#Dermatologic Drugs 2015-6th Hour-Sheet
12
Integumentary System Dermatologic Drugs 1 Surachai Unchern, Ph.D. School of Medicine, Siam University 1 Preparations for Eczema and Psoriasis, Warts and Calluses Preparations for Eczema and Psoriasis, Warts and Calluses Surachai Unchern, Ph.D. School of Medicine, Siam University Surachai Unchern, Ph.D. School of Medicine, Siam University 2 Eczema is a chronic, inflammatory skin condition that is characterised by • Dryness • Deep-seated itch • Redness and inflammation • Sometimes areas can be weepy or oozing Classification • Atopic eczema – having allergic tendencies (extrinsic) • Non-atopic eczema – not having allergic tendencies (intrinsic) • Regardless of the classification, it is thought that the primary problem is the skin barrier. Eczema Eczema 3 An autoimmune inflammatory and pruritic skin disease. It is a common condition, having been estimated to occur in 10-20% of children and 2-10% of adults. The onset of atopic eczema is usually before two years of age, with only 10% of cases diagnosed after five years of age. Although 60-75% of people experience substantial improvement in their symptoms before adulthood, the remaining 25-40% continue to have relapses during their adult life. Atopic Eczema (Atopic Dermatitis) Atopic Eczema (Atopic Dermatitis) 4 Pathogenesis is multifactorial, involving complex interactions of patient and environmental factors. Defective barrier is critical feature of atopic eczema, with degree of skin barrier damage correlating with severity of disease. With compromised permeability of the barrier, allergens and pathogens can enter the skin and cause secondary inflammation and intense itching and scratching. With changes to lipid component of the stratum corneum, transdermal water loss is increased, which contributes to dryer and rougher skin in people with atopic eczema. Atopic Eczema Atopic Eczema
-
Upload
waiwit-chotchawjaru -
Category
Documents
-
view
7 -
download
0
description
dermatology drugs sheeth#Dermatologic Drugs 2015-6th Hour-Sheet
Transcript of #Dermatologic Drugs 2015-6th Hour-Sheet

Integumentary System Dermatologic Drugs 1
Surachai Unchern, Ph.D. School of Medicine, Siam University
1
Preparations for Eczema and Psoriasis, Warts and CallusesPreparations for Eczema and Psoriasis, Warts and Calluses
Surachai Unchern, Ph.D.School of Medicine, Siam UniversitySurachai Unchern, Ph.D.School of Medicine, Siam University
2
Eczema is a chronic, inflammatory skin condition that is characterised by • Dryness• Deep-seated itch• Redness and inflammation• Sometimes areas can be
weepy or oozing Classification
• Atopic eczema – having allergic tendencies (extrinsic)• Non-atopic eczema – not having allergic tendencies
(intrinsic)• Regardless of the classification, it is thought that the
primary problem is the skin barrier.
EczemaEczema
3
An autoimmune inflammatory and pruritic skin disease. It is a common condition, having been estimated to occur in 10-20% of children and 2-10% of adults.
The onset of atopic eczema is usually before two years of age, with only 10% of cases diagnosed after five years of age.
Although 60-75% of people experience substantial improvement in their symptoms before adulthood, the remaining 25-40% continue to have relapses during their adult life.
Atopic Eczema (Atopic Dermatitis)Atopic Eczema (Atopic Dermatitis)
4
Pathogenesis is multifactorial, involving complex interactions of patient and environmental factors.
Defective barrier is critical feature of atopic eczema, with degree of skin barrier damage correlating with severity of disease.
With compromised permeability of the barrier, allergens and pathogens can enter the skin and cause secondary inflammation and intense itching and scratching.
With changes to lipid component of the stratum corneum, transdermal water loss is increased, which contributes to dryer and rougher skin in people with atopic eczema.
Atopic EczemaAtopic Eczema

Integumentary System Dermatologic Drugs 2
Surachai Unchern, Ph.D. School of Medicine, Siam University
5
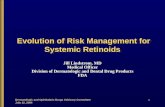
Healthy Skin & Skin with Atopic EczemaHealthy Skin & Skin with Atopic Eczema
6
Atopic eczema tends to be a chronic relapsing disease. Hence, the objectives of treatment are to reduce the frequency and severity of flares and minimize the risk of infection.
To achieve these objectives, treatments for atopic eczema is primarily address the disease components of skin barrier repair, barrier protection, inflammatory moderation and/or immunomodulation.
Treatment OptionsTreatment Options
7
The primary option for barrier protection and repair are emollients, which are considered key therapeutic agents in the ongoing management of dry skin diseases such as atopic eczema.
Topical corticosteroids are first-line treatment for acute exacerbations of atopic eczema. They typically lead to improvement or resolution of acute flares within several days.
Use of lower potency corticosteroids is recommended for children with atopic eczema to minimize risk of adverse effects, including skin atrophy.
Topical TreatmentsTopical Treatments
8
The topical calcineurin inhibitor, pimecrolimus, is an alternative to topical steroids particularly for higher risk areas such as the perioccular and periorbital regions.
Due to a theoretical association with increased cancer risk, however, topical calcineurin inhibitors are reserved for second-line treatment and are generally not used in children aged less than two years.
Topical TreatmentsTopical Treatments

Integumentary System Dermatologic Drugs 3
Surachai Unchern, Ph.D. School of Medicine, Siam University
9
A short course of oral antibiotic therapy may be necessary for widespread secondary bacterial infection, although a topical antibiotic can be used to treat localized infection.
For patients who have atopic eczema that is severe and widespread or refractory to treatment with topical agents, options such as ultraviolet phototherapy and the systemic immunomodulatoryagent, cyclosporin, can be prescribed under the guidance of a dermatologist.
Systemic TreatmentsSystemic Treatments
10
Many compounds are recognized as having skin protective properties, including dimethicone, mineral oil, colloidal oatmeal, paraffin, sodium bicarbonate, cocoa butter, glycerin and lanolin.
The primary agents used as skin protectants in atopic eczema are colloidal oatmeal and paraffin.
Although there is limited evidence that emollients benefit atopic eczema directly, they are widely used because they improve appearance and symptoms of dry skin associated with the disorder and may reduce need for topical corticosteroids.
Emollient TherapyEmollient Therapy
11
Emollients work by helping to repair the skin barrier breakdown. They achieve this by rehydrating the stratum corneum, causing the corneocytes to swell up leading to restoration of the integrity of the skin barrier.
Emollients also help maintain the barrier function by reducing water loss through the skin by occluding the skin surface.
With successful emollient therapy, the skin will become less dry, itchy and irritated. If not, the physicians should re-evaluate their treatment approach.
Emollient TherapyEmollient Therapy
12
Emollients are generally considered safe.
Most commonly reported adverse reaction:
• Stinging or discomfort on application.
• Usually transient and considered a normal response to an application of emollient rather than an adverse reaction.
Emollient TherapyEmollient Therapy

Integumentary System Dermatologic Drugs 4
Surachai Unchern, Ph.D. School of Medicine, Siam University
13
Are the correct emollients being used or should a greasier product be considered?
Is more frequent application needed and/or larger quantities?
Is the patient using soap substitutes when washing?
Is an additional treatment, such as a topical steroid, needed?
Is it possible that there is an underlying condition, such as a contact allergy, that requires referral to a dermatologist?
Evaluation of Emollient Treatment EfficacyEvaluation of Emollient Treatment Efficacy
14
The most important determinant in choosing an emollient is whether it is cosmetically acceptable to the patient and suits their lifestyle.
An emollient that smells and feels acceptable to a patient is also more likely to be used regularly; and one that is disliked will not be used.
Adherence to emollient therapy is likely to be increased if the recommended product meets patient preferences.
Providing patients with trial-sized quantities of different products will allow them to make an informed decision about which they prefer, which could help to improve adherence.
Choosing an EmollientChoosing an Emollient
15
Patients with atopic eczema should liberally apply emollient to their entire body.
Emollients should be continued as a maintenance treatment, even when flares of atopic eczema resolve.
Emollients should be applied as frequently as necessary to maintain skin integrity with a minimum of twice daily.
Emollients should be dotted over the skin and then spread gently to leave a thin film on the skin by using a stroking action in the direction of hair growth.
The emollient should be allowed to absorb before applying other topical products, e.g. corticosteroids.
How Should Emollients be Used?How Should Emollients be Used?
16
There are three main types of emollient formulation:
• Bath or shower additives
• Soap substitutes
• Leave-on formulations
With a three-stage treatment regimen for the application of emollients having been recommended.
How Should Emollients be Used?How Should Emollients be Used?

Integumentary System Dermatologic Drugs 5
Surachai Unchern, Ph.D. School of Medicine, Siam University
17
Stage 1: Bath or shower additives
• Add emollient bath washes to bath water or use emollient shower products when showering.
• They should not be rinsed off the skin, which should be dried by patting gently.
Stage 2: Soap substitutes
• Also known as skin cleansers or synthetic detergents, soap substitutes should be used to wash the skin instead of soap since they have the advantage of being non-drying.
• Soap substitutes should be applied using hands or a wash cloth and then rinsed off.
Three-stage Emollient RegimenThree-stage Emollient Regimen
18
Stage 3: Leave-on formulations
• Use an ointment, gel, cream, lotion or spray if neither bath additives nor soap substitutes prove to be effective.
• Leave-on topical emollients should be applied before going to bed or as soon as possible after showering or bathing to trap moisture into the skin.
Three-stage Emollient RegimenThree-stage Emollient Regimen
19
Oat oil contains a variety of active compounds: lipids with a high percentage of fatty acids, starches, antioxidants and vitamins.
Especially rich in linoleic acid, a lipid that is critical for maintenance of epidermal permeability barrier.
Oatmeal also has a high concentration of starches and beta-glucan, which may contribute to protective and moisture-holding properties.
Colloidal oatmeal has anti-inflammatory effects which partially attributed to avenanthramides(phenolic compounds present in oatmeal).
Preparations: creams, body washes and cleansers.• Well tolerated with no reports of serious adverse events
Colloidal OatmealColloidal Oatmeal
20
Atopic eczema is a common inflammatory pruritic skin condition, the psychosocial and economic burden of which can be considerable.
First-line therapy includes long-term emollient use and then topical corticosteroids during an exacerbation, followed by topical calcineurininhibitors, phototherapy and systemic therapy in more difficult cases.
Emollients, including colloidal oatmeal, are important in the treatment and prevention of skin barrier breakdown.
SummarySummary

Integumentary System Dermatologic Drugs 6
Surachai Unchern, Ph.D. School of Medicine, Siam University
21
The benefits of emollients include restoration of barrier function, increased hydration of the stratum corneum and a potential steroid-sparing effect.
Emollients should be continued after resolution of atopic eczema symptoms to maintain barrier protection and hydration.
Clinical studies have demonstrated the efficacy and safety of colloidal oatmeal emollients as adjunctive treatments in atopic eczema in infants, children and adults.
SummarySummary
22
A disease which affects the skin and joints.
Commonly causes red scaly patches to appear on the skin, “psoriatic plaques”, at areas of inflammation and excessive skin production.
Skin rapidly accumulates at these sites and takes a silvery-white appearance.
Plaques frequently occur on the skin of elbows and knees, but can affect any areas including scalp and genitals.
PsoriasisPsoriasis
23
Inflammatory skin disease in which skin cells replicate at an extremely rapid rate. New skin cells are produced 8 faster than normal, but the rate at which old cells slough off is unchanged. This causes cells to build up on the skin's surface, forming thick patches, or plaques, of red sores.
PsoriasisPsoriasis
24
The disorder is a chronic recurring condition which varies in severity from minor localized patches to complete body coverage.
Fingernails and toenails are frequently affected (psoriatic nail dystrophy) and can be seen as an isolated finding.
Psoriasis can also cause inflammation of the joints, which is known as psoriatic arthritis.
PsoriasisPsoriasis

Integumentary System Dermatologic Drugs 7
Surachai Unchern, Ph.D. School of Medicine, Siam University
25
The cause of psoriasis is not known, but it is believed to have a genetic component.
Several factors are thought to aggravate psoriasis. These include stress, excessive alcohol consumption, and smoking.
Individuals with psoriasis may suffer from depression and loss of self-esteem.
As such, quality of life is an important factor in evaluating the severity of the disease.
Certain medicines, including lithium salt and beta blockers, have been reported to trigger or aggravate the disease.
PsoriasisPsoriasis
26
There can be substantial variation between individuals in the effectiveness of specific psoriasis treatments. Because of this, dermatologists often use a trial-and-error approach to finding the most appropriate treatment for their patient.
The decision to employ a particular treatment is based on the type of psoriasis, its location, extent and severity. The patient’s age, gender, quality of life, comorbidities, and attitude toward risks associated with the treatment are also taken into consideration.
Treatment OptionsTreatment Options
27
Medications with the least potential for adverse reactions are preferentially employed.
As a first step, medicated ointments or creams are applied to the skin. If topical treatment fails to achieve the desired goal then the next step would be to expose the skin to ultraviolet (UV) radiation. This type of treatment is called phototherapy.
The third step involves the use of medications which are taken internally by pill or injection : systemic treatment.
Psoriasis can become resistant to a specific therapy. Treatments may be periodically changed to prevent tachyphylaxis developing and to reduce the chance of adverse reactions occurring: treatment rotation.
Treatment OptionsTreatment Options
28
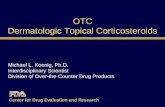
Psoriasis Treatment LadderPsoriasis Treatment Ladder
Incr
easi
ng
Toxi
city
Increasing Effectiveness
Topical
Photo
Systemic

Integumentary System Dermatologic Drugs 8
Surachai Unchern, Ph.D. School of Medicine, Siam University
29
Salicylic acid:
• Keratolytic agents, weak antifungals, antibacterial agents
• Remove accumulated scale, allow topical agents to pass through
• Adverse effects: irritation, salicylism (nausea & vomiting, tinnitus)
Topical TreatmentTopical Treatment
30
Coal tar:
• Preferred for limited or scalp psoriasis
• Can be effective in widespread psoriasis
• Antimitotic, anti-pruritic
• Not quick onset but longer remission
• Often combined with salicylic acid, UV light therapy
• 2 types: crude coal tar and liquor picis carbonis
Topical TreatmentTopical Treatment
31
Dithranol:
• May restore normal epidermal proliferation and keratinization
• Useful in thick plaque psoriasis
• Commonly used with salicylic acid
• 2 treatment approach: long contact and short contact
• Stains clothes, irritating to normal skin
Topical TreatmentTopical Treatment
32
Topical TreatmentTopical Treatment
Topical corticosteroids:
• Anti-inflammatory, immunosuppressive
• Quick onset than coal tar and dithranol
• Tachyphylaxis can occur
• High potent agents used in severe cases, thick plaques
• Adverse effects: local and systemic
• Should not be stopped abruptly – rebound psoriasis

Integumentary System Dermatologic Drugs 9
Surachai Unchern, Ph.D. School of Medicine, Siam University
33
PhototherapyPhototherapy
UVA, UVB, PUVA (Psoralen + UVA psoralencross-links with DNA in the presence of UVA radiation)
UVB preferred
Administered by lamp, sunlight exposure alone or in combination with another topical agent
PUVA (methoxsalen) given PO 2 hours before UVA or lotion applied 30 mins before exposure
Adverse effects: itching, edema
34
Immunomodulators
• Cyclosporin, methotrexate commonly used
Antibiotics in case of secondary bacterial infections
Systemic agents are generally recommended for patients with moderate-to-severe disease.
Moderate disease is defined as greater than 5% body-surface area involvement; severe disease is defined by greater than 10%
Systemic TherapySystemic Therapy
35
Psoriasis is a lifelong condition.
There is currently no cure but various treatments can help to control the symptoms. Many of the most effective agents used to treat severe psoriasis carry an increased risk of significant morbidity including skin cancers, lymphoma and liver disease.
Psoriasis does get worse over time but it is not possible to predict who will go on to develop extensive psoriasis or those in whom the disease may appear to vanish.
Individuals will often experience flares and remissions throughout their lives. Controlling the signs and symptoms typically requires lifelong therapy.
SummarySummary
36
Warts are small harmless lesions of the skin
caused by a virus: the human papilloma virus.
The appearance of warts can differ based on the type of wart and where it is located on the body.
Warts are common in children. Most cases occur between ages 12-16 years.
Up to 30% of warts disappear by themselves within 6 months. Most will disappear without any treatment within 3 years.
Warts may recur after treatment and require additional treatments.
WartsWarts

Integumentary System Dermatologic Drugs 10
Surachai Unchern, Ph.D. School of Medicine, Siam University
37
WartsWarts
38
Warts are caused by the DNA-containing human papillomavirus (HPV).
The virus enters the skin after direct contact with viruses kept alive in warm, moist environments such as a locker room, or by direct contact with an infected person.
The entry site is often an areaof recent injury. The incubationtime from when the virus iscontracted until a wart appearscan be 1-8 months.
WartsWarts
39
Home care is effective in making the wart or warts go away. No matter what technique you use, warts will disappear 60-70% of the time.
Techniques may be done with and without medication.
The ultimate goal of the medical therapies (not the surgical treatments) is to get your body to recognize the wart as something foreign and to destroy it, much like the body destroys a cold virus.
TreatmentTreatment
40
Most effective treatment option.
Soak, emery board, acid, occlusion.
Not on face – possible irritation and scarring.
Equivalent or more efficacy than monotherapy with 5-FU, cryotherapy, podophyllin.
After 6 weeks of treatment, 50% of warts resolve.
First Line Therapy: Salicylic Acid First Line Therapy: Salicylic Acid

Integumentary System Dermatologic Drugs 11
Surachai Unchern, Ph.D. School of Medicine, Siam University
41
Salicylic acid is available by many different trade names at the drug store.
It comes either as a liquid to paint on the wart or as a plaster to be cut out and placed on the wart tissue.
The area with the wart should be soaked in warm water for 5-10 minutes.
The wart should then be pared down with a razor. A simple razor works fine for this, then throw it away.
Do not shave far enough to make the wart bleed. Apply the salicylic acid preparation to the wart tissue. Do not apply it to other skin because of salicylic acid's
potential to injure normal tissue. Follow directions on the package for how long to apply
the acid.
Salicylic Acid TherapySalicylic Acid Therapy
42
Contraindicated in Reynaud's disease if treating hand/foot warts.
• Reynaud's disease causes some areas of your body such as your fingers and toes to feel numb and cold in response to cold temperatures or stress.
Aggressive use over superficial nerves on the volar or lateral aspects of the proximal phalanges of the fingers has caused neuropathy.
White halo for 5-20 sec. improves effectiveness.
Permanent nail changes may occur if the nail matrix is frozen.
Hypopigmentation is a possible complication.
Second Line Therapy: CryotherapySecond Line Therapy: Cryotherapy
43
Liquid nitrogen or cryotherapy is used to deep freeze the wart tissue.
With liquid nitrogen applied to the wart, the water in the cells expands, thus exploding the infected tissue.
The exploded cells can no longer hide the human papillomavirus from the body's immune system.
The immune system then works to destroy the virus particles.
Periungual area may scar if cryotherapy with liquid nitrogen is used improperly.
Scarring could lead to permanent nail disfiguration.
CryotherapyCryotherapy
44
Lasers are simply very intense light sources. This light has an enormous amount of energy that heats the tissue enough that it vaporizes.
Laser surgery uses an intense beam of light, or laser, to burn and destroy the wart tissue. It is usually done in a doctor's office or clinic.
Local or general anesthetic may be used, depending on the number of warts to be removed or the size of the area to be treated.
Laser TherapyLaser Therapy

Integumentary System Dermatologic Drugs 12
Surachai Unchern, Ph.D. School of Medicine, Siam University
45
Place several layers of waterproof adhesive tape over the wart region (even duct tape).
Do not remove the tape for 6-1/2 days. Then take off the tape and open the area to the air for 12 hours.
Reapply tape for another 6-1/2 days.
The tape works best in the region around the fingernail.
Tape works because the air-tight, moist environment under the tape does not allow the virus to grow and reproduce
Adhesive Tape TherapyAdhesive Tape Therapy
46
Shave removal and electrodessication of the base may be necessary when other treatment methods fail.
This would involve numbing the region around the wart and shaving the wart flat with the surface and light electrodessication of the base.
Shave RemovalShave Removal
47
Avoid touching warts on others or touching them on yourself (refrain from rubbing a warty finger across your face).
Children needs to avoid biting or chewing warts.
Wear shower shoes in the gym locker room to lower your risk of picking up the virus that causes plantar warts from the moist environment.
PreventionPrevention
48
Treatments of warts
• Topical salicylic acid
• Cryotherapy or laser therapy
• Duct tape or moleskin
• 5-FU with occlusive dressing
SummarySummary