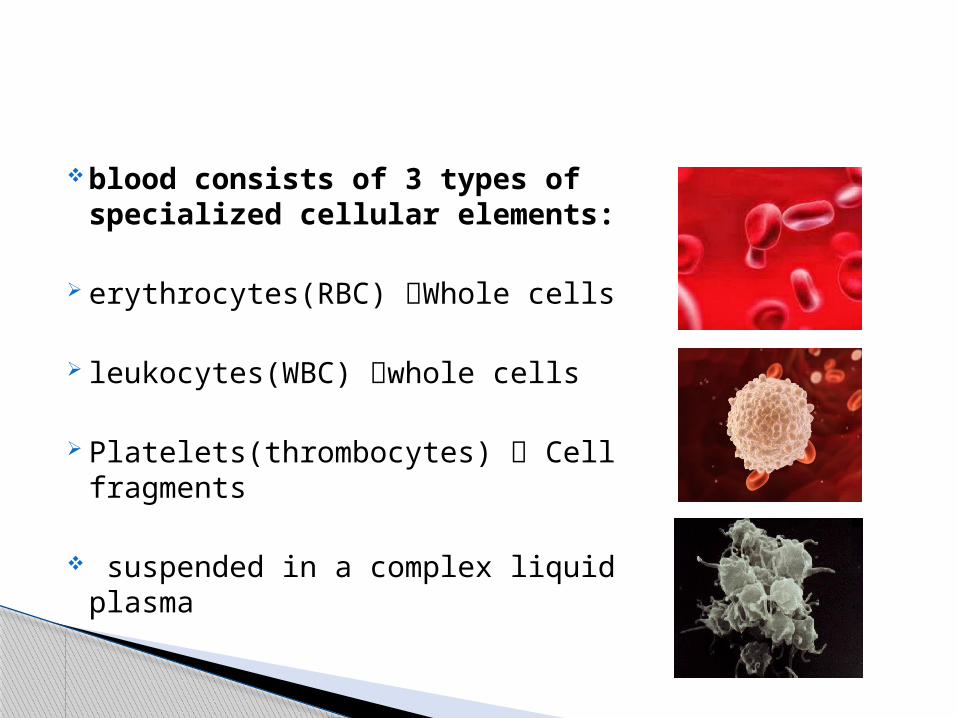
blood consists of 3 types of specialized cellular elements:
erythrocytes(RBC) Whole cells
leukocytes(WBC) whole cells
Platelets(thrombocytes) Cell fragments
suspended in a complex liquid plasma

Blood Volume & Plasma Volume
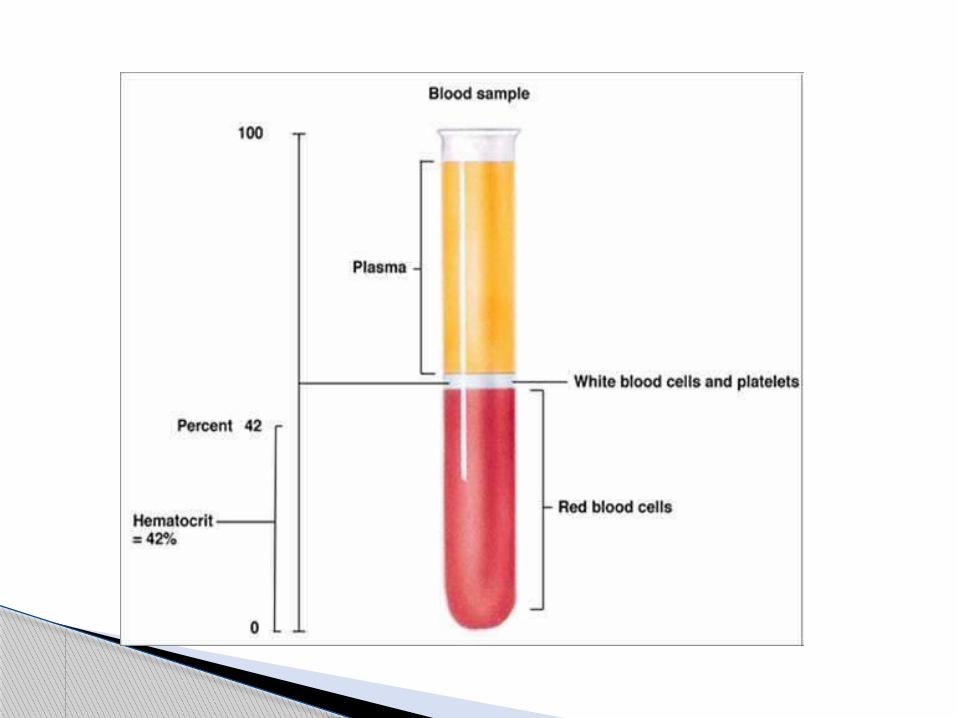

packed cell volume(PCV):
the fraction of the blood composed of red blood cellsdetermined by centrifuging
men=0.40
women=0.36
severe anemia= 0.10
Polycythemia= 0.65
Hematocrit

Measuring plasma volume:
serum albumin labeled with radioactive iodine (125I-albumin).
Evans blue dye (T-1824)
Measurements

Measuring blood volume
Total blood volume
Example:
Plasma volume=3 liters, hematocrit =0.40
= 5 liters
Measurements

Measuring blood volume
Another way: inject into the circulation red blood cells that have been labeled with radioactive chromium (51Cr).
Measurments

The average blood volume of adults is about 7% of body weight , or about 5 liters.
60 % :plasma
40% :RBC’S
these percentages differ, depending on gender, weight, and other factors.
Blood & plasma Volume

Plasma Composition & Function

3 liters.
the noncellular part of the blood
it exchanges substances continuously with the interstitial fluid through the pores of the capillary membranes.
These pores are highly permeable to all solutes except proteins
Blood plasma
Composition:
contains large amounts of sodium and chloride ions, reasonably large amounts of bicarbonate ions.
but only small quantities of potassium,calcium, magnesium, phosphate, and organic acid ions.
The composition of plasma is regulated by the kidneys.
Blood Plasma

The largest portion of the blood
90% water.
Water is a medium for materials being carried in the blood , & can absorb and distribute heat
Blood Plasma

Inorganic constituants :
1% of plasma weight
Most abundant ions in plasma Na⁺,Cl⁻
HCO₃⁻,K⁺, Ca⁺² in smaller amounts
They function in:
membrane excitability
osmotic distribution of fluid between Extracelluar fluid and cells
buffering of pH changes.
Blood Plasma

Organic constituants:
plasma protiens(6-8% of plasma weight)
Nutrients : glucose , Amino Acids, Lipids ,Vitamins.
waste products: creatinin, bilirubin , urea
Dissolved gases O2,CO2
Hormones
Blood Plasma

Plasma protiens functions
maintain plasma volume
Partially responsible for buffering pH .
Bind substances that poorly dissolve in plasma ( thyroid hormone , cholesterol , iron)
Blood clotting factors are plasma protiens
Inactive circulating precursor molcules (ex:angiotensinogenangiotensin).
Gamma globulins are immunoglobulins (antibodies)which are crucial to body defence mechanism.
Blood Plasma

Blood composition & cell count

Erythrocytes(RBC’s)
Function:
transport hemoglobin, which in turn carries oxygen
contain carbonic anhydrase, Acid-Base buffer( by hemoglobin)
Red Blood Cells

biconcave discs
diameter of about 7.8 micrometers and a thickness of 2.5 micrometers at the thickest point and 1 micrometer or less in the center.
The average volume of the red blood cell is 90 to 95 cubic micrometers.
The shapes of red blood cells can change remarkably as the cells squeeze through capillaries.
Red Blood Cells

Concentration of Red Blood Cells in the Blood.
In normal men, per cubic millimeter is 5,200,000 (±300,000)
in normal women 4,700,000 (±300,000).
Persons living at high altitudes have greater numbers of red blood cells.
Quantity of Hemoglobin in the Cells.
Red blood cells have the ability to concentrate hemoglobin in the cell fluid up to about 34 grams in each 100 milliliters of cells.
Red Blood Cells

In men :15 grams of hemoglobin per 100 milliliters of cells In women: 14 grams per 100 milliliters.
each gram of pure hemoglobin can combine 1.34 milliliters of oxygen.
In normal man, 20 milliliters of oxygen can be carried in
combination with hemoglobin in each 100 milliliters of blood.
in normal woman, 19 milliliters of oxygen can be carried.
Hemogobin
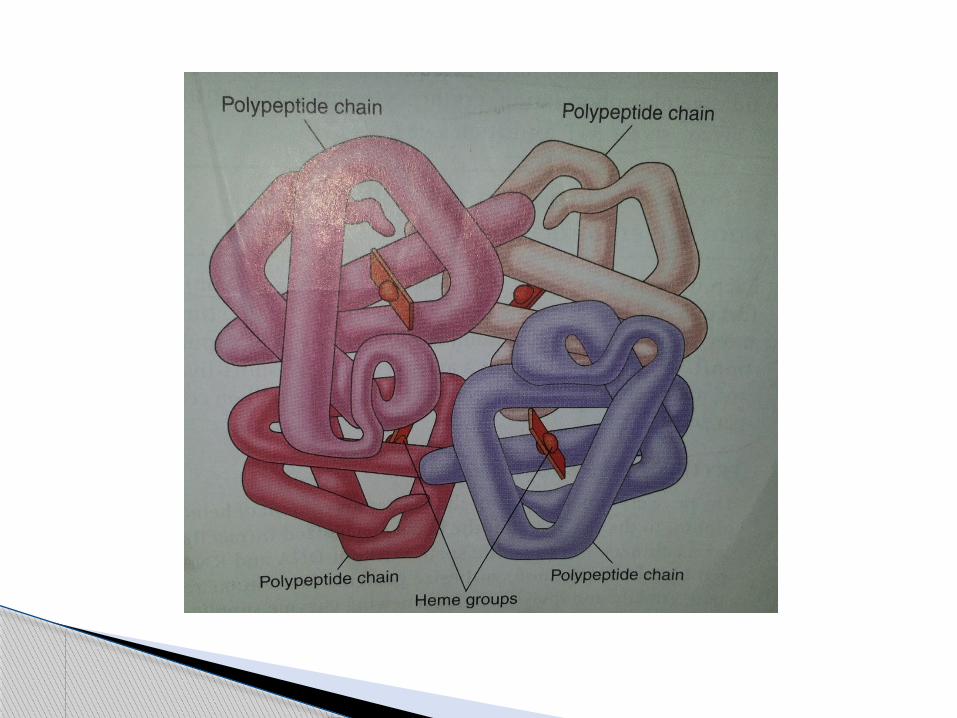
.each of the four iron atoms can combine reversibly with one molecule of O2
Each hemoglobin molecule can pick up 4 O2 passengers in the lungs.
98.5% of the O2 is carried in the blood is bound to hemoglobin
Due to iron, hemoglobin is a pigment
O2 binds loosely to iron atoms so that the combination is easily reversible
Hemoglobin
Each hemoglobin molecule contain 4 hemoglobin chains :Alpha , beta, gama , delta chains.
In adults: hemoglobin A ; 2 alpha and 2 beta chains
Sickle cell anemia results from abnormalities in 2 beta chains of hemoglobin
Hemoglobin
Transport and storage of iron
Iron in plasma : transferrin
Iron inside cell cytoplasm: ferritin (storage iron)
Small quantities as insolube hemosederin
Iron
Transferrin delivers iron to erythroblast cells in bone marrow to form hemoglobin
Low transferrin in blood failure to transport iron to the erythroblasts severe hypochromic anemia
Hypochromic anemia: red cells that contain much less hemoglobin than normal
Iron

When red blood cells are destroyed, the hemoglobin released from the cells is ingested by monocyte-macrophage cells.
There, iron is liberated and is stored mainly in the ferritin pool to be used as needed for the formation of new hemoglobin.
Iron

Life span and destruction of RBC’s
circulate for 120 days before being destroyed
do not have a nucleus ,mitochondria, or endoplasmic reticulum
they do have cytoplasmic enzymes that are capable of metabolizing glucose and forming small amounts of ATP.
Red Blood Cells

Life span and destruction of RBC’S
Red cells are destructed in the spleen
the hemoglobin is phagocytized by macrophages:
especially by the Kupffer cells (liver) macrophages of the spleen and bone marrow.
Iron and bilirubin are released into the blood
Red Blood Cels
deficiency of hemoglobin in the blood , which can be caused by too few RBC’s
1. Blood Loss Anemia.
2. Microcytic Hypochromic Anemia
3. Aplastic Anemia.
4. Megaloblastic anemia.
anemia
5. Hemolytic anemia (hereditary)
hereditary spherocytosis
sickle cell anemia
West African and American blacks, sickle cell disease “crisis”
*Anemia


erythroblastosis fetalis Rh-positive red blood cells in the fetus are attacked by antibodies from an Rh-negative mother
effects of anemia:1. greatly increased cardiac output2. increased pumping workload on the heart.
Anemia

1. Secondary polycythemia causes:
too little oxygen in the breathed air (highaltitudes)
failure of oxygen delivery to the tissues ( in cardiac failure) ex: Physiologic polycythemia
polycythemia

2. Polycythemia vera ( erythremia)
Genetic
The blast cells no longer stop producing red cells when too many cells are already present
Hematocrit & total blood volume increase
Cyanotic (bluish )skin
*Polycythemia

White Blood Cell Types & Function
The mobile units of the body’s protective system
Formed in: Bone Marrow lymph tissue
After formation, they are transported in the blood to different parts of the body where they are needed.
White Blood Cells

Types of White Blood Cells.
Polymorphonuclear granulocytes(granular appearance & multiple nuclei):
1. neutrophils2. eosinophils3. basophils
Mononuclear agranulocytes
1. monocytes 2. lymphocytes3. plasma cells
Characteristics of WBC’s

Granulocytes & monocytes protect the body by phagocytosis
The lymphocytes and plasma cells function mainly in connection with the immune system.
Characteristics of WBC’s
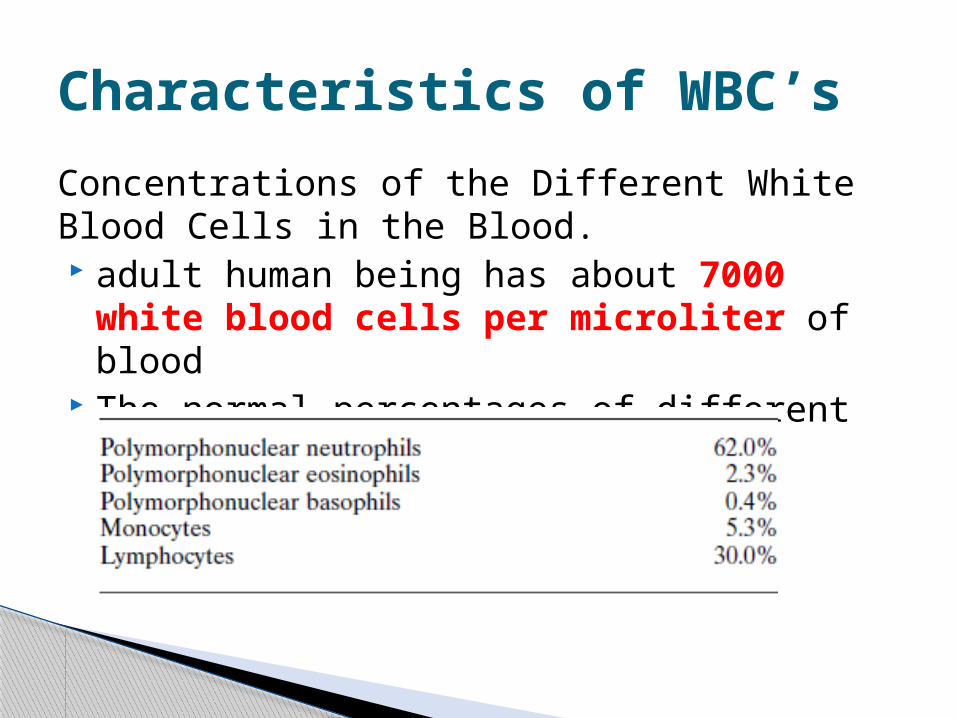
Concentrations of the Different White Blood Cells in the Blood. adult human being has about 7000 white
blood cells per microliter of blood The normal percentages of different WBC’s
Characteristics of WBC’s

granulocytes: normally 4 to 8 hours circulating in the
blood and another 4 to 5 days in tissues In times of serious tissue infection,this total
life span is often shortened to only a few hours because the granulocytes are destroyed.
Life Span of the White Blood Cells
The monocytes 10 to20 hours in the blood
Then ,through the capillary membranes into the tissues.
Once in the tissues , they become tissue macrophages
tissue macrophages can live for months unless destroyed while performing phagocytic functions.
Life Span of the White Blood Cells

Lymphocytes life spans of weeks or months
enter the circulatory system continually ,from the lymph nodes and other lymphoid tissue.
After a few hours, they pass out of the blood back into the tissues by diapedesis.
Later, they re-enter the lymph and return to the blood again and again
Life Span of the White Blood Cells
It is mainly the neutrophils and tissue macrophages that attack and destroy invading microorganisms
The neutrophils
mature cells
attack and destroy bacteria even in the circulating blood.
Neutrophils and Macrophages
Monocyte-tissue macrophages
Monocytes immature cells while still in the blood and have little ability to fight
infectious agents at that time.
tissue macrophages
begin life as blood monocytes
They enter the tissues
They swell to a size that can barely be seen with the naked eye.
extremely capable of combating intratissue disease agents
Neutrophils and Macrophages
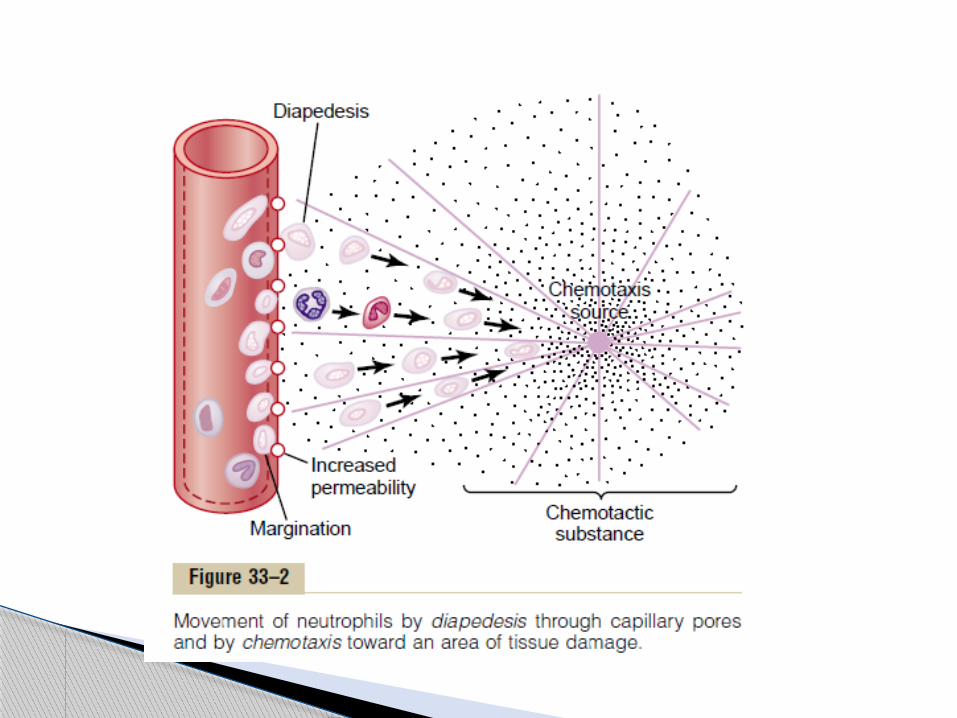
Neutrophils and monocytes can squeeze through the pores of the blood capillaries by diapedesis
Both neutrophils and macrophages can move through the tissues by ameboid motion,
Chemotaxis:chemical substances in the tissues cause both neutrophils and macrophages to move toward the source of the chemical .
Neutrophils and Macrophages

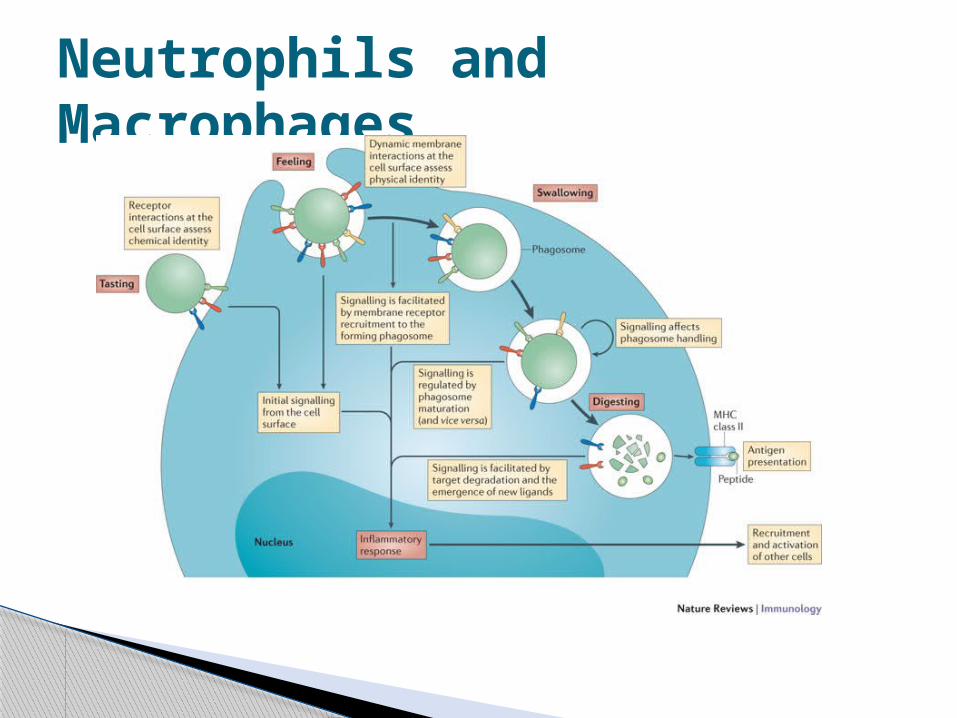
neutrophils and macrophages main function is phagocytosis
1. Antibodies adhere to bacterial membrane to make it susceptible to phagocytosis
2. the antibody combine with C3 . C3 molecules, in turn, attach to receptors on the phagocyte membrane.
This selection and phagocytosis processis called opsonization.
Neutrophils and Macrophages
Neutrophils and Macrophages
single neutrophil can usually phagocytize 3 to 20 bacteria
neutrophils are not capable of phagocytizing particles much larger than bacteria
Neutrophils and Macrophages
Macrophages
more powerful phagocytes than neutrophils
phagocytizing as many as 100 bacteria.
They also have the ability to engulf much larger particles (red blood cells ,malarial parasites)
Neutrophils and Macrophages
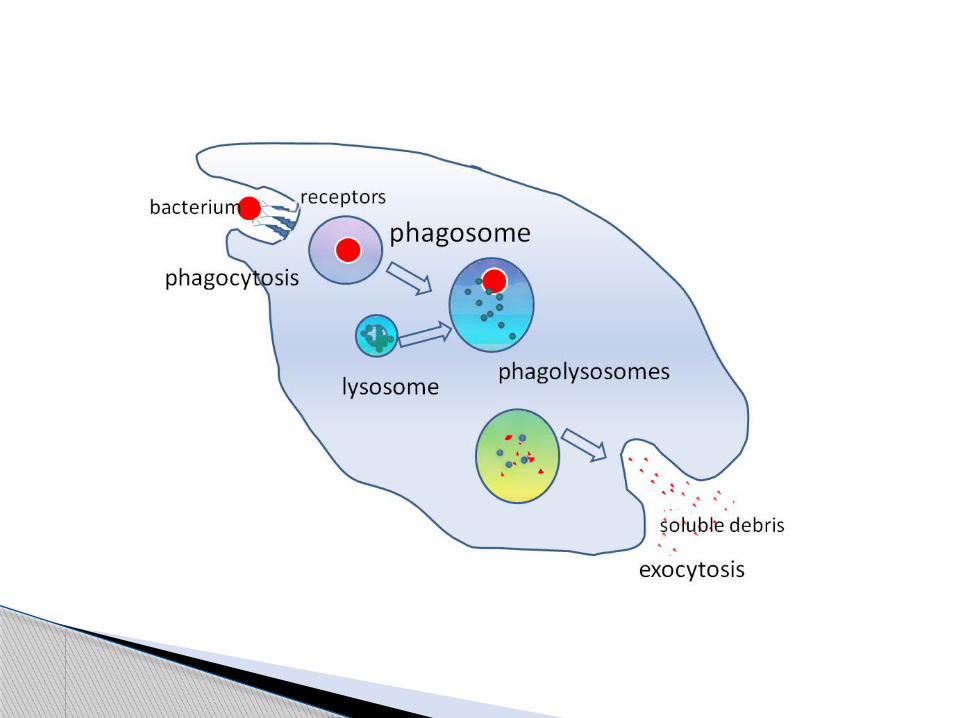

The phagocytic vesicle fuse with lysosomes and other granules and create digestive vesicle
Neutrophils and macrophages:
1. proteolytic enzymes
2. lipases
3. oxidizing agents
Neutrophils and Macrophages

Composed of :
Monocytes
mobile macrophages
fixed macrophages
Monocyte-macrophage system
Tissue Macrophages:
the Skin and Subcutaneous Tissues (Histiocytes)
Macrophages in the Lymph Nodes
Alveolar macrophages in the lungs
Kupffer cells in the liver
Macrophages of the Spleen and Bone Marrow
Microglia in the brain
Monocyte-Macrophage System
Defense lines
a First Line of Defense : Tissue Macrophage.Within minutes begin their phagocytic actions
Second Line of Defense : Neutrophil Invasion of the Inflamed Area Is a within a few hours
Neutrophilia: acute increase in the number of neutrophisthe number of neutrophils in the blood sometimes increases from a normal of (4000 to 5000) 15,000 to 25,000 )neutrophils per microliter
Neutrophils and Macrophages

Defense lines
Third Line of Defense : Second Macrophage Invasion into the Inflamed Tissue.
Fourth Line of Defense : Increased Production of Granulocytes and Monocytes by the Bone Marrow Is
It takes 3-4 days for the new granulocytes & monocytes to leave the bone marrow
Neutrophils and Macrophages
Pus: cavity is often excavated in the inflamed tissues that contains varying portions of necrotic tissue, dead neutrophils, dead macrophages, and tissue fluid
Neutrophils and Macrophages
2% of all the blood leukocytes
weak phagocytes,
parasitic infections.
eosinophils


release substances as: 1. hydrolytic enzymes
2. highly reactive forms of oxygen
3. major basic protein
eosinophils
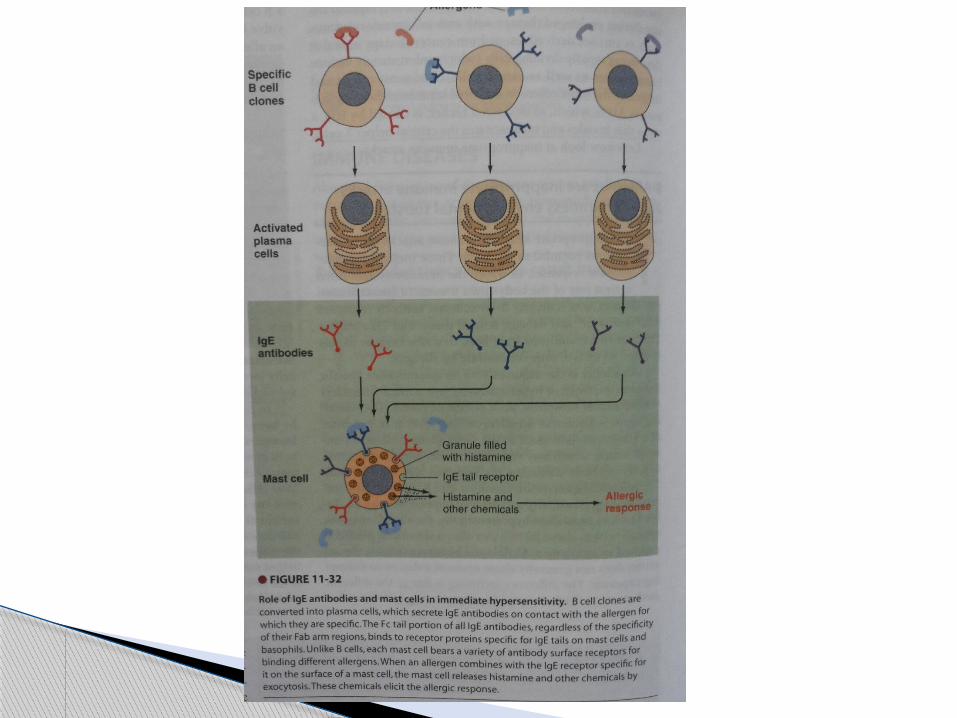
In allergic reactions:
1. detoxify some of the inflammation-inducing substances released by the mast cells and basophils and probably
2. phagocytize and destroy allergen-antibody complexes
thus preventing excess spread of the local inflammatory process.
eosinophils
Basophils In the blood
basophils are similar to tissue mast cells
mast cells and basophils release:
1. heparin
2. Histamine
3. bradykinin
Basophils & mast cells

They play an important role allergic reactions
Basophils & mast cells

Release of
1. histamine, 2. bradykinin, 3. serotonin, 4. heparin,5. slow-reacting substance of anaphylaxis6. lysosomal enzymes
Low WBC’s production
Without treatment, death often ensues in less than a week after acute total leukopenia begins.
Leukopenia
Causes of aplasia of the bone marrow Irradiation of the body by x-rays or gamma
rays
drugs and chemicals that contain benzene
chloramphenicol (an antibiotic), thiouracil (used to treat thyrotoxicosis), and even various barbiturate hypnotics, on very rare occasions cause leukopenia
Leukopenia
Uncontrolled production of white blood cells
can be caused by cancerous mutation of
1. myelogenous cells
2. lymphogenous cells.
leukemia
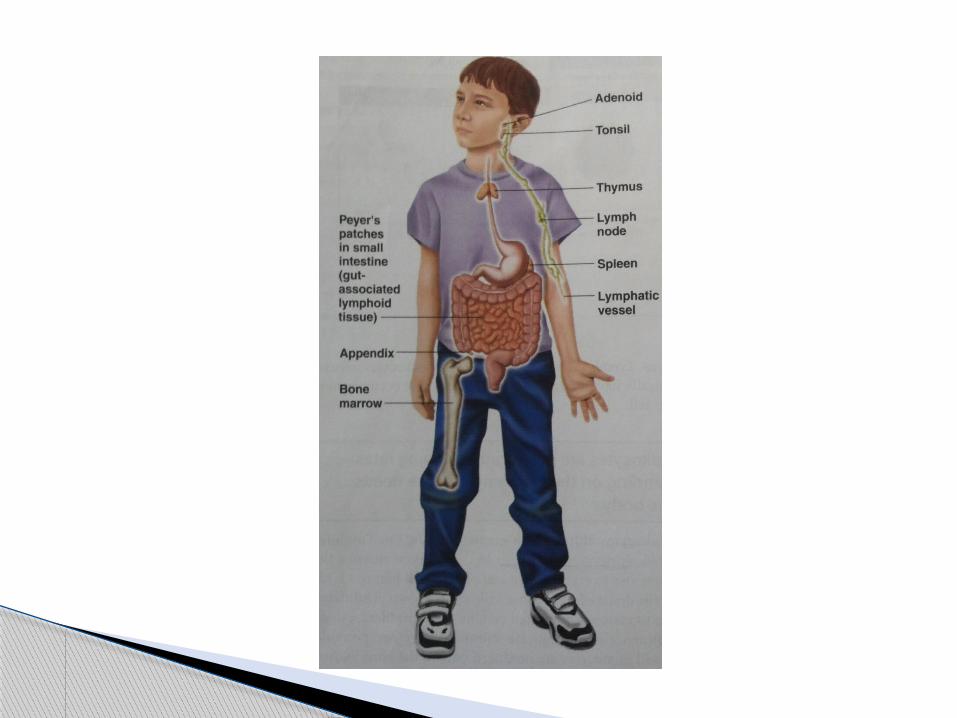
Blood cells that are concerned with acquired immunity
Present in lymph nodes and other lymphoid tissues
Acquired immunity: the formation of antibody and/or activation of lymphocytes that attack and destroy the specific invading organism or toxin.
LYMPHOCYTES

Types of Acquired Immunity:
1. Humoral (B-cell ) immunity: B lymphocytes produce antibodies.
2. Cell mediated (T-cell) immunity: formation of activated T-lymphocyte that are specifically crafted in L.N to destroy the foreign agent
Lymphocytes
Both types are initiated by antigen
Antigen: is a large molecule with a special epitope ( protein /polysaccharide ) on its surface to be recognized
It starts When the invading antigen reaches the lymphoid tissue (lymph nodes, spleen, thymus …)
lymphocytes

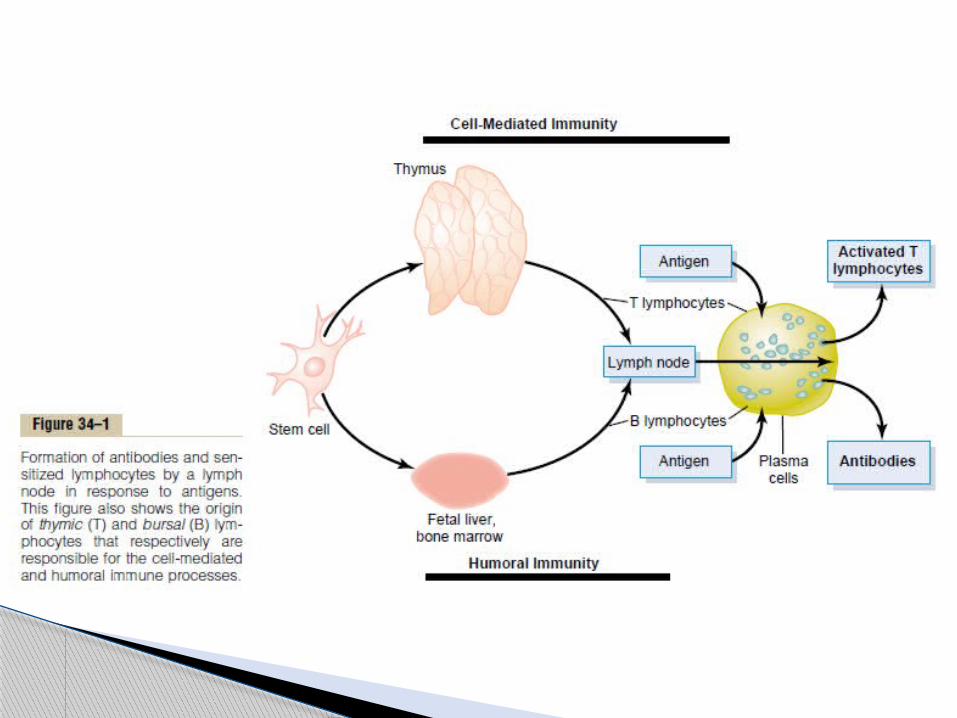
derived originally in the embryo from pluripotent hematopoietic stem cells
Lymphocytes that migrate and differentiate in the thymus form T-lymphocyte
Lymphocytes that differentiate in the fetal liver and bone marrow form B-lymhocytes
After differentiation , B,T lymphocytes migrate to lymphoid tissues throughout the body
Lymphocytes

B-lymphocytes remain dormant in lymphoid tissue
Macrophages phagocytize the antigen and present it to T& B-lymphocytes
T-helper cells activate B-lymphocytes
B-lymphocytes enlarge and differentiate to form plasma cells
Mature plasma cells produce gamma gobulin antibodies
Antibodies are secreted into the blood
Lymhocytes

IgM, IgG, IgA, IgD, and IgE.
Ig stands for immunoglobulin
75% of Ig’s of a normal person are IgG
IgE involved in allergy
Classes of antibodies

T-lymphocytes types and function:
T-helper cells:
most numerous T-cells,
major regulator of all immune functions by forming lymphokines (interleukins, interferon …)
in the abscense of T-helper cells the immune system is paralyzed
Lymphocytes


T-helper cells functions:
1. Stimulation of Growth and Proliferation of Cytotoxic T Cells and Suppressor T Cells
2. Stimulation of B-Cell Growth and Differentiation to Form Plasma Cells and Antibodies.
3. Activation of the Macrophage System.
4. Feedback Stimulatory Effect on the Helper Cells Themselves.
Lymphocytes

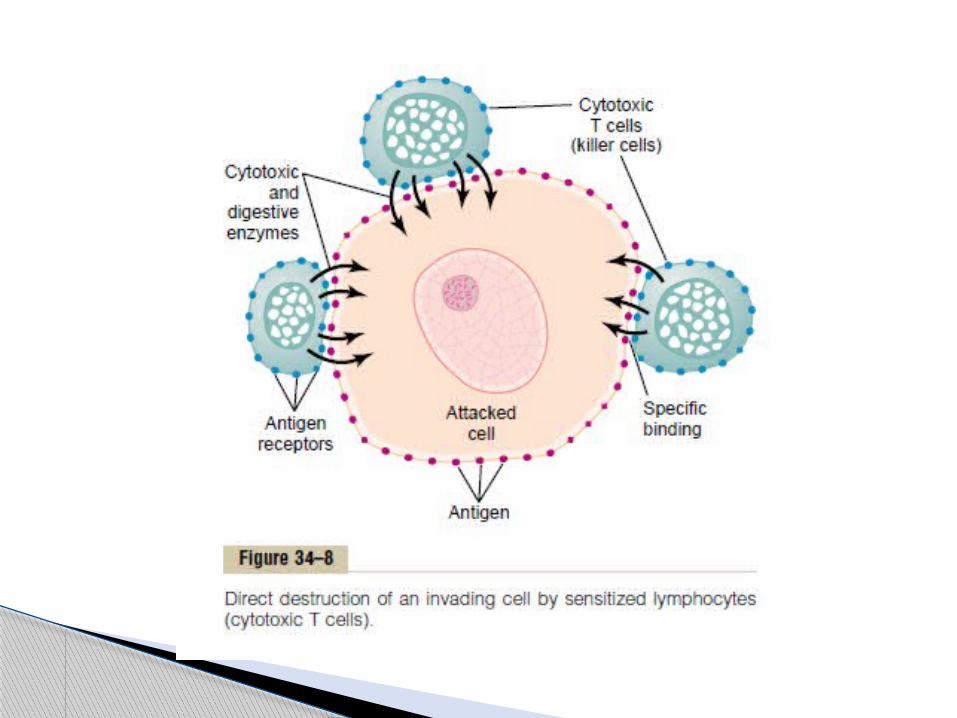

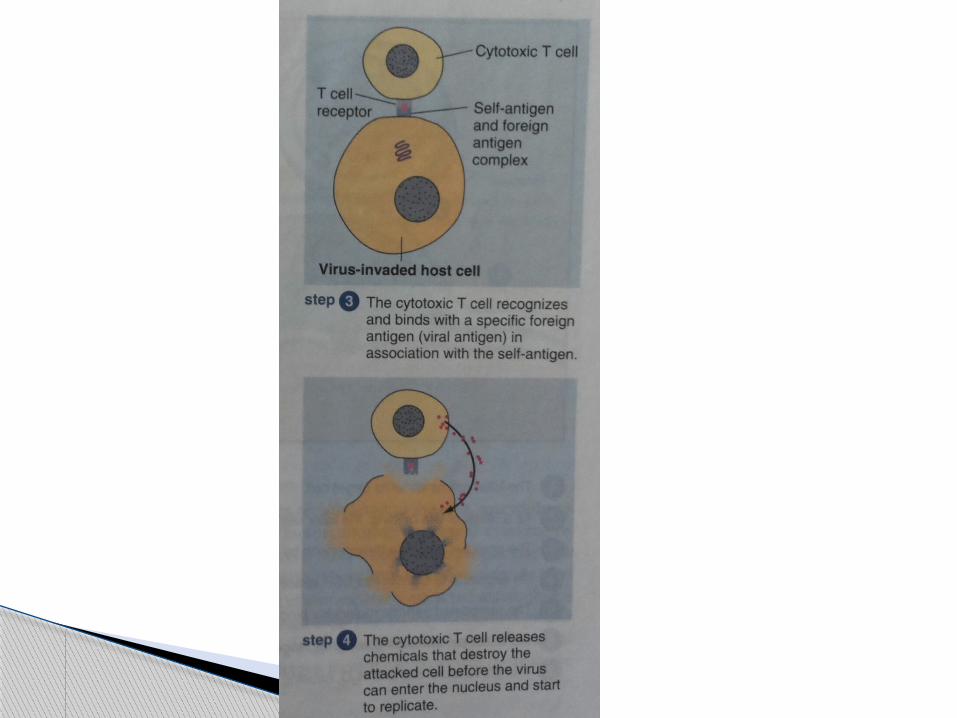
T-lymphocytes types and functions: Cytotoxic T Cells(killer cells): has a protien receptor that bind to a specific
antegin and secret perforins that punchholes in the attacked antigen and release cytotoxic substances
after that they pull away and kill more cells
Lymphocytes
Cytotoxic T-cells
They are lethal to cells invaded by viruses , cancer cells , and any other foreign cells
Lymphocytes


T-lymphocytes types and functions:
Supressor T-cells :
Capable of suppressing the functions of both cytotoxic and helper T cells
plays an important role in limiting the ability of the immune system to attack a person’s own body tissues, called immune tolerance
Failure of the Tolerance Mechanism Causes Autoimmune Diseases.
Lymphocytes
Old people
after destruction of the body’s own tissues , releasing considerable quantities of “self-antigens” that cause acquired immunity
• Rheumatoid fever• Glomerulonephritis• myasthenia gravis• lupus erythematosus,
Autoimmune disease
Other functions: Delayed-reaction allergy is caused by
activated T cells and not by antibodies on repeated exposure, it does cause the
formation of activated helper and cytotoxic T cells
the eventual result of some delayed-reaction allergies can be serious tissue damage in the tissue area where the instigating antigen is present.
Lymhocytes

“Allergic” Person, Excess IgE Antibodies Genetically passed IgE has strong propensity to attach to mast
cells and basophils. ,results in immediate change of the membrane and rupture of these cells and releasing substances that causes an allergic reaction (anaphylaxis, hay fever,asthma…)
Lymphocytes

Platelet count and function
Thrombocytes
(1-4 micrometer in diameter)
fragments of another type of cell found in the bone marrow, the megakaryocyte.
Function : activate the blood clotting mechanism
Normally: 150,000 -300,000 cells per microliter of blood.
Platelets

Lack nuclei , cannot reproduce They have contractile proteins in their cytoplasm:
1. actin2. Myocin3. Thrombosthenin
Residual E.R & G.A that synthesize enzymes and store Ca⁺²
Able to form ATP ,ADP , Fibrin stabilizing factor
Glycoprotiens on its cell membrane
platelets

replaced once every 10 days
Half life 8-12 days
Removed mainly by spleen macrophages
in other words, about 30,000 platelets are formed each day for each microliter of blood.
platelets

Hemostasis , mechanism & disorders
Means prevention of blood loss
After a vessel is ruptured, achieved by:
1. Vascular constriction2. Platelet plug3. Blood clot formation4. Growth of fibrous tissue into the clot to
close the hole permanently
hemostasis

Vascular constriction
Trauma to the blood vessel will cause its smooth muscles to contract ,to reduce blood flow from it
for the smaller vessels, platelets release a vasoconstrictor substance, thromboxane A2
The more severe a trauma is , the greater the degree of vascular spasm
Last from minutes to hours
hemostasis


Platelet plug.
When platelets comes to contact with exposed collagen
1. change in shape and contract2. They become sticky and adhere to
collagen and von willbrand factor3. They secrete ADP & thromboxane A2 that
activate other platelets and attract them
hemostasis
Blood coagulation
form in: 15-20 minutes in sever trauma 1-2 minutes in minor trauma
Activator substances & blood proteins adhere and initiate clotting process
Within 3 minute a clot it formed
after 20 minute the clot retracts to close the vessel even further
hemostasis


Fibrous organisation or dissolution of the blood clot
The clot is either invaded by fibroblasts which forms C.T through the clot. or it can dissolve
Mechanism of blood coagulation.
a complex cascade of chemical reactions occurs in the blood involving Coagulation factors. the net result is the formation of prothrombin activator.
The prothrombin activator catalyzes conversion of prothrombin into thrombin.
the thrombin acts as an enzyme to convert fibrinogen into fibrin fibers that enmesh platelets, blood cells, and plasma to form the clot.
hemostasis

Prothrombin is a plasma protein formed in the liver
Vitamin K is required in the liver for the formation of prothrombin and other clotting factors
Lack of vitamin K or presence of liver diseases lead to bleeding tendency
Hemostasis
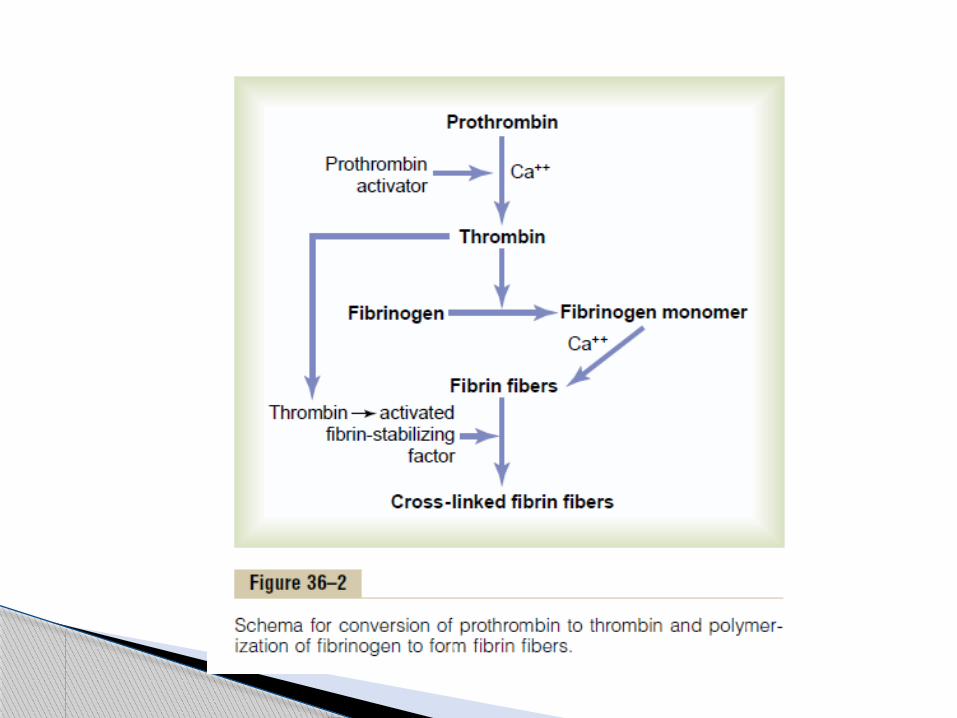

Conversion of prothrombin to thrombin
Prothrombin activator , In the presence of Ca⁺² causes the conversion of prothrombin to thrombin.
Platelets also help in prothrombin conversion
Thrombin polymerizes fibrinogen into fibrin
within 10-15 seconds
Hemostasis

Conversion of fibrinogen to fibrin-clot formation
Fibrin stabilizing factor produced by platelets add strength to this fibrin meshwork
Blood clot meshwork of fibrin fibers running in all directions & entrapping blood cells ,platelets & plasma

Clot retraction-serum
few minutes after clot is formed , it contracts, expressing the fluid from it( serum )
serum lacks fibrinogen and clotting factors
Serum differs from plasma that it lacks these clotting factors and so it cannot clot
Hemostasis

platelet thrombosthenin , actin, and myosin molecules causes clot contraction
The contraction is activated and accelerated by thrombin & calcium ions
the clot retracts
Hemostasis

Initiation of Coagulation: Formation of Prothrombin Activator
1. extrinsic pathway that begins with trauma to the vascular wall and surrounding tissues.
2. intrinsic pathway that begins in the blood itself.
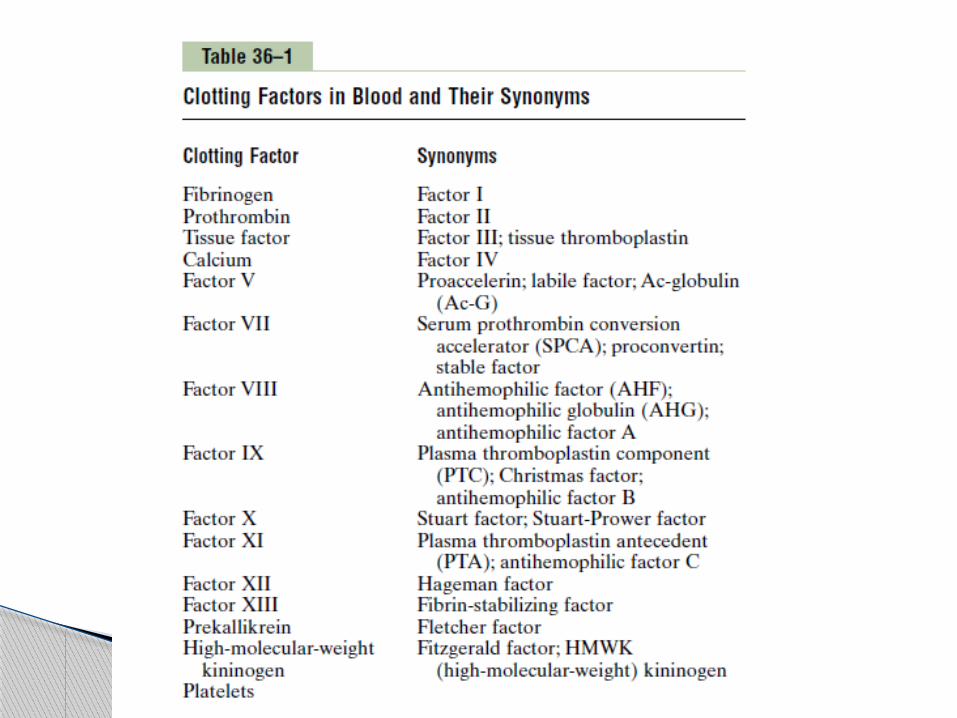
Blood clotting factors play major roles
Hemostasis
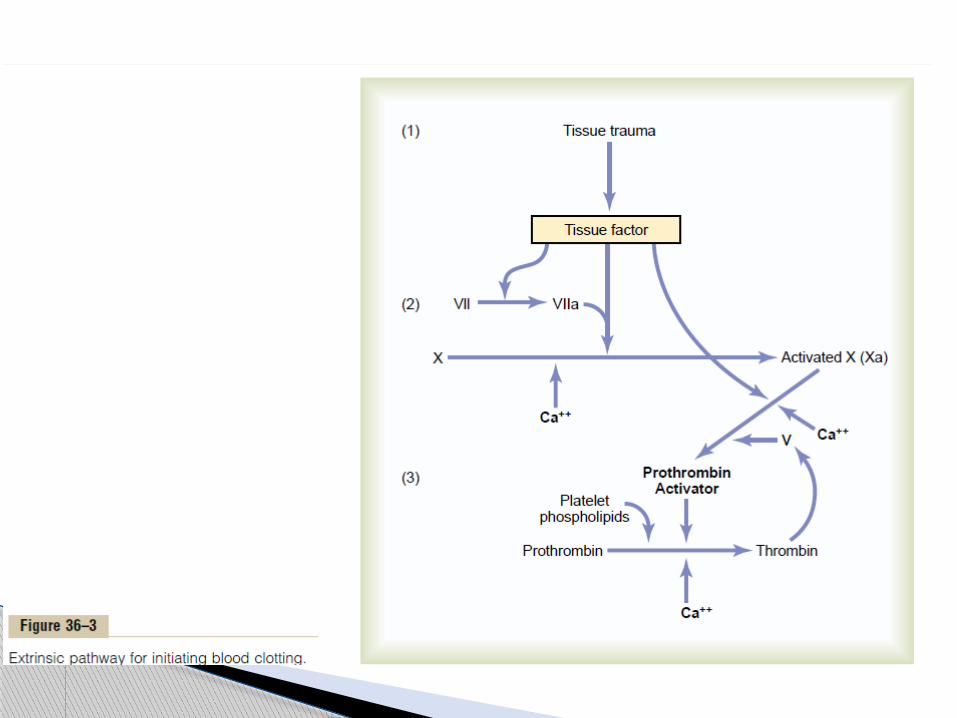

Extrinsic pathway Traumatized vascular wall that comes in contact with
blood results in release of tissue factor(tissue thromboplastin) that function as a proteolytic enzyme
Activation of factor X Xa combine with tissue factor and factor V in the
presence of Ca⁺² to form prothrombin activator Prothrombin is then convertedto thrombin & clotting
proceeds Factor V in the activator complex is inactive until
thrombin is formed,the proteolytic action of thrombin activate factor V
Hemostasis
Activated Factor X is the actual protease that causes splitting of prothrombin to form thrombin
Factor V is an accelerator
Hemostasis
Intrinsic pathway
begins with trauma to the blood itself or exposure of the blood to collagen from a traumatized blood vessel wall.
Hemostasis

Intrinsic pathway Blood trauma activate factor XII XIIa activate factor XI XIa activate factor IX XIa along with VIII and platelet phospholipds
activate factor XMissing factor VIIIhemophiliaLack of plateletsthrombocytopenia
Xa with factor V prothrombin activator
Hemostasis
Ca⁺² is an accelerator
in their absence blood clotting in either pathways does not occur
Both pathways occur simultaneously:
Clotting needs 15seconds in extrinsic pathway
Clotting needs 1-6 minutes in intrinsic pathway
Hemostasis

Prevention of Blood Clotting in the Normal Vascular System
Endothelial surface factors:
Smoothness of endothelial surface Glycocalyx layer on endothelium/repels
clotting factors Thrombomodulin: bind thrombin Anticoagulants in blood :antithrombin III,
heparin
Hemostasis

Lysis of clot
Plasmin
It destroys many of the clotting factors
Plasminogen entrapped inside the clot
t-PA (tissue plasminogen activator) is slowly released from injured tissue few days after the bleeding stops
Entrapped plasminogen is activated into plasmin
Hemostasis

1. Vitamin K deficiency
2. Hemophilia
3. thrombocytopenia
Bleeding disorders
Vitamin K deficiency
Vitamin K is necessary for liver formation of five of the important clotting factors:
1. prothrombin2. Factor VII3. Factor IX4. Factor X5. protein C
In the absence of vitamin K, subsequent insufficiency of these coagulation Factors in the blood can lead to serious bleeding tendencies.
Bleeding disorders
Hemophilia
In males
85% factor VIII deficiency :hemophilia A (classic hemophilia)
15% factor IX deficiency
Both factors are transmitted genetically
Bleeding disorders

Hemophilia
Bleeding occur following trauma
Even mild trauma can cause bleeding for days (e.x: tooth extraction)
Treatment of classic hemophilia is factor VIII injection
Hemophilia bleeding from large vessels
Bleeding disorders

Von Willbrand disease (vWD)
The most common hereditary coagulation abnormality
Defeciency of Von Willbrand factor (vWF)
vWF: protien required for platelet adhesion
Bleeding disorders
Thrombocytopenia
Low number of platelets circulating in the blood
Bleeding from small capillaries
Multiple small purplish blotches thrombocytopenic purura
Bleeding disorders

Thrombocytopenia
Bleeding occur when platelet number falls below 50,000/microliter
Levels below 10,000/microliter are lethal
Idiopathic thrombocytopenia:
specific antibodies destroy platelets
Treatment of thrombocytopenia: A. fresh whole blood transfusionB. splenectomy
Bleeding disorders

Thromboembolisms
Thrombus: abnormal clot that develop in a bood vessel
Emboli: free flowing clot
Causes:
Roughened endothelial surface
Slowly flowing blood
Treatment : genetically treated t-PA delivered through a catheter
Bleeding disorders
Femoral venous thrombosis & massive pulmonary embolism
Treatment: t-PA
Disseminated intravascular coagulation.
the clotting mechanism becomes activated in widespread areas of the circulation
Occurs in widespread septicemia in which endotoxins activate clotting mechanisms
Clots are small but numerous
Plug small peripheral blood vessels
Diminishes oxygen and nutrients delivery
leads to circulatory shock an death in 85% of patients
May cause bleeding
Anticoagulants
1. Heparins
increases clotting time to 30 minutes (normal=6 minutes)
the change in clotting time occurs immediately
action remains 1.5-4 hours
heparin is destroyed by the enzyme heparinase

Anticoagulants2. Coumarins
Ex:warfarin
blocking the action of vitamin K
Coagulation is not blocked immediately
Normal coagulation returns after 1-3 days of discontinuing coumarin therapy
INR international normalised ratio
1. Bleeding time
2. Clotting time
3. Prothrombin time
Blood coagulation tests
Bleeding time:
Normally 1-6 minutes
Lack of platelets causes prolonging the B.T
Blood Coagulation Tests

Clotting time
6-10 minutes
Not used anymore
Blood Coagulation Tests
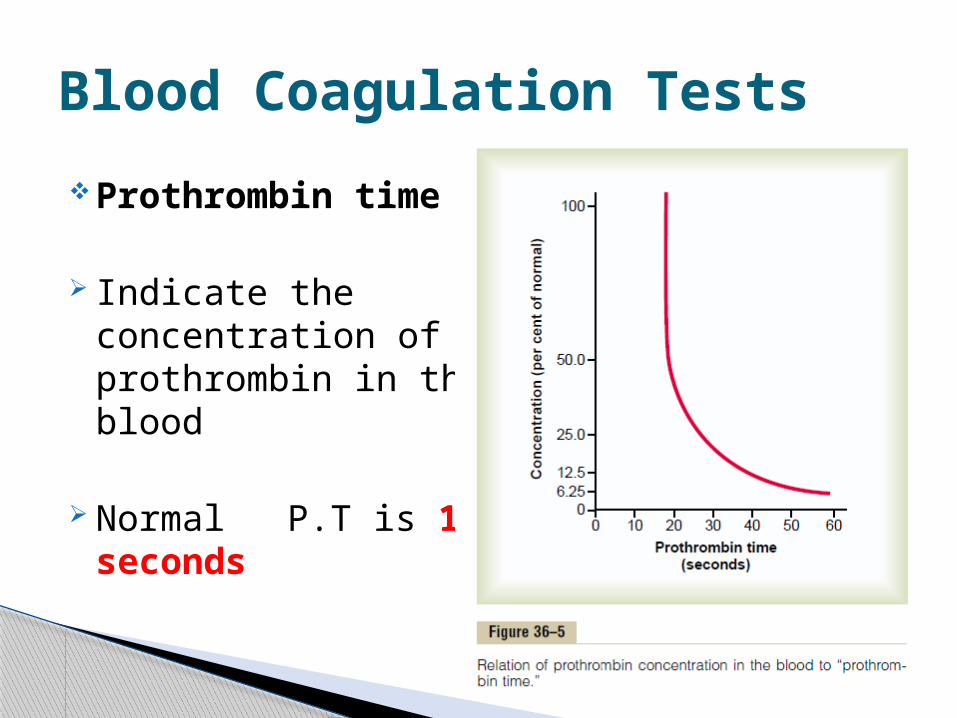
Prothrombin time
Indicate the concentration of prothrombin in the blood
Normal P.T is 12 seconds
Blood Coagulation Tests


















