Fine-Needle Aspiration Biopsymarkahurt.com/files/documents/19930145powe-DFSP-FNA.pdf · the...
6
Fine-Needle Aspiration Biopsy: Dermatofibrosarcoma Protuberans Celeste N. Powers, M.D., Ph.D., Mark A. Hurt, M.D., and William J. Frable, M.D. Dermatofibrosarcoma protuberans (DFSP) represents a spectrum of mesenchymal spindle cell tumors that typically involve both dermis and subcutis. Presented herein are six cases of DFSP, four of which were initially diagnosed by FNAB. The cytologicfeatures useful in the identification of this lesion on Papanicolaou- and Dig-Quik-stained smears are discussed. Chief among these are the storiform stromal fragments, presence of entrapped adipose tissue and the recognition offbrohistiocytic spindle cells. The potential pitfalls and the differential diagnostic possibilities of spindle-cell lesions, particularly those of fibrohistiocytic origin are discussed. Diagn Cytopathol 1993;9:145-150. @ 1993 Wiley-Liss, Inc. Key Words: Fine-needle aspiration; Soft-tissue tumors; Der- matofibrosarcoma Dermatofibrosarcoma protuberans (DFSP) is an uncom- mon mesenchymal spindle cell neoplasm that typically involves dermis and subcutis. While the histopathology of this tumor and its variants has been well described, the aspiration cytology of these neoplasms has not been fully characterized. Although Perry et al. in 1986" described the fine-needle aspiration biopsy (FNAB) cytology of a DFSP that was metastatic to the lung, there has been no formal attempt to characterize the spectrum of FNAB findings observed in a series of lesions of DFSP. Thus, we present a series of six cases of DFSP in which FNAB was used as a diagnostic procedure. The cytologic criteria that aid in the classification of this spindle cell neoplasm are presented. The potential pitfalls associated with this diag- nosis are also discussed. Received March 11, 1992. Accepted June 15, 1992. From the Department of Pathology, University of Texas Health Sci- ence Center, San Antonio, TX; St. John's Mercy Medical Center, Section of Cutaneous Pathology, St. Louis, MO; and Virginia Commonwealth University, Health Sciences Division, Medical College of Virginia, Rich- mond, VA. Presented in part at the Thirty-Ninth Annual meeting of the American Society of Cytology, Los Angeles, November 1991. Address reprint requests to Celeste N. Powers, M.D., Ph.D., Depart- ment of Pathology, State University of New York, Health Science Center at Syracuse, 750 E. Adams Street, Syracuse, N Y 13210. Materials and Methods A search of our files of FNA biopsies from The University of Texas Health Science Center at San Antonio (UTHSCSA) and the Medical College of Virginia (MCV) yielded aspirates with the diagnosis consistent with or suggestive of DFSP. Three aspirates from UTHSCSA and three from MCV were retrieved. All aspirates were per- formed by a pathologist and had confirmation by surgical biopsy and/or excision. Because of the superficial location of these nodular masses a standard FNAB technique with- out anesthesia was used. '' Smears and in one case (1) a cell block were made from the aspirated material. Smears were either air-dried or fixed in 95% alcohol and stained with a modified Wright-Giemsa stain (Diff-Quik; Ameri- can Scientific Products, Columbia, MD) or Papanicolaou stain, respectively. In addition, in Case 1, minute frag- ments obtained from a 10% formalin rinse of 22-gauge needles were routinely processed and embedded in paraf- fin for routine histology. Hematoxylin and eosin stains were performed on the slides obtained from this cell block. The aspiration biopsies of six cases of DFSP were re- viewed and correlated with their previous or subsequent histology. Results This series was comprised of four women and two men who ranged in age from 22 to 59 yr. Table I lists the clinical presentation of these patients as well as the diag- nostic role played by FNAB. Four of six patients pre- sented with no prior diagnosis of any soft-tissue neo- plasms, the remaining patients (cases 5 and 6) presented with a prior diagnosis and surgical treatment of DFSP. All patients presented with similar complaints of a nodular mass usually slowly enlarging over a long period of time. Examination revealed these masses to be located in the superficial dermis and with the exception of an occipital scalp lesion, all masses were located in the upper trunk. FNAB was the initial diagnostic procedure in 4 of 6 cases E 1993 WILEY-LISS, INC Diugnostic Cytoputhology, Vol 9, No 2 145
Transcript of Fine-Needle Aspiration Biopsymarkahurt.com/files/documents/19930145powe-DFSP-FNA.pdf · the...

Fine-Needle Aspiration Biopsy: Dermatofibrosarcoma Protuberans Celeste N. Powers, M.D., Ph.D., Mark A. Hurt, M.D., and William J. Frable, M.D.
Dermatofibrosarcoma protuberans (DFSP) represents a spectrum of mesenchymal spindle cell tumors that typically involve both dermis and subcutis. Presented herein are six cases of DFSP, four of which were initially diagnosed by FNAB. The cytologic features useful in the identification of this lesion on Papanicolaou- and Dig-Quik-stained smears are discussed. Chief among these are the storiform stromal fragments, presence of entrapped adipose tissue and the recognition offbrohistiocytic spindle cells. The potential pitfalls and the differential diagnostic possibilities of spindle-cell lesions, particularly those of fibrohistiocytic origin are discussed. Diagn Cytopathol 1993;9:145-150. @ 1993 Wiley-Liss, Inc.
Key Words: Fine-needle aspiration; Soft-tissue tumors; Der- matofibrosarcoma
Dermatofibrosarcoma protuberans (DFSP) is an uncom- mon mesenchymal spindle cell neoplasm that typically involves dermis and subcutis. While the histopathology of this tumor and its variants has been well described, the aspiration cytology of these neoplasms has not been fully characterized. Although Perry et al. in 1986" described the fine-needle aspiration biopsy (FNAB) cytology of a DFSP that was metastatic to the lung, there has been no formal attempt to characterize the spectrum of FNAB findings observed in a series of lesions of DFSP. Thus, we present a series of six cases of DFSP in which FNAB was used as a diagnostic procedure. The cytologic criteria that aid in the classification of this spindle cell neoplasm are presented. The potential pitfalls associated with this diag- nosis are also discussed.
Received March 1 1 , 1992. Accepted June 15, 1992. From the Department of Pathology, University of Texas Health Sci-
ence Center, San Antonio, TX; St. John's Mercy Medical Center, Section of Cutaneous Pathology, St. Louis, MO; and Virginia Commonwealth University, Health Sciences Division, Medical College of Virginia, Rich- mond, VA.
Presented in part at the Thirty-Ninth Annual meeting of the American Society of Cytology, Los Angeles, November 1991.
Address reprint requests to Celeste N. Powers, M.D., Ph.D., Depart- ment of Pathology, State University of New York, Health Science Center at Syracuse, 750 E. Adams Street, Syracuse, NY 13210.
Materials and Methods A search of our files of FNA biopsies from The University of Texas Health Science Center at San Antonio (UTHSCSA) and the Medical College of Virginia (MCV) yielded aspirates with the diagnosis consistent with or suggestive of DFSP. Three aspirates from UTHSCSA and three from MCV were retrieved. All aspirates were per- formed by a pathologist and had confirmation by surgical biopsy and/or excision. Because of the superficial location of these nodular masses a standard FNAB technique with- out anesthesia was used. '' Smears and in one case (1) a cell block were made from the aspirated material. Smears were either air-dried or fixed in 95% alcohol and stained with a modified Wright-Giemsa stain (Diff-Quik; Ameri- can Scientific Products, Columbia, MD) or Papanicolaou stain, respectively. In addition, in Case 1, minute frag- ments obtained from a 10% formalin rinse of 22-gauge needles were routinely processed and embedded in paraf- fin for routine histology. Hematoxylin and eosin stains were performed on the slides obtained from this cell block. The aspiration biopsies of six cases of DFSP were re- viewed and correlated with their previous or subsequent histology.
Results This series was comprised of four women and two men who ranged in age from 22 to 59 yr. Table I lists the clinical presentation of these patients as well as the diag- nostic role played by FNAB. Four of six patients pre- sented with no prior diagnosis of any soft-tissue neo- plasms, the remaining patients (cases 5 and 6) presented with a prior diagnosis and surgical treatment of DFSP. All patients presented with similar complaints of a nodular mass usually slowly enlarging over a long period of time. Examination revealed these masses to be located in the superficial dermis and with the exception of an occipital scalp lesion, all masses were located in the upper trunk. FNAB was the initial diagnostic procedure in 4 of 6 cases
E 1993 WILEY-LISS, INC Diugnostic Cytoputhology, Vol 9, No 2 145
POWERS ET AL.
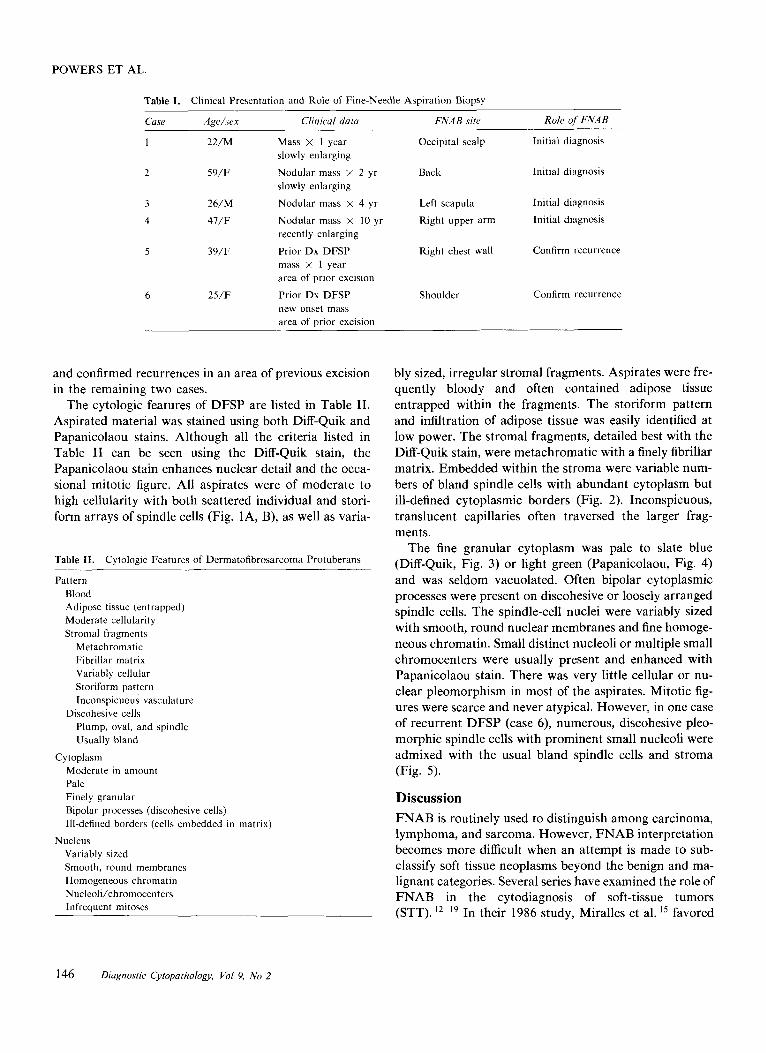
Table I.
Case Apehex Clinical data
Clinical Presentation and Role of Fine-Needle Aspiration Biopsy
FNAB site Role of FNAB ~~
1 22/M Mass x 1 year Occipital scalp Initial diagnosis
2 59/F Nodular mass X 2 yr Back Initial diagnosis
3 26/M Nodular mass X 4 yr Left scapula Initial diagnosis
47/F Nodular mass X 10 yr Right upper arm Initial diagnosis 4
slowly enlarging
slowly enlarging
recently enlarging 5 39/F Prior Dx DFSP Right chest wall Confirm recurrence
mass X 1 year area o f prior excision
Shoulder Confirm recurrence 6 25/F Prior Dx DFSP new onset mass area o f prior excision
and confirmed recurrences in an area of previous excision in the remaining two cases.
The cytologic features of DFSP are listed in Table 11. Aspirated material was stained using both Diff-Quik and Papanicolaou stains. Although all the criteria listed in Table I1 can be seen using the Diff-Quik stain, the Papanicolaou stain enhances nuclear detail and the occa- sional mitotic figure. All aspirates were of moderate to high cellularity with both scattered individual and stori- form arrays of spindle cells (Fig. lA, B), as well as varia-
Table 11.
Pattern
Cytologic Features of Dermatofibrosarcoma Protuberans
Blood Adipose tissue (entrapped) Moderate cellularity Stromal fragments
Metachromatic Fibrillar matrix Variably cellular Storiform pattern Inconspicuous vasculature
Discohesive cells Plump, oval, and spindle Usually bland
Cytoplasm Moderate in amount Pale Finely granular Bipolar processes (discohesive cells) Ill-defined borders (cells embedded in matrix)
Variably sized Smooth, round membranes Homogeneous chromatin Nucleoli/chromocenters Infrequent mitoses
Nucleus
bly sized, irregular stromal fragments. Aspirates were fre- quently bloody and often contained adipose tissue entrapped within the fragments. The storiform pattern and infiltration of adipose tissue was easily identified at low power. The stromal fragments, detailed best with the Diff-Quik stain, were metachromatic with a finely fibrillar matrix. Embedded within the stroma were variable num- bers of bland spindle cells with abundant cytoplasm but ill-defined cytoplasmic borders (Fig. 2). Inconspicuous, translucent capillaries often traversed the larger frag- ments.
The fine granular cytoplasm was pale to slate blue (Diff-Quik, Fig. 3) or light green (Papanicolaou, Fig. 4) and was seldom vacuolated. Often bipolar cytoplasmic processes were present on discohesive or loosely arranged spindle cells. The spindle-cell nuclei were variably sized with smooth, round nuclear membranes and fine homoge- neous chromatin. Small distinct nucleoli or multiple small chromocenters were usually present and enhanced with Papanicolaou stain. There was very little cellular or nu- clear pleomorphism in most of the aspirates. Mitotic fig- ures were scarce and never atypical. However, in one case of recurrent DFSP (case 6), numerous, discohesive pleo- morphic spindle cells with prominent small nucleoli were admixed with the usual bland spindle cells and stroma (Fig. 5).
Discussion FNAB is routinely used to distinguish among carcinoma, lymphoma, and sarcoma. However, FNAB interpretation becomes more difficult when an attempt is made to sub- classify soft tissue neoplasms beyond the benign and ma- lignant categories. Several series have examined the role of FNAB in the cytodiagnosis of soft-tissue tumors (STT). I 2 z l 9 In their 1986 study, Miralles et al. l 5 favored
146 Diagnostic CytopathoIogy, Vol 9, No 2

FNAB: DERMATOFIBROSARCOMA PROTUBERANS
Fig. 1. A: Storiform arrays of spindle cell fragments in a moderately cellular aspirate (Diff Quik, x 250). B: Spindle cells with uniform, bland nuclei embedded within dense matrix (Diff-Quik, ~ 4 0 0 ) .
the classification of soft tissue sarcomas into five catego- ries: I, low grade; 11, myxoid; 111, monomorphic; IV, round cell; and V, pleomorphic. The classification of an aspirate into the low grade category would imply a popu- lation of spindle cells with minimal cytologic atypia, a low mitotic index, and absence of necrosis. The diagnostic possibilities include not only DFSP and low-grade fibro- sarcoma but benign entities such as nodular fasciitis, fi- brous histiocytoma, and fibromatosis. Nguyen l6 has sug- gested dividing STT into only three categories: I, pleomorphic cell tumors; 11, spindle cell tumors; and 111, small round cell tumors. Once classified into one of these broad categories, additional cytologic criteria and im- munocytochemistry can be applied to help further classify these tumors. This technique is especially useful if enough material is aspirated to produce a cell block. Based on this classification schema, DFSP would be assigned to the sec- ond category, spindle cell tumors.
As in other areas of aspiration biopsy, the importance of clinicopathologic correlation can not be overempha- sized. DFSP is usually a firm, nodular (protuberant) cuta- neous mass that has been slowly enlarging over a pro- longed period of time, often years. Occasionally there is a history of antecedent trauma. Although typically located on the trunk or proximal extremities, a small percentage occur as scalp lesions.''
The initial classification of an aspirate as a STT, possi- bly DFSP begins with the identification of the neoplastic cell as fibrohistiocytic, rather than neural or muscular. This separation can sometimes be made on the basis of nuclear shape alone. Reactive fibroblasts often have an- gulated nuclei, while those of DFSP tend to have a round/ oval shape. Nuclei from smooth muscle tumors are often described as cigar-shaped with blunt ends; those from neural lesions are twisted, slender, and elongate. In gen- eral, DFSP fibroblasts tend to have moderate amount of
Diagnostic Cytopathology, Vol 9, No 2 147
POWERS ET AL.
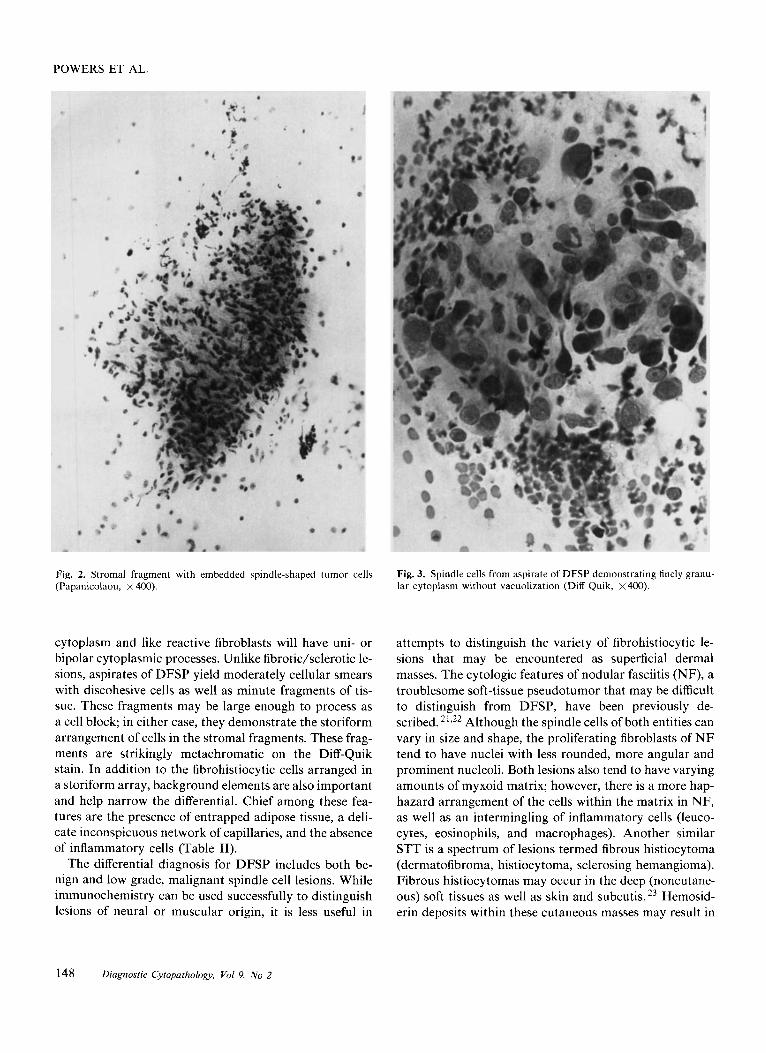
Fig. 2. Stromal fragment with embedded spindle-shaped tumor cells (Papanicolaou, x 400).
Fig. 3. Spindle cells from aspirate of DFSP demonstrating finely granu- lar cytoplasm without vacuolization (Diff Quik, X 400).
cytoplasm and like reactive fibroblasts will have uni- or bipolar cytoplasmic processes. Unlike fibrotic/sclerotic le- sions, aspirates of DFSP yield moderately cellular smears with discohesive cells as well as minute fragments of tis- sue. These fragments may be large enough to process as a cell block; in either case, they demonstrate the storiform arrangement of cells in the stromal fragments. These frag- ments are strikingly metachromatic on the Diff-Quik stain. In addition to the fibrohistiocytic cells arranged in a storiform array, background elements are also important and help narrow the differential. Chief among these fea- tures are the presence of entrapped adipose tissue, a deli- cate inconspicuous network of capillaries, and the absence of inflammatory cells (Table 11).
The differential diagnosis for DFSP includes both be- nign and low grade, malignant spindle cell lesions. While immunochemistry can be used successfully to distinguish lesions of neural or muscular origin, it is less useful in
attempts to distinguish the variety of fibrohistiocytic le- sions that may be encountered as superficial dermal masses. The cytologic features of nodular fasciitis (NF), a troublesome soft-tissue pseudotumor that may be difficult to distinguish from DFSP, have been previously de- scribed. 21,22 Although the spindle cells of both entities can vary in size and shape, the proliferating fibroblasts of N F tend to have nuclei with less rounded, more angular and prominent nucleoli. Both lesions also tend to have varying amounts of myxoid matrix; however, there is a more hap- hazard arrangement of the cells within the matrix in NF, as well as an intermingling of inflammatory cells (leuco- cytes, eosinophils, and macrophages). Another similar STT is a spectrum of lesions termed fibrous histiocytoma (dermatofibroma, histiocytoma, sclerosing hemangioma). Fibrous histiocytomas may occur in the deep (noncutane- ous) soft tissues as well as skin and subcutis. 23 Hemosid- erin deposits within these cutaneous masses may result in
148 Diagnostic Cytopathology, Vol 9, No 2

FNAB: DERMATOFIBROSARCOMA PROTUBERANS
Fig. 4. Details of loosely cohesive spindle cells with cytoplasmic pro- cesses, smooth nuclear membranes, homogeneous chromatin, and small nucleoli (Papanicolaou, x 1,000).
red to brown discoloration of the overlying skin. This may help clinically to distinguish them from DFSP. Aspirates from these masses produce stromal fragments of increased cell density and less intercellular matrix. In addition, background elements that may be present include plump histiocytes and multinucleate tumor giant cells that are often pigment laden, as well as inflammatory cells. The presence of entrapped adipose tissue suggests an infiltra- tive pattern as seen in DFSP, rather than the more circum- scribed histiocytoma. Fibromatosis and low-grade fibro- sarcoma are also problematic, 1 2 , ’ 5 9 1 7 especially since an adequate sample is sometimes difficult to obtain because of tight cellular cohesion. The cytologic features of these fibroblasts can vary considerably, from the deceptively bland low-grade sarcoma to the worrisome nuclear pleo- morphism of aggressive fibromatosis. Other less likely en- tities that may be included in the differential diagnosis of DFSP include Kaposi’s sarcoma and amelanotic mela-
Fig. 5. Aspirate from case 6, demonstrating high cellularity with dis- cohesive and more pleomorphic spindle cells having prominent but small nucleoli. These are mixed with the usual bland spindle-tumor cells most commonly seen in the other cases of DFSP in this series (Diff-Quik, x 400).
noma. Aspirates from Kaposi’s sarcoma typically contain delicate, discohesive, elongate spindle cells in a back- ground of abundant blood. Even less likely to be confused cytologically with DFSP are melanomas. Aspirates from these lesions may show pleomorphic spindle cells, but with minimal stroma and no discernible storiform pattern. Although clinical correlation may be very helpful in a majority of cases, there are instances when a specific diag- nosis may not be possible. In these cases, a more general diagnosis such as “spindle-cell tumor” or “mesenchymal lesion” with a list of probable diagnoses may have to suffice.
Because of the propensity of DFSP to recur, surgical treatment includes ample (3-cm) margins. Even with these margins the recurrence rate can be as high as 20%.24 Unfortunately, the likelihood of metastatic disease in-
Diagnostic Cytopathology, Vol 9, No 2 149
POWERS ET AL.
creases with multiple recurrences. 3,24 An additional prob- lem is the occurrence of frank sarcomatous change; areas of fibrosarcoma (FS) and malignant fibrous histiocytoma (MFH) can be found in initial, as well as recurrent DFSP and are associated with a less favorable prognosis. ' 9 8 3 2 5
Because FNAB samples very discreet areas, sarcomatous change can be missed entirely on FNAB (sampling error) or can be diagnosed as MFH or FS. The variability of some of these tumors histologically requires multiple FNAB's with sampling from different areas. DFSP will more often have a consistent cytologic pattern from mul- tiple samples. It is unlikely that the standard surgical treatment for DFSP will adversely affect the patient in either case.
Soft-tissue tumors, particularly those of fibrohistiocytic origin, may be difficult to accurately diagnose on FNAB. The presence of stromal fragments in aspirate smears or cell block sections allows not only examination of individ- ual cell morphology but recognition of distinctive pat- terns, that in conjunction with good clinical data, are helpful in the subclassification of these lesions. Cytologic features useful in the diagnosis of DFSP include storiform arrays of spindle cells, presence of entrapped adipose tis- sue, and lack of background elements such as inflamma- tory cells.
References 1. Borrie P. Dermatofibrosarcoma protuberans Br J Surg 1952; 39:
452-3. 2. Burkhardt BR, Soule EH, Winkelmann RK, Ivins JC. Dermatofi-
brosarcoma protuberans: a study of 56 cases. Am J Surg 1966; 1 1 1: 638-44.
3. McPeak CJ, Cruz T, Nicastri AD. Dermatofibrosarcoma protuber- ans: An analysis of 86 cases-five with metastasis. Ann Surg 1967; 66(suppl 12): 803-16.
4. Frierson HF, Cooper PH. Myxoid variant of dermatofibrosarcoma protuberans. Am J Surg Pathol 1983; 7:445-50.
5. Dupree WB, Langloss JM, Weiss SW. Pigmented dermatofibrosar- coma protuberans (Bednar tumor) A pathologic, ultrastructural and immunohistochemical study. Am J Surg Pathol 1985; 9: 630-9.
6. Fletcher CDM, Macartney JC, Smith N, Wilson Jones E, McKee PH. Dermatofibrosarcoma protuberans: a clinicopathological and immunohistochemical study with review of the literature. Histopa-
7. Wrotnowski U, Cooper PH, Shmookler BM. Fibrosarcomatous change in dermatofibrosarcoma protuberans. Am J Surg Pathol 1988; 12:287-93.
8. Ding J, Hashimoto H, Enjoji M. Dermatofibrosarcoma protuberans with fibrosarcomatous areas Cancer 1989; 64: 721-9.
9. Beham A, Fletcher CDM. Dermatofibrosarcoma protuberans with areas resembling giant cell fibroblastoma: report of two cases. Histo- pathology 1990; 17: 165-82.
10. Perry MD, Furlong JW, Johnston WW. Fine-needle aspiration cy- tology of metastatic dermatofibrosarcoma protuberans. Acta Cytol 1986; 30:507-12.
11. Frable WJ. Thin-needle aspiration biopsy. A personal experience with 469 cases. 1976;65: 168-82.
12. Akerman M, Idvall I, Rydholm A. Cytodiagnosis of soft tissue
thology 1985; 9: 921-38.
tumors and tumor-like conditions by means of fine-needle aspiration biopsy. Arch Othop Traum Surg 1980;96:61-7.
13. Rydholm A, Akerman M, Idvall I, Persson BM. Aspiration cytol- ogy of soft tissue tumors: A prospective study of its influence on choice of surgical procedure. Int Orthop 1982; 6: 209-14.
14. Kindblom LG. Light and electron microscopic examination of em- bedded fine-needle aspiration biopsy specimens in the preoperative diagnosis of soft tissue and bone tumors. Cancer 1983;51:2264- 77.
15. Miralles TG, Gosalbez F, Menedez P, Astudillo A, Torre C, Buesa J. Fine-needle aspiration cytology of soft-tissue lesions. Acta Cytol 1986; 30:671-8.
16. Nguyen GK. What is the value of fine-needle aspiration biopsy in the cytodiagnosis of soft-tissue tumors? Diagn Cytopathol 1988; 4: 352-5.
17. Oland J, Rosen A, Reif R, Sayfan J, Orda R. Cytodiagnosis of soft tissue tumors. J Surg Oncol 1988;37: 168-70.
18. Gonzalez-Campora R, Otal-Salaverri C, Hevia-Vazquez A, Munoz- Munoz G, Garrido-Cintado A, Galera-Davidson H. Fine-needle aspiration in myxoid tumors of the soft tissues. Acta Cytol 1990; 34: 179-91.
19. Ferno M, Baldetorp B, Akerman M. Flow cytometric DNA ploidy analysis of soft tissue sarcomas: a comparative study of preoperative fine-needle aspirates and post operative fresh tissues and archival material. Acta Cytol 1990; 12:251-8.
20. Rockley PF, Robinson JK, Magid M, Goldblatt D. Dermatofi- brosarcoma protuberans of the scalp: a series of cases. J Am Acad Dermatol 1989;21:278-83.
21. Dahl I, Akerman M. Nodular fasciitis: a correlative cytologic and histologic study of 13 cases. Acta Cytol 1981;25:215-23.
22. Jelen M, Wozniak Z . Cytological findings in nodular fascitis. Zen- tralb Allg Pathol Anat 1988; 134:505-9.
23. Fletcher CDM. Benign fibrous histiocytoma of subcutaneous and deep soft tissue: a clinicopathologic analysis of 21 cases. Am J Surg Pathol 1990; 14:801-9.
24. Roses DF, Valensi Q, LaTrenta G, Harris MN. Surgical treatment of dermatofibrosarcoma protuberans. Surg Gynecol Obstet 162:
25. Kamino H, Jacobson M. Dermatofibroma extending into the subcu- taneous tissue: differential diagnosis from dermatofibrosarcoma pro- tuberans. Am J Surg Pathol 1990; 14: 1156-64.
26. Domagala WM, Markiewski M, Tuziak T, Kram A, Wber K, Os- born M. Immunocytotechmistry on fine-needle aspirates in paraffin miniblocks. Acta Cytol 1990; 34: 291-6.
27. Kung ITM, Chan SK, Lo ESF. Application of the immunoperoxi- dase technique to cell block preparations from fine-needle aspirates. Acta Cytol 1990; 34: 297-303.
28. Fletcher CDM, Theaker JM, Flanagan A, Krausz T. Pigmented dermatofibrosarcoma protuberans (Bednar tumor): melanocytic col- onization or neuroectodermal differentiation? A clinicopathological and immunohistochemical study. Histopathology 1988; 13: 631-43.
29. Lautier R, Wolff HH, Jones, RE. An immunohistochemical study of dermatofibrosarcoma protuberans supports its fibroblastic char- acter and contradicts neuroectodermal or histiocytic components. Am J Dermatopathol 1990; 12:25-30.
30. Kindbloom LG, Jacobsen GK, Jacobsen M. Immunohistochemical investigation of tumors of supposed fibroblastic-histiocytic origin. Hum Pathol 1982; 13:834-40.
31. Enzinger FM, Weiss SW. Soft Tissue Tumors. 2nd Ed. St. Louis, CV Mosby, 1988:111, 120, 140, 151, 210.
32. Battifora H. Immunohistochemistry in tumor diagnosis. Handout Manual. Boston: International Academy of Pathology Short Course. 1990: 30.
33. Kiyshi M, Schollmeyer JV, Rosai J. Immunohistochemical localiza- tion of actin. Am J Surg Pathol 1981;5:91-7.
449-52, 1986.
150 Diagnostic Cytopathology, Vol 9, No 2