Deep Vein Thrombosis
26
Deep Vein Thrombosis Brian M. Johnson, MD CCRMC PBL 11/7/12
description
Deep Vein Thrombosis. Brian M. Johnson, MD CCRMC PBL 11/7/12. Case 1. - PowerPoint PPT Presentation
Transcript of Deep Vein Thrombosis
PowerPoint Presentation
Deep Vein ThrombosisBrian M. Johnson, MDCCRMC PBL11/7/12Case 1Mrs. Z, a 44-year-old woman without significant PMH, presents for an urgent visit with left leg swelling of two days duration. She takes no medications and reports moderate leg pain but no chest pain, shortness of breath, or palpitations.
What is the differential diagnosis of unilateral leg swelling?DVT2. Cellulitis3. Bakers cyst4. Lymphedema5. FracturePost-thrombotic syndromeVenous insufficiencyScorpions? Or bee stings?ToxinsMassTrauma / Compartment syndrome
What are risk factors for DVT?HospitalizationLong-term immobilityOCPSmokingAgeSurgeryCancerCHFRenal diseaseCirrhosisPregnancyAnti-psychoticsThrombophiliasObesityRestrictive clothingGenderLupus (and other autoimmune diseases)Sickle Cell
Case ContinuedShe reports that she has no family history of blood clots to her knowledge and that she is not pregnant. She denies any warning signs of cancer and is up to date on her cancer screening (mammogram, Pap smear; no colorectal cancer screening, but she denies family history of colorectal cancer so she is not yet due). She denies recent immobilization or trauma. Her exam is significant for a minimally swollen right calf. To ensure a reliable assessment of circumference, you mark off 10cm below each tibial tuberosity and measure the circumference at that level. You find that the right calf measures 1cm larger in circumference than the left. There is no edema or skin changes; no masses/cords are palpable. The thighs are symmetric, and no superficial veins are noted.
How could you determine the probability of the DVT in this patient?
What is the probability that this patient has a DVT? Modified WellsClinical feature Score*Active cancer within 6 mo 1 Paralysis, paresis, or cast of lower extremity 1 Recently bedridden >3 d or major surgery within 4 wk 1 Localized tenderness along distribution of deep vein system 1 Calf diameter >3 cm larger than opposite leg1 Pitting edema 1 Collateral superficial veins (nonvaricose) 1 Alternative diagnosis as likely or greater than that of DVT Clinical model for predicting pretest probability for DVT*Interpretation: 0 = low probability = 3% frequency of DVT; 1-2 = medium probability= 17% frequency of DVT; 3 = high probability = 75% frequency of DVT.Measured 10 cm below tibial tuberosity.
-2 How would a d-dimer help?StatisticallySensitive not Specific (useful if its negative)High false positive rateBiomedically measures level of coagulation process in the bodyCase 2Ms. W, comes with the exact same presenting complaint and past medical history. The only difference in the presentation of Ms. W. is that she does report that she had the flu about one week ago and was in bed for four to five days.
Additionally, her exam is significant for a swollen and tender right calf, measuring 4 cm wider in circumference than the left. There is pitting edema on the right lower extremity, extending to the inferior calf. There is no change in the skin, and no masses/cords are palpable. The thighs are symmetric, and no superficial veins are noted. Whats the probability this patient has a DVT?75%!! High, with wells score greater than 3
Whats the value of doing a d-dimer?
If high probability 21% still positive for DVT even with negative D-dimerWhat other test could you preform?
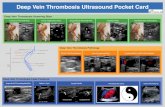
Venous Doppler (venography)
13
13Remember: the superficial femoral vein is a deep veinOperating characteristics of diagnostic tests for proximal DVT* Black et al.
Diagnostic test Sensitivity, % Specificity, % Positive LR Negative LR Venography ~100 ~100 Infinity 0 Duplex ultrasonography 95 95 19 0.05 Impedence plethysmography 80 95 16 0.21 Iodine 125 fibrinogen scan 79 62 2.1 0.34 D-Dimer level 88-100 55-80 1.9-5.0 0.4-0.02 LR = likelihood ratio. *
U/S negative. End of story?With high probability clinical exam but NEGATIVE U/S:Consider other imaging, repeat study or obtain D-dimer.Consider treatment
U/S positive. Can she be treated as an outpatient?YesNeed immediate anticoagulation (i.e. Lovenox) then can bridge to warfarin
NoObesity CacheticRenal failure (GFR 30%Kearon, American Society Hematology Dec. 2004
19This is why duration of therapy is based on provoked vs. unprovokedIs longer anticoagulation better in idiopathic DVT?TRIALDurationRecurrenceDurationRecurrenceTHRIVE3mo7.6/ 100pt yrs2.1 yrs2.6/100pt yrsPREVENT6mo12.6%18 mo2.8%Schulman et al. N Engl J Med 2003 Ridker et al. N Engl J Med. 2003PREVENT: Idiopathic DVTTHRIVE20Do the experts agree with the ACCP recommendations? 8th ACCP guidelineBritish Thoracic SocietyRecent recommendationsFirst VTE,Provoked3 months4-6 weeks3 months if distal or upper extremity; 6 if proximal DVT or PEFirst VTE,IdiopathicAt least 3 months, evaluate for indefinite tx3 monthsIndefinite
21Samuel Z. GoldhaberShould I do the thrombophilia work up?23Incidence of recurrent VTEChristensen et al. JAMA 2005.Patient group (total 474 pt)Recurrence of VTE/yearWith 1 thrombophilia2.5%Initial VTE provoked1.8%Initial VTE idiopathic3.3%Idiopathic with thrombophilia3.4%Idiopathic without thrombophilia 3.2%Total group2.6%23So basically having a thombophilia is much less predictive of recurrence than having an idiopathic VTE. But this is a small study that didnt separate out the thrombophilias individually. Later they do comment that APLA does increase risk of recurrence. Based on this data, both the author of the above study and the author of a recent article in the american journal of medicine (2008) suggests that thrombophilia work up is almost never useful after a first event. They do recommend testing for APLA as it does have a significant impact on risk of recurrence.
24How can I determine whos at risk for recurrent clot?
ThrombophiliaMale genderActive cancer (i.e. ongoing risk factors)Recurrent dvtProximal over distalMorbidity from DVTRepeat studies (US and ddimer)
Algorithm for Determining Duration of TreatmentREFERENCES
Bates SM, Kearon C, Crowther M, et al. A diagnostic strategy involving a quantitative latex D-dimer assay reliably excludes deep venous thrombosis. Annals of Internal Medicine. 2003;138(10):787-794.
Black ER, Bordley DR, Tape TG, Panzer RJ. Diagnostic Strategies for Common Medical Problems. Philadelphia: American College of Physicians; 1999.
Bruinstoop, E., Klok, F. A.,Van de Ree, M. A., Oosterwijk, F. L. and Huisman, M. V., Elevated d-dimer levels predict recurrence in patients with idiopathic venous thromboembolism: a meta-analysis. Journal of Thrombosis and Haemostasis, 2009;7:611618
Ofri D Diagnosis and treatment of deep vein thrombosisWest J Med. 2000 September; 173(3): 194197.
Ridker PM, Goldhaber SZ, Danielson E, Rosenberg Y, Eby CS, Deitcher SR, Cushman M, Moll S, Kessler CM, Elliott CG, Paulson R, Wong T, Bauer KA, Schwartz BA, Miletich JP, Bounameaux H, Glynn RJ, PREVENT Investigators N Engl J Med. 2003;348(15):1425
Rodger et al. Identifying unprovoked thromboembolism patients at low risk for recurrence who can discontinue anticoagulant therapy. CMAJ August 26, 2008 vol. 179 no. 5
Schulman S, Whlander K, Lundstrm T, Clason SB, Eriksson H. Secondary prevention of venous thromboembolism with the oral direct thrombin inhibitor ximelagatran.. N Engl J Med 2003 Oct 30;349:1713-21