GALVANIC STIMULATION TO PREVENT DEEP-VEIN THROMBOSIS
2
406 RESULTS OF ENZYME ASSAYS AND PROTEIN AND GLUCARIC-ACID MEASUREMENTS I I I N.D. = Not detected N.S. = Not significant. The values quoted are the means together with the standard deviations of determinations carried out on at least six placentas. The P values were obtained from the Student’s t test, values <0’05 being taken as significant. ately before the induction of labour was measured by a modified method of Marsh 3; microsomal protein was estimated by Lowry’s method. 4 RESULTS The results are summarised in the table. The human full-term placenta possessed measurable activities of hexobarbitone oxidase, p-nitroreductase, and 1-leucyl--naphthylamide splitting enzyme. Hexo- barbitone-oxidase activity was induced by barbiturate treatment while that of p-nitroreductase was signifi- cantly repressed. The activity of 1-leucyl-&bgr;-naphthyl- amide splitting enzyme was not affected by the indu- cing agent. Glucaric-acid excretion and placental pro- tein were significantly increased in the treated group. In neither the control nor the treated groups was ethyl- morphine-N-demethylase, cytochrome P450, or U.D.P.- glucuronyl transferase detected. The presence of cyto- chrome P, in human placenta has been demonstrated by Meigs and Ryan using a different method in which the enzyme was solubilised. The absence of U.D.P.- glucuronyl transferase confirms the work of others. 6 The electron micrographs showed that the fractions used contained predominantly vesicles of fragmented endoplasmic reticulum, mitochondria and nuclei being absent. DISCUSSION Work on the metabolism of foreign substances by placental enzymes has been reviewed by Juchau.7 Van Petten et al. demonstrated that pentobarbitone and amphetamine were rapidly oxidised by enzymes in the supernatant fraction of the full-term human placenta. Significant levels of hexobarbitone-oxidase activity were detected in rabbit placenta by Dixon and Wilson 9 following pre-treatment of animals with chlordane but not phenobarbitone. Berté et al. reported more amino- pyrine-N-demethylase in the 9000 g supernatant fraction of rabbit placenta at day 14 than day 30. The repression of p-nitroreductase in the human placenta by barbiturates with the concomitant induc- tion of hexobarbitone oxidase in the same tissue is interesting. This repression has been observed by Chhabra 2 and El-Tayeb 10 in hepatic tissue of rats, using organochlorine substances as inducing agents. The capacity of the human placenta to metabolise some drugs and the induction or repression of some of the enzyme systems involved by barbiturates makes it essential to re-evaluate the place of these drugs in the treatment of women during pregnancy. Microsomal drug-metabolising enzymes are non-specific and catalyse the biotransformation of natural body con- stituents such as cholesterol, fatty acids, steroids, bilirubin, and hormones. We do not know what effect the altered metabolism of some of these substances would have on the developing fetus or on the progress of pregnancy. Induction of u.D.P.-glucuronyl trans- ferase has been used to treat neonatal hyperbilirubin- aemia, but, since this enzyme could not be detected in human placenta even after barbiturate treatment, the conjugation of bilirubin must be extraplacental. Our findings reinforce the widely held view that the placenta supplements the developing fetal tissue and is capable, in a limited way, of metabolising a wide range of substances. We thank the surgeons and nurses of the obstetric department of St. Bartholomew’s Hospital for their cooperation. D. K. is in receipt of a fellowship from the Rockefeller Foundation. Requests for reprints should be addressed to P. T. REFERENCES 1. Hunter, J., Maxwell, J. D., Carrella, M., Stewart, D. A. Lancet, 1971, i, 572. 2. Chhabra, R. PH.D. thesis, University of London, 1970. 3. Marsh, C. A. Biochem. J. 1963, 86, 77. 4. Lowry, O. H. J. biol. Chem. 1957, 193, 265. 5. Meigs, R. A., Ryan, K. J. Biochim. biophys. Acta, 1968, 165, 476. 6. Berté, F., Manzo. L., de Bernardi, M., Benzi, G. Archs int. Pharmacodyn. 1969, 182, 182. 7. Juchau, M. R. Fedn Proc. 1972, 31, 48. 8. Van Petten, G. R., Hirsch, G. H., Cherrington, A. D. Can. J. Biochem. 1968, 46, 1057. 9. Dixon, R. L., Wilson, V. J. Archs int. Pharmacodyn. 1968, 172, 453. 10. El-Tayeb, I. B. Personal communication. Methods and Devices GALVANIC STIMULATION TO PREVENT DEEP-VEIN THROMBOSIS J. M. POWLEY Eastbourne Hospital Group F. S. A. DORAN Mid-Worcester Hospitals of Bromsgrove and Kidderminster INTERMITTENT contraction of the calf muscles by galvanic stimulation reduces the risk of deep-vein thrombosis during long operations.1-3 The standard machines used in depart- ments of physical medicine are unsuitable for a busy theatre list. Trailing wires and a mains connection are hazardous, and skill and time are required to prepare and position the saline-pad electrodes. The " electronic gaiters " described below can be applied rapidly by inexperienced junior staff and used in the smallest peripheral hospital or nursing-home. Lately many methods have been proposed in the battle against thromboembolism. Most of these
Transcript of GALVANIC STIMULATION TO PREVENT DEEP-VEIN THROMBOSIS

406
RESULTS OF ENZYME ASSAYS AND PROTEIN AND GLUCARIC-ACID MEASUREMENTS
I I I
N.D. = Not detected N.S. = Not significant.The values quoted are the means together with the standard deviations of determinations carried out on at least six placentas. The P values were obtained
from the Student’s t test, values <0’05 being taken as significant.
ately before the induction of labour was measured by amodified method of Marsh 3; microsomal protein was
estimated by Lowry’s method. 4
RESULTS
The results are summarised in the table.The human full-term placenta possessed measurable
activities of hexobarbitone oxidase, p-nitroreductase,and 1-leucyl--naphthylamide splitting enzyme. Hexo-barbitone-oxidase activity was induced by barbituratetreatment while that of p-nitroreductase was signifi-cantly repressed. The activity of 1-leucyl-&bgr;-naphthyl-amide splitting enzyme was not affected by the indu-cing agent. Glucaric-acid excretion and placental pro-tein were significantly increased in the treated group.In neither the control nor the treated groups was ethyl-morphine-N-demethylase, cytochrome P450, or U.D.P.-glucuronyl transferase detected. The presence of cyto-chrome P, in human placenta has been demonstratedby Meigs and Ryan using a different method in whichthe enzyme was solubilised. The absence of U.D.P.-
glucuronyl transferase confirms the work of others. 6The electron micrographs showed that the fractionsused contained predominantly vesicles of fragmentedendoplasmic reticulum, mitochondria and nuclei beingabsent.
DISCUSSION
Work on the metabolism of foreign substances byplacental enzymes has been reviewed by Juchau.7 VanPetten et al. demonstrated that pentobarbitone andamphetamine were rapidly oxidised by enzymes in thesupernatant fraction of the full-term human placenta.Significant levels of hexobarbitone-oxidase activitywere detected in rabbit placenta by Dixon and Wilson 9
following pre-treatment of animals with chlordane butnot phenobarbitone. Berté et al. reported more amino-pyrine-N-demethylase in the 9000 g supernatantfraction of rabbit placenta at day 14 than day 30.The repression of p-nitroreductase in the human
placenta by barbiturates with the concomitant induc-tion of hexobarbitone oxidase in the same tissue is
interesting. This repression has been observed byChhabra 2 and El-Tayeb 10 in hepatic tissue of rats,using organochlorine substances as inducing agents.The capacity of the human placenta to metabolise somedrugs and the induction or repression of some of theenzyme systems involved by barbiturates makes itessential to re-evaluate the place of these drugs in thetreatment of women during pregnancy. Microsomal
drug-metabolising enzymes are non-specific andcatalyse the biotransformation of natural body con-
stituents such as cholesterol, fatty acids, steroids,bilirubin, and hormones. We do not know what effectthe altered metabolism of some of these substanceswould have on the developing fetus or on the progressof pregnancy. Induction of u.D.P.-glucuronyl trans-ferase has been used to treat neonatal hyperbilirubin-aemia, but, since this enzyme could not be detected inhuman placenta even after barbiturate treatment, theconjugation of bilirubin must be extraplacental. Our
findings reinforce the widely held view that the placentasupplements the developing fetal tissue and is capable,in a limited way, of metabolising a wide range ofsubstances.
We thank the surgeons and nurses of the obstetric departmentof St. Bartholomew’s Hospital for their cooperation. D. K. is in
receipt of a fellowship from the Rockefeller Foundation.
Requests for reprints should be addressed to P. T.
REFERENCES
1. Hunter, J., Maxwell, J. D., Carrella, M., Stewart, D. A. Lancet,1971, i, 572.
2. Chhabra, R. PH.D. thesis, University of London, 1970.3. Marsh, C. A. Biochem. J. 1963, 86, 77.4. Lowry, O. H. J. biol. Chem. 1957, 193, 265.5. Meigs, R. A., Ryan, K. J. Biochim. biophys. Acta, 1968, 165, 476.6. Berté, F., Manzo. L., de Bernardi, M., Benzi, G. Archs int.
Pharmacodyn. 1969, 182, 182.7. Juchau, M. R. Fedn Proc. 1972, 31, 48.8. Van Petten, G. R., Hirsch, G. H., Cherrington, A. D. Can. J.
Biochem. 1968, 46, 1057.9. Dixon, R. L., Wilson, V. J. Archs int. Pharmacodyn. 1968, 172, 453.
10. El-Tayeb, I. B. Personal communication.
Methods and Devices
GALVANIC STIMULATION TO PREVENT
DEEP-VEIN THROMBOSIS
J. M. POWLEYEastbourne Hospital Group
F. S. A. DORAN
Mid-Worcester Hospitals of Bromsgrove and Kidderminster
INTERMITTENT contraction of the calf muscles by galvanicstimulation reduces the risk of deep-vein thrombosis duringlong operations.1-3 The standard machines used in depart-ments of physical medicine are unsuitable for a busytheatre list. Trailing wires and a mains connection arehazardous, and skill and time are required to prepare andposition the saline-pad electrodes. The " electronic gaiters
"
described below can be applied rapidly by inexperiencedjunior staff and used in the smallest peripheral hospital ornursing-home. Lately many methods have been proposedin the battle against thromboembolism. Most of these
407
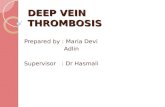
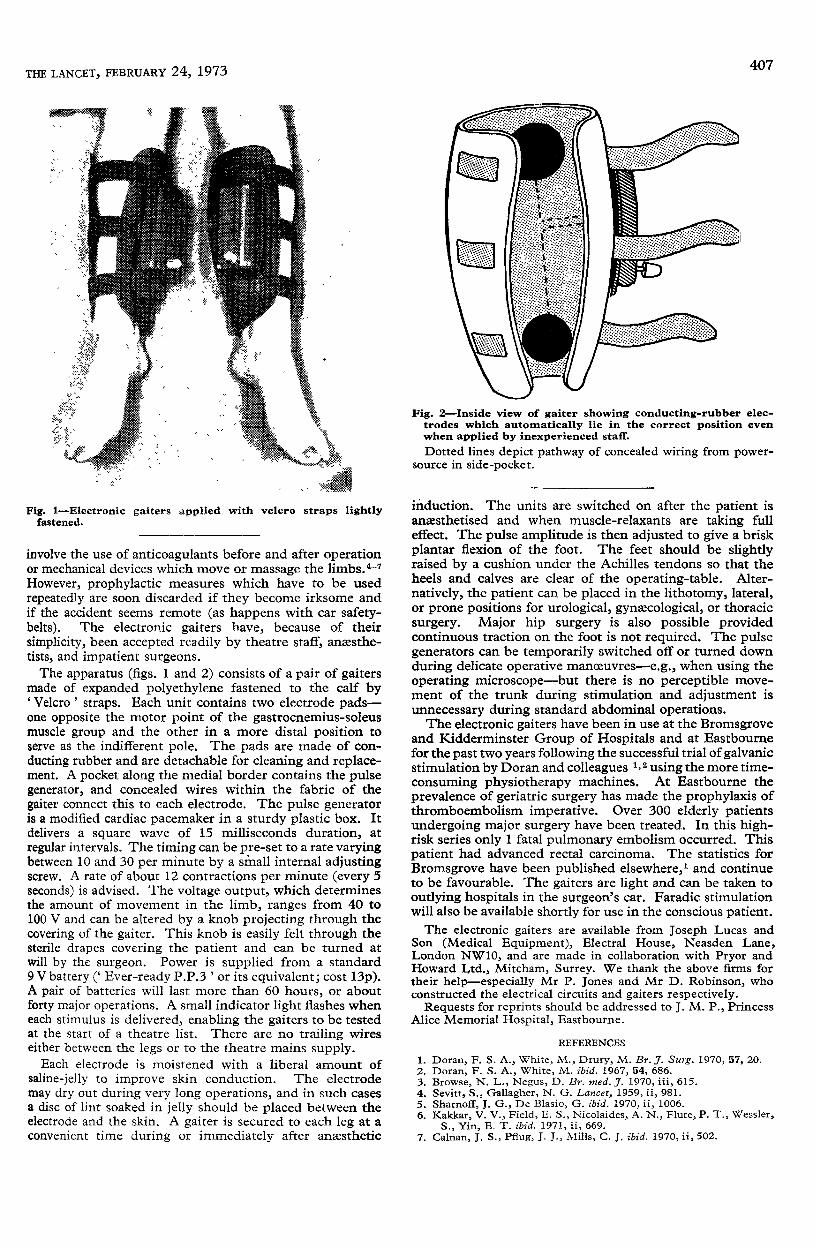
Fig. 1-Electronic gaiters applied with velcro straps lightlyfastened.
involve the use of anticoagulants before and after operationor mechanical devices which move or massage the limbs. 4-7However, prophylactic measures which have to be usedrepeatedly are soon discarded if they become irksome andif the accident seems remote (as happens with car safety-belts). The electronic gaiters have, because of theirsimplicity, been accepted readily by theatre staff, anaesthe-tists, and impatient surgeons.The apparatus (figs. 1 and 2) consists of a pair of gaiters
made of expanded polyethylene fastened to the calf by’Velcro’ straps. Each unit contains two electrode pads-one opposite the motor point of the gastrocnemius-soleusmuscle group and the other in a more distal position toserve as the indifferent pole. The pads are made of con-ducting rubber and are detachable for cleaning and replace-ment. A pocket along the medial border contains the pulsegenerator, and concealed wires within the fabric of thegaiter connect this to each electrode. The pulse generatoris a modified cardiac pacemaker in a sturdy plastic box. Itdelivers a square wave of 15 milliseconds duration, at
regular intervals. The timing can be pre-set to a rate varyingbetween 10 and 30 per minute by a small internal adjustingscrew. A rate of about 12 contractions per minute (every 5seconds) is advised. The voltage output, which determinesthe amount of movement in the limb, ranges from 40 to100 V and can be altered by a knob projecting through thecovering of the gaiter. This knob is easily felt through thesterile drapes covering the patient and can be turned atwill by the surgeon. Power is supplied from a standard9 V battery (’ Ever-ready P.P.3 ’ or its equivalent; cost 13p).A pair of batteries will last more than 60 hours, or aboutforty major operations. A small indicator light flashes wheneach stimulus is delivered, enabling the gaiters to be testedat the start of a theatre list. There are no trailing wireseither between the legs or to the theatre mains supply.Each electrode is moistened with a liberal amount of
saline-jelly to improve skin conduction. The electrodemay dry out during very long operations, and in such casesa disc of lint soaked in jelly should be placed between theelectrode and the skin. A gaiter is secured to each leg at aconvenient time during or immediately after anxsthetic
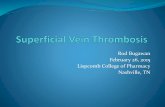
Fig. 2-Inside view of gaiter showing conducting-rubber elec-trodes which automatically lie in the correct position evenwhen applied by inexperienced staff.Dotted lines depict pathway of concealed wiring from power-
source in side-pocket.
induction. The units are switched on after the patient isanxsthetised and when muscle-relaxants are taking fulleffect. The pulse amplitude is then adjusted to give a briskplantar flexion of the foot. The feet should be slightlyraised by a cushion under the Achilles tendons so that theheels and calves are clear of the operating-table. Alter-natively, the patient can be placed in the lithotomy, lateral,or prone positions for urological, gynaecological, or thoracicsurgery. Major hip surgery is also possible providedcontinuous traction on the foot is not required. The pulsegenerators can be temporarily switched off or turned downduring delicate operative manoeuvres-e.g., when using theoperating microscope-but there is no perceptible move-ment of the trunk during stimulation and adjustment isunnecessary during standard abdominal operations.The electronic gaiters have been in use at the Bromsgrove
and Kidderminster Group of Hospitals and at Eastbournefor the past two years following the successful trial of galvanicstimulation by Doran and colleagues 1,2 using the more time-consuming physiotherapy machines. At Eastbourne the
prevalence of geriatric surgery has made the prophylaxis ofthromboembolism imperative. Over 300 elderly patientsundergoing major surgery have been treated. In this high-risk series only 1 fatal pulmonary embolism occurred. Thispatient had advanced rectal carcinoma. The statistics forBromsgrove have been published elsewhere, and continueto be favourable. The gaiters are light and can be taken tooutlying hospitals in the surgeon’s car. Faradic stimulationwill also be available shortly for use in the conscious patient.The electronic gaiters are available from Joseph Lucas and
Son (Medical Equipment), Electral House, Neasden Lane,London NW10, and are made in collaboration with Pryor andHoward Ltd., Mitcham, Surrey. We thank the above firms fortheir help-especially Mr P. Jones and Mr D. Robinson, whoconstructed the electrical circuits and gaiters respectively.
Requests for reprints should be addressed to J. M. P., PrincessAlice Memorial Hospital, Eastbourne.
REFERENCES
1. Doran, F. S. A., White, M., Drury, M. Br. J. Surg. 1970, 57, 20.2. Doran, F. S. A., White, M. ibid. 1967, 54, 686.3. Browse, N. L., Negus, D. Br. med. J. 1970, iii, 615.4. Sevitt, S., Gallagher, N. G. Lancet, 1959, ii, 981.5. Sharnoff, J. G., De Blasio, G. ibid. 1970, ii, 1006.6. Kakkar, V. V., Field, E. S., Nicolaides, A. N., Flute, P. T., Wessler,
S., Yin, E. T. ibid. 1971, ii, 669.7. Calnan, J. S., Pflug, J. J., Mills, C. J. ibid. 1970, ii, 502.