
dentate mouth
5
Annals of the Royal College of Surgeons of England (I974) vol 55 Precision attachments for the partially dentate mouth H W Preiskel MDS MSC FDSRCS Consultant, Department of Dental Prosthetics, Guy's Hospital, London Smnmary Some uses of precision attachments in re- storing the partially dentate mouth are con- sidered. These devices are indicated where neither the clasp-retained denture nor the fixed bridge is entirely suitable. Introduction The broadening scope of the examination for the Fellowship in Dental Surgery now requires candidates to be familiar with modem meth- ods of restoring the partially dentate mouth. This summary of a lecture which was given in a recent FDS course outlines some of the applications of precision attachments in this field. Despite noteworthy efforts by the Etrus- cans and by the Romans, functional dental prostheses have a comparatively short history. Fauchard in 1728' and Mouton in I 7502 contributed to partial denture designs, but De la Barre (I82o)3 and Schange (I84I)4 probably constructed the earliest effective par- tial dentures. Towards the end of the igth century Parr, Peeso, Chayes, and other experts were able to provide a reasonable standard of bridge- work. They also designed gadgets sub- sequently called precision attachments. These devices allowed prostheses to combine the advantages of fixed and of removable restorations. The development of precision attachments has paralleled that of dentistry itself-an initial restricted interest in mechan- ical technique later supplemented with an understanding of biological principles. Any restoration placed in the mouth has to satisfy demanding criteria on both counts. While the fixed bridge or clasp-retained den- ture is usually the restoration of choice, attachments have to be employed where neither of these two would be satisfactory. Intracoronal attachments Most intracoronal attachments consist of a parallel-sided flange engaging a slot. Vertical space of at least 4 mm and buccolingual space of 3 mm is usually required. Where vertical space is restricted a laboratory-produced Channel Shoulder Pin system5 can be em- ployed. Retention is provided by a series of parallel-sided pins augmented by guiding grooves. Small bounded spaces, with appreciable bone loss, may be restored with intracoronal attachments. Making the prosthesis remov- able simplifies oral hygiene practice and allows artificial mucosa to replace missing bone (Fig. i). The prosthesis is little bulkier than the tissues it replaces, yet it is well re- tained by the attachments. Where larger restorations are involved,
-
Upload
doannguyet -
Category
Documents
-
view
228 -
download
2
Transcript of dentate mouth

Annals of the Royal College of Surgeons of England (I974) vol 55
Precision attachments for the partially
dentate mouth
H W Preiskel MDS MSC FDSRCS
Consultant, Department of Dental Prosthetics, Guy's Hospital, London
SmnmarySome uses of precision attachments in re-storing the partially dentate mouth are con-sidered. These devices are indicated whereneither the clasp-retained denture nor thefixed bridge is entirely suitable.
IntroductionThe broadening scope of the examination forthe Fellowship in Dental Surgery now requirescandidates to be familiar with modem meth-ods of restoring the partially dentate mouth.This summary of a lecture which was givenin a recent FDS course outlines some of theapplications of precision attachments in thisfield.
Despite noteworthy efforts by the Etrus-cans and by the Romans, functional dentalprostheses have a comparatively short history.Fauchard in 1728' and Mouton in I 7502contributed to partial denture designs, butDe la Barre (I82o)3 and Schange (I84I)4probably constructed the earliest effective par-tial dentures.Towards the end of the igth century Parr,
Peeso, Chayes, and other experts were ableto provide a reasonable standard of bridge-work. They also designed gadgets sub-sequently called precision attachments. Thesedevices allowed prostheses to combine theadvantages of fixed and of removable
restorations. The development of precisionattachments has paralleled that of dentistryitself-an initial restricted interest in mechan-ical technique later supplemented with anunderstanding of biological principles.Any restoration placed in the mouth has
to satisfy demanding criteria on both counts.While the fixed bridge or clasp-retained den-ture is usually the restoration of choice,attachments have to be employed whereneither of these two would be satisfactory.
Intracoronal attachmentsMost intracoronal attachments consist of aparallel-sided flange engaging a slot. Verticalspace of at least 4 mm and buccolingual spaceof 3 mm is usually required. Where verticalspace is restricted a laboratory-producedChannel Shoulder Pin system5 can be em-ployed. Retention is provided by a series ofparallel-sided pins augmented by guidinggrooves.
Small bounded spaces, with appreciablebone loss, may be restored with intracoronalattachments. Making the prosthesis remov-able simplifies oral hygiene practice andallows artificial mucosa to replace missingbone (Fig. i). The prosthesis is little bulkierthan the tissues it replaces, yet it is well re-tained by the attachments.Where larger restorations are involved,

Precision attachments for the partially dentate mouth
FIG. I Intracoronal attachments allow theconstruction of a neat, well-retained prosthesisinicorporating artificial mucosa.
intracoronal attachments may replace claspsas a means of retaining partial dentures. Theattachment engages within the crown contourand provides a better-looking, neater, andmore effective connection than is usually ob-tained with a clasp.The precise path of insertion and with-
drawal provided by the atttachments preventsrotational movements of the denture baseaway from the mucosa-particularly usefulwhen distal extension restorations are made.Splinted abutment teeth are usually neces-
sary if transmitted loads are to be withstoodwith safety.
Another application of intracoronal attach-ments is to join in the mouth a series ofcrowns that do not share a common pathof insertion. Devitalization of tilted abutmentsmay thus be avoided. Larger-span bondedgold and porcelain restorations may be splitinto sections. Connecting each section with an
intracoronal attachment minimizes the effectsof dimensional changes of the metal that mayaccompany porcelain firing.
For retaining partial dentures semiprecisionrests are simpler and more economical to em-
ploy than precision attachments. Fewer abut-ment preparations may be involved, but a
separate retaining arm is required.Intracoronal attachments have a variety of
applications. Clinical and laboratory tech-niques are demanding, but the results com-
pensate for the time and skills required.
Extracoronal attachmentsUnlike intracoronal attachments these unitsneed no space within the abutment crownand are unrestricted by pulpal considerations.They may be employed where buccolingualspace is limited-particularly useful wherelower canines are the most distal abutments.Extracoronal attachments are often employedto retain bilateral distal extension prostheses.
Because mucosa is more readily displacedthan natural teeth many extracoronal attach-ments are designed to allow play between thecomponents-a technique mis-termed 'stress-breaking'. Since we find that continual ver-tical denture movements exceeding 0.3 mmare likely to damage the distal gingivae, wenow concentrate on producing stable, well-supported prostheses that do not requireto make perceptible movements. The move-ment allowed by some extracoronal attach-ments should be regarded as a safety valveand not as a means of anchoring an unstableprosthesis to natural teeth.
Extracoronal attachments transmit verticalloads away from the long axes of the abut-ment teeth, a drawback overcome by splintedabutments and a well-constructed denture.These attachments should not be placed dis-tal to a cantilevered pontic as the leverage ofthe loads applied may then reach damagingproportions.
Extracoronal attachments are often mosteffective denture retainers and invisible whenthe removable prosthesis is in place (Fig. 2).Regular inspection and maintenance is essen-tial to avoid the vicious circle of denturemovement contributing to ridge resorptionand more denture movement.
Complete overlay dentureThe complete overlay denture derives addi-tional retention and support from the remain-ing roots. While the periodontium of the rootcontributes to denture support, its functions gofurther6. Within the periodontium are pro-
295

296 H W Preiskel
poor plaque control.Stud attachments are simple and versatile
.~~~ii connecting a complete overlay denture tothe root. Bar joint attachments serve a sim-
function but splint the remaining roots(a) ij(Fig 3). Their applications are limited by the
vertical and labiolingual space they require.Bar joints and most stud attachments allowsome slight vertical play.
Bar units employ parallel-sided bars and,unlike bar joints, there is virtually no play
; i _ ~~~~~~~~Artificial mucosa may be incorporated and
|!! _ g _ ; ~~~~Additional rtention by pins or plungers canbe incorporatedbetween thesleeve and bar.
FIG. 2 Partial denture retained by two Dalbo Telescopic prosthesesextracuronal attachments: (a) fixed section Telescopic prostheses are made in two layerson master cast; (b) assembled prosthesis in and union of teeth can be achieved by jointthe mouth. ep ..
prioceptors of remarkable sensitivity whose /(il ltactile discrimination often surprises investi- t\gators and practitioners alikeb i. Brill et al." b 31 ba1f eltthat loss of natura ltooth proprioception \ \following extractionwould b ecompensated T t a m ifor by a co-ordination of sensory signalsfrom c b acithe temporomandibularJoints and denture-bearing areas, but this has not been borne .mout by other investigators'2. Anterior teethi; . :,. ijmay be more sensitive than others'-" , whileal.the canines may be the most sensitive ofall"g6.Removal of pulpaltissuedoesnot ap-;o-
pear to make a significant difference to tactile ' . - ..sensitivity""7. Considering the possible bene- . 2ficial effect of retained roots on mandibular .,">.v:- 'resorption18"9 there is much to be said for .; .:Xpreserving canine roots. A weak point in theconstruction is the necessity to cover the gin- FIG. 3 Diauram of a complete overlay dengival margins, a potential source of irritation ture wvith additional retention provided byaggravated by denture base movement and a Dolder bar.
Precision attachments for the partially dentate mouth
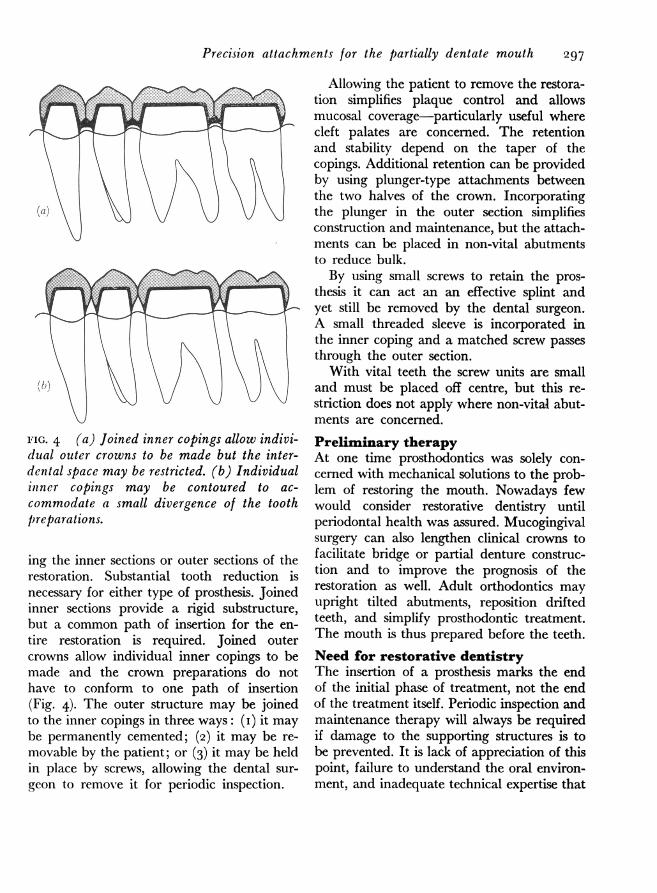
FIG. 4 (a) Joined inner copings allow indivi-duzal outer crowns to be made but the inter-dental space may be restricted. (b) Individualinner copings may be contoured to ac-
commodate a small divergence of the toothpreparations.
ing the inner sections or outer sections of therestoration. Substantial tooth reduction isnecessary for either type of prosthesis. Joinedinner sections provide a rigid substructure,but a common path of insertion for the en-
tire restoration is required. Joined outercrowns allow individual inner copings to bemade and the crown preparations do nothave to conform to one path of insertion(Fig. 4). The outer structure may be joinedto the inner copings in three ways: (i) it maybe permanently cemented; (2) it may be re-
movable by the patient; or (3) it may be heldin place by screws, allowing the dental sur-
geon to remove it for periodic inspection.
Allowing the patient to remove the restora-tion simplifies plaque control and allowsmucosal coverage-particularly useful wherecleft palates are concerned. The retentionand stability depend on the taper of thecopings. Additional retention can be providedby using plunger-type attachments betweenthe two halves of the crown. Incorporatingthe plunger in the outer section simplifiesconstruction and maintenance, but the attach-ments can be placed in non-vital abutmentsto reduce bulk.By using small screws to retain the pros-
thesis it can act an an effective splint andyet still be removed by the dental surgeon.A small threaded sleeve is incorporated inthe inner coping and a matched screw passesthrough the outer section.
With vital teeth the screw units are smalland must be placed off centre, but this re-striction does not apply where non-vital abut-ments are concerned.
Preliminary therapyAt one time prosthodontics was solely con-cerned with mechanical solutions to the prob-lem of restoring the mouth. Nowadays fewwould consider restorative dentistry untilperiodontal health was assured. Mucogingivalsurgery can also lengthen clinical crowns tofacilitate bridge or partial denture construc-tion and to improve the prognosis of therestoration as well. Adult orthodontics mayupright tilted abutments, reposition driftedteeth, and simplify prosthodontic treatment.The mouth is thus prepared before the teeth.
Need for restorative dentistryThe insertion of a prosthesis marks the endof the initial phase of treatment, not the endof the treatment itself. Periodic inspection andmaintenance therapy will always be requiredif damage to the supporting structures is tobe prevented. It is lack of appreciation of thispoint, failure to understand the oral environ-ment, and inadequate technical expertise that
297

298 H W Preiskel
are the major contributors to the high in-cidence of iatrogenic disturbances that we allsee. A sound restoration, be it a small inlayor a complete denture, should protect its sup-porting structures and is therefore an im-portant preventive measure. While otherpreventive measures will, it is hoped, reducethe devastation of caries and periodontal dis-ease, restorative dentistry will always hold thecritical-and final-second line of defence.With about 22 million denture wearers inEngland and Wales, many below the age of35, the need to provide sound restorative den-tistry for generations to come is apparent.In fact the increasing life expectancy of ourpopulation is likely to enlarge the scope ofrestorative dentistry in the future.Over the next few years we may look for-
ward to a change of emphasis in restorativedentistry. Dental surgeons will require abroad-based education together with technicalknowledge and ability to enable them bothto understand and to treat the problems thatconfront them. The restoration of the partiallydentate mouth will continue to tax thtingenuity of the dental practitioner, whileprecision attachments will continue to providelimited but valuable assistance where conven-ventional prostheses are unsuitable.I would like to thank Professor K P Liddelow forhis help with this manuscript, Mr J D Walter forhis assistance with the historical aspects of the paper,and Messrs Henry Kimpton for permission to useillustrations from my textbook.
Referencesi Fauchard, P (1728) Le chirurgien dentiste. Mari-
ette, Paris.
2 Mouton, C (1746) Essay d'odontotechnie ou dis-sertation sur les dents artificielles. Boudet, Paris.
3 De La Barre, C F (I820) Traite de la partiemecanique de l'art du chirurgien-dentiste.Croulebois, Paris.
4 Schange, J M A (I84I) Precis sur le redressementdes dents. Bechet Jeune et Late, Paris.
5 Steiger, A A, and Boitel, R (1959) PrecisionWork for Partial Dentures. Stebo, Zurich.
6 Crum, R J, and Loiselle, R J (1972) Journal ofProsthetic Dentistry, I2, I23.
7 Hannam, A G, Mathews, B, and Yemm, R(I968) Archives of Oral Biology, 13B, 36I.
83 Anderson, D J, Hannam, A G, and Mathews, B(1970) Physiological Reviews, 50, 171.
9 Tryde, G, Frydenburg, 0, and Brill, N (I962)Acta odontologica Scandinavica, 25, 563.
io Shrila, H, and Laine, (I963) Acta odonto-logica Scandinavica, 21, 415.
I IBrill, N, Schubbeler, S, and Tryde, G (I962)Journal of Prosthetic Dentistry, I 2, I23.
I2 Kawamura, Y and Watanabe, M (i960) MedicalJournal of Osaka University, I0, 291.
13 Kawamura, Y (I964) in Advances in Oral Bio-logy, ed P E Staple, Academic Press, New York.
I4 Grossman, R C (I964) Journal of Dental Re-search, 43 (suppI.), 833.
T5 Kruger, L, and Michel, F (I962) Archives ofOral Biology, 7, 49I.
16 Bonaguro, J G, Dusza, G R, and Bowman, D C(I969) Journal of Dental Research, 48, 236.
17 Adler, P (I947) Journal of Dental Research,26, 279.
I8 Tallgren, A (I967) Acta odontologica Scandinz-vica, 25, 563.
I9 Tallgren, A (I969) Acta odontologica Scandina-vica, 27, 539.


















