Deep Vein Thrombosis
21
Deep Vein Thrombosis Lewis, pp. 882-890 Concept 22.4 pp. 1389- 1397
description
Deep Vein Thrombosis. Lewis, pp. 882-890 Concept 22.4 pp. 1389-1397. Terminology. Sometimes called thrombophlebitis, phlebothrombosis, venous thrombosis, venous thromboembolism Venous thrombosis refers to clot formation in a vein with inflammation Superficial—in small vein (INT site) - PowerPoint PPT Presentation
Transcript of Deep Vein Thrombosis

Deep Vein Thrombosis
Lewis, pp. 882-890
Concept 22.4 pp. 1389-1397

Terminology
• Sometimes called thrombophlebitis, phlebothrombosis, venous thrombosis, venous thromboembolism
• Venous thrombosis refers to clot formation in a vein with inflammation– Superficial—in small vein (INT site)– Deep—AKA: DVT—located in deep veins,
usually iliac or femoral

Etiology
• Virchow’s triad:– Venous stasis
– Damage of endothelium
– Hypercoagulability

Risk Factors for Virchow’s Triad
• Venous stasis —incompetent valves, inactivity, obesity, heart failure, afib, orthopedic and pelvic surgeries
• Endothelial damage—trauma from various causes, external pressure
• Hypercoagulability— blood disorders, sepsis, pregnancy, hormones, smoking

Pathophysiology
• When vein is traumatized, inflammation occurs and platelet aggregation and fibrin attract cells to form a thrombus
• In venous stasis, clot forms at valve cusps or bifurcations.
• If clot gets big enough to occlude vein, manifestations of DVT occur; if not, body will reabsorb it.

Assessment of DVT
• 50% are asymptomatic unless the clot is in the ileofemoral vein.
• Symptomatic patients and those with ileofemoral clot have edema ,redness, pain, warmth, decreased movement, +Homan’s sign (20% reliable).
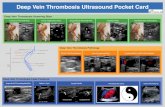
• Dx Tests: Duplex scanning, venogram, D-dimer blood test

Preventative Management
• Antiembolism stockings (TEDs)
• Intermittent compression device (DVT boots, Venodynes)
• Antiembolism exercises (AEEs)
• SQLMWH (Lovenox)
• Early ambulation
• Encourage fluids
• Avoid popliteal pressure, crossing legs

Prevention—Surgical Care Improvement Project
• Started in 1999 to identify and implement ways to decrease postoperative complications
• Research found that in all major surgical procedures that 25% of pts developed DVT and 7% developed pulmonary embolism
• Recommendation was that patients receive prophylaxis within 24h before or after surgery. Could be TEDS, IPCD, LMWH*, ASA.

Core Measures for Venous Thromboembolism (VTE)
• VTE Prophylaxis
• ICU VTE Prophylaxis• VTE Patients with Anticoagulation Overlap
Therapy • VTE Patients Receiving Unfractionated Heparin
with Dosages/Platelet Count Monitoring by Protocol
• Anticoagulant Discharge Instructions

Elements of Performance: In other words, how does the hospital meet this NPSG?
• Reduce the likelihood of patient harm associated with the use of anticoagulant therapy.
– Use only oral unit-dose products, prefilled syringes, or premixed infusion bags and make sure they are age-appropriate.
– Use only programmable pumps when administering continuous IV heparin– Use approved written protocols for initiation and maintenance of therapy.– Use approved written protocols for addressing baseline and ongoing labs t– Assess baseline coagulation status i.e., INR, PT, PTT.– Manage potential food and drug interactions.
– Provide education to prescribers, staff, patients, and families which includes follow-up, compliance, drug-food interactions, adverse reactions
– Evaluate these safety practices, make improvements, and measure their effectiveness.

Acute Management
• Hospital or home?—depends on size of clot and presence of comorbidities
• BR or some degree of ambulation?—EBP has shown no difference
• Heat application
• Extremity elevation

• IV Heparin—bolus followed by infusion with pump—dosage depends on established hospital protocol
• SQ Lovenox q12h—EBP show results as good
• PO Warfarin daily—dosage depends on PT, INR
• Analgesics—not NSAIDs
Acute Pharmacologic Mgmt

Acute Management cont’d
• PTT, PT, INR qam—heparin and warfarin doses depend on results; not needed for Lovenox
• Monitor for complications—50% develop pulmonary embolism
• Surgery—thrombectomy, vena cava filter

Nursing Management of DVT
• Practice prevention for at-risk pts. • For acute cases:
– Monitor VS, NV status, and extremity measurements– Maintain activity orders – Discourage activities that can cause bleeding– Encourage fluids– Monitor anticoagulants meds and labs– Analgesics and heat– Monitor Vit K in diet– Monitor for complications-PE and hemorrhage

Patient Education
• Anticoagulant therapy (890)• Home treatment of DVT (Concept p. 1395)• Prevention• Dietary restrictions related to warfarin tx• Complications • How to give Lovenox at home• Home INR testing• How to apply TEDs

Peripheral Vascular Disease
• Affects arteries and veins• Arteriosclerosis--Narrowing and sclerosis of large
arteries (femoral, iliac, popliteal) especially at bifurcations due to plaque formation
• Chronic Venous Insufficiency—inadequate venous return due to incompetent valves. Venous stasis causes problems with diminished circulation and immune response

Manifestations of PVD
• Arterial:– Diminished or absent pulses– Smooth, shiny, dry skin,– No hair– No edema– Round, painful ulcers on
distal foot, toes or webs of toes
– Dependent rubor– Pallor and pain when legs
elevated– Intermittent claudication– Brittle, thick nails
• Venous:– Normal pulses– Brown patches of
discoloration on lower legs– Dependent edema– Irregularly shaped, usually
painless ulcers on lower legs and ankles
– Dependent cyanosis and pain– Pain relief when legs elevated– No intermittent claudication– Normal nails– Dermatitis, pruritis

Management of Leg Ulcers
• Goals of care:
– Promote skin integrity
– Increase mobility
– Provide good nutrition

Management cont’d
• Promoting skin integrity includes good foot care, avoiding trauma, avoiding pressure and standing for long periods. It also includes proper tx of existing ulcers.
• Increase mobility as allowed and tolerated.
• Good nutrition includes protein, Vits A & C, Fe, Zn, and weight control.

Wound Care Management of Leg Ulcers
• Compression tx—stockings, Unna boots, etc. Amount of compression depends on ABI index.
• Keep wound moist—irrigate with saline, apply moisture-retentive dressings
• Prevent infection using good technique; wound culture if indicated.
• For persistent and unresponsive ulcers, surgical debridement, wound vacs, hyperbaric O2 chambers, or skin grafts may be indicated.

Education
• Good skin and foot care• Teach pt and family to check feet and skin regularly• Proper diet—Vits A & C, Fe, Zn, weight control• Appropriate activity• Avoidance of trauma • S/S infection• May need to teach patient and family dressing
changes