Emerging Therapies for Triple Negative Breast...
66
Emerging Therapies for Triple Negative Breast Cancer Joseph A. Sparano, MD Professor of Medicine & Women’s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore Medical Center Bronx, New York
Transcript of Emerging Therapies for Triple Negative Breast...

Emerging Therapies for
Triple Negative Breast Cancer
Joseph A. Sparano, MD Professor of Medicine & Women’s Health
Albert Einstein College of Medicine
Associate Chairman, Department of Oncology
Montefiore Medical Center
Bronx, New York

Triple-Negative Disease Compared with Other
Phenotypes in the California Cancer Registry Study Bauer et al. Cancer 2007: 109; 721
Parise et al. The Breast Journal 2009: 15: 593
• Population-based study
– 6370 with “triple-negative” disease compared with 44,704
“other” cases (12% of all cases)
• TNBC more likely to be associated with
– Younger age (<40): OR 1.53
– Non-Hispanic black (OR 1.77) or Hispanic (OR 1.23)
– Higher grade (72% grade 3)
– More advanced stage (66% >/= stage II vs. 50% ER+HER2-)
– Poorer 5 year RFI irrespective of stage
• TNBC: 76% (similar to 76% for HER2-Pos)
• HR-Pos, HER2-Neg: 94%

Lin et al. Cancer 2012

The Future - What Trials are Currently Accruing? Search of Clinical Trials.Gov Using Search Term “Triple Negative Breast Cancer”
(accessed 9/24/13)
• Number of trials
– 201 “active “ trials, 95 recruiting (8 phase III trials)
• Selected adjuvant phase III trials (not yet reported)
– TITAN (N=614/1800) - AC → weekly paclitaxel x 12 vs. ixabepilone x 4 (00789581)
– PACS08 (N=762/2500) - FEC100 x 3 → docetaxel x 3 vs. ixabepilone x 3 (00630032)
– Spanish Breast Cancer Group –Ciboma (N=876) – AC-T +/- capecitabine (00130533)
– China (N=520) – FEC → docetaxel vs. doc/capecitabine→ capecitabine + EC (01642771)
– China (N=600) – AC-T +/- capecitabine (01112826)
• Neoadjuvant trials
– C40603 (400): Paclitaxel (+/-carbopatin) → AC (+/- bevacizumab)
– Neo-TN (N=270) – AC→docetaxel/capecitabine vs. high-dose alkylators (01057069)
• Metastatic trials
– China (N=232) – Gemcitabine/cisplaitn vs. gem/paclitaxel (01287624)
– UK (N=400) – Carboplatin vs. docetaxel (00532727)
– Celgene (N=790) – Nab-paclitaxel + gem vs. carbo (01881230)
4

The Future – New Agents Being Tested in TNBC Search of Clinical Trials.Gov Using Search Term
“Triple Negative Breast Cancer” - Novel Agents
• Met inhibitor: ARQ197, Onartuzumab (Metmab), foretinib
• PI3K and/or inhibitor: BKM 120, temsirolimus (+neratinib)
• HDAC inhibitors: entinostat, vorinosat
• Demethylating agents: azacitidine (+entinostat)
• PARP inhibitors: ABT-888, E7449
• Angiogenesis inhibitor: cediranib (+olaparib), ramucirumab, IMC18F1, foretenib,
sorafenib, tivozanib
• Hsp90 Inhibitors: ganetespib
• Aurora kinase inihbitors: ENMD 2076
• EGF inhibitors: erlotinib (+metformin,), afatanib
• MEK inhibitors: GSK1120212
• Wnt inhibitor: LGK974
• CDK inhbitor: Dinaciclib, P276-00
• FMS-Kit inhbitor: PLX3397
• Apoptosis inducer: LCL161 (deactivating inhibitor of apoptosis proteins (IAPs),
• Immunotherapy: MUC1 vaccine, adoptive cellular therapy (DC-CIK)
• Cytotoxics: SN38 -NK012, AEZS-108 (LHRH-dox)
5

TNBC:
Selected Reports and Clinical Trial Results
• Biomarker discovery
• Lymphocytic infiltration
• Gene expression
• Next generation sequencing
• Platinums
– GeparSixto
– PrE0105
– C40601 pending
• Antiangiogenic agents
– Adjuvant - BEATRICE (& C40601 pending)
– Neoadjuvant – NSABP and GBG

Loi et al.. J Clin Oncol 2013; 31: 860

Systematic Review & Metaanalysis of TILs and Response to Neoadjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2013 Murali Janakiram, MD
• Methods:
– 1147 reports in Pubmed, ASCO abstracts (2009 -2012), & Embase between 1/91-5/13
– 7 studies including 1641 patients met inclusion criteria
• Results:
– TIL ratio classified as either high or positive was associated with a significantly higher likelihood of achieving a pCR/near pCR after NAC
– Effect was driven mainly by a difference in in ER negative tumors and Her2 positive tumors
Subtype N Noof
studies
pCR% OR 95%CI
TILlow TILhighAll 1641 7 12.5% 28.6% 3.68 1.93–7.01
ER-/PR- 403 4 23.6% 41.3% 4.04 2.16–7.57Her2+ 326 3 16.9% 23.4% 5.61 1.80-17.47ER/PR+ 558 2 5.6% 11.5% 2.17 0.95–4.98


Topalian et al. NEJM 2012

Topalian et al. NEJM 2012
Tumor PD-L1 as a Predictive Biomarker for anti-PD1 Antibody

MCF-7
Ductal
Carcinoma
Normal
Lobule
MDA-231

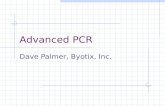
Gene Expression and Genomic Profiling

Breast cancer intrinsic subtypes by gene expression profiling
Perou et al. Nature 2000; Parker et al. JCO, 2009
Luminal A Luminal B ERBB2+ Basal NormL

Intrinsic Subtype Frequencies by ER/PgR Cut-
offs within TNBC Across 3 Adjuvant Trials: GIECAM 9906, MA5, MA12
ER/PR <1% (n=283) ER/PR <10% (n=331)
Cheang et al. ASCO 2012, abstract 1008

TNBC Subtypes 21 publicaly available gene expression breast cancer datasets, 587 TNBCs
Basal-like 1 (BL1): Cell-cycle, proliferation and
DNA damage response genes
Basal-like 2 (BL2): Growth factor signaling (EGF,
MET, Wnt/β-catenin, IGF1R)
Immunomodulatory (IM): Immune cell & cytokine
signaling (overlap with medullary signature)
Mesenchymal (M): Cell motility and differentiation
(Wnt, ALK, TGF-β)
Mesenchymal stem-like (MSL): Similar to M, but
increased growth factors signaling, low
proliferation, enrichment of stem cell genes
Luminal androgen receptor (LAR): Enriched in
hormonally-regulated pathways, androgen
receptor signaling. Displays luminal expression
patterns (molecular apocrine carcinomas)
Copyright © 2011, American Society for Clinical Investigation
Lehmann BD, et al. Journal of
Clinical Investigation, 2011

Are the Subtypes Clinically Relevant? Maybe
• Basal Cisplatin
• LAR Bicalutamide
• Mesenchymal-like
Src inhibition

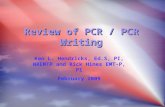
BRCA1-Deficient Cells are
Hypersensitive to Cisplatin
• BRCA1 deficient cells have defect in DNA DS repair
• BRCA1 deficient cells were more sensitive to cisplatin compared to other cell lines
• BRCA1 loss increases sensitivity to DNA damaging agents like cisplatin
Tassone P et al. Br J Cancer 2003; 88:1285-1291
HCC1937, BRCA-deficient cell line
MCF-7, hormone-sensitive
MDA-MB230, hormone-insensitive


Genomic Sequencing vs. Gene Expression
Whole Exome Sequencing – 1% Genome
Coding regions only
Whole Genome Sequencing –100% Genome (22,000 genes)
Exons (coding), Introns (non-coding), & Intergenic Regions
Targeted Sequencing – 0.003% Genome
200-400 exons – potentially actionable mutations
Gene Expression Profiling
7 (BCI), 21 (Oncotype), 50 (PAM50), 70 (Mammaprint), others
Poor risk proflles identify patients with ER-pos, HER2 neg
disease & 0-3 pos nodes who derive greatest chemo benefit
Non-coding RNA
DNA methylation
Histone modfications
Resea
rch &
D
isco
ve
ry
Clin
ical P
ractice
Proteomics
Presented by: Joseph A. Sparano, MD

The Genomic and Transcriptomic Architecture of 2000 Breast Tumors Reveals Novel Subgroups
Curtis, C et al. Nature 2012

Shah et al. Nature, 2012

Nature, 2012

Role of Platinums


Presented at the 2013 ASCO Annual Meeting. Presented data is the property of GBG and AGO-B.
Her2-pos: Trastuzumab 6(8) mg/kg q3w (for 1 year) +
Lapatinib 750 mg/d 18 wks
TNBC: Bevacizumab 15 mg/kg q3w
Su
rgery
GeparSixto:
Subtype Specific Targeted Therapy
Paclitaxel 80 mg/m² q1w Carboplatin AUC 1.5* q1w
*reduced from AUC 2 at amendment 1 after enrolment of 330 patients
R
N=595
centrally
confirmed
TNBC
or
Her2-positive
breast cancer
PM
PMCb
Non-pegylated liposomal
doxorubicin
20 mg/m² q1w

Presented at the 2013 ASCO Annual Meeting. Presented data is the property of GBG and AGO-B.
Key Eligibility Criteria*
untreated, uni- / bilateral, primary breast
carcinoma
TNBC (ER and PgR <1%) or HER2-pos BC
(IHC Score 3+ or FISH pos.) by central pathology
breast lesion 2 cm by palpation
or 1 cm by ultrasound
tumor stages (M0):
cT2, cT3, or cT4a-d or
cT1 and cN+ or pNSLN+
*von Minckwitz et al, Ongoing trials, ASCO 2011

Presented at the 2013 ASCO Annual Meeting. Presented data is the property of GBG and AGO-B.
Patients & Tumor Characteristics
PM PMCb
(N=293) (N=295)
age (median yrs) 47 48
palpable T-size (median cm) 3.0 3.0
% %
cT 3 / 4 18.8 16.9
cN + 42.4 37.6
grade 3 64.5 65.1
TNBC (N=315) 53.6 53.6
HER2-positive (N=273) 46.4 46.4
- HER2-positive / HR-negative 18.8 18.3
- HER2-positive / HR-positive 27.6 28.1

Presented at the 2013 ASCO Annual Meeting. Presented data is the property of GBG and AGO-B.
Flow of Patients (N=595)
PM PMCb N N
Randomized 299 296
Started treatment 293 295
% %
Discontinued all treatments
adverse event 31.5 37.7
investigator‘s decision 2.1 2.8
patient’s wish 3.5 5.2
progressive disease 0.7 1.7
death* 1.4 0.3
Completed 6 cycles of treatment 60.9 52.2 *PM: TNBC: acute myocardial infarction (1), febrile neutropenia (1); HER2+: asystole (1), pneumonia (1)
PMC: TNBC: sepsis after port infection (1)

Presented at the 2013 ASCO Annual Meeting. Presented data is the property of GBG and AGO-B.
pCR Rates by Subtype
37.9% 58.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PM PMCb
TNBC
36.3% 33.1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PM PMCb
HER2-positive
P<0.05 n.s.
ypT0 ypN0
N=157 N=158 N=136 N=137

PrECOG 0105 Schema PI: Melinda Telli, MD
Every 21 days x 6 cycles
n = 80
Definitive
Surgery
Assess
Pathologic
Response
Carboplatin AUC 2 D 1, 8
Gemcitabine 1000 mg/m2 D 1, 8
Iniparib 5.6 mg/kg D 1, 4, 8, 11
Newly
Diagnosed
Stage I-IIIA (T 1cm by MRI)
Triple-negative (ER/PR ≤ 5%)
or
BRCA1/2
mutation
Primary Endpoint: Pathologic complete response (pCR) [no invasive disease in breast + axilla]
Secondary Endpoint: Correlation of gene expression profiles & gene copy number with response

Iniparib (BSI-201)
Initially investigated as a PARP1 inhibitor
Subsequently observed that iniparib does not possess
characteristics typical of the PARP inhibitor class
Iniparib is a pro-drug activated through nitro-reduction
Balance between activation <-> inactivation via glutathione conjugation
Iniparib metabolites uncouple electron transport from
oxidative phosphorylation in cell lines
Produce reactive oxygen species at cytotoxic levels1
1. Licht S et al. Mol Cancer Ther 2011;10(11 Suppl): Abstract A226

Statistical Analysis
The primary analysis included patients registered with the intent-to-treat for 6 cycles
Efficacy analyses performed on all eligible patients
Safety analyses performed on all patients who received at least 1 dose of trial therapy
Assuming 76 of 80 patients were eligible & treated:
Regimen would be deemed of interest if lower bound of 90% exact binomial confidence interval (CI) on the pCR rate exceeded 25%
87.5% power to detect 15% absolute improvement from 25% to 40% in pCR rate, using binomial test with 1-sided alpha level of 5%

Results
Patient Characteristics (n=80)
Age, median (yrs) 48 26-73 (range)
n %
Clinical Stage
I 10/80 13%
IIA 29/80 36%
IIB 29/80 36%
IIIA 12/80 15%
Breast Cancer Subtype
ER-/PR-/HER2- 77/80 96%
ER and/or PR+/HER2- 3/80 4%
Germline BRCA1/2 status
BRCA1 mutation 14/80 18%
BRCA2 mutation 4/80 5%
BRCA1 & BRCA2 mutation 1/80 1%

Molecular Subtype Distribution
PAM 50
Subtype1
n = 65
65 patients with GE 51 passed TNBC subtype filter
Vanderbilt
TNBC Subtype2
n = 51
1. Parker JS, et al. J Clin Oncol 2009; 2. Lehmann BD, et al. J Clin Invest, 2011

Results ITT population
Pathologic Response (n=80)
All patients
*******
n = 80
BRCA 1/2
wild-type
n = 61
BRCA 1/2
mutant
n = 19
TN & BRCA
1/2 mutant
n = 16
pCR [RCB 0]; n (%) 29 (36%) 20 (33%) 9* (47%) 9* (56%)
90% CI 27–46 23–44 27-68 33-77
RCB 0/1; n (%) 45 (56%) 31 (51%) 14 (74%) 12 (75%)
90% CI 46-66 40-62 52-89 52-91
* One BRCA1 carrier had bilateral TNBC & achieved pCR in both breasts
Target: lower bound of 90% exact binomial CI pCR rate exceeds 25%
87.5% power to detect 15% absolute improvement from 25% to 40% in pCR rate (binomial test with 1-sided alpha level of 5%)

Perc
en
t
Responders
(RCB 0-1%)
Non-responders
(RCB 2-3%)
n = 8 n = 2 n = 14 n = 4 n = 14 n = 3 n = 6
Results Pathologic response in TNBC subtypes
•
•
•
•
• •
• BRCA1/2
mutant
• • •
• •
n = 51

Grade 3/4 Adverse Events (possibly, probably, definitely related to GCI) CTCAE 3.0
Grade 3
n (%)
Grade 4
n (%)
Neutropenia*
Febrile neutropenia
33 (41%)
0
6 (8%)
0
ALT elevation 12 (15%) 0
Anemia 8 (10%) 0
AST elevation 7 (9%) 0
Thrombocytopenia 4 (5%) 2 (3%)
Fatigue 2 (3%) 0
Subdural hematoma 0 1 (1%)
Cerebrovascular accident 0 1 (1%)
Pulmonary embolism 0 1 (1%)
Headache 1 (1%) 0
Nausea 1 (1%) 0
Vomiting 1 (1%) 0
Flu-like illness 1 (1%) 0
Urinary tract infection 1 (1%) 0
* 99% received at least one dose of filgrastim or pegfilgrastim Grade 2 alopecia = 5%
Grade ≥ 2 neuropathy = 1%

Homologous Recombination Deficiency
(HRD) Assay
Goal:
To detect a genomic HR deficiency ‘footprint’ in a tumor caused by various defects in the HR pathway
Potential to identify non-BRCA1/2 mutation carriers with ‘BRCA-like’ cancers who may benefit from DNA repair targeted treatment strategies
Assay development:
Association of genomic patterns of loss of heterozygosity (LOH) & HR deficiency assessed in ovarian cancer
Major Finding:
LOH regions of intermediate size were observed more frequently in tumors with defective BRCA1 or BRCA2
HRD Score = Count of the # of LOH regions of intermediate size (> 15 Mb and < whole chromosome) observed in the tumor genome
Abkevich V, et al. British Journal of Cancer, 2012

Rate of Favorable Response (RCB 0/1)
by HRD Score
p = 0.0001
Telli ML, Timms K, Hartmann A-R, Ford JM, et al. SABCS 2012; abstract PD09-04
HRD score
Non-responders
BRCA1/2 intact responders
BRCA1/2 mutant responders

Conclusions
The study met the primary endpoint with a pCR rate of
36% (90% CI 27- 46) in the intent-to-treat population
Given the non-randomized nature of this study, the
relative contribution of iniparib therapy cannot be
assessed
The regimen was well tolerated and the safety
experience was similar to that observed in prior studies
Alopecia and neuropathy were uncommon

Conclusions
Germline BRCA1/2 mutation carriers had a higher rate
of response compared to non-carriers
Pathologic response varied among TNBC subtypes
11/14 (79%) of immunomodulatory (IM) subtype pts responded
No luminal androgen receptor (LAR) subtype pts responded
HRD score was significantly correlated with pathologic
response
70% of patients with HRD score ≥ 10 responded compared with
20% of patients with HRD score < 10 (p=0.0001)

E5112: Randomized Phase II Triall of
Neoadjuvant AC-T vs. Carboplatin plus
Gemcitabine in TNBC
PI: Melinda Telli
S U R G E R Y
HRD Assay in
CLIA Lab
R A N D O M I Z A T I O N
Dose Dense AC-T (8 doses, 16 weeks)
Carbo/Gem x 6 cycles (12 doses, 18 weeks)
Radiotherapy after completion of adjuvant chemotherapy and
radiation therapy
1:1 Randomization & stratify:
• HRD: High vs Low
• T: < 2 vs. 2-4 vs. > 4 cm
• N: Pos vs. Neg
• ER/PR: Pos vs. Neg
• Clinical stage: II-III disease
• Subtype: • TNBC • BRCA1/2 pos • ER/PR pos & </45 years
or meeting NCCN criteria for BRCA testing
• Candidate for neoadjuvant chemotherapy
REGISTER
• Primary endpoint: invasive pCR in breast/nodes in high HRD group
• 85% power to detect 20% improvement in pCR in high HRD group (30% vs. 50%), and 80% in low
HRD group (30 vs. 50%) and overall population (30% vs. 45%)
• N=352 randomized (232 in high HRD group) , 25 patients/month, total duration 14 months

High residual disease burden (RDB) in the post-treatment,
surgically-excised cancers has been shown to correlate with
a high rate of recurrence and death in TNBC
von Minckwitz, JCO 2012 Liedtke, JCO 2008

Prognostic Effect of Mitotic Count after Neoadjuvant Chemotherapy
Susan Feinberg, MD BCRT 2013
Age(years) Mean 52.9
Median 52
Range 29-83
SurgicalProcedure
Mastectomy 60(75%)
Lumpectomy 20(25%)
AxillarySurgery
SentinelLymphNodesOnly
12(15%)
AxillaryDissection 67(84%)
NoAxillarySurgery 1(1%)
AJCCyTStage
T0 12(15%
Tis 2(2.5%)
T1 29(36%)
T2 26(32.5%)
T3 6(7.5%)T4 4(5%)
Unknown 1(1%)
AJCCyNStage
N0 29(36%)
N1 15(19%)
N2 19(24%)
N3 7(21%)
RCBScore
RCBScore
0 13(16.3%)
I 9(11.3%)
II 15(18.7%)
III 43(53.7%)

Prognostic Effect of Mitotic Counts in RCB3 (N=43)

Molecular discovery in
drug-resistant residual TNBC (after neoadjuvant chemo)
Balko/ Arteaga, Nat Med 2012
Clinical outcomes of 89 patients with stage II-III basal-like and non-basal-like TNBC with residual disease
after treatment with neoadjuvant chemotherapy
Balko/ Arteaga, unpublished data

E1113: Randomized Phase III Post-
Neoadjuvant Cisplatin in TNBC
PIs: Ingrid Mayer, Vanderbilt University
Standard care: No additional therapy
S U R G E R Y
PAM50 CLIA Lab
R A N D O M I Z A T I O N
Cisplatin 75 mg/m2 every 3 weeks x 4 cycles
Radiotherapy after completion of adjuvant chemotherapy and
radiation therapy
2:1 randomization and stratify:
• PAM50: Basal vs. other
• T: < 2 vs. 2-4 vs. > 4 cm
• N: Pos vs. Neg
• ER/PR: Pos vs. Neg
• Localized breast cancer
• Subtype: • TNBC
• Completed neoadjuvant chemotherapy including anthracycline and taxane
• Residual disease • Breast >/= 1 cm • Or lymph nodes
REGISTER
• Primary endpoint: DFS in basal group
• 80% power to detect 33.3% reduction in DFS hazard rate (median 48 vs. 72 months), assumes 15%
non-adherence, 75% basal subtype
• N=840 randomized (630 in PAM50 basal group) , 12 patients/month, total duration 53 months accrual +
30 months followup

Antiangiogenic Therapy

54
0.0
0.2
0.4
0.6
0.8
1.0
PFS by Treatment
ER Positive, PgR Positive
Months
PF
S P
rob
ab
ilit
y
0 6 12 18 24 30
PB
P
P < 0.0001
Medians: 7, 14.1
0.0
0.2
0.4
0.6
0.8
1.0
PFS by Treatment
ER Negative, PgR Negative
Months
PF
S P
rob
ab
ilit
y
0 6 12 18 24 30
PB
P
P < 0.0001
Medians: 4.7, 8.6
E2100: Weekly paclitaxel alone or plus bevacizumab as first-line
therapy for metastatic breast cancer – outcomes by ER/PR expression
P P+B
All 17% 34%
Measurable
(79%)
17% 41%
P P+B
All 23% 37%
Measurable
(46%)
30% 51%
ER/PR Negative
ER and/or PR Positive

Meta-analysis of First-line Bevacizumab Plus
Chemotherapy in Triple-negative Breast Cancer: Efficacy
• This meta-analysis represents the largest reported
population of patients randomized to treatment for
metastatic TNBC
O’Shaughnessy et al. SABCS 2010; abstract P6-12-03.
Bevacizumab +
chemo
(n = 363)
Chemo
alone
(n = 258)
HR (95% CI) P value
Median PFS (mo) 8.1 5.4 0.649 (0.538-0.783) < .0001
ORR (%) 42 23 NR < .0001
Median OS (mo) 18.9 17.5 0.959 (0.790-1.164) .6732
1-yr OS rate 71 65 NR .1140

Bear et al. NEJM 2012; 366: 310

Von Mickwitz et al. NEJM 2012; 366: 299

CALGB 40603
Triple-negative preop trial
Breast imaging
Blood
MUGA
Tumor Biopsy*
S
U
R
G
E
R
Y
Carboplatin
Paclitaxel
No carboplatin
Breast imaging
Blood
MUGA
Breast imaging
Blood
Dose-dense
AC
RT prn
Bevacizumab
Carboplatin
Paclitaxel
No carboplatin
ER/PR-
HER2-
Stage
II-IIIB

San Antonio Breast Cancer Symposium, 2012 Cameron et al. Lancet Oncology 2013: 14; 933






BEATRICE- Secondary Outcomes
Cameron et al. Lancet Oncology 2013: 14; 933



IDFS by Baseline Plasma VEGF-A
Cameron et al. Lancet Oncology 2013: 14; 933

IDFS by Baseline Plasma VEGFR-2
Cameron et al. Lancet Oncology 2013: 14; 933

Conclusions
• Platinum agents have significant clinical activity
• Several candidate biomarkers (eg, HRD, PAM50 basal)
• Clinical trials in progress and/or development may
establish a role for some of these agents and/or
biomarkers
76