
Breast filariasis - A fine needle aspiration cytology report
5
Breast filariasis - A fine needle aspiration cytology report
-
Upload
apollo-hospitals -
Category
Health & Medicine
-
view
107 -
download
0
Transcript of Breast filariasis - A fine needle aspiration cytology report

Breast filariasis - A fine needle aspiration cytology report

Case Report
Breast filariasis e A fine needle aspiration cytologyreport
Abdul Hakeem Attar*, K. Naseer
Department of Pathology & Medicine, ESIC Medical College & Owais Hospital Gulbarga, India
a r t i c l e i n f o
Article history:
Received 14 January 2014
Accepted 11 March 2014
Available online xxx
Keywords:
Wuchereria bancrofti
Filariasis
Fine needle aspiration cytology
a b s t r a c t
Filariasis is a major health problem in tropical countries. The disease is endemic in large
areas of India. Lymphatic filariasis in human is commonly caused by Wuchereria bancrofti
and Brugia malayi. Extranodal filariasis is a rare entity and the breast is an uncommon site
for filariasis. We report a case of female who presented with lump in the left breast. Fine
needle aspiration cytology of lump revealed numerous adult filarial worms.
Copyright ª 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
Lymphatic filariasis or elephantiasis affects more than 90
million people worldwide and has been identified by WHO as
thesecond leadingcauseofpermanentand long termdisability
after leprosy.1 Bancroftian filariasis has a worldwide distribu-
tion with disease prevalence in Africa, Asia including China,
India and Southeast Asia. It is a major problem in tropical
countries.2 The breast is an unusual site for occurrence of a
filarial nodule and only a few such cases have been docu-
mented. Microfilaria and adult worms are detected by needle
aspirates from the breast, which aid in the diagnosis and
treatmentofdisease.2Wepresentanold femalewhopresented
with lump in the left breast, mimicking carcinoma of breast.
2. Case presentation (clinical details)
A 68 year old femalewho presentedwith a painless lump in the
left breast of one year duration. It was gradually increasing in
size. On examination there was a single hard non-tender lump
measuring about 4 � 5 cm and was located in the upper outer
quadrant of the breast with fixity to overlying with peau d’or-
ange. There were no palpable axillary lymphnodes.
3. Cytological findings
Fine needle aspiration of the breast nodule was performed
using a 22 e gauge needle attached to a 5 ml disposable
syringe. The aspirate was smeared on a slide, air-dried and
stained with May-Grunwald-giemsa stain. Cytologic
examination revealed a gravid female adult worm along
with numerous microfilarias both in coiled and uncoiled
forms (Fig. 1). The microfilarias were sheathed with elon-
gated terminal nuclei and caudal space at the posterior end
(Fig. 4). There were scattered ductal epithelial cells, in-
flammatory cells and lymphatic fluid seen in the back-
ground (Figs. 2 and 3). A diagnosis of microfilaria of the
breast morphologically consistent with the Wuchereria ban-
crofti was entertained.
* Corresponding author. C/O Abdul Azeem Attar, Shameem Masala Attar Bazar, Gulbarga 585101, India.E-mail addresses: [email protected], [email protected] (A. Hakeem Attar).
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.elsevier .com/locate/apme
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3
Please cite this article in press as: Hakeem Attar A, Naseer K, Breast filariasis e A fine needle aspiration cytology report, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.03.001
http://dx.doi.org/10.1016/j.apme.2014.03.0010976-0016/Copyright ª 2014, Indraprastha Medical Corporation Ltd. All rights reserved.
4. Discussion
Filariasis is a serious socioeconomic and public health problem
of huge magnitude. It is endemic in large areas of India. W.
bancrofti accounts for approximately 90% of all filarial cases in
theworld followedbyBrugiamalayi. Femalebreast is anunusual
site for theoccurrenceoffilarialnoduleand fewsuchcaseshave
been documented in literature.1 Other rare unusual sites in
which microfilaria are reported includes the thyroid nodule,
salivary gland, cervicovaginal smear, ovarian cyst fluid, bron-
chial brushings, effusion fluid and gastric brush.2 The common
habitat of the adult filarial worms is the lymphatic vessels and
lymph nodes of limbs and their occurrence in breast is un-
common.3 Bancroftian filariasis has a worldwide distribution.
Insectsparticularlymosquitoesservesas the intermediatehost.
While taking a bloodmeal the insect ingestsmicrofilaria. Over 2
to 3 weeks the MF develop within the insect in to the infective
third stage larvae.Theyreenter thedefinitivehumanhostwhen
the insect feeds again. The larvae mature in to adult worm
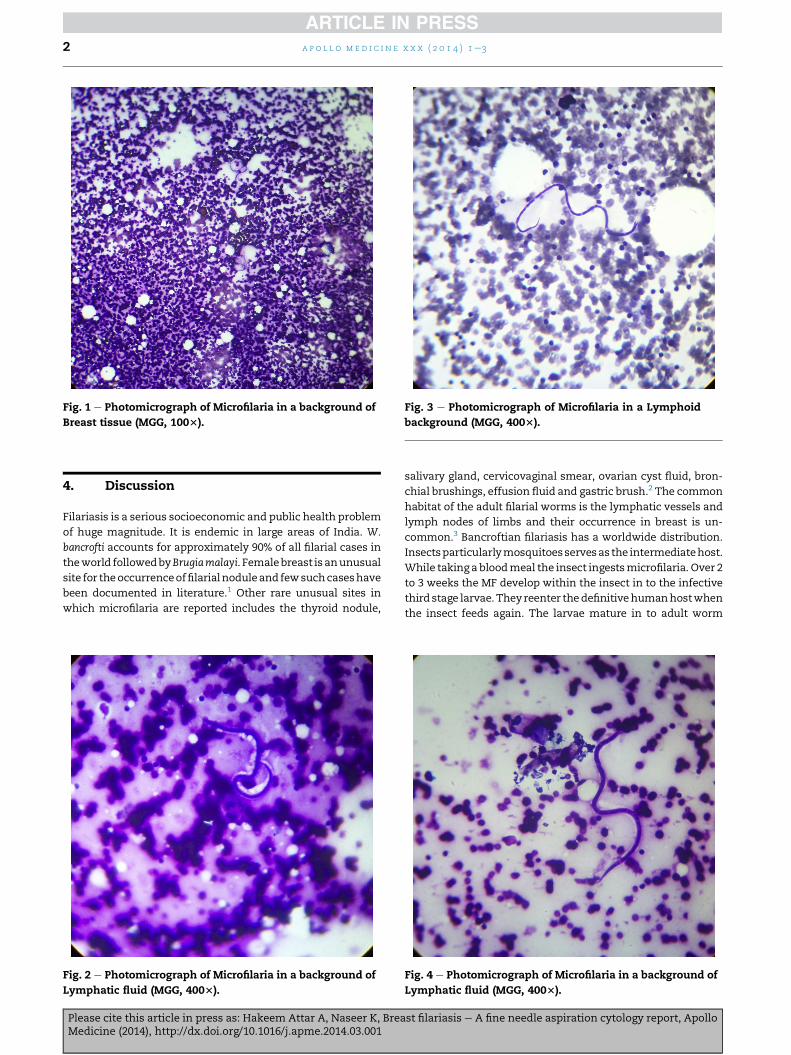
Fig. 1 e Photomicrograph of Microfilaria in a background of
Breast tissue (MGG, 1003).
Fig. 2 e Photomicrograph of Microfilaria in a background of
Lymphatic fluid (MGG, 4003).
Fig. 3 e Photomicrograph of Microfilaria in a Lymphoid
background (MGG, 4003).
Fig. 4 e Photomicrograph of Microfilaria in a background of
Lymphatic fluid (MGG, 4003).
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e32
Please cite this article in press as: Hakeem Attar A, Naseer K, Breast filariasis e A fine needle aspiration cytology report, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.03.001

which lives for 10 to 15 years and produces MF. The patient
usually presents with a solitary painless nodule in the upper
outer quadrant of the breast. Multiple lesions are uncommon.2
FNA has been employed to diagnose cases of breast involve-
ment. In the present case, an FNA smears yielded numerous
microfilarial worms.
5. Conclusion
To conclude FNA cytology appears to be more convenient and
effective diagnostic method in patients with mass lesion.
Demonstration and identification of the parasite in the smear
played a significant role in the prompt recognition of the dis-
ease and institution of specific therapy.
Conflicts of interest
All authors have none to declare.
Acknowledgements
The work was indeed a mammoth task to accomplish
and would not have been possible without active
co-operation, constant strategic support and encouragement
by our beloved e Dean e (ESIC Medical College Gulbarga)dDr.
S Chandrashekhar.
r e f e r e n c e s
1. Dayal A, Selvaraju Ka. Filariasis of the breast. Webmed CentSurg. 2010;1(11). WMC00942.
2. Singh NG, Chatterjee L. Filariasis of the breast, diagnosed byfine needle aspiration cytology. Ann Saudi Med.2009;29:414e415.
3. Rukmangadha N, Shanthi V, Kiran CM. Breast filariasisdiagnosed by fine needle aspiration cytology e a case report.Indian J Pathol Microbiol. 2006;49(2):243e244.
a p o l l o m e d i c i n e x x x ( 2 0 1 4 ) 1e3 3
Please cite this article in press as: Hakeem Attar A, Naseer K, Breast filariasis e A fine needle aspiration cytology report, ApolloMedicine (2014), http://dx.doi.org/10.1016/j.apme.2014.03.001

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/


















