Ercp
22
ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP) Jinu Janet Varghese Group IV Year III
-
Upload
tbilisi-state-medical-university -
Category
Health & Medicine
-
view
346 -
download
2
Transcript of Ercp
ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY (ERCP)
Jinu Janet Varghese
Group IV
Year III

INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) is a technique
that combines the use of endoscopy and fluoroscopy to diagnose and
treat certain problems of :
• the duodenum (the first portion of the small intestine),
• the papilla of Vater (a small structure with openings leading to the
bile ducts and the pancreatic duct),
• the bile ducts, and
• the gallbladder and the pancreatic duct.

USES
Diagnostic
Used when it is suspected a person’s bile or pancreatic ducts may be
narrowed or blocked due to:
• tumors
• gallstones that form in the gallbladder and become stuck in the ducts
• inflammation due to trauma or illness, such as pancreatitis
• infection
• Dysfunction of valves in the ducts, called sphincters,
• scarring of the ducts (sclerosis),
• Pseudo-cysts—accumulations of fluid and tissue debris

Therapeutic
• Sphincterotomy
• Stone Removal
• Stent Placement
• Balloon Dilation
• Tissue Sampling

PREPARATION OF PATIENT BEFORE ERCP
• The upper GI tract must be empty. Generally, no eating or drinking is
allowed 8 hours before ERCP.
• Smoking and chewing gum are also prohibited during this time.
• Current medications may need to be adjusted or avoided. Most
medications can be continued as usual.
• Removal of any dentures, jewelry, or contact lenses before having an
ERCP.

• Before ERCP, all of the patient’s previous abdominal imaging findings
(from CT scans, magnetic resonance imaging [MRI], ultrasonography,
and cholangiography or pancreatography) should be reviewed.
• Deep sedation is desirable during ERCP because a stable endoscopic
position in the duodenum is important for proper cannulation,
therapeutic intervention, and avoidance of complications.

PROCEDURE
• Patients receive a local anesthetic that is gargled or sprayed on the
back of the throat & IV sedatives.
• patients lie on their back or side on an x-ray table
• Then a flexible camera (endoscope) is inserted through the mouth,
down the esophagus, into the stomach, through the pylorus into the
duodenum where the ampulla of Vater (the opening of the common
bile duct and pancreatic duct) exists. The sphincter of Oddi is a
muscular valve that controls the opening of the ampulla. The region
can be directly visualized with the endoscopic camera while various
procedures are performed.

• A plastic catheter or cannula is inserted through the ampulla, and
radiocontrast is injected into the bile ducts and/or pancreatic duct.
Fluoroscopy is used to look for blockages, or other lesions such as
stones.
• When needed, the opening of the ampulla can be enlarged
(sphincterotomy) with an electrified wire (sphincterotome) and access
into the bile duct obtained so that gallstones may be removed or other
therapy performed.

FLUOROSCOPIC IMAGE SHOWING DILATATION OF THE PANCREATIC DUCT DURING ERCP INVESTIGATION. ENDOSCOPE IS VISIBLE.

FLUOROSCOPIC IMAGE OF COMMON BILE DUCT STONE SEEN AT THE TIME OFERCP. THE STONE IS IMPACTED IN THE DISTAL COMMON BILE DUCT. A
NASOBILIARY TUBE HAS BEEN INSERTED.

• Other procedures associated with ERCP include the trawling of the
common bile duct with a basket or balloon to remove gallstones and
the insertion of a plastic stent to assist the drainage of bile. Also, the
pancreatic duct can be cannulated and stents be inserted. The
pancreatic duct requires visualisation in cases of pancreatitis.
• In specific cases, a second camera can be inserted through the channel
of the first endoscope. This is termed duodenoscope-assisted
cholangiopancreatoscopy (DACP) or mother-daughter ERCP. The
daughter scope can be used to administer direct electrohydraulic
lithotripsy to break up stones, or to help in diagnosis by directly
visualizing the duct.
AFTER THE PROCEDURE
• Patients are monitored in the endoscopy area for 1-2 hours until the
effects of the sedatives have worn off & observed for complications.
• Eating or drinking is allowed if the throat is no longer numb and are
able to swallow without choking.
• If a gallstone was removed or placed a stent during the test, the
patient is made to stay in the hospital overnight.

AN EXAMPLE (BILE DUCT CANCER (CHOLANGIOCARCINOMA)
• Cholangiocarcinoma is a cancer that arises from the cells within the bile
ducts; both inside and outside the liver. tumors arise along the bile ducts
that enter the liver, the tumors are smaller than those which arise from
within.

COMPARISON OF RADIOGRAPHIC IMAGES SHOWING CHOLANGIOCARCINOMA; A, COMPUTED TOMOGRAPHY (CT) IMAGE; B, CHOLANGIOGRAM (ERCP) IMAGE.
ARROWS DESIGNATE THE TUMOR

A, B, POSITION OF THE ENDOSCOPE IN THE DUODENUM DURING ERCP
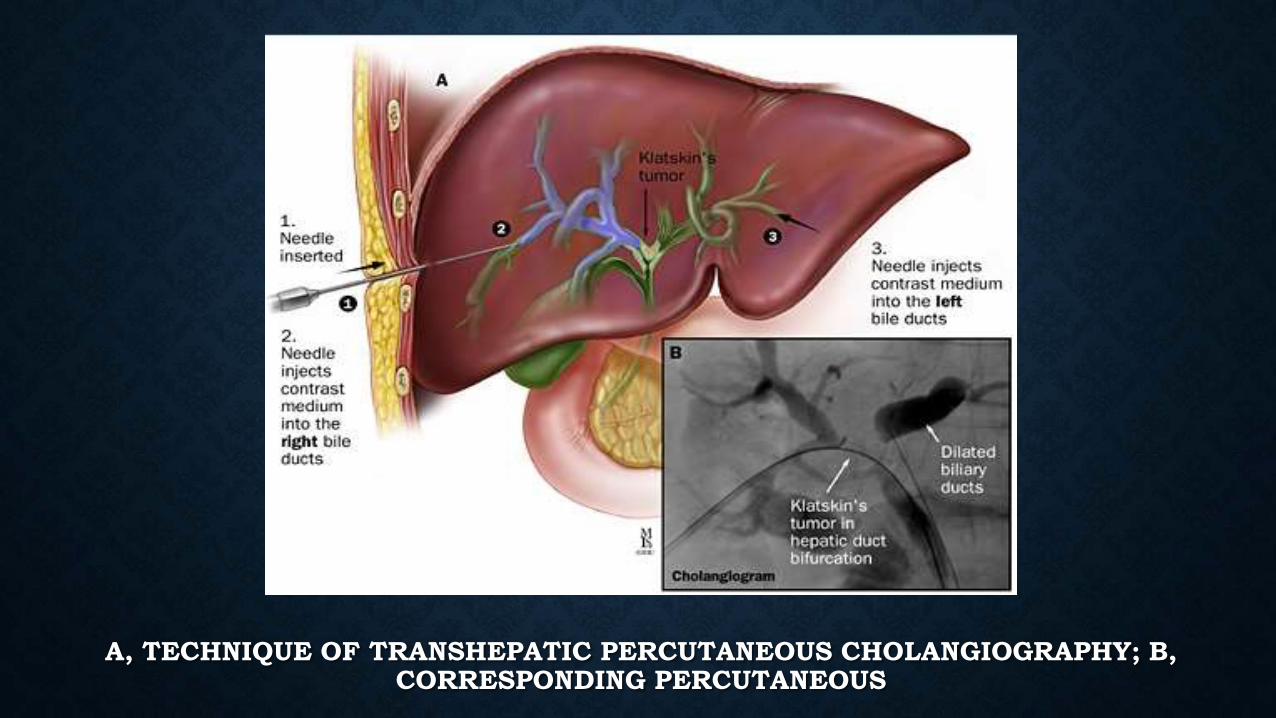
A, TECHNIQUE OF TRANSHEPATIC PERCUTANEOUS CHOLANGIOGRAPHY; B, CORRESPONDING PERCUTANEOUS


COMPLICATIONS
• ERCP is a highly specialized procedure which requires a lot of
experience and skill.
• The procedure is quite safe and is associated with a very low risk
when it is performed by experienced physicians.
• The success rate in performing this procedure varies from 70% to 95%
depending on the experience of the physician.
• Complications can occur in approximately one to five percent
depending on the skill of the physician and the underlying disorder.

Significant risks associated with ERCP include
• infection
• pancreatitis
• allergic reaction to sedatives
• excessive bleeding, called hemorrhage
• puncture of the GI tract or ducts
• tissue damage from radiation exposure
• death, in rare circumstances

CONTRAINDICATIONS
• Unstable cardiopulmonary, neurologic, or cardiovascular status; and
existing bowel perforation.
• Structural abnormalities of the esophagus, stomach, or small intestine
may be relative contraindications for ERCP.
• An altered surgical anatomy.
• ERCP with sphincterotomy or ampullectomy is relatively
contraindicated in coagulopathic patients.

REFERENCES
• http://www.webmd.com/digestive-disorders/endoscopic-retrograde-
cholangiopancreatogram-ercp?page=5
• http://digestive.niddk.nih.gov/ddiseases/pubs/ercp/
• http://en.wikipedia.org/wiki/Endoscopic_retrograde_cholangiopancreatography
• http://www.medicinenet.com/ercp/page3.htm
• http://www.asge.org/patients/patients.aspx?id=386
• http://www.sages.org/publications/patient-information/patient-information-for-ercp-
endoscopic-retrograde-cholangio-pancreatography-from-sages/
• http://www.patient.co.uk/health/ercp