Damage control surgery and resuscitation
42
DAMAGE CONTROL SURGERY AND RESUSCITATION by Phongthorn Tuntivararut, MD , R.Ph . Surgical Residency Police General Hospital, Thailand
-
Upload
phongthorn-tuntivararut -
Category
Health & Medicine
-
view
106 -
download
5
Transcript of Damage control surgery and resuscitation

DAMAGE CONTROL SURGERYAND
RESUSCITATION
by
Phongthorn Tuntivararut, MD, R.Ph.
Surgical Residency
Police General Hospital, Thailand

“The modern operation is safe for the
patient. The modern surgeon must make the
patient safe for the modern operation.”
- Lord Moynihan -

DAMAGE CONTROL SURGERY
• Damage control surgery is one of the major advances in
surgical technique in the past 20 years, including
• Minimizing time at the scene of trauma and in the emergency
department (ED)
• Minimizing admission laboratory testing
• Initiating resuscitation in the operating room for patients with
severe hypotension, cardiac arrest, or external hemorrhage
• Early operative control of hemorrhage
DAMAGE CONTROL SURGERY
• Damage control surgery are performed in injured patients with
profound hemorrhagic shock and preoperative or
intraoperative metabolic unstable that are known to adversely
affect survival

WHO NEEDS DCS??
• Thoracic Trauma
• Penetrating thoracic wound and systolic blood pressure <90
mmHg
• Pericardial fluid on surgeon-performed ultrasound after blunt or
penetrating thoracic trauma
• S/p emergency department thoracotomy for penetrating thoracic
wound
• Trauma to an Extremity
• Shotgun wound to femoral triangle of thigh
Mattox. Trauma 6th Edition

WHO NEEDS DCS??
• Abdominal or Pelvic Trauma
• Penetrating abdominal wound and systolic blood pressure <90
mmHg
• Blunt abdominal trauma, systolic blood pressure <90 mmHg, and
peritoneal fluid on surgeon-performed ultrasound or gross blood
on diagnostic peritoneal tap
• Closed pelvic fracture, systolic blood pressure <90 mmHg, and
peritoneal fluid on surgeon-performed ultrasound or gross blood
on diagnostic peritoneal tap
• Open pelvic fracture
Mattox. Trauma 6th Edition

Why we need Damage Control Surgery ??

ER OR ICU
ER OR Death
OR

“Multiple trauma patients are more likely to
die from their intra-operative metabolic failure
that from a failure to complete operative
repairs”
www.trauma.org

LETHAL TRIADS
• Hypothermia
• Severe hypothermia despite warming maneuvers initiated in the
ED and continuing in the operating room
• Acidosis
• Persistent acidemia despite vigorous resuscitation and control of
hemorrhage
• Coagulopathy

HYPOTHERMIA
• Hypovolemic shock in the preoperative period adversely
affects oxygen delivery and leads to decreases in oxygen
consumption and production of heat
• Hypothermia is the gateway to the triad because almost all
clotting mechanisms are temperature dependent
• Cold inhibits the clotting cascade, leading to coagulopathy
• Platelet dysfunction at low temperature
• Clinically important if less than 37˚C for more than 4 hr

Class I II III IV
Blood loss (ml) <750 750-1,500 1,500-2,000 ≥2,000
%Blood volume lost <15% 15-30% 30-40% ≥40%
Pulse rate <100 >100 >120 >140
Blood pressure Normal Normal Decreased Decreased
Pulse pressure Normal or increased Decreased Decreased Decreased
Capillary refill Normal Delayed Delayed Delayed
Respiratory rate 14-20 20-30 30-40 >35
Urine output(ml/hr) >30 20-30 5-15 Negligible
Mental status Slightly anxious Mildly anxiousAnxious,
confused
Confused,
lethargic
Recommended fluid
replacement0.9%saline, 3:1 0.9%saline, 3:1
0.9%saline+
red cells
0.9%saline+
red cells
ATLS program for physician, student and instructor manual, American College of Surgeons, 1993

COAGULOPATHY
• Unchecked hemorrhage, in turn, decreases blood pressure and
the amount of available oxygen, causing cells to convert to
anaerobic metabolism
• Hypothermia, acidosis and the consequences of massive blood
transfusion all lead to the development of a coagulopathy
• Haemodilution following massive resuscitation
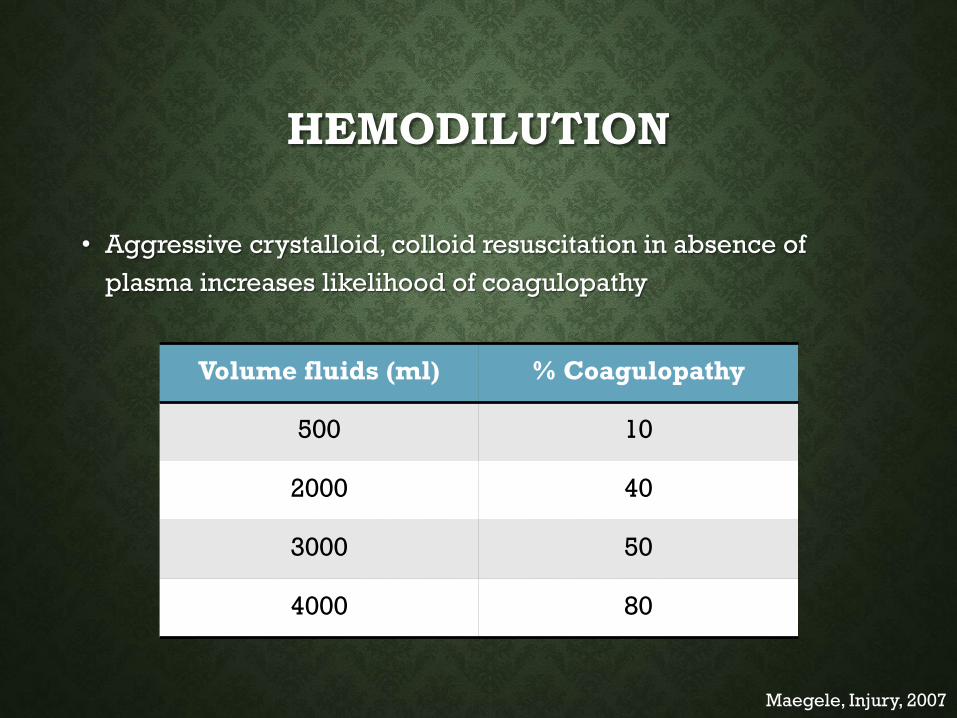
HEMODILUTION
• Aggressive crystalloid, colloid resuscitation in absence of
plasma increases likelihood of coagulopathy
Maegele, Injury, 2007
Volume fluids (ml) % Coagulopathy
500 10
2000 40
3000 50
4000 80

ACIDOSIS
• Interferes with blood clotting mechanisms and promotes
coagulopathy and blood loss
• Can lead to cardiac arrhythmias, decreased cardiac output,
increassed systemic vascular resistance

ER OR ICU OR ICU

Limited operation
Resuscitation
Reoperation
Trauma patients
withMetabolic failure

Mattox. Trauma 6th Edition

LIMITED OPERATION
• Control of hemorrhage from the heart or lung
• Conservative management of injuries to solid organs
• Resection of major injuries to the gastrointestinal tract without
reanastomosis
• Control of hemorrhage from major arteries and veins in the
neck, trunk, or extremities
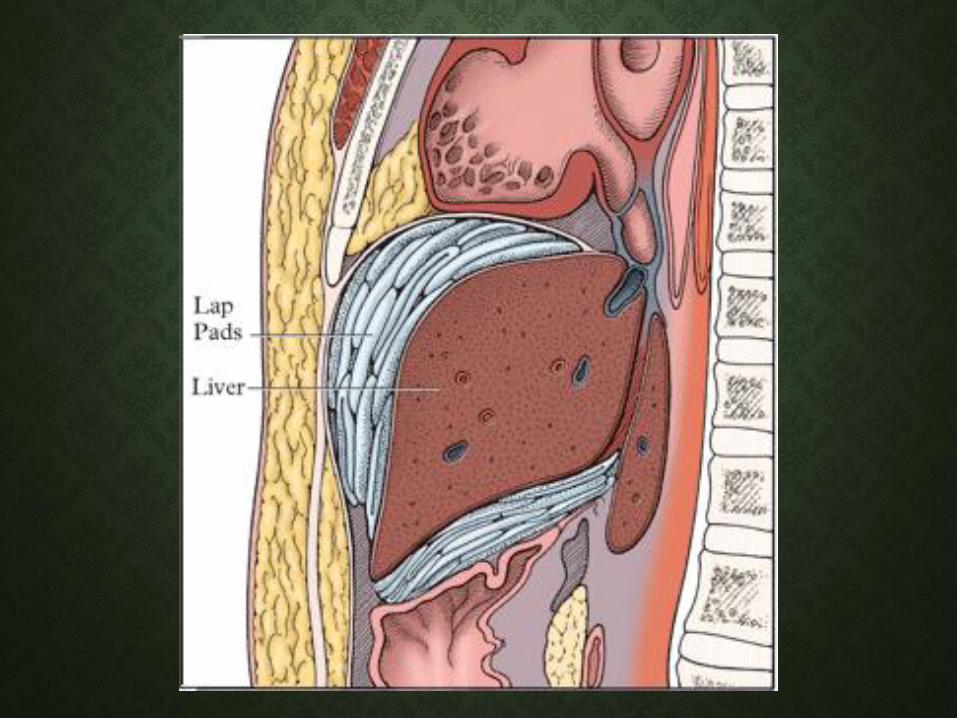
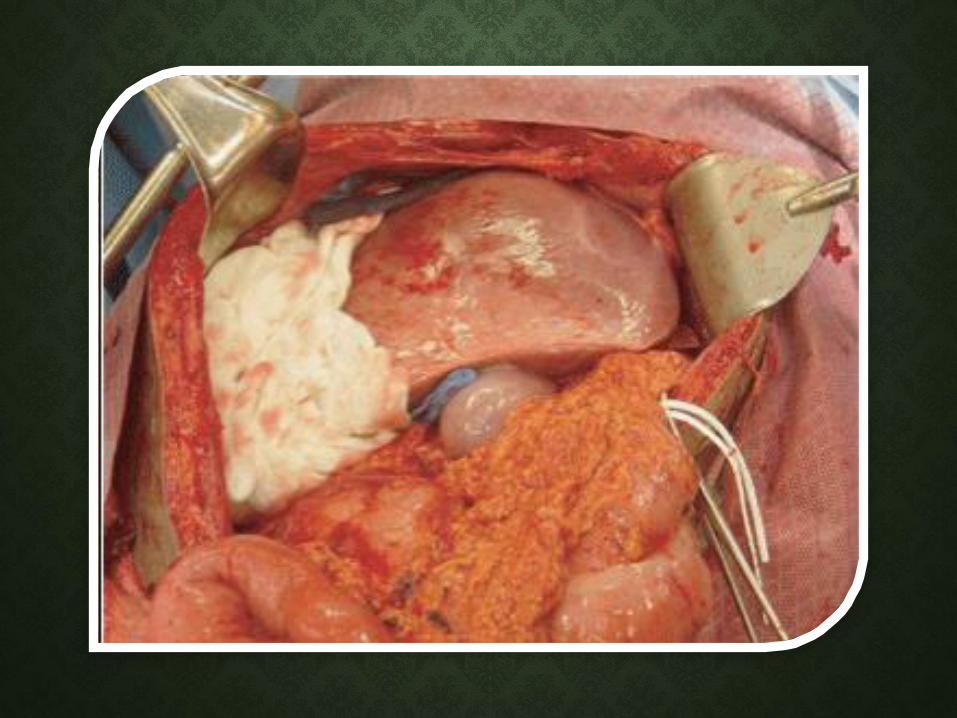
• Packing of organs or spaces to control the inevitable
coagulopathy


RESUSCITATION
• Vigorous rewarming of the hypothermic patient
• Restoration of a normal cardiovascular state by the infusion of
fluids and blood and the use of inotropic and related drugs
• Correction of residual coagulopathy after hypothermia is
reversed
• Supportive care for stunned lungs and kidneys

REWARMING
• Bair Hugger
• Warming light, fluid and
blood product
• Gentilello
• Continuous arteriovenous
rewarming device

COAGULATION MANAGEMENT
• Plasma and platelet transfusion
• The ratio of 2:1:1 or 3:1:1
• Serial coagulation parameters should be monitored
• The administration of recombinant activated factor VII
(Novoseven) may also play a role in the management of a life-
threatening coagulopathy
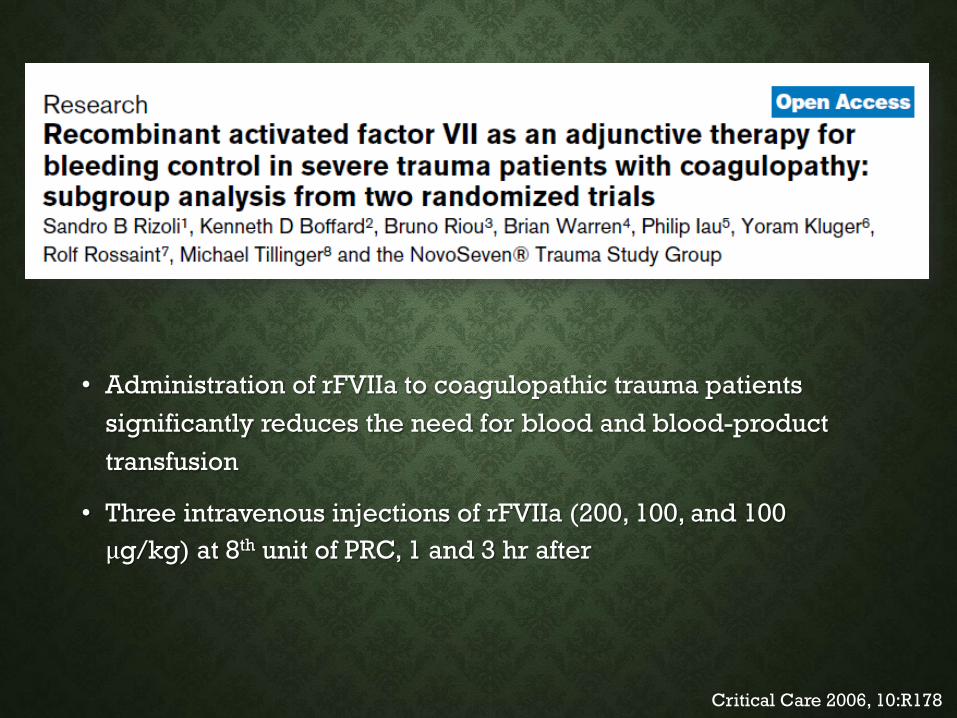
• Administration of rFVIIa to coagulopathic trauma patients
significantly reduces the need for blood and blood-product
transfusion
• Three intravenous injections of rFVIIa (200, 100, and 100
μg/kg) at 8th unit of PRC, 1 and 3 hr after
Critical Care 2006, 10:R178

Critical Care 2006, 10:R178
ENDPOINT OF RESUSCITATION
• Permissive Hypotensive Resuscitation
• The optimal MAP is one which would provide a sufficient flow of
blood to delicately balance hemostasis
• The minimal MAP for the functioning of the vital organs is about
50 - 70 mmHg
• The goal blood pressure for these patients is a MAP of 40-50
mmHg or a SBP ≤ 80 mmHg

ENDPOINT OF RESUSCITATION
• Contraindication of Permissive hypotension
• Preexisting hypertension
• Preexisting cardiovascular disease
• Traumatic brain injury
• Pregnancy
• Underlying disease of cerebrovascular disease, carotid artery
stenosis, and compromised renal function

• Controlled resuscitation can effectively
• ↓ Additional blood loss
• avoid excessive hemodilution and coagulopathy
• Improve the early survival rate, and
• ↓ Apoptosis of visceral organs
J Trauma 2007; 63(4): 798-804

• In uncontrolled hemorrhage shock (UCHS) fluid treatment is
aimed at
• Restoration of radial pulse
• Obtaining a SBP of 80 mmHg By titration of 250 ml of isotonic
solution (Control resuscitation)
• High blood pressure (SBP>100 mmHg, MAP>70 mmHg) in
head-injured and in pregnant patients
World J Emerg Surg 2006; 31(4): 339-44

ENDPOINT OF RESUSCITATION
• Simple restoration of normal vital signs is not adequate as a
patient may simply be in “compensated” shock while
continuing to have occult hypoperfusion and ongoing tissue
damage
• Endpoint of resuscitation can be divided to :
• Global endpoint
• Regional endpoint

• Cardiac output, Cardiac index
• Oxygen delivery
• Mixed venous oxygenation
• Right ventricular end-diastolic volume
• Left-ventricular stroke work index
• Left-ventricular power output
• Base excess
• Lactate level
Global Endpoint
• Gastric tonometry
• Intramucosal pH (pHi)
• The gap between intramucosaland arterial pCO2
• Esophageal CO2, pH
• Sublingual CO2, pH
• Intramuscular pH
• Intramuscular pCO2
• Tissue O2 and CO2
Regional Endpoint
2003 Eastern Association for the surgery of Trauma
REOPERATION
• Completion of definitive repairs
• Search for missed injuries
• Formal closure of the incision
Mattox. Trauma 6th Edition

Mattox. Trauma 6th Edition

THANK YOU FOR YOUR ATTENTION