Filed: March 3, 2015 UNITED STATES PATENT AND...
67
Filed: March 3, 2015 UNITED STATES PATENT AND TRADEMARK OFFICE ———————————————— BEFORE THE PATENT TRIAL AND APPEAL BOARD ———————————————— MYLAN PHARMACEUTICALS INC. Petitioner, v. YEDA RESEARCH & DEVELOPMENT CO. LTD. Patent Owner. ———————————————— Patent No. 8,969,302 ———————————————— PETITION FOR INTER PARTES REVIEW
-
Upload
trinhnguyet -
Category
Documents
-
view
215 -
download
1
Transcript of Filed: March 3, 2015 UNITED STATES PATENT AND...

Filed: March 3, 2015
UNITED STATES PATENT AND TRADEMARK OFFICE
————————————————
BEFORE THE PATENT TRIAL AND APPEAL BOARD
————————————————
MYLAN PHARMACEUTICALS INC.Petitioner,
v.
YEDA RESEARCH & DEVELOPMENT CO. LTD.Patent Owner.
————————————————Patent No. 8,969,302
————————————————
PETITION FOR INTER PARTES REVIEW
i
TABLE OF CONTENTS
I. INTRODUCTION .........................................................................................1
II. MANDATORY NOTICES ...........................................................................2
A. Real Parties-In-Interest (37 C.F.R. § 42.8(b)(1))..............................2
B. Related Matters (37 C.F.R. § 42.8(b)(2))...........................................2
C. Identification of Counsel (37 C.F.R. § 42.8(b)(3)) andService Information (37 C.F.R. § 42.8(b)(4)) ....................................3
D. Service Information (37 C.F.R. § 42.8(b)(4)) ....................................3
III. GROUNDS FOR STANDING......................................................................4
IV. IDENTIFICATION OF CHALLENGE AND STATEMENT OFTHE PRECISE RELIEF REQUESTED.....................................................4
V. THRESHOLD REQUIREMENT FOR INTER PARTESREVIEW.........................................................................................................5
VI. STATEMENT OF REASONS FOR THE RELIEF REQUESTED.........5
A. Summary of the Argument.................................................................5
B. Background of the ’302 Patent...........................................................7
1. The ’302 Patent..........................................................................7
2. The Prosecution of the ’302 Patent .......................................10
C. Level of Ordinary Skill in the Art ...................................................11
D. Claim Construction ...........................................................................12
E. Patents and Printed Publications Relied On In This Petition.......14
1. Pinchasi (Ex. 1005)..................................................................14
2. 1996 FDA SBOA (Ex. 1007A) ................................................15
3. Flechter 2002A (Ex. 1008) ......................................................17
4. Prior Art Informing the General Knowledge of thePOSA ........................................................................................18
F. Ground 1: Claims 1-3, 6-10 and 12 Are Anticipated byPinchasi...............................................................................................19
1. Independent Claim 1 Is Anticipated by Pinchasi.................19
2. Independent Claim 10 Is Anticipated by Pinchasi. .............22
3. Dependent Claims 2 and 12 Are Anticipated byPinchasi. ...................................................................................24

ii
4. Dependent Claim 3 Is Anticipated by Pinchasi....................24
5. Dependent Claims 6 and 7 Are Anticipated byPinchasi. ...................................................................................25
6. Dependent Claims 8 and 9 Are Anticipated byPinchasi. ...................................................................................26
G. Summary of Petitioner’s Obviousness Positions. ...........................27
1. The Law of Obviousness.........................................................27
2. The Prior Art Renders the Claims Obvious.........................32
a. Investigation into Different Dosing Protocolsfor GA Therapy.............................................................32
b. The Prior Art Motivated a Person of OrdinarySkill to Investigate Different Dosing Protocolsand Provided A Reasonable Expectation ofSuccess ...........................................................................35
H. Ground 2: Claims 1-12 Are Unpatentable As Obvious overPinchasi...............................................................................................40
1. Independent Claims 1 and 10 Are Obvious OverPinchasi. ...................................................................................40
2. Dependent Claim 2 Is Obvious Over Pinchasi. ....................43
3. Dependent Claim 3 Is Obvious Over Pinchasi. ....................43
4. Dependent Claims 6-9 and 12 Are Obvious OverPinchasi. ...................................................................................45
5. Dependent Claims 4-5 and 11 Are Obvious OverPinchasi. ...................................................................................45
I. Ground 3: Claims 1-12 Are Unpatentable As Obvious OverPinchasi in View of the 1996 SBOA.................................................46
1. Independent Claims 1 and 10 Are Obvious OverPinchasi in View of the 1996 FDA SBOA. ............................46
2. Dependent Claims 2-9 and 11-12 Are Obvious OverPinchasi in View of the 1996 FDA SBOA. ............................49
J. Ground 4: Claims 1-12 Are Unpatentable As Obvious overPinchasi in View of Flechter 2002A. ................................................50
1. Independent Claims 1 and 10 Are Obvious OverPinchasi in View of Flechter 2002A.......................................50

iii
2. Dependent Claims 2-9 and 11-12 Are Obvious OverPinchasi in View of Flechter 2002A.......................................51
K. Any Secondary Considerations Fail to Overcome theShowing of Obviousness....................................................................51
1. The Methods Recited in the ’302 Patent Produced NoUnexpected Results. ................................................................52
2. The ’302 Patent Satisfied No Long-Felt But UnmetNeed. .........................................................................................53
3. Copying By Generic Drug Makers Is Irrelevant. ................54

iv
LIST OF EXHIBITS
Exhibit No. Description
1001U.S. Patent No. 8,969,302, LOW FREQUENCYGLATIRAMER ACETATE THERAPY (filed February 19,2013) (issued March 3, 2015)
1002 File History for U.S. Patent No. 8,969,302
1003 Declaration of Stephen J. Peroutka, M.D., Ph.D.
1003A Curriculum Vitae of Stephen J. Peroutka, M.D., Ph.D.
1003B Materials Reviewed by Stephen J. Peroutka, M.D., Ph.D.
1004 Expert Declaration of Ari Green, M.D.
1004A Curriculum Vitae of Ari Green, M.D.
1004B Materials Reviewed by Ari Green, M.D.
1005Irit Pinchasi: International Publication No. WO2007/081975 (published July 19, 2007)
1006Cohen et al., Randomized, Double-Blind, Dose-ComparisonStudy of Glatiramer Acetate in Relapsing-Remitting MS,68:12 NEUROLOGY, 939-44 (2007)
1007 Affidavit of Marlene S. Bobka dated December 9, 2014
1007AJessop, Review and Evaluation of PharmacologyToxicology Data Original NDA Review (1996) (the 1996FDA SBOA) (attached as Exhibit A to Exh. 1007)
1008
Flechter et al., Copolymer 1 (Glatiramer Acetate) inRelapsing Forms of Multiple Sclerosis: Open MulticenterStudy of Alternate-Day Administration. 25:1 CLINICAL
NEUROPHARMACOLOGY, 11-15 (2002) (Flechter 2002A)
1009 Meiner et al., Copolymer 1 in Relapsing-Remitting Multiple

v
Exhibit No. Description
Sclerosis: A Multi-Centre Trial, in FRONTIERS IN MULTIPLE
SCLEROSIS: CLINICAL RESEARCH AND THERAPY (OdedAbramsky and Haim Ovadia, eds., 1997)
1010
Khan et al., Randomized, Prospective, Rater-Blinded, Four-Year, Pilot Study to Compare the Effect of Daily VersusEvery-Other-Day Glatiramer Acetate 20 mg SubcutaneousInjections in Relapsing-Remitting Multiple Sclerosis, 14MULTIPLE SCLEROSIS, S296 (2008)
1011
Caon et al., Randomized, Prospective, Rater-Blinded, FourYear Pilot Study to Compare the Effect of Daily VersusEvery Other Day Glatiramer Acetate 20 mg SubcutaneousInjections in RRMS, 72:11(3) NEUROLOGY, A317 (2009)
1012
Flechter et al., Comparison of glatiramer acetate
sclerosis patients: an open-label 2-year follow up, 197JOURNAL OF THE NEUROLOGICAL SCIENCES, 51-55 (2002).(“Flechter 2002B”)
1013Miller, The importance of early diagnosis of multiplesclerosis, 10(3) (Suppl. S-b) J. MANAG. CARE PHARM., S4-11 (2004)
1014Bornstein, Multiple Sclerosis: Trial of a SyntheticPolypeptide, 11:3 ANNALS OF NEUROLOGY, 317-19 (1982)
1015Bornstein et al., Clinical Trial of Copolymer I in MultipleSclerosis, 436 ANNALS NEW YORK ACADEMY OF SCIENCES,366-372 (1984)
1016Bornstein et al., A Pilot Trial of COP 1 in Exacerbating-Remitting Multiple Sclerosis, 317:7 THE NEW ENGLAND
JOURNAL OF MEDICINE, 408-14 (1987)
1017FDA, GUIDELINE FOR INDUSTRY: Dose-ResponseInformation to Support Drug Registration (1994)
1018 Johnson et al., Copolymer 1 reduces relapse rate and

vi
Exhibit No. Description
improves disability in relapsing-remitting multiplesclerosis, 43 NEUROLOGY, 1268-1276 (1995)
1019 Affidavit of Marlene S. Bobka dated January 5, 2015
1019A1996 FDA Meeting Agenda minutes from the Peripheraland Central Nervous System Drug Advisory Committee(dated September 19, 1996) (Exhibit A to Exhibit 1019)
1020 Arnon, The Development of Cop 1(Copaxone®), AnInnovative Drug for the Treatment of Multiple Sclerosis:Personal Reflections, 50 IMMUNOLOGY LETTERS 1-15(1996)
1021 Benet et al., Pharmacokinetics: The Dynamics of DrugAbsorption, Distribution, and Elimination, in THE
PHARMACOLOGICAL BASIS OF THERAPEUTICS, 3 (AlfredGoodman Gilman ed. 1996)
1022Lobel, et al., Copolymer-1, 21(2) DRUGS OF THE FUTURE,131-134 (1996)
1023
Haines et al., Linkage of the MHC to Familial MultipleSclerosis Suggests Genetic Heterogeneity. The MultipleSclerosis Genetics Group, HUM. MOL. GENET. 7:1229-34(Aug 1998)
1024U.S. Patent No. 6,342,476, Copolymer-1 Improvements inCompositions of Copolymers (2002).
1025Ge et al., Glatiramer Acetate (Copaxone) Treatment inRelapsing-Remitting MS: Quantitative MR Assessment, 54NEUROLOGY, 813-17 (2000)
1026
Comi et al., European/Canadian Multicenter, Double-Blind, Randomized, Placebo-Controlled Study of the Effectsof Glatiramer Acetate on Magnetic Resonance Imaging-Measured Disease Activity and Burden in Patients withRelapsing Multiple Sclerosis: European/CanadianGlatiramer Acetate Study Group, 49:3 ANN. NEUROL., 290-

vii
Exhibit No. Description
97 (2001)
1027
McDonald et al., Recommended Diagnostic Criteria forMultiple Sclerosis: Guidelines from the International Panelon the Diagnosis of Multiple Sclerosis, ANN. NEUROL.50:121-27 (2001)
1028McBride, Second International Multiple Sclerosis WeekMultiple Sclerosis, INT’L J. MS CARE 4:85 (2002)
1029Simpson, Adis Drug Evaluation Glatiramer Acetate – AReview of its use in Relapsing-Remitting Multiple Sclerosis,16:12 CNS DRUGS, 825-50, 834 (2002)
1030Edgar, et al., Lipoatrophy in Patients with MultipleSclerosis on Glatiramer Acetate, 31 CAN. J. NEUROL. SCI.,58-63 (2004)
1031
Ziemssen et al., Effects of Glatiramer Acetate on Fatigueand Days of Absence from Work in First-Time TreatedRelapsing-Remitting Multiple Sclerosis, HLTH. & QUAL.LIFE OUTCOMES 6:67 (2008)
1032Stuart, Clinical Management of Multiple Sclerosis: TheTreatment Paradigm and Issues of Patient Management, J.MANAGED CARE PHARMACY 10:S19-S25 (June 2004)
1033Bakshi et al., Imaging of Multiple Sclerosis: Role inNeurotherapeutics, 2(2) NEURORX, 277–303 (2005)
1034 Beringer et al., Clinical Pharmacokinetics andPharmacodynamics, in REMINGTON: THE SCIENCE AND
PRACTICE OF PHARMACY, 1191-1205, 1197, 1201 (PaulBeringer ed., 2005)
1035 Franklin et al., Drug Absorption, Action, and Disposition, inREMINGTON: THE SCIENCE AND PRACTICE OF PHARMACY,1142-1170, 1167 (Paul Beringer ed., 2005)
1036 James Rasmussen: International Patent Publication No. WO

viii
Exhibit No. Description
2005/120542 A2 (published December 22, 2005)
1037
Devonshire et al., The Global Adherence Project – AMulticentre Observational Study on Adherence to Disease-Modifying Therapies in Patients Suffering from Relapsing-Remitting Multiple Sclerosis, MULTIPLE SCLEROSIS 12:S1(P316) (2006)
1038
Ford et al., A Prospective Open-Label Study of GlatiramerAcetate: Over a Decade of Continuous Use in MultipleSclerosis Patients, 12 MULTIPLE SCLEROSIS, 309-320(2006)
1039Frohman, Multiple Sclerosis – The Plaque and itsPathogenesis, NEW ENGLAND J. MED. 354:942-55 (2006)
1040 Kragt et al., How Similar are Commonly Combined Criteriafor EDSS Progression in Multiple Sclerosis?, 12(6)MULTIPLE SCLEROSIS782-786 (2006)
1041Manso et al., Life Cycle Management of AgeingPharmaceutical Assets, 3:7 PHARMACEUTICAL LAW
INSIGHT, (2006)
1042
Soares et al., Localized Panniculitis Secondary toSubcutaneous Glatiramer Acetate Injections for theTreatment of Multiple Sclerosis: A Clinicopathologic andImmunohistochemical Study, J. AM. ACAD. DERM. 55:968-74 (2006)
1043Klauer and Zettl, Compliance, Adherence and theTreatment of Multiple Sclerosis, J. NEUROL. 255 [Suppl.6]:87-92 (2008)
1044
Pelidou et al., Multiple Sclerosis Presented as ClinicallyIsolated Syndrome: The Need for Early Diagnosis andTreatment, THER. CLIN. RISK MANAGEMENT 4:627-30 (June2008)

ix
Exhibit No. Description
1045Jacobs et al., Intramuscular interferon beta-1a therapyinitiated during a first demyelinating event in multiplesclerosis,” NEW ENGL. J. MED. 343:898-904 (2008)
1046 Teva Provides Update on Forte Trial Jerusalem, Israel(July 7, 2008)
1047 Copaxone® U.S. Product Label (2001)
1048 Betaseron® U.S. Product Label (2003)
1049 Rebif® U.S. Product Label (2003)
1050 Avonex® Product Label (2006)
1051 Tysabri® Product Label (2008)
1052 Copaxone® U.S. Product Label (Feb. 2009)
1053 Extavia® Product Label (2009)
1054 Rebif® Product Label (June 2005)
1055U.S. Patent No. Patent 3,849,550, THERAPEUTICCOPOLYMER (filed March 31, 1972) (issued November19, 1974)
1056U.S. Patent Publication No. 2009/0149541A1 (filed Nov.26, 2008)
1057Concepts in Clinical Pharmacokinetics, in INTRODUCTION
TO PHARMACOKINETICS AND PHARMACODYNAMICS, Tozerand Rowland eds (Lippincott Williams & Wilkins 2006)
1058Rich et al., Stepped-Care Approach to Treating MS: AManaged Care Treatment Algorithm, J. MANAGED CARE
PHARM. 10:S26-S32 (June 2004)
1059FDA GUIDANCE FOR INDUSTRY - POPULATION
PHARMACOKINETICS (1999)

x
Exhibit No. Description
1060U.S. Published Patent Application No. US 2013/0165387,LOW FREQUENCY GLATIRAMER ACETATE THERAPY(published June 27, 2013)

1
I. INTRODUCTION
Pursuant to 35 U.S.C. §§ 311-319 and 37 C.F.R. Part 42, Mylan
Pharmaceuticals Inc. (“Petitioner”) petitions for Inter Partes Review (“IPR”) of
claims 1-12 of U.S. Patent No. 8,969,302 to Klinger, titled “Low Frequency
Glatiramer Acetate Therapy” (“the ’302 patent,” Ex. 1001). Concurrently filed
herewith is a Power of Attorney pursuant to 37 C.F.R § 42.10(b). Pursuant to
37 C.F.R. § 42.103, the fee set forth in § 42.15(a) accompanies this Petition.
This Petition demonstrates that a preponderance of the evidence shows a
reasonable likelihood that claims 1-12 of the ’302 patent are unpatentable over the
prior art. Specifically, Teva, the commercial partner of Yeda for Copaxone®, in
2007 disclosed to the public in a published patent application to Irit Pinchasi (Ex.
1005) the claimed subject matter more than one year before Yeda filed its patent
application that led to the ’302 patent. This disclosure anticipates claims 1-3, 6-10
and 12 and renders all claims obvious to a person having ordinary skill in the art
(“POSA”) as of the priority date. All of the ’302 patent’s claims are alternatively
obvious over Pinchasi in view of either of two additional prior art publications: the
published Summary Basis of Approval for 20 mg Copaxone® (“the 1996 FDA
SBOA,” Ex. 1007A) or a 2002 article by Flechter et al. (Ex. 1008).

2
II. MANDATORY NOTICES
A. Real Parties-In-Interest (37 C.F.R. § 42.8(b)(1))
The real parties-in-interest for Petitioner are Mylan Pharmaceuticals Inc.,
Mylan N.V., Mylan Inc. and Mylan Teoranta.
B. Related Matters (37 C.F.R. § 42.8(b)(2))
Petitioner is not aware of any reexamination certificates or pending
prosecution concerning the ’302 patent.
While there is presently no litigation concerning the ’302 patent, Petitioner
is a defendant in the following litigations involving U.S. Patent No. 8,232,250
(“the ’250 patent”) and U.S. Patent No. 8,399,413 (“the ’413 patent”), two patents
in the same family as the ’302 patent: Teva Pharms. USA, Inc. v. Mylan Pharms.
Inc., 14-01278 (D. Del. Oct. 6, 2014); Teva Pharms. USA, Inc. v. Mylan Pharms.
Inc., 14-00167 (N.D. W. Va. Oct. 7, 2014). Other pending litigations involving the
’250 and ’413 patents include Teva Pharms. USA, Inc. v. Sandoz, Inc., No. 14-cv-
01171 (D. Del. Sept. 10, 2014); Teva Pharms. USA, Inc. v. Dr. Reddy’s Labs., No.
14-cv-01172 (D. Del. Sept. 10, 2014); Teva Pharms. USA, Inc. v. Dr. Reddy’s
Labs., No. 14-cv-05672 (D.N.J. Sept. 11, 2014); Teva Pharms. USA, Inc. v.
Synthon Pharms. Inc., No. 14-cv-01419 (D. Del. Nov. 18, 2014); Teva Pharms.
USA, Inc. v. Synthon Pharms., No. 14-cv-00975 (M.D.N.C. Nov. 19, 2014); and
Teva Pharms. USA, Inc. v. Amneal Pharms., LLC., No. 15-cv-00124 (D. Del. Feb.
3, 2015).

3
A patent application in the same patent family is pending as U.S. Patent
Application No. No. 14/630,326.
Petitions requesting inter partes review of the ’250 and ’413 patents were
previously filed. See IPR2015-00643 and IPR2015-00644, respectively.
C. Identification of Counsel (37 C.F.R. § 42.8(b)(3)) and ServiceInformation (37 C.F.R. § 42.8(b)(4))
Lead Counsel Back Up Counsel
Jeffrey W. Guise
(Reg. No. 34,613)
Wilson Sonsini Goodrich & Rosati
12235 El Camino Real, Suite 200
San Diego, CA 92130
Tel: (858) 350-2307
Fax: (858) 350-2399
Brandon M. White
(Reg. No. 52,354)
Perkins Coie LLP
700 13th St., NW, Suite 600
Washington, DC 20005
Tel: (202) 654-6206
Fax: (202) 654-9681
D. Service Information (37 C.F.R. § 42.8(b)(4))
Please direct all correspondence to lead counsel and back-up counsel at the
contact information above. Petitioner consents to service by electronic mail at

4
III. GROUNDS FOR STANDING
As required by 37 C.F.R. § 42.104(a), Petitioner certifies that the ’302 patent
is available for inter partes review and that the Petitioner is not barred or estopped
from requesting inter partes review on the grounds identified herein.
IV. IDENTIFICATION OF CHALLENGE AND STATEMENT OF THEPRECISE RELIEF REQUESTED
Petitioner requests inter partes review and cancellation of claims 1-12 of the
’302 patent under 35 U.S.C. §§ 102 and 103, as set forth herein. The ’302 patent is
to be reviewed under pre-AIA §§ 102 and 103. Petitioner’s detailed statement of
the reasons for the relief requested is set forth below in the section titled
“Statement of Reasons for Relief Requested.” In accordance with 37 C.F.R.
§ 42.6(c), copies of the exhibits are filed herewith. In addition, this Petition is
accompanied by the Declaration of Stephen J. Peroutka, M.D., Ph.D. (Ex. 1003)
and the Declaration of Ari Green, M.D. (Ex. 1004).
The challenged claims of the ’302 patent are generally directed to methods
of treating a relapsing form of multiple sclerosis (“MS”) by the administration of at
least “three subcutaneous injections of a 40 mg/ml dose of glatiramer acetate per
week.” Claims 1-12 of the ’302 patent are unpatentable based on the following
grounds:
Ground 1: Claims 1-3, 6-10 and 12 are anticipated by Pinchasi.
Ground 2: Claims 1-12 are obvious over Pinchasi.
5
Ground 3: Claims 1-12 are obvious over Pinchasi in view of the 1996 FDA
SBOA.
Ground 4: Claims 1-12 are obvious over Pinchasi in view of Flechter
2002A.
V. THRESHOLD REQUIREMENT FOR INTER PARTES REVIEW
A petition for inter partes review must demonstrate “a reasonable likelihood
that the petitioner would prevail with respect to at least 1 of the claims challenged
in the petition.” 35 U.S.C. § 314(a). This Petition meets this threshold. As
explained below, there is a reasonable likelihood that Petitioner will prevail with
respect to at least one of the challenged claims.
VI. STATEMENT OF REASONS FOR THE RELIEF REQUESTED
A. Summary of the Argument
Glatiramer acetate (“GA”) was first patented in 1974 as copolymer-1, U.S.
Patent No. 3,849,550 (“the ’550 patent”). Ex. 1003 ¶ 44. In the 1980s, Yeda
partnered with Teva to develop GA commercially and seek FDA approval to
market it, as Copaxone®, to treat MS. The FDA first approved Copaxone® for use
in treating MS in the U.S. in 1996 in a dosing regimen of 20 mg daily administered
by subcutaneous (“SC”) injection. In the 1990s, following the expiration of the
’550 patent and in preparation for the U.S. launch of 20 mg Copaxone®, Teva
sought additional U.S. patent protection and received patents on the GA compound
and on methods of making and using it. In 2013, with the last of the patents

6
covering Teva’s 20 mg daily dosage form ready to expire, Teva sought FDA
approval of a 40 mg, three times per week Copaxone® and upon FDA approval,
began to switch patients from the old, 20 mg daily product to its “new,” 40 mg
three times per week Copaxone®.
The ’302 patent is generally directed to “low frequency glatiramer acetate
therapy” and describes a method of treatment of a human patient suffering from a
relapsing form of MS. Ex. 1001 at Title, col. 2, ll. 51-61, and col. 3, ll. 6-14. In
general, the claims of the ’302 patent recite an open-ended method comprising
administration of 40 mg of GA SC at least three times per week to treat MS and,
for claims 4-5, with at least one day between each injection. Ex. 1001 at claims 1-
12. All claims, however, describe an MS treatment method that was already
known in, or obvious in view of, the prior art.
Before the earliest possible priority date (August 20, 2009), various GA
dosages and injection frequencies were tested and known. As explained in detail
below, a 2007 Teva patent application to Pinchasi (Ex. 1005) taught the
administration of 40 mg of GA every other day, anticipating claims 1-3, 6-10 and
12 of the ’302 patent under the broadest reasonable construction of the claims.
Moreover, all of the claims are obvious in light of the prior art, including
Pinchasi and others. A number of prior art references taught administering GA
every other day for inter alia improved patient compliance and adherence. See,

7
e.g., Ex. 1004 ¶¶ 52-57; see also Ex. 1003 ¶¶ 22-24, 55-63, 66-76. The prior art
also disclosed that no additional adverse side effects are associated with
administering 40 mg of GA per dose, as compared to 20 mg of GA per dose as had
been previously administered. Ex. 1004 ¶ 59 (citing Ex. 1005 at 19, ll. 8-14); Ex.
1003 ¶ 96, 113 (citing Ex. 1005 at 19, ll. 11-15). And so, in light of Pinchasi
alone, or in combination with other references detailed below, the claims of the
’302 patent were obvious at the time of the alleged invention.
B. Background of the ’302 Patent
1. The ’302 Patent
The ‘302 patent was filed on February 19, 2013 and claimed priority to
earlier patent applications. The ’302 patent names Ety Klinger as inventor and
Yeda Research & Development Co., Ltd. as assignee. The ’302 patent’s earliest
possible priority date is August 20, 2009.
The ’302 patent issued with 12 claims. Claims 1 and 10 are independent
claims. Independent claim 1 relates to “[a] method of treatment of a human patient
suffering from a relapsing form of multiple sclerosis.” The claimed method
includes the “administration to the human patient of three subcutaneous injections
of a 40 mg/ml dose of glatiramer acetate per week so as to treat the human
patient.” Independent claim 10 recites a similar method and includes additional
limitations directed to the pH, excipient content and volume of the GA

8
formulation, presence of the GA in a prefilled syringe, self-injection by a human
patient and the time interval between injections. As each independent claim
employs the open-ended transition “comprising,” the claims are not limited to only
three SC injections per week. Instead, the claim recitations after the transition
serve only to set the floor for the number of injections administered per week and,
in claim 10, a minimum time interval between such injections.
The dependent claims recite limitations directed to characteristics of the
disease (claims 2-3 and 12), that the method employs a pre-filled syringe, just like
prior art Copaxone® (claims 6-7), the pH of the product, again the same as prior art
Copaxone® (claims 8-9) and the days of the week the product can be administered
(claims 4-5 and 11).
The patent’s specification acknowledges that treating MS patients with GA
is not new. Ex. 1001 at col. 2, ll. 13-47. GA had been known for years to be a safe
and effective treatment for MS and had been FDA approved as a 20 mg daily
injection therapy for MS patients since 1996. Id. While the patent acknowledges
prior art Copaxone®, it fails to acknowledge the extensive body of prior art related
to alternate dosages and dosing schedules for treating MS with GA. See, e.g., Exs.
1005, 1006, 1007A, 1008, 1010, 1011. Much of this highly relevant prior art is
authored by Yeda, its commercial partner, Teva, or those working on their behalf.

9
The patent’s specification includes one example (col. 8, ll. 54 to col. 15, ll.
50), which, according to the Patent Owner, is prophetic (Ex. 1002 at [Interview
Summary], dated Dec. 9, 2014) and does not provide any actual in vitro or in vivo
data or data from a concluded human clinical trial to show safety or efficacy of the
claimed method. No unexpected results for GA are alleged in the patent. The
patent does not suggest that the claimed methods are more efficacious than prior
art methods, including daily administration of 20 mg Copaxone®. Instead, the
patent states only that “[t]reatment with 40 mg s.c. GA three times weekly is at
least as effective as 20 mg s.c. GA daily administration” for various clinical
endpoints. See, e.g., Ex. 1001 at col. 13, ll. 47 to col. 15, ll. 50. While the patent
generally alleges that “due to the complex pharmacokinetic behavior of a drug,
variation in the frequency of administration is unpredictable and requires empirical
testing,” no such empirical testing is included in the patent. See In re Paulsen,
30 F.3d 1475, 1481 n.9 (Fed. Cir. 1994) (noting the specification would not be
enabling if held to the same standard urged for the reference). Instead, the patent
cites an article addressing the unrelated interferon class of drugs without
correlating the stated proposition or the teachings of the article specifically to GA.
This article is immaterial especially when considered in light of the extensive prior
art disclosures of the many different safe and efficacious dosages and dosing
10
schedules for GA, ranging from 20 through 40 mg daily injections and from daily
to alternate day dosing regimens. See, e.g., Ex. 1003 ¶¶ 52-75; Ex. 1004 ¶¶ 58-78.
2. The Prosecution of the ’302 Patent
During prosecution, the Examiner issued a non-final office action rejecting
all claims. Ex. 1002 at 472-496. All of the claims were rejected on various
grounds under 35 U.S.C. § 112. Nearly all of the claims were rejected as
anticipated by or obvious. The Applicant attempted to traverse these rejections in
an Amendment. Ex. 1002 at 438-455. Applicant argued that its invention was
“drawn to a dosage regime,” but it did not amend the claims to incorporate such a
limitation.
A final rejection issued on February 5, 2014 finding the Applicant’s attempts
to traverse the rejections in the non-final office action unpersuasive and finally
rejecting all the claims on the same grounds. Ex. 1002 at 428-437. In an August 5,
2014 request for continued examination, the Applicant cancelled all pending
claims and added new claims 34-45, which eventually issued as claims 1-12. Ex.
1002 at 140-166. The Applicant responded to the outstanding rejections by, again,
arguing that the invention was drawn to a “dosage regime” without amending the
claims to incorporate such limitation. Ex. 1002 at 147.
On October 24, 2014, the Examiner issued a notice of allowance without
providing a statement of reasons for allowance or otherwise commenting on the

11
new claims added in the August 5, 2014 request for continuing examination. Ex.
1002 at 116-123.
C. Level of Ordinary Skill in the Art
The field of the invention relates to therapeutic methods of administering
GA. A POSA1 would have had several years of experience in the pharmaceutical
industry or in practicing medicine. See, e.g., Ex. 1003 ¶¶ 38-39; Ex. 1004 ¶¶ 27-
28. Such a person would have had experience with the administration or
formulation of therapeutic agents, dosing schedules and frequencies, and drug
developmental study and design. Ex. 1003 ¶ 39; Ex. 1004 ¶¶ 28. Such a person
would also have been well-versed in the world-wide literature that was available as
of the priority date. Ex. 1003 ¶ 39; Ex. 1004 ¶¶ -28. Such a person typically
would have been a Ph.D. in pharmacology (or a Pharm.D.) or a physician with
experience in clinical pharmacology. Ex. 1003 ¶ 39; see also Ex. 1004 ¶ 28. Such
person typically would have consulted with one or more members of a team of
experienced professionals in the pharmaceutical industry, including as one
example a physician with experience in clinical pharmacology. Ex. 1003 ¶ 39; see
also Ex. 1004 ¶ 28.
1 All references herein to the knowledge or understanding of a POSA or a POSA’s
interpretation or understanding of a prior art reference are as of the earliest possible
priority date unless specifically stated otherwise.

12
D. Claim Construction
The claims of the ’302 patent are presumed to take on the “broadest
reasonable construction in light of the specification of the patent in which it
appears.” 37 C.F.R. § 42.100(b); see also In re Cuozzo Speed Techs., LLC, No.
2014-31, 2015 WL 448667 (Fed. Cir. Feb. 4, 2015) (affirming the application of
the broadest reasonable construction standard in inter partes review). According
to the broadest reasonable construction, a POSA would understand the following
claim terms to have the following meanings.
Comprising. The independent claims of the ’302 patent use the open-ended
“comprising” transition. As a transition in a patent claim, “comprising” is
inclusive or open-ended and does not exclude additional, unrecited elements or
method steps. See, e.g., Invitrogen Corp. v. Biocrest Mfg., L.P., 327 F.3d 1364,
1368 (Fed. Cir. 2003) (“The transition ‘comprising’ in a method claim indicates
that the claim is open-ended and allows for additional steps.”); see also Medichem,
S.A. v. Rolabo, S.L., 353 F.3d 928, 933-34 (Fed. Cir. 2003) (claim that uses the
transition “comprising” “includes not only the steps listed in the claim, but also
any additional steps that may be added”); MPEP 2111.03 (collecting cases).
For example, in Gillette Co. v. Energizer Holdings Inc., 405 F.3d 1367,
1369, 1371-73 (Fed. Cir. 2005), the Federal Circuit held that a claim to “a safety
razor blade unit comprising a guard, a cap, and a group of first, second, and third
13
blades” encompasses razors with four blades because of the open-ended phrase
“comprising” in the preamble. “The word ‘comprising’ transitioning from the
preamble to the body signals that the entire claim is presumptively open-ended.”
Id. Here, as in Gillette, the claims are open ended and are thus not limited to
periodic administration of three and only three injections per week. Given their
broadest reasonable construction, the claims cover, e.g., the addition of a fourth
dose every other week, as occurs with alternate day dosing.
In determining “what is or is not excluded” by the transitional phrase
“comprising,” MPEP 2111.03, the only limitation on the claimed dosing schedule
in the independent claims is that there must be at least three injections per week
and, in claim 10, at least one day between each injection. Thus, the Patent
Owner’s choice to employ the transition “comprising” allows the claims to
encompass three or more subcutaneous injections per week. This includes every-
other-day dosing, in which three doses are administered during the first week and
four doses are administered during the second week.
“Per Week.” The independent claims of the ’302 patent use the term “per
week” to describe the rate at which the SC injections are administered. The phrase
“per week” defines a rate of administration and not a duration of treatment.
Nothing in the claims requires the injections to be continually administered over an
extended period of time. And, unlike the ’250 and ’413 patents, the claims of

14
the ’302 patent do not recite a “regimen” or otherwise provide any instruction to
the POSA that the method of treatment recited in the claims must extend beyond a
single week. Thus, the phrase “per week” in the context of the phrase “three
subcutaneous injections of a 40 mg/ml dose of glatiramer acetate per week” (claim
1) and “subcutaneous injection by the human patient of a 40 mg/ml dose of
glatiramer acetate three times per week” (claim 10) means the subcutaneous
injections are administered at a rate of at least three injections in a single week.
E. Patents and Printed Publications Relied On In This Petition
Petitioner relies on the following patents and printed publications:
1. Pinchasi (Ex. 1005)
Pinchasi discloses methods of treating MS and alleviating symptoms of a
patient suffering from a relapsing form of multiple sclerosis, which includes
relapsing-remitting multiple sclerosis (“RRMS”) by administering a
pharmaceutical composition comprising 40 mg of GA. See, e.g., Ex. 1005 at 1, l.
3, 1, l. 30-2, l. 2, l. 8, ll. 2-15 and 13, ll. 21-23; Ex. 1003 ¶ 18; Ex. 1004 ¶ 59.
Certain embodiments involve daily administration of this dosage, while other
embodiments involve every-other-day administration. See, e.g., Ex. 1005 at 8,
ll. 2-11. Pinchasi discusses experimental data demonstrating that daily injection of
40 mg (280 mg GA weekly) was safe and therapeutically effective. See, e.g., Ex.
1003 ¶¶ 70-74, 79-81; Ex. 1004 ¶ 59. Pinchasi’s data also formed the basis of the

15
Cohen 2007 article in Neurology, a preeminent peer-reviewed journal in the field
of neurology, which would have led a POSA to consider the data especially
persuasive and credible. Ex. 1003 ¶ 64-65; Ex. 1006. Treating MS patients using
both Pinchasi’s daily and alternate-day embodiments will have beneficial treatment
effects such as (among other things) the reduction in the mean cumulative number
of Gd-enhancing lesions and new T2 lesions in the brain of the patients. See, e.g.,
Ex. 1005 at 5, ll. 2-8, 8, ll. 2-15, 9, ll. 7-12; Ex. 1003 ¶¶ 78-82. A POSA would
understand that treating patients to provide these beneficial effects is the treatment
of MS. Ex. 1003 ¶ 73; Ex. 1004 ¶ 80.
As Pinchasi was published on July 19, 2007, more than one year before
the ’302 patent’s earliest possible priority date, it qualifies as prior art to the ’302
patent at least under pre-AIA 35 U.S.C. § 102(b).
2. 1996 FDA SBOA (Ex. 1007A)
In 1996, the FDA reviewed Teva’s new drug application (NDA) for 20 mg
daily Copaxone®. That document—the 1996 FDA SBOA—was disclosed to
Mylan (and so publicly available) more than one year prior to the earlier possible
priority date of the ’302 patent.2 The 1996 FDA SBOA explicitly encouraged less
2 Ex. 1007, Affidavit of Marlene S. Bobka dated December 9, 2014 attaching as
Ex. A, John J. Jessop, Review and Evaluation of Pharmacology Toxicology Data:
Original NDA Review (1996) (“the 1996 FDA SBOA”, Ex. 1007A).

16
frequent GA injections and provided half-life data demonstrating that Copaxone®
treatments with injections as infrequent as about 80 hours apart would be as
effective as daily injections. See Ex. 1003 ¶¶ 128-147. In particular, one FDA
reviewer stated that “it is unclear to me why it is necessary to inject the drug on a
daily basis. This dosing regimen seems like it would subject the patient to an
excessive amount of discomfort if it is not necessary to maintain efficacy.” Ex.
1007A at 121; Ex. 1003 ¶ 144. The reviewer “recommend[ed] that [Teva] evaluate
the necessity of daily s.c. [subcutaneous] injections as opposed to more infrequent
intermittent administration of the drug.” Ex. 1007A at 121; Ex. 1003 ¶ 144. The
1996 FDA SBOA therefore demonstrated the desirability and effectiveness of less
frequent GA injections while also defining a range of viable choices for those of
ordinary skill seeking to optimize the schedule. See Ex. 1003 ¶ 143-144.
To qualify as a printed publication within the meaning of § 102(b), a
reference “must have been sufficiently accessible to the public interested in the art”
before the critical date. In re Cronyn, 890 F.2d 1158, 1160 (Fed. Cir. 1989).
Public accessibility is based on the “facts and circumstances surrounding the
reference’s disclosure to members of the public.” In re Lister, 583 F.3d 1307,
1311 (Fed. Cir. 2009). A reference is considered publicly accessible if it is
disseminated or otherwise made available such that interested persons interested
and ordinarily skilled artisans, exercising reasonable diligence, can locate it. Id.
17
The 1996 FDA SBOA was publicly available at least as of July 17, 2007.
Ex. 1007, M. Bobka Affidavit (demonstrating availability to the public more than
one year before the priority date). As the 1996 FDA SBOA was publicly available
as a printed publication more than one year before the ’302 patent’s earliest
possible priority date (see Ex. 1007), it qualifies as prior art to the ’302 patent at
least under pre-AIA 35 U.S.C. § 102(b).
3. Flechter 2002A (Ex. 1008)
Flechter 2002A3 discloses alternate-day treatment of MS with 20 mg of GA.
Ex. 1003 ¶¶ 55-63; Ex. 1004 ¶¶ 63-64; Ex. 1008 at Abstract. In the study, MS
patients, including patients with RRMS, were switched from daily administration
of 20 mg to alternate-day administration of 20 mg GA. Ex. 1008 at 11-12. The
frequency of exacerbations (“relapse rate”) and Expanded Disability Status Scale
(“EDSS”) scoring endpoints were measured. Id. Using those endpoints, Flechter
2002A found similar efficacy rates with 20 mg daily and 20 mg alternate day
treatment. Id. at 15. Moreover, Flechter 2002A’s results indicated increased
compliance for patients treated with alternate day dosing—60.3% of patients
treated with alternate day dosing completed two years of treatment while only
3 Ex. 1008, Flechter et al. “Copolymer 1 (glatiramer acetate) in relapsing forms of
multiple sclerosis: Open multicenter study of alternate-day administration” Clin.
Neuropharm. 25:11-15 (2002) (“Flechter 2002A”).

18
39.7% of patients receiving daily treatment completed two years of treatment. Id.
at 15.
Given the similar efficacy of daily and alternate day dosing, Flechter 2002A
stated that “20 mg of Copolymer 1 on alternate days already has a maximal effect,
and daily injections are unnecessary.” Id. at 15. Therefore, Flechter 2002A
suggested that:
It is possible that the biologic effect of Copolymer 1 is not dose-
related but is related to the exposure of the immune system to its
presence by the continuity of administering the drug with
rechallenging the immune system, thus making daily injections
unnecessary.
Id. Thus, Flechter 2002A taught alternate day dosage of GA for MS patients,
including patients with relapsing forms of MS.
As Flechter 2002A was published in 2002, more than one year before
the ’302 patent’s earliest possible priority date (see Ex. 1008), it qualifies as prior
art to the ’302 patent at least under pre-AIA 35 U.S.C. § 102(b).
4. Prior Art Informing the General Knowledge of the POSA
In addition to the prior art discussed above, the declarations of Drs. Peroutka
and Green address additional publications confirming the general knowledge of a
POSA as of the priority date. These additional publications confirm that a POSA
would have recognized that reducing the number of injections per week would
19
increase patient adherence and compliance. See, e.g., Ex. 1003 ¶¶ 98-101, 107; Ex.
1004 ¶¶ 52-78; see also Ex. 1010; see also Ex. 1011. The additional publications
also confirm that as of the priority date a POSA would have recognized that
alternate day dosing would have equivalent efficacy to a 20 mg daily dose of GA.
See Ex. 1003 ¶¶ 121-126, 149-154; Ex. 1004 ¶¶ 65-72; see also Ex. 1008 at 11; see
also Ex. 1006 at 941-944.
F. Ground 1: Claims 1-3, 6-10 and 12 Are Anticipated by Pinchasi.
1. Independent Claim 1 Is Anticipated by Pinchasi.
Claim 1 recites an open-ended method for treating MS using GA that
includes the following elements:
a preamble reciting “[a] method of treatment of a human patient
suffering from a relapsing form of multiple sclerosis,”
the administration of “three subcutaneous injections of a 40 mg/ml
dose of glatiramer acetate per week,” and
administration “so as to treat the human patient.”
As explained below, Pinchasi expressly discloses each element of claim 1. See Ex.
1003 ¶¶ 77-82; Ex. 1004 ¶¶ 79-86.
Pinchasi discloses the preamble: As a threshold matter, Mylan does not
concede that the preamble of claim 1 is limiting rather than simply as statement of
intended use. Regardless, Pinchasi expressly discloses the preamble of claim 1.
20
The preamble of claim 1 recites a “method of treatment of a human patient
suffering from a relapsing form of multiple sclerosis.” Pinchasi discloses a method
of treating a patient suffering from relapsing forms of MS. Pinchasi disclosed that
the invention is a method of treating MS and is to “provide[] a method of
alleviating a symptom of a patient suffering from a relapsing form of multiple
sclerosis.” Ex. 1005 at 1, l. 3, 8, ll. 2-4. A POSA would understand the teaching
of alleviation of symptoms of MS to be the treatment of MS. Ex. 1003 ¶ 78; Ex.
1004 ¶ 80. Pinchasi thus discloses a “method of treatment of a human patient
suffering from a relapsing form of multiple sclerosis” as recited in the preamble of
claim 1. Ex. 1003 ¶¶ 78, 82; Ex. 1004 ¶ 80.
Pinchasi discloses the administration step: Pinchasi discloses each aspect
of the open-ended method of claim 1, including “administration to the human
patient of three subcutaneous injections of a 40 mg/ml dose of glatiramer acetate
per week.” See Ex. 1003 ¶¶ 79-81; Ex. 1004 ¶¶ 81-85.
First, with respect to the dose amount, Pinchasi discloses “periodically
administering to the patient by subcutaneous injection a single dose of a
pharmaceutical composition comprising 40 mg of [GA] so as to thereby alleviate
the symptom of the patient.” Ex. 1005 at 5, ll. 2-8.
Second, with respect to the dose schedule, Pinchasi discloses “periodically
administering . . . a single dose of a pharmaceutical composition comprising 40 mg

21
of [GA]” and states that “the periodic administration is every other day” in one
specifically disclosed embodiment. Id. at 8, ll. 2-11. Pinchasi’s disclosure of the
administration of 40 mg of GA on an every-other-day basis discloses providing at
least “three subcutaneous injections” of that dose per week. Ex. 1003 ¶¶ 77, 79-81;
Ex. 1004 ¶¶ 81-85. Injecting 40 mg GA “every other day” (as Pinchasi discloses)
results in administration of that drug that alternates between three and four
injections per week with at least one day between injections, which necessarily
results in at least three subcutaneous injections per week. Ex. 1003 ¶¶ 79-81; Ex.
1004 ¶¶ 81-82. While Pinchasi’s dosing schedule may result in four injections per
week one week and three injections the next, claim 1 does not exclude this
schedule, and indeed encompasses it because “comprising” is an open-ended term.
See, e.g., Invitrogen, 327 F.3d at 1368. As previously explained, claim 1 does not
exclude additional, unrecited elements or method steps, and thus encompasses
Pinchasi’s one additional injection every other week. Accordingly, Pinchasi
discloses the administration step of claim 1. Ex. 1003 ¶¶ 77-82; Ex. 1004 ¶ 81.
See, e.g., Gillette, 405 F.3d at 1371-73.
Pinchasi discloses that the administration is “to treat the human patient”:
Pinchasi discloses that its administration of GA is to treat the human patient.
Pinchasi is titled “Method of Treating Multiple Sclerosis.” Ex. 1005 at 1, l. 3.
Pinchasi also states that the administration of GA according to its teachings
22
“reduces a symptom of MS [including] the frequency of relapses.” Ex. 1005 at 9,
ll. 13-17. A POSA would understand that the disclosure that Pinchasi’s GA
administration results in the reduction of the symptoms of MS is the treatment of
MS. Ex. 1003 ¶ 82; Ex. 1004 ¶ 80; see In re Baxter Travenol Labs., 952 F.2d 388
(Fed. Cir. 1991) (holding that an invention requiring a blood bag system
incorporating a bag containing DEHP, an additive to the plastic which improved
the bag’s red blood cell storage capability was anticipated by a prior art reference
that disclosed only a blood bag because extrinsic evidence established that a POSA
would understand that prior art’s use of the term “blood bag” to include blood bags
with DEHP). Accordingly, Pinchasi expressly discloses an administration of GA
that is, as recited in claim 1, “so as to treat the human patient.”
* * * *
Accordingly, at least for the reasons discussed above, Pinchasi discloses
each element of claim 1 of the ’302 patent and this claim is unpatentable as
anticipated. Ex. 1004 ¶¶ 79-86; Ex. 1003 ¶¶ 77-82.
2. Independent Claim 10 Is Anticipated by Pinchasi.
Independent claim 10 is similar to claim 1, except that claim 10 requires that
“subcutaneous injection by the human patient of a 40 mg/ml dose of glatiramer
acetate three times per week with at least one day between every subcutaneous
injection.” Claim 10 thus requires that the human patient administer the SC

23
injection and that there is at least one day between such injections. Claim 10 also
requires that the GA is present in l ml of a mannitol-containing pharmaceutical
composition with a pH in the range of 5.5 to 7.0 and in a prefilled syringe for self
injection by the human patient. Pinchasi discloses each of these elements.
Pinchasi discloses that the composition of 40 mg for injection “is a
solution containing [a] dose of 40 mg of the drug substance and 40 mg
of Mannitol USP in 1 mL sterilized water for injection.” Ex. 1005 at
13, ll. 21-24, Example 1; Ex. 1004 ¶ 88; Ex. 1003 ¶ 84.
Pinchasi also discloses that “the pharmaceutical composition is in a
prefilled syringe and is self-administered by the patient.” Ex. 1005 at
8, ll. 24-26; Ex. 1004 ¶ 88; Ex. 1003 ¶ 84.
Pinchasi further discloses that its pharmaceutical formulations have a
pH between 5.5 and 7.0. Ex. 1005 at 8, ll. 21-23 (“[i]n an
embodiment, the pharmaceutical composition has a pH in the range of
5.5 to 7.0”); Ex. 1004 ¶ 88; Ex. 1003 ¶ 84.
Pinchasi claim 10 shows that this combination of features in a single
embodiment; Ex. 1005 at 21-22.
Accordingly, at least for the reasons discussed above with respect to claim 1
and for the additional reasons discussed here, Pinchasi discloses each element of

24
claim 10 and this claim is unpatentable as anticipated. Ex. 1003 ¶¶ 77-84; Ex.
1004 ¶ 87-89.
3. Dependent Claims 2 and 12 Are Anticipated by Pinchasi.
Dependent claims 2 and 12 depend from claims 1 and 10, respectively.
These claims recite that “the human patient is suffering from relapsing-remitting
multiple sclerosis.” To the extent these claims further narrow claims 1 and 10, as
shown in the claim chart below, Pinchasi teaches this element. Accordingly,
Pinchasi anticipates claim 2 and 12 for the reasons stated above with respect to
claims 1 and 10 in view of these further disclosures of Pinchasi. Ex. 1004 ¶ 90;
Ex. 1003 ¶¶ 85.
Claim Disclosure in Pinchasi2. The method of claim 1,wherein the human patient issuffering from relapsing-remitting multiple sclerosis.
Pinchasi discloses that the human patientadministered GA is suffering from a “relapsingform of multiple sclerosis [that] is relapsing-remitting multiple sclerosis.” Ex. 1005 at 8, ll. 2-13.
12. The method of claim 10,wherein the human patient issuffering from relapsing-remitting multiple sclerosis.
See claim 2.
4. Dependent Claim 3 Is Anticipated by Pinchasi.
Dependent claim 3 depends from claim 1. The claim recites that “the
human patient has experienced a first clinical episode and has MRI features
consistent with multiple sclerosis.”
Pinchasi discloses a method of treating a patient that is suffering from a

25
relapsing form of MS. Ex. 1005 at 8, ll. 2-13. The recitation in claim 3 that
“human patient has experienced a first clinical episode and has MRI features
consistent with multiple sclerosis” would have been understood by a POSA to
indicate that the human patient has clinically isolated syndrome (“CIS”). Ex.
1003 ¶¶ 86-87; Ex. 1004 ¶¶ 42, 91-92. CIS, along with RRMS, were both known
to POSAs to be relapsing forms of MS. Ex. 1004 ¶42. A POSA would have
understood Pinchasi’s disclosure of a method of treating a patient suffering from a
relapsing form of MS to include patient with CIS, i.e., a “human patient has
experienced a first clinical episode and has MRI features consistent with multiple
sclerosis”. Ex. 1003 ¶¶ 86, 89; Ex. 1004 ¶¶ 42, 91-92.
Accordingly, Pinchasi anticipates claim 3 for the reasons stated above with
respect to claim 1 in view of these further disclosures of Pinchasi. Ex. 1004
¶¶ 91-92; Ex. 1003 ¶¶ 89-90.
5. Dependent Claims 6 and 7 Are Anticipated by Pinchasi.
Dependent claims 6 and 7 depend from claims 2 and 3, respectively. Both
claims recite that “the glatiramer acetate is present in l ml of a pharmaceutical
composition in a prefilled syringe for self administration by the human patient.”
As shown in the claim chart below, Pinchasi teaches this element. Accordingly,
Pinchasi anticipates claims 6 and 7 for the reasons stated above with respect to

26
claims 2 and 3 in view of these further disclosures of Pinchasi. Ex. 1004 ¶ 93; Ex.
1003 ¶¶ 91.
Claims Disclosure in Pinchasi6. The method of claim 2,wherein the glatiramer acetateis present in l ml of apharmaceutical compositionin a prefilled syringe for selfadministration by the humanpatient.
Pinchasi discloses that the 40 mg GApharmaceutical composition administered “is in aprefilled syringe and is self-administered by thepatient.” Ex. 1005 at 22, ll. 3-5.
Pinchasi also discloses that the 40 mg GApharmaceutical composition administered “is asolution containing [a] dose of 40 mg of the drugsubstance and 40 mg of Mannitol USP in 1 mLsterilized water for injection.” Ex. 1005 at 13, ll.21-24, Example 1.
7. The method of claim 3,wherein the glatiramer acetateis present in l ml of apharmaceutical compositionin a prefilled syringe for selfadministration by the humanpatient.
See claim 6.
6. Dependent Claims 8 and 9 Are Anticipated by Pinchasi.
Dependent claims 8 and 9 depend from claims 6 and 7, respectively. Both
claims recite that “the pharmaceutical composition further comprises mannitol and
has a pH in the range of 5.5 to 7.0.” As shown in the claim chart below, Pinchasi
teaches this element. Accordingly, Pinchasi anticipates claims 8 and 9 for the
reasons stated above with respect to claims 1-3 and 6-7 in view of these further
disclosures of Pinchasi. Ex. 1004 ¶ 94; Ex. 1003 ¶ 92.
27
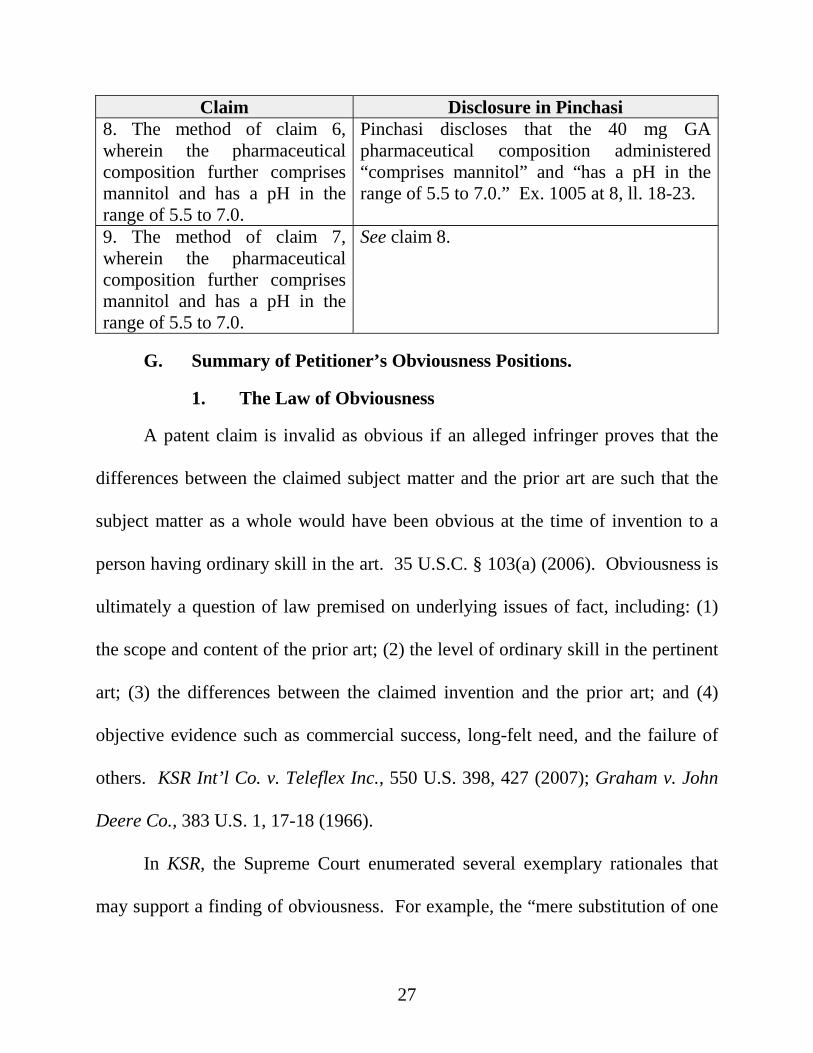
Claim Disclosure in Pinchasi8. The method of claim 6,wherein the pharmaceuticalcomposition further comprisesmannitol and has a pH in therange of 5.5 to 7.0.
Pinchasi discloses that the 40 mg GApharmaceutical composition administered“comprises mannitol” and “has a pH in therange of 5.5 to 7.0.” Ex. 1005 at 8, ll. 18-23.
9. The method of claim 7,wherein the pharmaceuticalcomposition further comprisesmannitol and has a pH in therange of 5.5 to 7.0.
See claim 8.
G. Summary of Petitioner’s Obviousness Positions.
1. The Law of Obviousness
A patent claim is invalid as obvious if an alleged infringer proves that the
differences between the claimed subject matter and the prior art are such that the
subject matter as a whole would have been obvious at the time of invention to a
person having ordinary skill in the art. 35 U.S.C. § 103(a) (2006). Obviousness is
ultimately a question of law premised on underlying issues of fact, including: (1)
the scope and content of the prior art; (2) the level of ordinary skill in the pertinent
art; (3) the differences between the claimed invention and the prior art; and (4)
objective evidence such as commercial success, long-felt need, and the failure of
others. KSR Int’l Co. v. Teleflex Inc., 550 U.S. 398, 427 (2007); Graham v. John
Deere Co., 383 U.S. 1, 17-18 (1966).
In KSR, the Supreme Court enumerated several exemplary rationales that
may support a finding of obviousness. For example, the “mere substitution of one

28
element for another known in the field” to “yield a predictable result” may support
a finding of obviousness. Id. at 416 (citation omitted). The Court also explained
that obviousness may be shown if it was “obvious to try”: “When there is a design
need or market pressure to solve a problem and there are a finite number of
identified, predictable solutions, a person of ordinary skill in the art has good
reason to pursue the known options within his or her technical grasp. If this leads
to the anticipated success, it is likely the product not of innovation but of ordinary
skill and common sense.” Id. at 421 (emphasis added).
The Federal Circuit has frequently invalidated as obvious patents that seek to
claim modified dosing protocols for prior art drugs. For example, the Federal
Circuit recently affirmed a district court’s grant of summary judgment of
obviousness of two patents that claimed a single monthly dose of 150 mg of the
drug risedronate, which belongs to a class of pharmaceutical compounds called
bisphosphonates. See Warner Chilcott Co. v. Teva Pharms. USA, Inc., Nos. 2014-
1439, 1441, 1444-46, 2014 WL 6435042 (Fed. Cir. Nov. 18, 2014). That case is
strikingly similar to this one. There, the prior art products included
bisphosphonates dosed at 5 mg daily, and one bisphosphonate dosed at 35 mg
weekly. The prior art daily dosed products were known to cause irritation to
mucous membranes and significant adverse esophageal and gastrointestinal side
effects, which resulted in noncompliance issues with patients on the daily

29
regimens. Those problems were only somewhat alleviated by weekly dosing of
bisphosphonates. See id. at *1.
In affirming the invalidity of these patents, the Federal Circuit held that the
district court correctly determined that the cited prior art references disclosed or
suggested each limitation, and provided both motivation to pursue the claimed
monthly regimen and a reasonable expectation of success in doing so. Id.
According to the Federal Circuit, the district court correctly found that the prior art
suggested less frequent dosing schedules and also established a reasonable
expectation that once-monthly dosing of risedronate could successfully treat
osteoporosis. The Federal Circuit found that “[a]s longer dosing intervals suit
patient convenience and compliance, the prior art therefore provided express
motivation to pursue a monthly dosing regimen.” Id. at *5.
The patent owner argued that uncertainty as to the safety and efficacy of a
once monthly 150 mg dosing protocol precluded a finding of obviousness. The
Federal Circuit flatly rejected that argument, holding that a “[w]hile it is true that,
as of [the priority date], the highest single dose of risedronate that had actually
been tested in a patient was 50 mg, obviousness does not require absolute certainty
or a guarantee of success.” Id. at *6. As for the patent owner’s evidence of
secondary considerations of non-obviousness, including an alleged long-felt need
30
for, and skepticism of others toward, the claimed dosing regimen, the court found
that “lack of certainty does not preclude a conclusion of obviousness.” Id.
Warner Chilcott is not an outlier. The Federal Circuit reached a similar
conclusion in Hoffmann-La Roche Inc. v. Apotex Inc., 748 F.3d 1326 (Fed. Cir.
2014), where it invalidated as obvious over other patents related to modified
dosing protocols for a similar pharmaceutical product. Along the way, the court
noted that “[c]onclusive proof of efficacy is not necessary to show obviousness,”
and held that the claimed dosing regimen in the invalidated patents was “obvious
to try: There was a need to solve the problem of patient compliance by looking to
less-frequent dosing regimens.” Id. at 1331-32; see also In re Kubin, 561 F.3d
1351, 1357 (Fed. Cir. 2009) (“Even if no prior art of record explicitly discusses the
[limitation], the [patent applicant’s] application itself instructs that [the limitation]
is not an additional requirement imposed by the claims . . . but rather a property
necessarily present in the [claimed invention].”).
The Board itself has reached a similar conclusion. In Biomarin
Pharmaceutical Inc. v. Genzyme Therapeutic Products Ltd. Partnership, the Board
held that a patent claiming “[a] method of treating a human patient with Pompe’s
disease, comprising intravenously administering biweekly to the patient a
therapeutically effective amount of human acid alpha glucosidase, whereby the
concentration of accumulated glycogen in the patient is reduced and/or further

31
accumulation of glycogen is arrested” to be obvious. Biomarin Pharm. Inc. v.
Genzyme Therapeutic Prods. Ltd. P’ship, Final Written Decision, Paper No. 81,
IPR 2013-00534, at 11-18 (PTAB 2015). The Board found that biweekly
administration as claimed was “routine optimization” that would have been
obvious to one of ordinary skill in the art “achievable through the use of standard
clinical trial procedures” even in the absence of human clinical trials and where the
POSA could not have predicted with absolute certainty the safe and effective
dosing regimen for the drug. Id. at 12-14. The Board concluded that
the experimentation needed to achieve biweekly administration
recited in claim 1 was “‘nothing more than the routine’ application of
a well-known problem-solving strategy, . . . ‘the work of a skilled
[artisan], not of an inventor.’” Pfizer, Inc. v. Apotex, Inc., 480 F.3d
1348, 1368 (Fed. Cir. 2007) (quoting Merck & Co. v. Biocraft Labs.,
Inc., 874 F.2d 804, 809 (Fed. Cir. 1989); DyStar Textilfarben GmbH
& Co. Deutschland KG v. C.H. Patrick Co., 464 F.3d 1356, 1371
(Fed. Cir. 2006)); see also In re Aller, 220 F.2d 454, 456 (CCPA
1955) (“[W]here the general conditions of a claim are disclosed in the
prior art, it is not inventive to discover the optimum or workable
ranges by routine experimentation.”); In re Boesch, 617 F.2d 272, 276
(CCPA 1980) (“[D]iscovery of an optimum value of a result effective
variable in a known process is ordinarily within the skill of the art.”).
The motivation to optimize the therapy disclosed in [the primary prior
art reference] “flows from the ‘normal desire of scientists or artisans
to improve upon what is already generally known.’” Pfizer, 480 F.3d

32
at 1348 (quoting In re Peterson, 315 F.3d 1325, 1330 (Fed. Cir.
2003)).
Id. at 14. The Board similarly held that “[t]he fact that a suggested dose (as taught
in [the primary prior art reference]) and dosing schedule had not been established
yet as safe and effective in human clinical trials at the time of invention does not
demand a conclusion of nonobviousness.” Id. at 15. Similar to the facts in the
present Petition, the Board recognized that in the Biomarin petition “all that
remained to be achieved over the prior art was the determination that a specific
dose within a previously suggested dose range, and its corresponding dosing
schedule, would have been safe and effective for the treatment of human patients.
That is, this is not a case where the prior art teaches merely to pursue a general
approach that seemed to be a promising field of experimentation or gave only
general guidance as to the particular form of the claimed invention or how to
achieve it. Id. (internal quotations omitted).
2. The Prior Art Renders the Claims Obvious
a. Investigation into Different Dosing Protocols for GATherapy
It has long been known that that the prior art dosing protocol of 20 mg
Copaxone® administered daily was “rather arbitrarily selected.” Ex. 1008 at 11.
Persons of skill in the art had extensive interest in optimizing the dosing protocol

33
for Copaxone® and, as discussed in the next section, had more than ample reason to
do so.
The POSAs would have been familiar with many investigations of different
dosing protocols for the treatment of MS with GA. These investigations studied
different dose amounts and different dosing schedules and combinations thereof.
For example, several studies examined administering 20 mg of GA to RRMS
patients every other day. One study examined a 40 mg daily dose. Each study
reported encouraging results. These studies, and other patents and printed
publications in the prior art, informed a POSA of at least the following
foundational facts, each well known to a POSA as of the priority date and each of
which would have informed their development of improved treatment protocols:
The half-life of GA was greater than 80 hours and therefore did not require
daily administration. See Ex. 1007A at 66; Ex. 1003 ¶¶ 140-144;
A POSA would have known that patients universally preferred dosing
schedules for GA treatment that required less frequent injections. See Ex.
1003 ¶ 99 and Ex. 1004 ¶¶ 64-67, both discussing Khan 2008 (in study of
daily vs. every-other-day 20 mg Copaxone® injections, “[a]fter 2 years, all
patients in the [daily] group opted to switch to [every other day]”);
The administration of a 40 mg daily injection of GA did not create any
safety or tolerability concerns as compared to the daily administration of 20

34
mg GA. See, e.g., Ex. 1005 at 19, ll. 8-14 (“The increased efficacy observed
with 40 mg/day GA … is not accompanied by a corresponding increase of
adverse reactions which would be expected upon a doubling of the
administered dose.”);
That 40 mg GA administered daily was safe and effective. See, e.g., Ex.
1005 at 19, ll. 8-14; Ex. 1006 at 939 (Abstract) (“Glatiramer Acetate (GA)
40 mg was safe and well tolerated. The overall efficacy results suggested
that a 40-mg dose of GA may be more effective than the currently approved
20-mg daily dose in reducing MRI activity and clinical relapse.”);
Patient adherence and compliance for chronic therapies, a serious concern in
the art, is improved with less frequent and more convenient dosing
protocols. See, e.g., Ex. 1010 (noting that “[t]here is considerable interest in
alternate dosing regimens of GA in RRMS. Daily SC injectable therapy can
be challenging for long-term patient compliance,” and finding that “[a]fter 2
years, all patients in the [daily] group opted to switch to [every other day]”).
Here, the Patent Owner may be expected to argue that the difference
between the claimed invention and the prior art is the difference between an every-
other-day 40-mg dosing schedule (as disclosed in Pinchasi) and a 40-mg dosing
schedule that requires exactly three injection per week period with one day
between each injection. While Petitioner does not believe there are any differences

35
between the prior art and the clamed invention, even taking the scenario most
favorable to the Patent Owner, this amounts to just one additional injection in
Pinchasi’s administration every other week as compared to the administration in
some of the ’302 patent claims. That is, the disclosure of Pinchasi is a dosing
schedule that alternates between 3 injections per week with at least one day in
between injections and 4 injections per week with at least one day in between
injections.
b. The Prior Art Motivated a Person of Ordinary Skillto Investigate Different Dosing Protocols andProvided A Reasonable Expectation of Success
Armed with this extensive knowledge of GA therapy, a POSA as of the
priority date would be motived to devise the dosing schedule of the ’302 patent and
would have a reasonable expectation of success in doing so.
First, a POSA would have been motivated to either alter Pinchasi alone
(which discloses 40 mg alternate day administration), or combine it with another
reference (disclosing similar alternate day dosing regimens), with a goal of
lowering the number of injections a patient must endure and thus optimizing
patient adherence and compliance. Pinchasi stressed the efficacy, tolerability and
safety of daily injections of 40 mg GA in its clinical studies, finding that the onset
of action with 40 mg GA was more rapid as compared to 20 mg GA treatment. See
Ex. 1005 at 19, ll. 8-14. Moreover, this increased efficacy was seen in the absence

36
of an increase in injection site reactions with 40 mg GA administration. Ex. 1005
at 19, ll. 8-14; Ex. 1004 at ¶¶ 59, 98-100; Ex. 1003 ¶¶ 74, 96, 113. Pinchasi
demonstrated that the occurrence of injection site reactions in patients treated with
40 mg GA daily was the same as, if not slightly less, than treatment with 20 mg
daily. See, e.g., Ex. 1005 at Table 5; Ex. 1004 at ¶100. As a result of the increased
efficacy combined with the lack of an increase in adverse injection site reactions,
Pinchasi explicitly encouraged and motivated a POSA to use 40 mg GA in the
treatment of RRMS:
The increased efficacy observed with 40 mg/day GA in reducing
MRI-measured disease activity and relapse rate indicates that it is well
tolerated and can improve the treatment of RRMS patients. The
improvement in efficacy, however, is not accompanied by a
corresponding increase of adverse reactions which would be expected
upon a doubling of the administered dose.
Ex. 1005 at 19, ll. 8-14; Ex. 1004 ¶100; see also Ex. 1003 ¶¶ 73-74. Pinchasi,
which Teva owns, is no fluke. In Teva’s 2008 press release previewing results of
its FORTE trial—which compared 40 mg daily day dosing with 20 mg daily
dosing of Copaxone®—Teva reported no difference in efficacy with similar
tolerability. Ex. 1046; Ex. 1004 ¶ 99.
A POSA would also have been motivated to pursue less-than-daily dosing as
a means to improve patient compliance (the degree to which patients regularly take

37
medication as prescribed) and adherence (the extent to which a person’s behavior
corresponds with a caregiver’s instructions). Ex. 1004 ¶¶ 52-57; Ex. 1003 ¶¶ 98-
101, 107, 122, 127. Pinchasi expressly disclosed and claimed “periodic
administration,” including “every other day” dosing, with 40 mg of GA. Ex. 1005
at 8, ll. 10-11 & 21, ll. 11-12 (claim 3). Moreover, reducing the number of
injections is simply common sense to a POSA: patients are most likely to take
painful injections as prescribed when the injection is taken less often. Ex. 1003 ¶
97-101; Ex. 1004 ¶¶ 52-57. Even setting this common sense aside, however, the
prior art is filled with this motivation. Khan noted, for example, that there “is
considerable interest in alternate dosing regimens of GA in RRMS” because
“[d]aily SC injectable therapy can be challenging for long-term patient
compliance.” Ex. 1010; Ex. 1004 ¶ 66; Ex. 1003 ¶ 99. Khan also reported that
when given a choice, all patients who were treated with GA on a daily basis chose
to switch to alternate day GA therapies. Ex. 1010; Ex. 1004 ¶ 67; Ex. 1003 ¶ 112.
The 1996 FDA SBOA provided similar motivation. In it, the FDA reviewer told
Teva: “I would recommend that the Sponsor evaluate the necessity of daily s.c.
[subcutaneous] injections as opposed to more infrequent intermittent
administration of the drug.” Ex. 1007A at 121; see also Ex. 1003 ¶ 144.
Second, a POSA as of the priority date would have had a reasonable
likelihood of success in administering 40 mg GA according to the dosing schedule
38
claimed in the ’302 patent. Pinchasi disclosed 40 mg of GA administered every
other day as a safe and effective dose, and Flechter and Khan demonstrated that 20
mg every other day was safe and effective. Ex. 1005 at 19, ll. 8-14; Ex. 1008 at
63, 66-67; Ex. 1010. Thus, a skilled artisan would have expected that 40 mg of
GA administered every other day, or three times per week with at least one day
between doses, would be safe and effective. See, e.g., Ex. 1003 ¶¶ 99-101, 111-
116; Ex. 1004 ¶¶ 95-103. Moreover, a POSA would have had a reasonable
expectation that such dosing would improve patient compliance and adherence. In
addition to the skilled artisan’s common sense, Khan had demonstrated that
patients uniformly preferred alternate day dosing. Ex. 1003 ¶¶ 99, 112, 152; Ex.
1004 ¶ 102; Ex. 1010.
The table below compares the narrowest reading of the ’302 patent—exactly
three doses per week with at least one day between doses—with dosing schedules
in the prior art.
In sum, the published prior art provided all of the data a POSA would need
to try—with a reasonable expectation of success—a reduced-injection approach
within the scope of the of the ’302 patent claims.

39
DayBornstein
1984
Flechter
2002A/B;
Khan
’302
PatentPinchasiCopaxone®
Cohen;
Pinchasi
1 5 mg 20 mg 40 mg 40 mg 20 mg 40 mg
2 5 mg 20 mg 40 mg
3 5 mg 20 mg 40 mg 40 mg 20 mg 40 mg
4 5 mg 20 mg 40 mg
5 5 mg 20 mg 40 mg 40 mg 20 mg 40 mg
6 20 mg 40 mg
7 20 mg 40 mg 20 mg 40 mg
8 5 mg 20 mg 40 mg
9 5 mg 20 mg 40 mg 40 mg 20 mg 40 mg
10 5 mg 20 mg 40 mg
11 5 mg 20 mg 40 mg 40 mg 20 mg 40 mg
12 5 mg 20 mg 40 mg
13 20 mg 40 mg 40 mg 20 mg 40 mg
14 20 mg 40 mg
Total / 2 wks 50 mg 140 mg 240 mg 280 mg 280 mg 560 mg
Avg. / wk 25 mg 70 mg 120 mg 140 mg 140 mg 280 mg
Injections / wk 5 3, 4 3 3, 4 7 7

40
H. Ground 2: Claims 1-12 Are Unpatentable As Obvious overPinchasi.
1. Independent Claims 1 and 10 Are Obvious Over Pinchasi.
Claim 1 recites a method for treating MS using GA having the following
elements:
a preamble that recites a “method of treatment of a human patient suffering
from a relapsing form of multiple sclerosis”;
“administration to the human patient of three subcutaneous injections of a 40
mg/ml dose of glatiramer acetate per week;” and
a final clause stating that the claimed administration is “so as to treat the
human patient.”
Claim 10 recites a similar method, but also requires that the “subcutaneous
injection [be] by the human patient,” that there be “at least one day between every
subcutaneous injection” and that “the glatiramer acetate is present in l ml of a
pharmaceutical composition in a prefilled syringe for self injection by the human
patient” and that the “pharmaceutical composition further comprises mannitol and
has a pH in the range of 5.5 to 7.0.”
As explained below, Pinchasi teaches each element of claims 1 and 10.
First, as explained above, Pinchasi discloses each limitation of claims 1 and
10 when the administration is understood to be at least three injections per week,
including with one day between each injection, and therefore anticipates these

41
claims. Supra § F.1-2. If, however, the dosing frequency is limited to include only
three doses per week and to require administration of GA at that frequency over
multiple weeks – and there is no basis to read this claim so narrowly – Pinchasi
renders claim 1 obvious.
For example, a strict three times per week schedule would have been
obvious from Pinchasi alone because a POSA as of the priority date would have
viewed six doses over two weeks to be therapeutically equivalent to seven doses
over the same period. Ex. 1004 ¶¶ 82, 95-102. A POSA would have also
understood that three injections of 40 mg GA per week (i.e., 120 mg per week) and
alternate-day injections of 40 mg GA (i.e., 120 mg – 160 mg per week) would have
had substantially the same pharmacological effect. Ex. 1004 ¶¶ 83m 95-102; Ex.
1003 ¶¶ 120-123. A POSA knew from the prior art that administering a 40 mg SC
dose of GA was safe and effective, and that administering 120 mg of GA per week
(i.e., three 40 mg injections) was in the middle of the safe and effective range for
GA. See supra § G.2.b. at Table. Moreover, the POSA knew that less frequent SC
injections would be expected to decrease the incidence of side effects associated
with injectable medicines, and that less frequent adverse events would increase
patient compliance. See, e.g., Ex. 1004 ¶¶ 52-57 95-101; Ex. 1003 ¶ 102-105, 122.
A POSA would be motivated to modify the dosing schedule disclosed in
Pinchasi to reduce the number of doses to exactly three injections per week (rather

42
than having a fourth dose every other week) because this would reduce the
frequency of injections every other week by one injection, thereby reducing the
frequency of side effects. See, e.g., Ex. 1004 ¶¶ 52-57, 98-100, 109; Ex. 1003
¶¶ 107, 115. Modifying the Pinchasi schedule to a schedule having only 3
injections per week also allows for a more convenient dosing schedule (i.e.,
allowing the patient to medicate on the same days of each week) which would
improve patient adherence to the regimen, an important consideration in the
treatment of chronic conditions. Ex. 1004 ¶¶ 52, 85, 102; Ex. 1003 ¶¶ 98-101. A
POSA would have predicted that this modified dosing regimen would be safe and
efficacious based on the pharmacological data and clinical trials known in the art.
Ex. 1004 ¶¶ 93-10210; Ex. 1003 ¶¶ 111-116. Similarly, a POSA knew that
administering a 40 mg injection of GA did not impact the tolerability as compared
to 20 mg injections of GA again based on the pharmacological data and clinical
trials known in the art. Ex. 1004 ¶¶ 93-102; Ex. 1003 ¶¶ 112-116. The wealth of
pharmacological and clinical data in the art provided the POSA with a reasonable
expectation of success. Ex. 1004 ¶¶ 93-102; Ex. 1003 ¶¶ 111-116.
In addition to the clinical motivations, by 2009 there was an industry
recognized motivation to investigate different dosages and dosing regimens for
successful products to achieve further marketplace exclusivity. Ex. 1003 ¶¶ 108.
By 2009, prior art Copaxone® had been on the market for more than a decade and

43
faced competition from less frequently injected competitor products and oral
therapies as well as the expiration of the patents covering prior art Copaxone®. For
example, since at least 2003 the dosing schedule for Betaseron® required SC
injections on alternate days and Rebif® was injected three times per week. Ex.
1003 ¶ 109; Ex. 1004 ¶¶ 48, 55. The ’302 patent did not contribute an inventive
MS dosing schedule to the art, but instead adopted a predictably safe and effective
schedule that met the market pressures to offer a less frequent dosing schedule
while also allowing for market exclusivity based on new patents.
The recitations in claim 10 of self administration of the pharmaceutical
product in a prefilled syringe, pH, mannitol content, and volume of pharmaceutical
composition are each expressly disclosed in Pinchasi. See supra § F.2.
2. Dependent Claim 2 Is Obvious Over Pinchasi.
Dependent claim 2 depends from claim 1. The limitation of this claim is
disclosed in Pinchasi. See supra § F.3. For that reason and all of the reasons that
claim 1 is obvious in view of Pinchasi, dependent claim 2 is obvious in view of
Pinchasi.
3. Dependent Claim 3 Is Obvious Over Pinchasi.
Claim 3 depends from claim 1. To the extent claim 3 is not anticipated by
Pinchasi, it is rendered obvious. The claim recites that “the human patient has
experienced a first clinical episode and has MRI features consistent with multiple

44
sclerosis.” Pinchasi discloses a method of treating a patient that is suffering from a
relapsing form of MS. Ex. 1005 at 8, ll. 2-13. The recitation in claim 3 that
“human patient has experienced a first clinical episode and has MRI features
consistent with multiple sclerosis” would have been understood by a POSA to
indicate that the human patient has CIS. Ex. 1003 ¶¶ 86-88, 125; Ex. 1004 ¶¶ 92,
104-108. A POSA would have recognized that a treatment schedule of 40 mg
three times per week could be used with patients diagnosed with CIS as 20 mg
daily glatiramer acetate treatment was already approved and indicated for patients
with CIS syndrome by this time period. See Copaxone® Label (Feb. 2009) [Ex.
1052]; Ex. 1003 at ¶ 87; Ex. 1004 ¶¶ 104-105 The ’302 patent also recognizes that
based on the treatment of CIS patients with 20 mg daily, the claimed schedule is
“also expected to work in the treatment of patients who have experienced a
clinically isolated syndrome (CIS).” Ex. 1001 at col. 16, ll. 20-34; Ex. 1003 ¶ 87;
Ex. 1004 ¶ 105. Thus, a POSA would have considered a treatment plan with 40
mg GA administered three times per week to treat patients with CIS obvious to try
with a reasonable expectation of success. Ex. 1004 ¶¶ 104-105; Ex. 1003 ¶¶ 87,
111-116. Claim 3 is therefore obvious in view of Pinchasi. Ex. 1004 ¶¶ 104-105;
Ex. 1003 ¶¶ 86-90, 125.

45
4. Dependent Claims 6-9 and 12 Are Obvious Over Pinchasi.
Dependent claims 6-9 and 12 each ultimately depend from claim 1. The
limitations of each of these claims are disclosed in Pinchasi. See supra § F.3-6.
For that reason and all of the reasons that claim 1 is obvious in view of Pinchasi,
dependent claims 6-9 and 12 are obvious in view of Pinchasi.
5. Dependent Claims 4-5 and 11 Are Obvious Over Pinchasi.
Claims 4-5 and 11 depend from claims 2, 3 and 10, respectively. Claims 4-5
and 11 recite specific days of the week on which the three SC injections per week
of claims 1 and 10 are administered by the patient. Claims 4-5 and 11 each recite
seven different combinations of days. If these claims are read narrowly to require
only three injections per week and only on the specific days recited in claims 4-5
and 11, they are obvious in view of Pinchasi. Ex. 1004 ¶ 107; Ex. 1003 ¶ 127.
The administration of three injections of GA per week is obvious. Supra at
§ H.1. The ’302 patent makes no suggestion that the three specific days of the
week that the GA injections are administered is critical. Setting a course of
treatment for the same day each week, for example on Monday, Wednesday and
Friday, would have been recognized by a POSA as increasing compliance and
adherence to a dosing regimen. Ex. 1004 at ¶85. The three specific days of the
week are a matter of patient and physician choice from a limited number of
possibilities. See In re Peterson, 315 F.3d at 1330 (selection within known range

46
is presumptively obvious); In re Petering, 301 F.2d 676, 681-82 (CCPA 1962)
(embodiment need not be stated if a POSA would appreciate the embodiment from
the limited number of possibilities). In light of the reasons above and because
claims 1-3 and 10 are obvious over Pinchasi, claims 4-5 and 11 are obvious over
Pinchasi.
I. Ground 3: Claims 1-12 Are Unpatentable As Obvious OverPinchasi in View of the 1996 SBOA.
While the common knowledge and common sense of a POSA renders the
’302 patent obvious in view of Pinchasi alone, combining Pinchasi with the 1996
SBOA confirms that claims 1-12 of the ’302 patent are unpatentable as obvious.
Ex. 1004 ¶¶ 108-111; Ex. 1003 ¶¶ 128-147.
1. Independent Claims 1 and 10 Are Obvious Over Pinchasi inView of the 1996 FDA SBOA.
As supra, all limitations of claims 1 and 10 are obvious in view of Pinchasi.
One of those limitations includes “administration to the human patient of three
subcutaneous injections of a 40 mg/ml dose of glatiramer acetate per week so as to
treat the human patient” (claim 1) and “subcutaneous injection by the human
patient of a 40 mg/ml dose of glatiramer acetate three times per week with at least
one day between every subcutaneous injection” (claim 10). If read narrowly that
limitation may require only three injections per week. If Pinchasi alone does not
render that obvious, Pinchasi in view of the 1996 FDA SBOA confirms the

47
limitation is obvious. Ex. 1004 ¶¶ 108-111; Ex. 1003 ¶¶ 128-129, 145-146.
As discussed supra, a strict three times per week schedule would have been
obvious from Pinchasi alone for the reasons stated above. See supra § H.1. When
the teachings of Pinchasi are combined with the teachings of the 1996 FDA SBOA,
the motivation to modify the dosing schedule of Pinchasi to offer a patient less
frequent injections and the POSAs expectation of success in doing so are
unassailable. Ex. 1004 ¶¶ 109-110; Ex. 1003 ¶¶ 144-146.
The 1996 FDA SBOA teaches that the half-life for Copaxone® is
approximately 80 hours in the primate Cynomolgus monkey. Ex. 1003 ¶ 129.
Pharmacokinetic data, including half-life data, from a Cynomolgus monkey was a
reliable model for predicting human pharmacokinetic parameters and creating
dosing schedules for human administration of Copaxone as of the priority date.
See Ex. 1007A at 66; Ex. 1003 at ¶¶ 129, 138. When FDA reviewed this data,
submitted by Yeda’s partner, Teva, the reviewing pharmacologist commented:
In light of the fact that Copolymer-1 is most likely acting as a peptide
vaccine, it is unclear to me why it is necessary to inject the drug on a
daily basis. This dosing regimen seems like it would subject the
patient to an excessive amount of discomfort if it is not necessary to
maintain efficacy. Furthermore, if there should be a problem in
humans with saturation of the clearance mechanism, thus increasing
the amount of intact drug in the systemic circulation over time, this
problem might be lessened with intermittent rather than daily

48
administration. I would recommend that the Sponsor evaluate the
necessity of daily s.c. injections as opposed to more infrequent
intermittent administration of the drug.
Ex. 1007A at 121. A POSA would have agreed with the reviewer’s analysis based
on the data presented by Teva. The 1996 FDA SBOA notes that more frequent
injections subject the patient to discomfort, indicating that reducing the frequency
of injections is generally desirable and more frequent dosing “is not necessary to
maintain efficacy.” See Ex. 1007A at 121; Ex. 1003 at ¶¶ 144-146; Ex. 1004 ¶¶ 78
and 109. A POSA would have understood that the reported half-life of Copaxone®
indicated that injection frequencies could be reduced as far as approximately once
every 80 hours while maintaining the same safety and tolerability profiles. Ex.
1003 ¶¶ 129, 140-143. The 20 mg daily dosage amount of Copaxone®
administered SC with a predicted average half-life of 80 hours was established as
safe and effective for humans in 1996 when the FDA approved Copaxone®. Id. ¶
143. A POSA as of the priority date would therefore have understood that daily,
alternate-day, or at least three doses per week were interchangeable. Id. Thus,
well before the priority date, a POSA would have expected both 40 mg GA three
times per week and 20 mg daily to provide the same therapeutic profile to a
patient. Ex. 1003 ¶ 143; Ex. 1004 ¶¶ 109-110.
Based on these teachings, a POSA would have recognized that (1) reducing
the frequency of injections is generally desirable, (2) 40 mg dosing three times per

49
week would provide the same therapeutic profile with the potential for a
substantially improved safety and tolerability profile compared to daily 20 mg
dosing, and (3) maintaining the efficacy established for daily GA injections (i.e.
maintaining a steady state concentration) would require a dosing interval no greater
than approximately 80 hours. Ex. 1003 ¶¶ 128-146. Therefore, as explained
further below, it would have been obvious to a POSA to select Pinchasi’s alternate
day injection schedule and slightly adjust the injection frequency to provide
exactly three injections per week (instead of alternating between three and four
injections per week). This would also provide a more desirable schedule that is at
least as effective and safe as daily injections. Ex. 1003 ¶¶ 145-146.
In light of the reasons above and because claims 1 and 10 are obvious over
Pinchasi, claims 1 and 10 are obvious over Pinchasi and the 1996 FDA SBOA.
Ex. 1004 ¶¶ 108-111; Ex. 1003 ¶¶ 128-146.
2. Dependent Claims 2-9 and 11-12 Are Obvious OverPinchasi in View of the 1996 FDA SBOA.
Claims 2-9 depend from claim 1 and claims 11-12 depend from claim 10.
All of the additional limitations are obvious over Pinchasi. Supra § F.1-6 and §
H.1-5. For that reason and the reasons described above rendering claims 1 and 10
obvious in view of Pinchasi and the 1996 FDA SBOA, claims 2-9 and 11-12 are
obvious in view of Pinchasi and the 1996 FDA SBOA. Ex. 1004 ¶ 112; Ex. 1003
¶¶ 128-147.

50
J. Ground 4: Claims 1-12 Are Unpatentable As Obvious overPinchasi in View of Flechter 2002A.
1. Independent Claims 1 and 10 Are Obvious Over Pinchasi inView of Flechter 2002A.
As explained above, all limitations of claims 1 and 10 are obvious in view of
Pinchasi. One of those limitations includes “administration to the human patient of
three subcutaneous injections of a 40 mg/ml dose of glatiramer acetate per week so
as to treat the human patient” (claim 1) and “subcutaneous injection by the human
patient of a 40 mg/ml dose of glatiramer acetate three times per week with at least
one day between every subcutaneous injection” (claim 10). See supra § F.1-2. If
read narrowly that limitation may require only three injections per week. If
Pinchasi alone does not render that obvious, Pinchasi in view of Flechter 2002A
does. Ex. 1004 ¶¶ 113-118; Ex. 1003 ¶¶ 148-154.
As discussed, a POSA would have recognized that the dosage amount of 120
mg per week fell squarely within the established ranges, established by Pinchasi
and Flechter 2002A. See supra § G.2.b. at Table; Ex. 1003 ¶¶ 76, 93, 116, 148-
149; Ex. 1004 at ¶¶ 114, 116-117. Moreover, setting a course of treatment for the
same day each week, for example on Monday, Wednesday and Friday, would have
been recognized by a POSA as increasing compliance and adherence to a dosing
schedule. Ex. 1004 at ¶ 85. And Flechter 2002A taught the POSA that less
frequent dosing of GA, including alternate day dosing, was safe and efficacious

51
and preferred by patients. Ex. 1003 ¶¶ 149-154; Ex. 1004 ¶¶ 116-117. In light of
the reasons above and because claims 1 and 10 are obvious over Pinchasi, claims 1
and 10 are obvious over Pinchasi and Flechter 2002A. Ex. 1004 ¶¶ 113-118
2. Dependent Claims 2-9 and 11-12 Are Obvious OverPinchasi in View of Flechter 2002A.
Claims 2-9 depend from claim 1 and claims 11-12 depend from claim 10.
All of the additional limitations are obvious over Pinchasi. See supra § F.1-6 and §
H.1-5. For that reason and the reasons described above rendering claim 1 obvious
in view of Pinchasi and the 1996 FDA SBOA, claims 2-9 and 11-12 are obvious in
view of Pinchasi and Flechter 2002A. Ex. 1004 ¶ 119; Ex. 1003 ¶¶ 148-155.
K. Any Secondary Considerations Fail to Overcome the Showing ofObviousness.
To counter the overwhelming evidence that all claims of the ’302 patent are
obvious, the Patent Owner may try to rely on secondary considerations of
nonobviousness, despite no showing of such secondary considerations in the
patent. While any such evidence would be “insufficient” to “overcome the strong
[case] of obviousness” here (Pfizer, Inc. v. Apotex, Inc., 480 F.3d 1348, 1372 (Fed.
Cir. 2007)), Petitioner nonetheless preliminarily addresses some of the alleged
secondary considerations that Patent Owner may argue and reserves the right to
respond to any arguments asserted by the Patent Owner in this proceeding.

52
1. The Methods Recited in the ’302 Patent Produced NoUnexpected Results.
The ’302 patent makes no claim that the methods recited in its claims
achieve any unexpected result. Quite to the contrary, the best the ’302 patent could
claim is that its methods “are at least as effective” as the prior art. Ex. 1001 at col.
13, ll. 47 to col. 15, ll. 50.. And even these statements are unsupported by any
concrete data in the patent since the only example, example 1, is a prophetic one.
Nonetheless, in view of the extensive disclosures in the prior art as discussed in
this Petition, the efficacy of the administration of GA as recited in the ’302 patent’s
claims is not surprising, and is certainly not unexpected. Ex. 1003 ¶¶ 87, 94-95;
Ex. 1004 ¶ 52-78. Indeed, the Board has held in a previous decision that the
absence of any discussion of unexpected or superior results related to the
administration of a drug on a difference dosing schedule is evidence that the
administration schedule was a product of routine clinical trial processes and well
within the grasp of a POSA. Biomarin, IPR2013-00534 at 18.
Even assuming that the methods claimed in the ’302 patent have
“unexpected properties,” they “do[] not upset an already established motivation to
treat patients with glatiramer acetate “based on [its] expected properties.” Bristol-
Myers Squibb Co. v. Teva Pharms. USA, Inc., 752 F.3d 967, 976 (Fed. Cir. 2014).
As discussed supra, a POSA would have been motivated to treat patients with 40
mg injections of GA three times per week with a reasonable expectation that it
53
would alleviate symptoms of relapsing forms of MS and would be well tolerated
with fewer side effects. See supra § G.2. Thus, any “evidence of [the claimed
method’s] superior efficacy does nothing to undercut the showing that there was a
reasonable expectation of success ... , even if the level of success may have turned
out to be somewhat greater than would have been expected.” Hoffmann-La Roche,
748 F.3d at 1334.
2. The ’302 Patent Satisfied No Long-Felt But Unmet Need.
The Patent Owner may also claim that there was a long-felt but unmet need
for a method of treating patients suffering from relapsing forms of MS with less
frequent injections and that the ’302 patent met that need. Yet, if there was any
long-felt need was it was met long ago by Pinchasi, among other references.
Therefore, “others had previously solved” any “long-felt need” alleged to be met
by the claims of the ’302 patent. See In re PepperBall Techs., Inc., 469 F. App’x
878, 882-83 (Fed. Cir. 2012). Moreover, as of the priority date, there were a
number of effective MS treatments on the market and approved by the FDA that
resulted in less frequent injections. Ex. 1003 ¶ 24, 87; Ex. 1004 ¶ 48. Finally, the
fact that no one else had made and commercialized a method of treatment as in the
’302 patent as of the priority date is irrelevant. Because the ’302 patent recites
methods of using GA, a compound that was covered by other U.S. patents at the
priority date, “no entity other than” the Patent Owner “could have successfully

54
brought [the claimed methods] to market.” Galderma Labs. v. Tolmar, Inc., 737
F.3d 731, 740 (Fed. Cir. 2013).
3. Copying By Generic Drug Makers Is Irrelevant.
Finally, to the extent the Patent Owner argues that Petitioner and other
generic drug companies seek to copy the invention of the ’302 patent by
commercializing generic versions of GA, this too fails to support non-obviousness.
As “copying” “is required for FDA approval” of generic drugs, any “evidence of
copying in the [generic drug] context is not probative of nonobviousness.” Bayer
Healthcare Pharms., Inc. v. Watson Pharms., Inc., 713 F.3d 1369, 1377 (Fed. Cir.
2013).

55