Excretory urography
61
Transcript of Excretory urography


• Aka Excretory urography• Use decreased significantly in recent years CT, US, MR
• Remains primary modality for visualization of pelvi-calyceal system

• Haematuria• Renal colic• Recurrent urinary tract infection• Trauma• Renal tumor• Renal hypertension• Calculi (kidney , ureter, bladder)• Bladder pathology ( diverticula ,fistula )
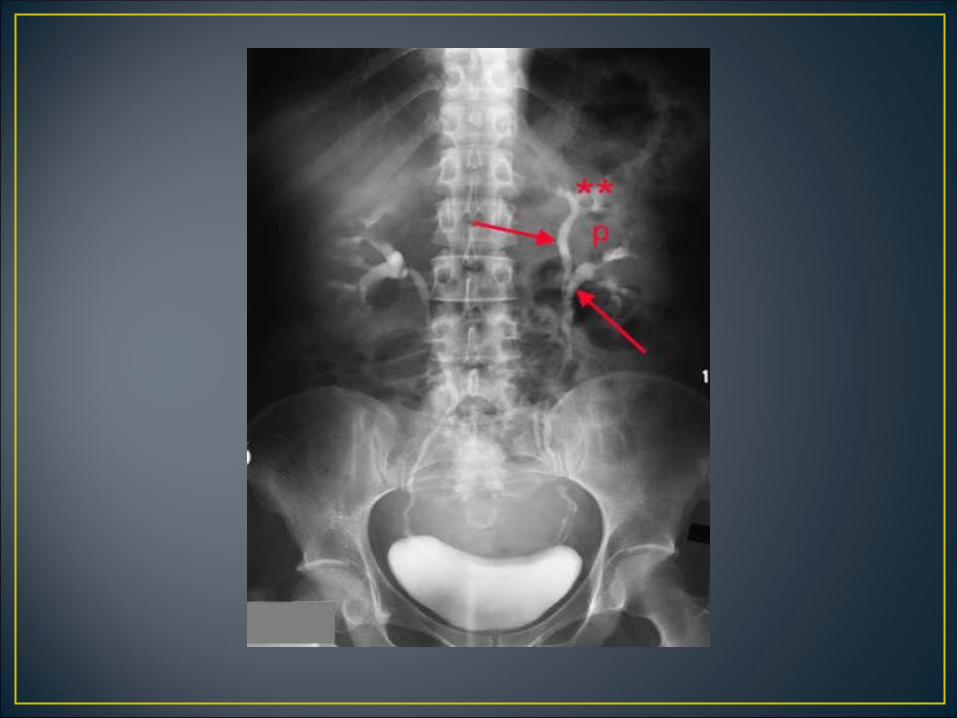
Urogram•Visualization of kidney parenchyma,calyces and pelvis resulting from IV injection of contrast
Pyelogram•Describes retrograde studies visualizing o nly the collecting system So, IVP is misnomer, should be IVU
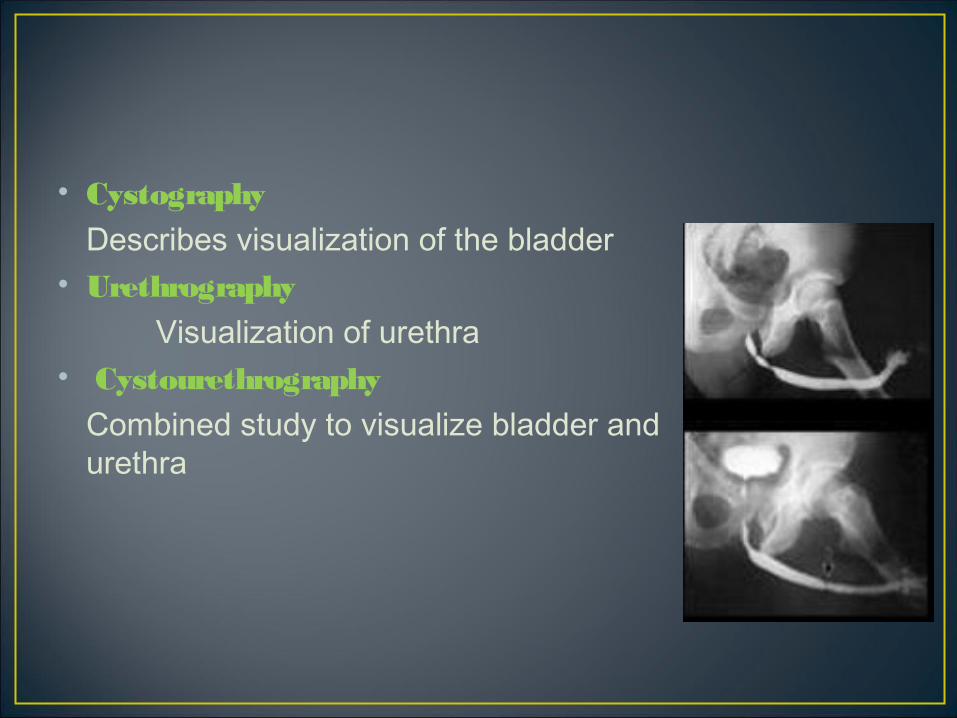
• Cystography Describes visualization of the bladder• Urethrography Visualization of urethra• Cystourethrography Combined study to visualize bladder and
urethra

• NBM for 5 hrs• Ambulent for 2 hrs to reduce bowel gases
• Inject nonionic contrast Or LOCM as bolus, 30-60 s e c• Adult 50-100 ml• Pediatric 1ml/kg

• True contrast reactions are uncommon
• Most commonly seen are minor side effectsFlushing
Metallic taste in mouthTachycardiaUsually resolve within a few minutes
• Scout view• Additional views

• Supine , full-length AP abdomen, full inspiration• Lower border of cassette at the level of symphysis pubis,
beam centered in midline at the level of iliac crests
• Often difficult to fit this large area on a single radiograph, may need….
• 14 x 17 of abdomen• 10 x 12 of lower pelvis
• Look for…• Calcifications• Abnormal soft tissue• Air within urinary tract• Bony abnormalities• Determine if a contraindication to abdominal
compression exists


• Oblique Views (35 degree posterior oblique) - Good for questionable ureteral lesions - For differentiating extrinsic and intrinsic renal and
ureteral masses -Visualization of posterolateral aspect of bladder
• Supine AP of renal areas in expiration• Tomography of kidneys


• Immediate Film• AP of renal areas.• 10-14 sec after injection• Shows nephrogram
• 5-min Film• AP of renal areas• Determine if excretion symmetrical• Assess the need to modify technique • Application of compression band baloon at level of anterior
superior iliac spines

• Compression contraindicated in• Recent abdominal surgery• Renal trauma• Large abdominal mass or aortic aneurysm• Already dilated calyces on 5-min film

• 10-min Film• AP of renal areas• Compression released if pelvicalyceal system adequately
visualized• Release film• Supine AP abdomen• Whole urinary tract• Empty bladder
• Post voiding Film• Full length OR • Coned view of bladder(tube 15 degree caudal, centered 5 cm
above symphysis pubis)• Must be obtained immediately after voiding
• To determine residual urine in bladder >especially in older male patients
• To look for bladder neoplasms• VUJ calculi• Urethral diverticulum in females

TCC

Delayed Views•1 hour to 48 hours- in cases of obstruction •Better to CT patient for immediate diagnosis

Prone film•Helps fill ureteral areas not seen in supine position since upper ureters more anterior than kidney

Erect film•Promotes e m p ty ing of collecting system •Optimal for showing bladder hernias•Shows layering of calculi in cysts•Demarcates areas of ureteral obstruction be tte r than prone views





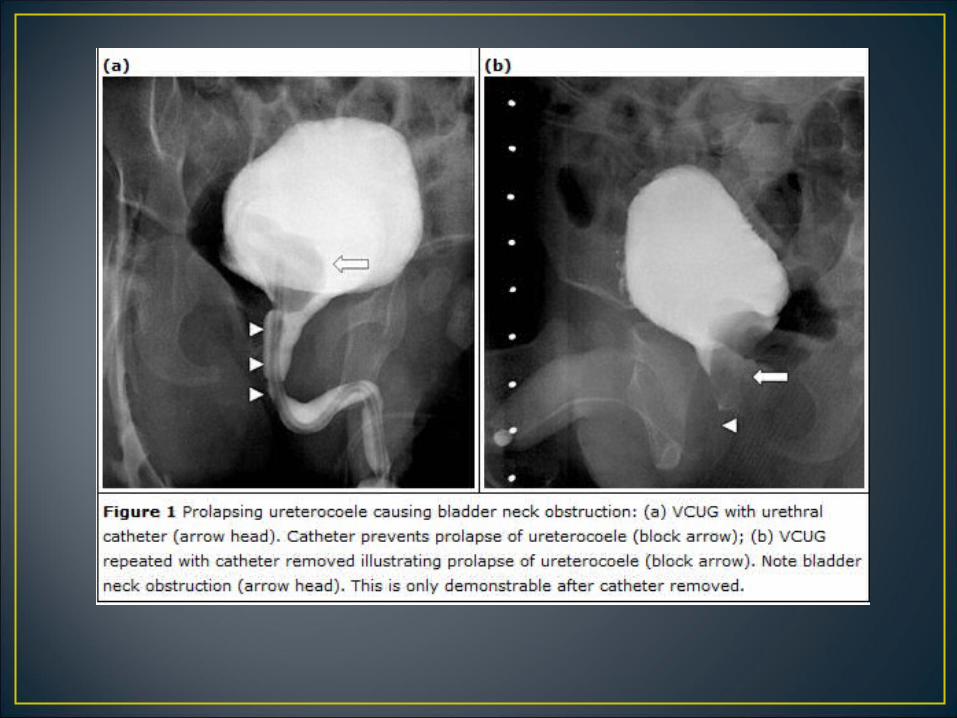
Dynamic test used to define• The anatomy • the function of the lower urinary tract.
Performed by..•placing a catheter through the urethra into the bladder•filling the bladder with contrast material•taking x-rays while the p a tie nt vo id s .

• Vesico-ureteric reflux• Bladder abnormalities• Stress incontinence• Urethral trauma leading to obstruction• Posterior urethral valves
• Acute UTI

• HOCM or LOCM• Fluoroscopy unit with spot film device and tilting table• Video recorder• Jaque’s or folley’s catheter. In small infants 5-7 size
feeding tube is adequate

Patient preparation•Micturate prior to examination
Preliminary Film•Coned view of bladder , using the under-couch tube
To demonstrate vesico-ureteric refluxExclusively in children•Supine on x-ray table•Insert catheter aseptically•Drain residual urine•Contrast medium dripped into bladder and observed under fluoroscopy•Record reflux•Patient asked to micturate•Spot films taken during m ic turitio n
• Oblique/lateral position for males to observe entire urethra
• Full length abdominal view to look for..• Unnoticed contrast reflux into kidneys• Post-micturition residue
To demonstrate vesico-vaginal / recto-vesical fistula•Films taken in lateral position
To demonstrate stress incontinence•Catheter left in situ until patient is in erect position
Include sacrum and symphysis pubis•Lateral bladder•Lateral bladder, straining - catheter removed•Lateral bladder during micturition
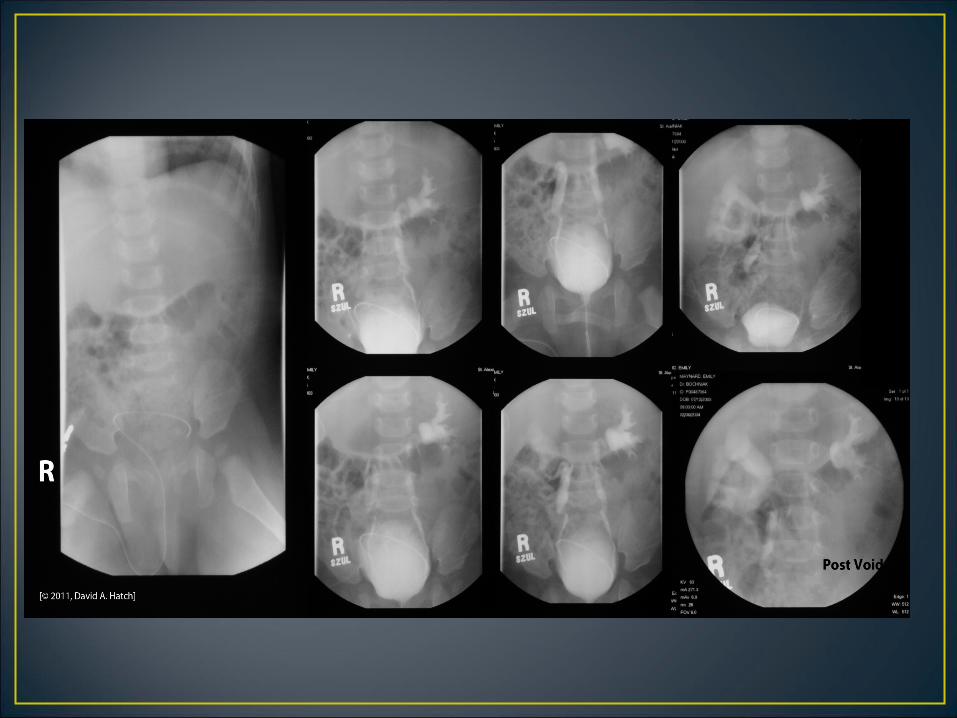
• KUBevaluate the bones of the spine and pelvis (injury or
congenital anomaly such as spina bifida) and the soft tissues (calcifications, foreign bodies, etc.)


• posterior processes are absent below L-4. This patient has lower lumbar spina bifida.
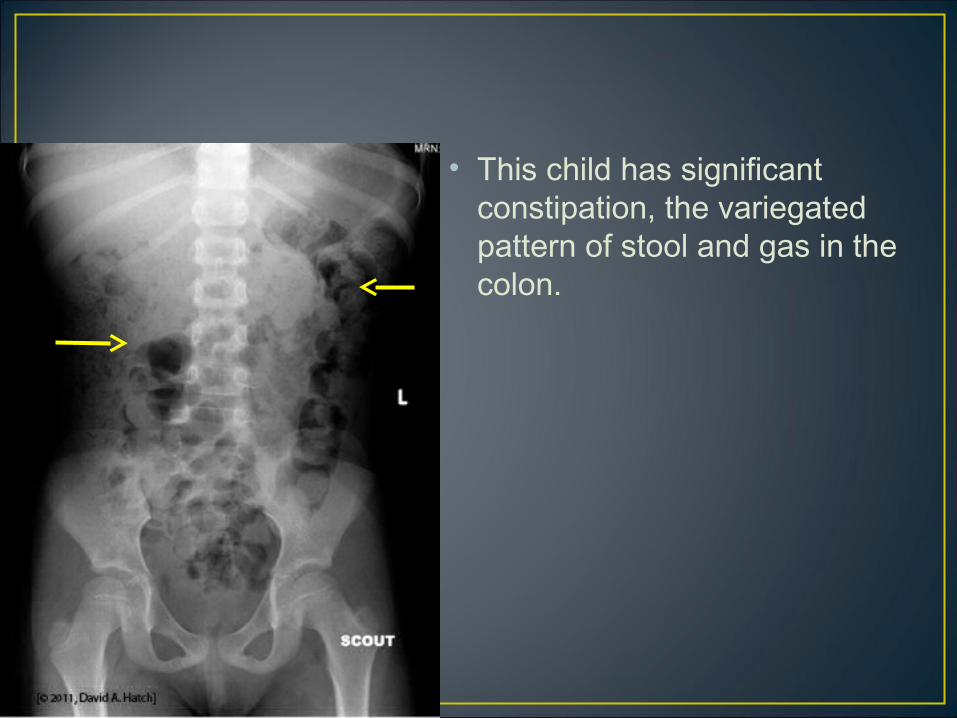
• This child has significant constipation, the variegated pattern of stool and gas in the colon.
• Images are obtained while the bladder is being filled with liquid contrast.
• The bladder should appear smooth and regular and there should be no filling defects e x c e p t the balloon of the urethral catheter.
• The edges of the bladder image should be smooth.

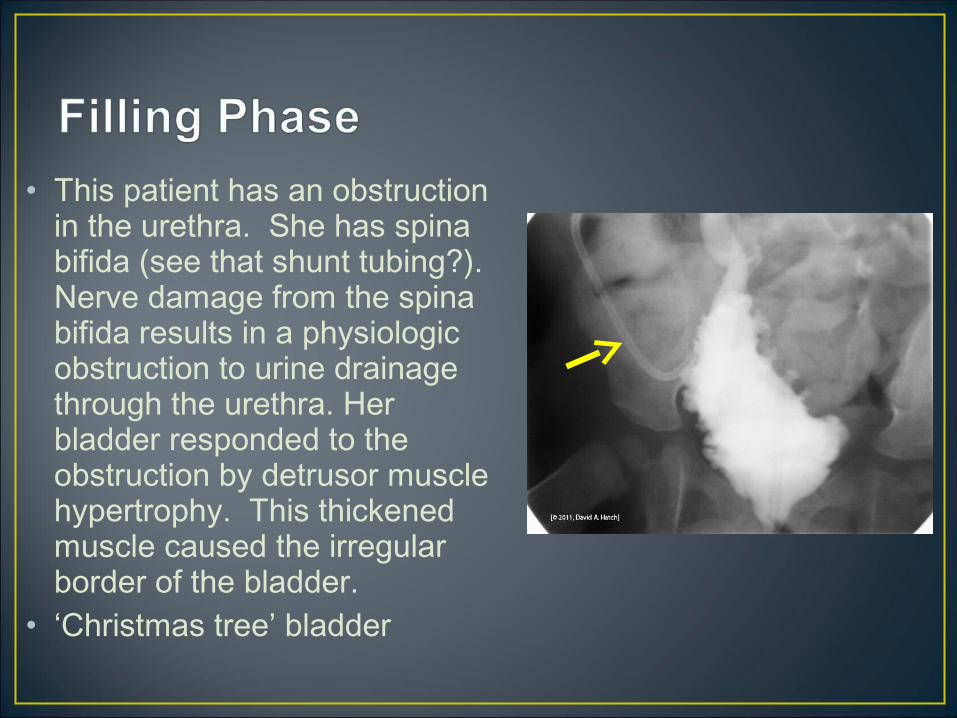
• This patient has an obstruction in the urethra. She has spina bifida (see that shunt tubing?). Nerve damage from the spina bifida results in a physiologic obstruction to urine drainage through the urethra. Her bladder responded to the obstruction by detrusor muscle hypertrophy. This thickened muscle caused the irregular border of the bladder.
• ‘Christmas tree’ bladder

• To demonstrate the urethra (strictures or obstruction) and the bladder
• The presence or absence of vesicoureteral reflux.

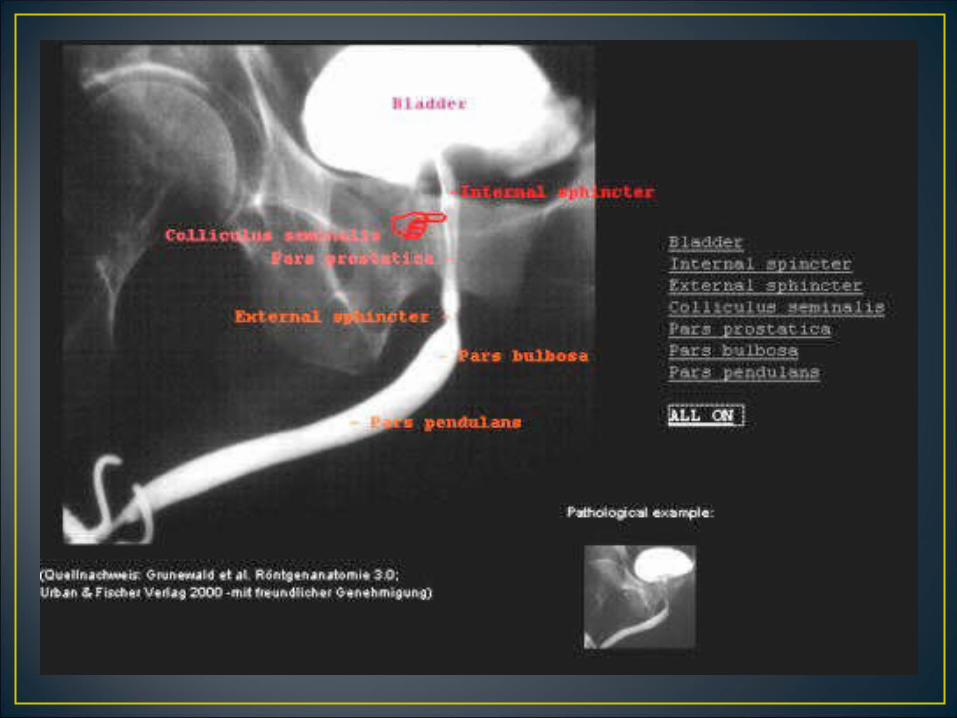
• This film shows a normal male urethra; there is no obstruction. The variation seen in the diameter of the urethra is normal.
Indentation at the urethral sphincter (normal)

• May demonstrate • Reflux• Extravasation of urine from the
bladder or urethra• Residual urine in bladder
• No reflux and no residual bladder urine is seen in normal post-void film.
Normal post-void film

• No special care needed• Rarely dysuria leading to urinary retention - analgesic• Antibiotics prescription to patients with reflux
• Due to contrast medium1.Contrast induced cystitis2.Contrast reaction due to absorption by bladder mucosa
• Due to technique1.Acute UTI2.Catheter trauma - dysuria , frequency, hematuria ,
retention3.Perforation from over distention4.Catheterization of vagina or an ectopic ureteral orifice5.Retention of Foley's catheter
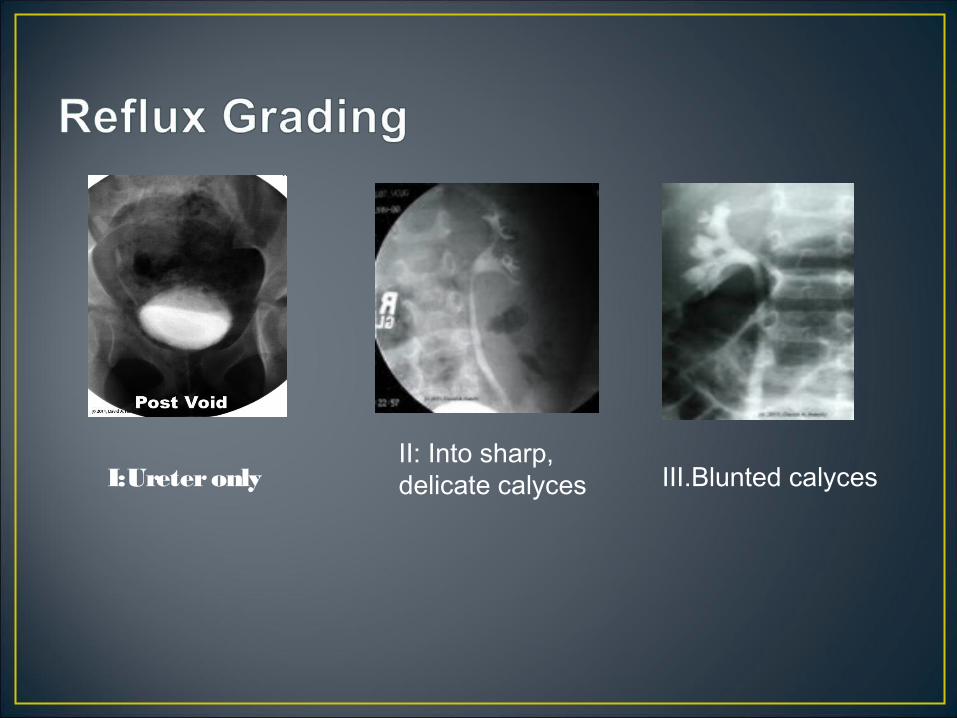
I:Ureter onlyII: Into sharp, delicate calyces III.Blunted calyces
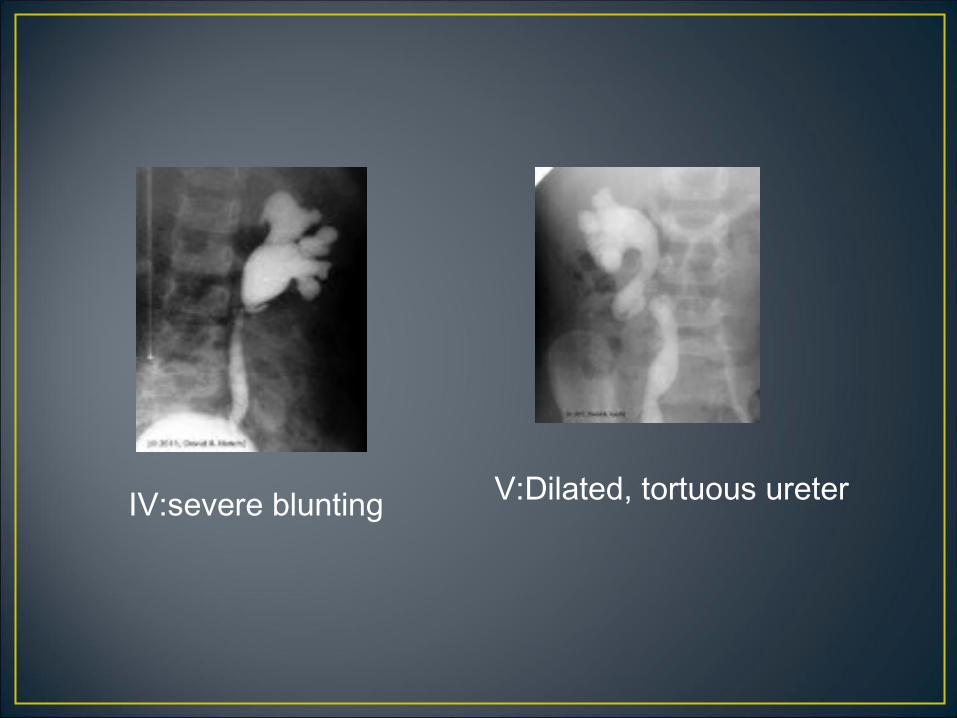
IV:severe blunting V:Dilated, tortuous ureter