
Financing PHC in Kazakhstan. 510 15 Switzerland Germany France Greece Portugal Malta Netherlands EU...
27
Financing PHC in Kazakhstan
-
Upload
matthew-riley -
Category
Documents
-
view
214 -
download
0
Transcript of Financing PHC in Kazakhstan. 510 15 Switzerland Germany France Greece Portugal Malta Netherlands EU...

Financing PHC in Kazakhstan

5 10
SwitzerlandGermany
FranceGreece
PortugalMalta
NetherlandsEU average
IsraelSweden
DenmarkItaly
NorwayNordic average
SloveniaUnited Kingdom
SpainCzech Republic
FinlandHungary
IrelandEUROPE
CSEC average Slovakia
LithuaniaEstonia
LatviaBelarusUkraine
CIS averageMoldova
UzbekistanKyrgyzstanKazakhstanAzerbaijan

Total and MCH Spending Per Capita 2002
0.05.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
50.0
East Kazakhstan Akmola Kzylorda South Kazakhstan
National EstimatePer Capita Spending (US$)
MCH Per Capita Spending (US$)

Regional Variation in Per capita spending (US$)
-20
-15
-10
-5
0
5
10
15
20
25
30
Man
gista
u
Kosta
nai
Wes
t Kaz
akhs
tan
Akmola
Almat
y City
Atyrau
Pavlod
ar
Astana
City
Repub
lic o
f Kaz
akhs
tan
East K
azak
hsta
n
Kyzyl-
Orda
North
Kaz
akhs
tan
Karag
anda
Aktobe
Sout K
azak
hsta
n
Zham
byl
Almat
y
Area
+/-
fro
m M
ean
P.C
. S
pend
ing
Dif from Mean

Structure of current local budgetinЫегксегку ща текущих расходовIn Akmola Oblast, health care, 2002, in %
49,1
3,810,9
2,6
5,2
4,7
25,9 Salary
Nutrition
Drugs
Suppliesинвентарь,Utilities
Building maintenance
Others

Main findings on the financing and budgeting study
• Resource allocation rules are not oriented to population health needs and risk of illness.
• Spending is not allocated to most cost-effective interventions.
• No clear budgeting rules across oblasts.
• Budget structure does not allow for the clear separation of primary care expenditures, versus secondary and hospital care.

Main findings on the financing and budgeting study
• No common budget structure across oblasts leads to difficulty in comparing spending.
• Capital spending is very low and is crowded out by spending on salaries and other spending.
• Spending on drugs is not standardized to a unique formulary and drug prices are not referenced.

What drives outcomes?

IMR and Spending
IMR vs. Per Capita Spending
R2 = 0.0029
-
5
10
15
20
25
30
35
40
45
0 5 10 15 20 25 30
IMR
Sp
end
ing
pe
r ca
pita
Spending per capita is not allocated according to need but has a small, positive impact on IMR.

MMR and Spending
MMR v. Per Capita Spending (US$)
-
5
10
15
20
25
30
35
40
45
0 20 40 60 80 100 120
MMR per 100,000
Per
Cap
ita S
pend
ing
(US
$)
…with similar results in terms of MMR and…

Does infrastructure matter?
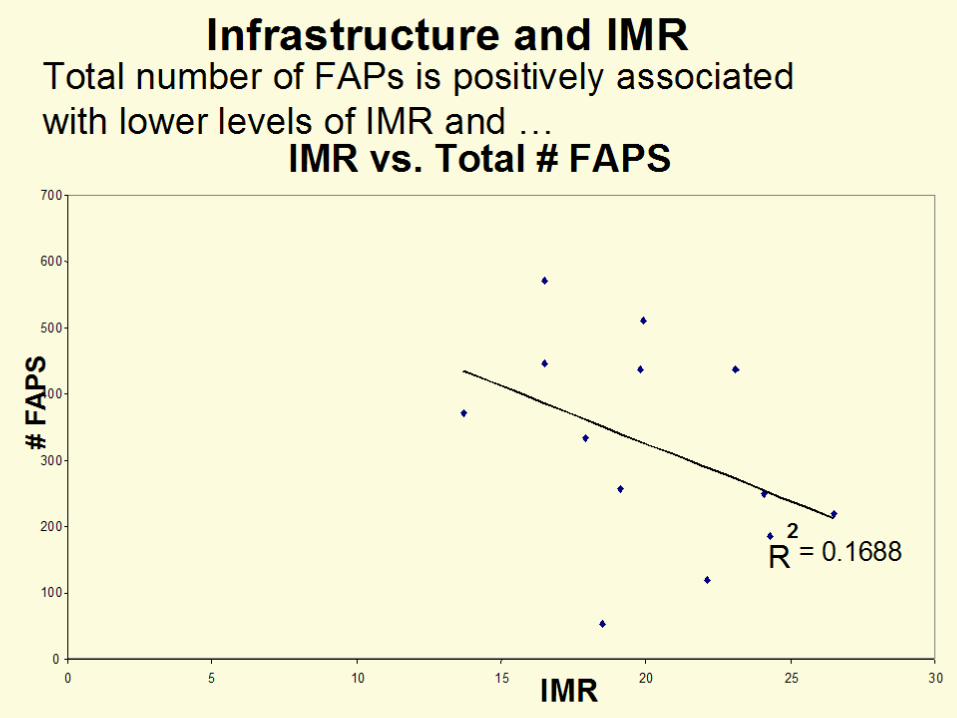
Infrastructure and IMR
IMR vs. Total # FAPS
R2
= 0.1688
0
100
200
300
400
500
600
700
0 5 10 15 20 25 30
IMR
# F
AP
S
Total number of FAPs is positively associated with lower levels of IMR and …

IMR and Medical/Obstetric Units
R2 = 0.1637
0
100
200
300
400
500
600
700
0 5 10 15 20 25 30
IMR
# U
nit
s

IMR vs. Beds per 10,000
R 2 = 0.0422
0
20
40
60
80
100
120
0 5 10 15 20 25 30IMR
Be
d / 1
0,0
00

Conclusions
• Outcomes appear to be linked to elements that improve access to MCH services (more FAPS and more obstetric units).
• Outcomes in IMR/MMR/Anemia are not linked to financing or to inputs. In some cases, outcomes are worse where inputs are greater.
• Improved outcomes depend on better access and quality of care.
• Resource allocation formulas should to take into account a population needs based formula.

Challenges to Health Systems: Conceptual Framework
Changes in:•Regulation•Financing- Pooling•Purchasing•Delivery Models
Health Status
Equity &Access
Effectiveness Quality
Financialsustainability
Efficiency &Productivity
Satisfaction
FinancialRisk
Protection
Social responsive
ness
Intermediate Goals Final GoalsMeansAA BB CC

Assessing overall performanceEquity and Access
• Distribution of funds not allocated according to population needs.
• Equity in outcomes is limited as a very small % of women in lowest income groups meet standards of care in key protocols
• In general people have access to health services…but…• Geographic access to well developed PHC is limited and
forces many rural people into hospitals as first line provider.
• Financial access is a problem. Out-of-pocket payments, many times in excess of a monthly salary, keep 20% of all patients from obtaining required medical care.
• Access to quality medical services in rural areas is impeded as years of under investment have eroded the technical capacity of providers.
Assessing overall performanceEffectiveness and Quality
• Observance of treatment protocols is limited. For example, only 50 % of all suspected cases of eclampsia had blood pressure taken.
• Over 50 percent of the 62 percent of neonatal deaths could be prevented.
• Many of the neonatal deaths are due to a problems in management of high risk births, lack of EOC or lack of timely access to PHC.
• Outcomes are limited by problems with the management of programs thereby limiting effectiveness.
• MOH should develop improved capacity to monitor and evaluate the use of protocols at all levels of system.
• Very little activity related to promotion. PHC focused on minor palliative care.

Assessing overall performanceFinancing and sustainability
• Overall level of financing health care in Kazakhstan is nearly the lowest in CAR and European countries.
• Most countries are spending over 5 percent of GDP• Maternal child health care services receive limited resources
for true PHC.• At current financing levels, it will be difficult to ensure access
to a cost effective basic package and improve existing technological stock.
• Problems with risk pooling create a serious financial burden for the population. While majority of the population pays only a small amount per visit, hospitalization is a catastrophic risk.
• Problems with budgetary structure and reporting that makes it difficult to estimate national health accounts and make policy decisions regarding allocation of funds.

Assessing overall performanceEfficiency and productivity• Overall trends in health status are not improving.• Hospitals do not appear to be operating efficiently in
terms of producing maximum output with minimum input.
• PHC services are not capturing patients in rural areas (at least 25% went directly to hospitals).
• Lack of solidarity in the financing model is highly inefficient at the macro level.
• Staff productivity is limited by a lack of equipment, drugs and supplies.
• There is very limited production and penetration on the key messages of the project or the health insurance fund.

Assessing overall performance
Satisfaction and community participation
• Satisfaction levels with care received are high (over 75% of all people very satisfied or satisfied with the doctor).
• Nurses receive similar rankings with respect to physicians.
• Very limited community participation in the oversight and planning associated with local government.
• Need to introduce more outreach programs—school health—to improve information and education.

RecommendationsTowards Strengthening PHC

Challenges to Health Systems: Conceptual Framework
Changes in:•Regulation•Financing-Pooling•Purchasing•Delivery Models
Health Status
Equity &Access
EffectivenessQuality
Financialsustainability
Efficiency &Productivity
Satisfaction
FinancialRisk Protection
Social responsiveness
Intermediate Goals Final GoalsMeansAA BB CC

Towards strengthening PHC
Regulation/policy• MOH has to strengthen regulation over the
quality of care. • Important role of private sector in provision of
drugs underscores the need for stronger regulation
• Seek initiatives to strengthen influence over direction of local governments
• Important standarize indicators across oblasts• Encourage benchmarking among providers and
Oblasts• Need to take an active role in health education.

Towards strengthening PHCFinancing• Introduce resource allocation formula that reflects
the population’s health needs and risks• Attempt to strengthen the capacity of PHC and
increase the per capita financing PHC/MCH• Link transfer of funds and introduce performance
based payment mechanisms that link funds to results.
• Efforts need to be made to reduce the financial burden for a basic package of services. This means that all services required to deliver the package are free of charge.
• Risk pooling at the national level is highly desireable.

Towards strengthening PHCPurchasing
• The introduction of the purchasing function critical to orient resources and actions in the sector.
• Purchasing orients funds towards the population’s priority health needs.
• Holds Oblasts and providers accountable for improvements in results.
• Introduces performance based payments.• Strong monitoring and evaluation function
related to productivity, quality and satisfaction.

Towards strengthening PHCDelivery Model
• Need to orient PHC services to priority health problems and to design package of services that meets the population’s health needs.
• This includes consultation, drugs, materials and all services NOT just one aspect.
• Examples of services organized around key population groups.
• Package of services includes entire spectrum of PHC; not just palliative and curative.
• Initiate disease management approach which integrates protocols across levels of care.
• Wider use of care guidelines in PHC.• Training in key areas to fill the knowledge gap.


















