
Damage Control Resuscitation: Beyond the MTPmsic.org.my/filedownloader.asp?filename=asmic2015... ·...
82
Damage Control Resuscitation: Beyond the MTP Dr Jonathan Tan Senior Consultant, Anaesthesiology, Intensive Care, Tan Tock Seng Hospital, Singapore
Transcript of Damage Control Resuscitation: Beyond the MTPmsic.org.my/filedownloader.asp?filename=asmic2015... ·...
Damage Control
Resuscitation: Beyond
the MTP Dr Jonathan Tan
Senior Consultant,
Anaesthesiology, Intensive Care,
Tan Tock Seng Hospital, Singapore
Trauma shock and
Coagulopathy
Acute Coagulopathy of Trauma
Shock
Multifactorial aetiological Combination
Shock
Tissue injury related thrombin generation
Anticoagulant and Fibrinolysis activation
Hypothermia, Acidosis, Hemodilution, Factor
consumption.
Inflammation, SIRS, Coagulation. Crosstalk
Hess JR et al. J Trauma 2008,65:748-754 Nascimento et al. Critical Care 2010,14:202
Brohi K et al. J Trauma 2003;54:1127-1130
Brohi K et al. J Trauma 2008,64:1211-1217



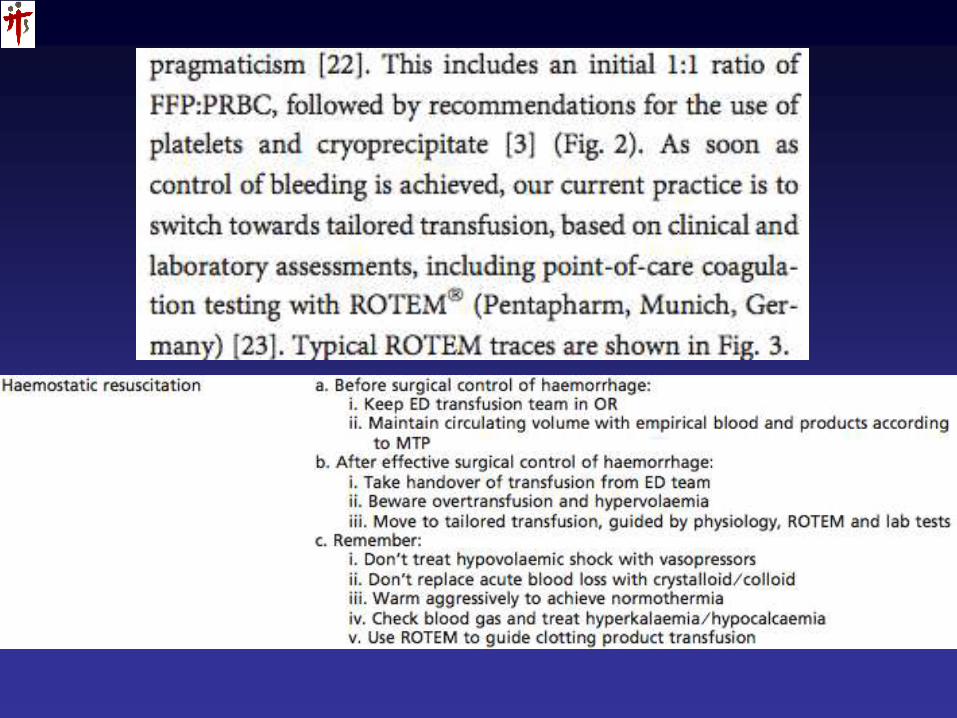
Damage Control Resuscitation
Haemostatic Resuscitation;
Damage Control Resuscitation
Goal:
Minimize iatrogenic resuscitation injury
Prevent worsening shock & coagulopathy
Rapid correction of hypothermia, acidosis & direct correction of coagulopathy.
Obtain definitive haemostasis
Restore Physiology • HessJR, Holcomb JB et al.Transfusion 2006; 46:685-686
• Holcomb et al. J Trauma;2007;62:307-310
• Beekley AC et al. Crit Care Med 2008;36:S267-274
DCR Principles
Rapid recognition of at risk patient:- For MT, early coagulopathy of trauma.
“Permissive hypotention” before surgical hemostasis
Rapid definitive control of bleeding!
Treat Hypothermia, Acidosis, Hypocalcaemia. Resus!
Avoid excessive crystalloids and haemodilution
DCR Principles
Early transfusion of
PRBC:Plasma:Platelets in ? ratio!
Use of fresh whole blood? Fresh RBCs?
Adjuncts where appropriate: rFVIIa, anti-fibrinolytics, cryoprecipitate…
Frequent laboratory monitoring of coagulation status; use of point of care tests (Thromboelsatography).
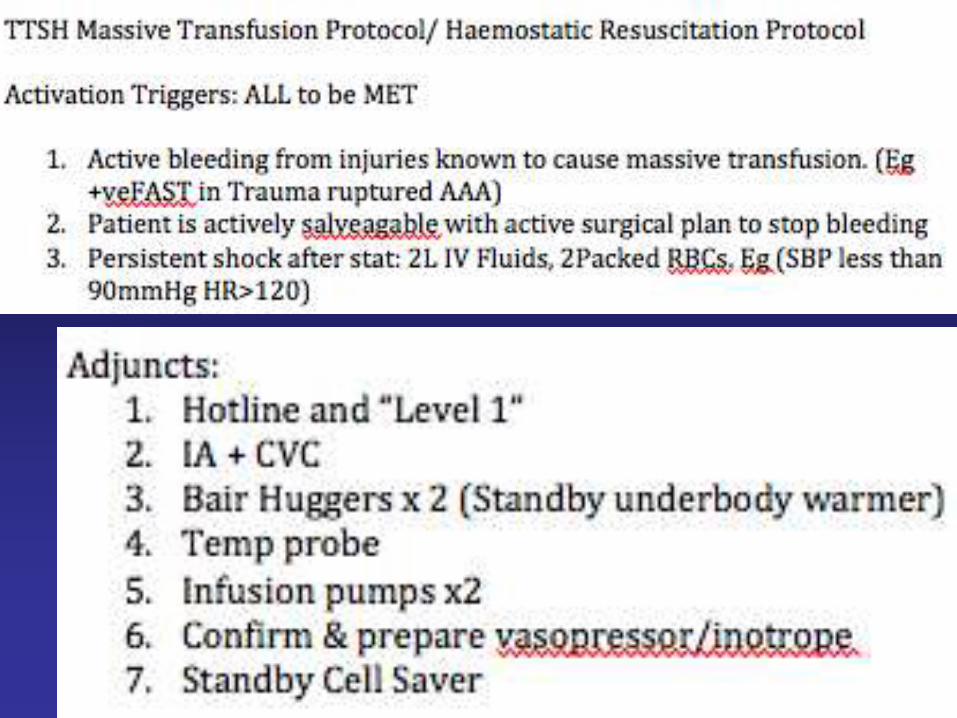
MTP / Haemostatic
Resuscitation Protocol
Beyond just MORE blood…
MTP Key Components
Trigger: wastage vs too late!
Blood Packs: What? Ratio?
Adjuncts: +/- Pharmacologic
Monitoring: Targets?
Physiological Goals?
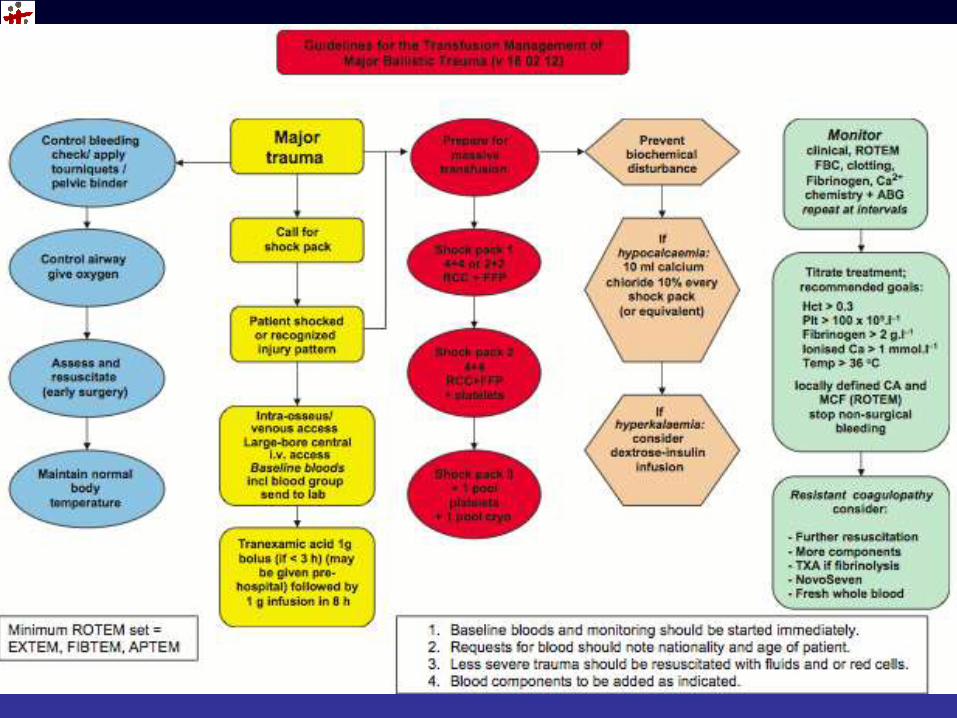
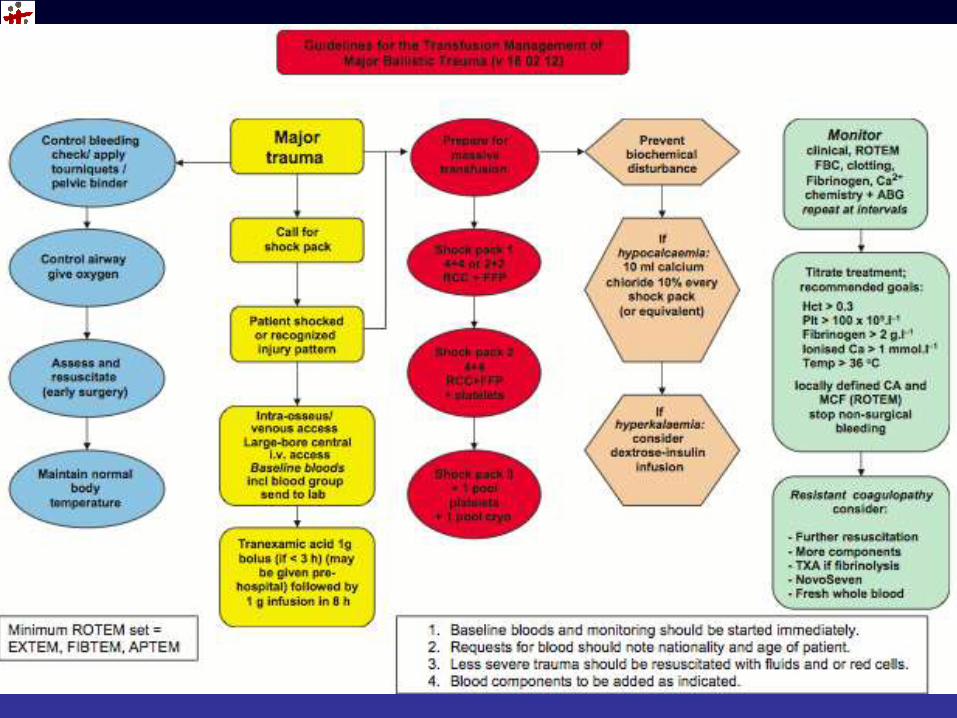
Treatment algorithm
Standardised
UK-DMS Protocol
Summary of UK-DMS experience in last 12 years: Afghanistan; Iraq

PROMMT: Findings
Pts did NOT receive constant ratio components during active resus
81% Hemorrhagic deaths within 1st 6hours.
Higher Plasma/Platelet:RBC ratios independently assosc with decreased 6hr mortality.
<1:2, 3-4Times more likely to die vs 1:1 or higher grp.
Only 72% rec Platelets by hour 3!
PROMMT: Findings
Survivors hour 6- 24: risk of death higher for low plasma ratios
>24hrs to 30days: Risk of death not assoc with component ratios
Survival bias still an issue
Supports 1:1:1 in MTP during resuscitation, DCS phase?
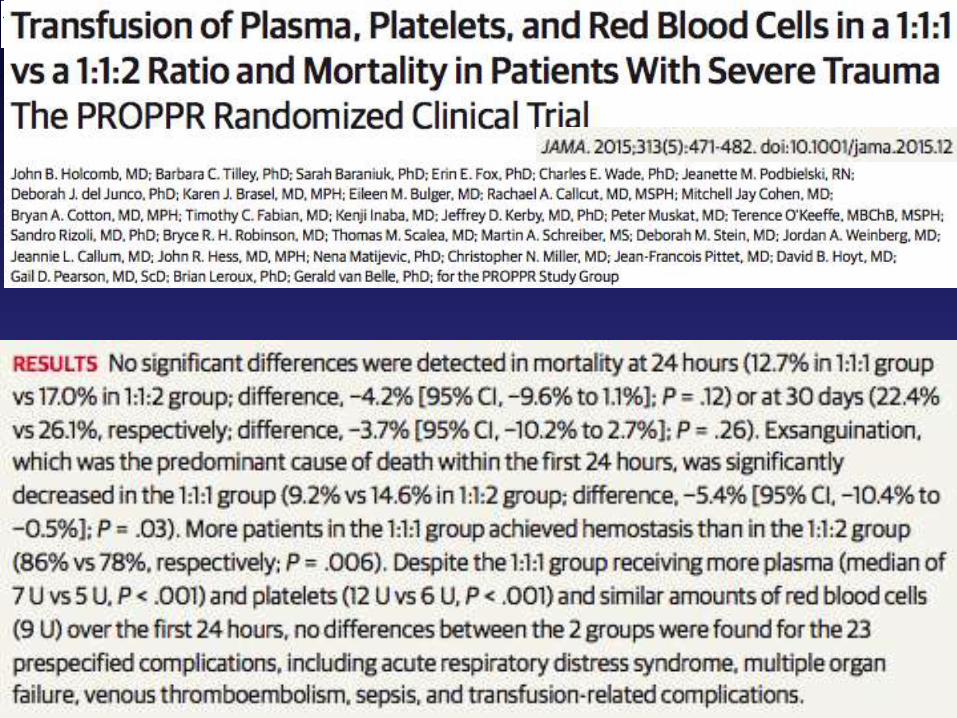

PROPPR: Findings
Less Exsanguination deaths
More Haemostasis achieved
More FFP but no increased Safety differences
Lower than predicted mortality in 1:1:2 group
1:1:1 ASAP on arrival then switch to guided therapy when haemorrhage control achieved
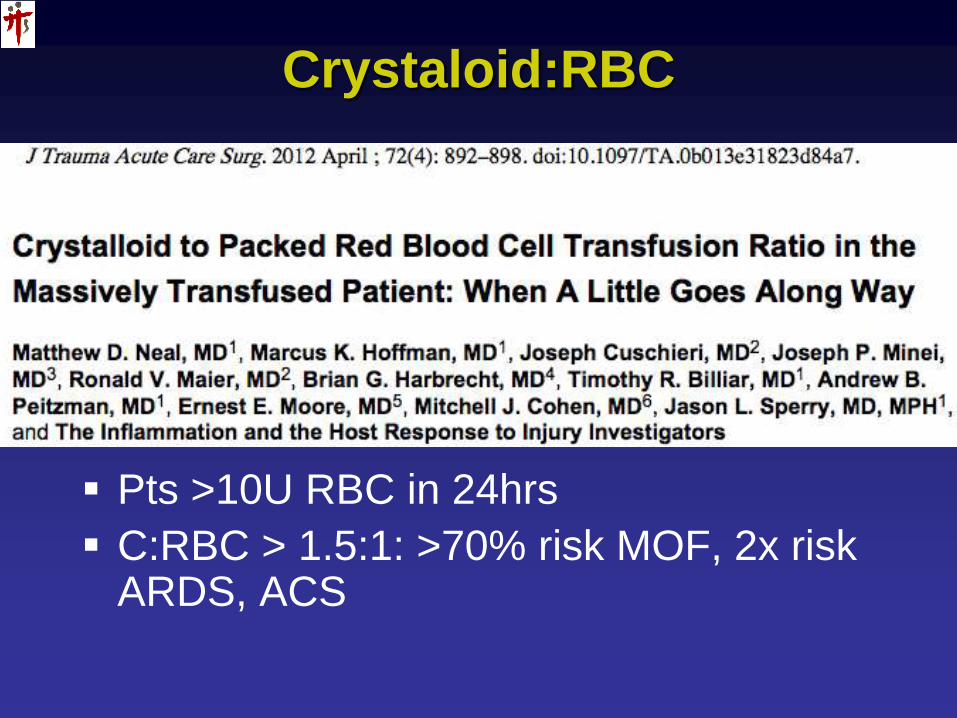
Crystaloid:RBC
Pts >10U RBC in 24hrs
C:RBC > 1.5:1: >70% risk MOF, 2x risk ARDS, ACS
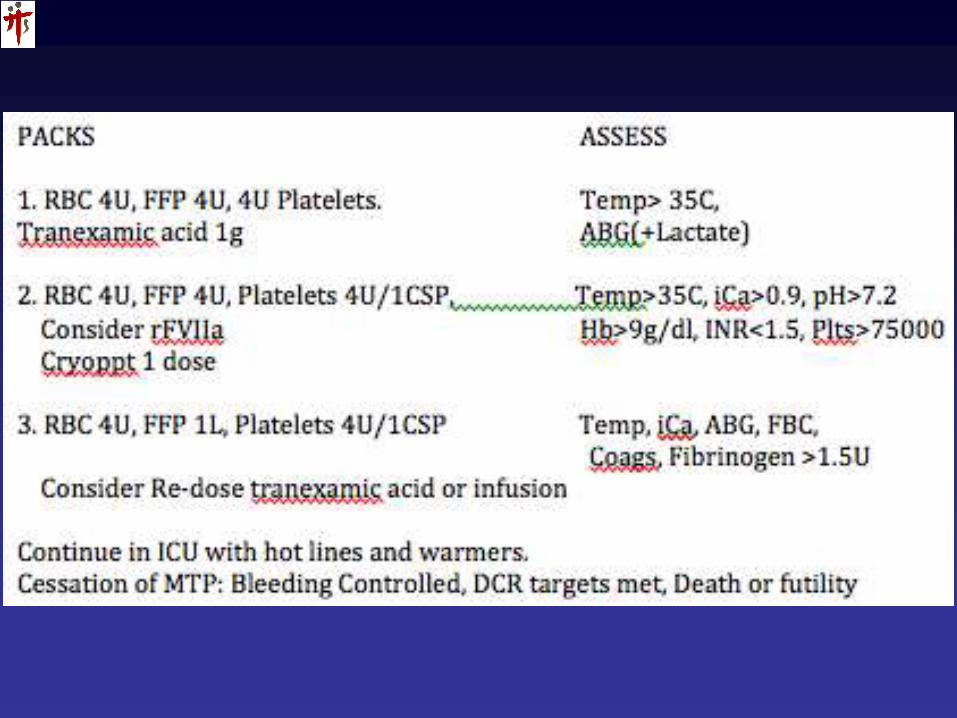
So Far…
1:1:1 restore circulating vol and blood components
Limit Crystalloids
Warm!
Correct electrolytes: Ca, K
Adjuncts: Pharmacological
Haemorrhage control: stop 1:1:1; directed transfusions
Coagulation Monitoring
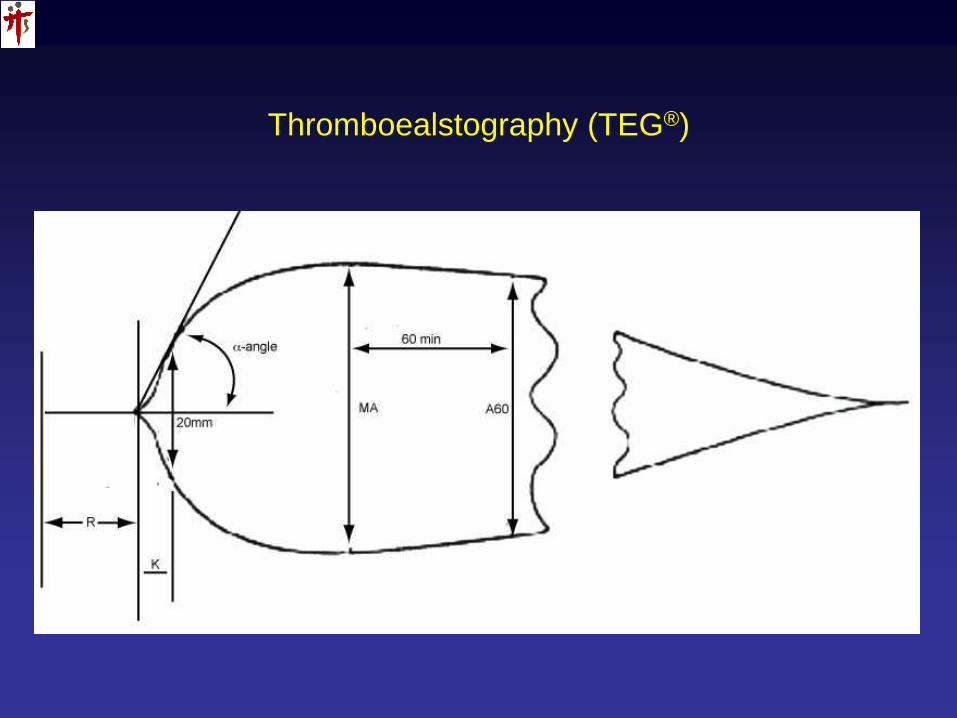
Thromboealstography (TEG®)

Rotational Thromboelastometry (ROTEM®)
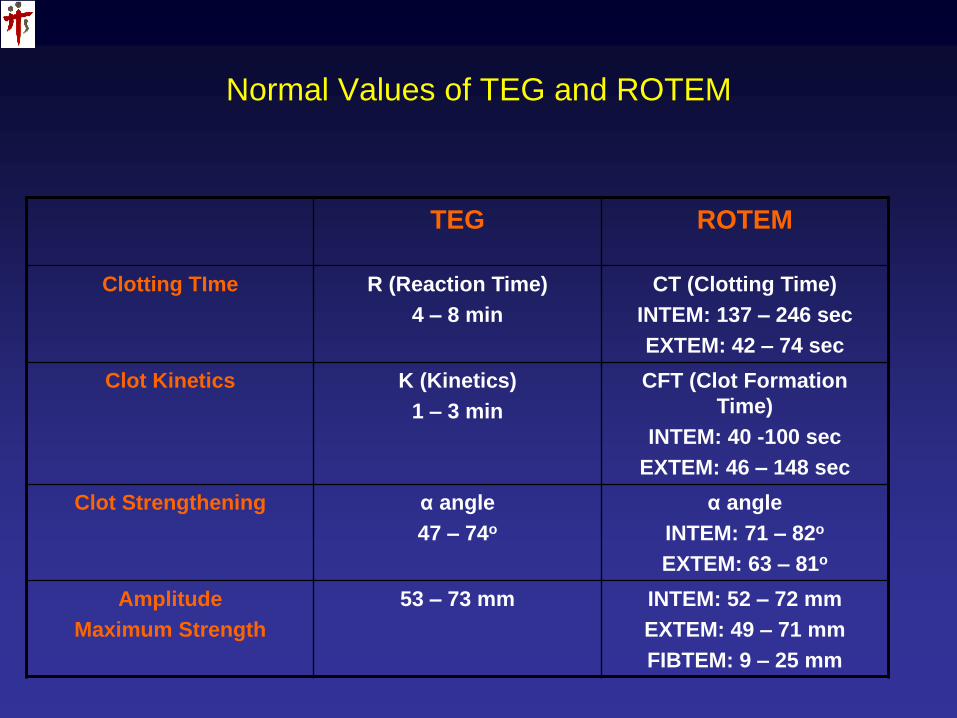
Normal Values of TEG and ROTEM
TEG ROTEM
Clotting TIme R (Reaction Time)
4 – 8 min
CT (Clotting Time)
INTEM: 137 – 246 sec
EXTEM: 42 – 74 sec
Clot Kinetics K (Kinetics)
1 – 3 min
CFT (Clot Formation
Time)
INTEM: 40 -100 sec
EXTEM: 46 – 148 sec
Clot Strengthening α angle
47 – 74o
α angle
INTEM: 71 – 82o
EXTEM: 63 – 81o
Amplitude
Maximum Strength
53 – 73 mm INTEM: 52 – 72 mm
EXTEM: 49 – 71 mm
FIBTEM: 9 – 25 mm
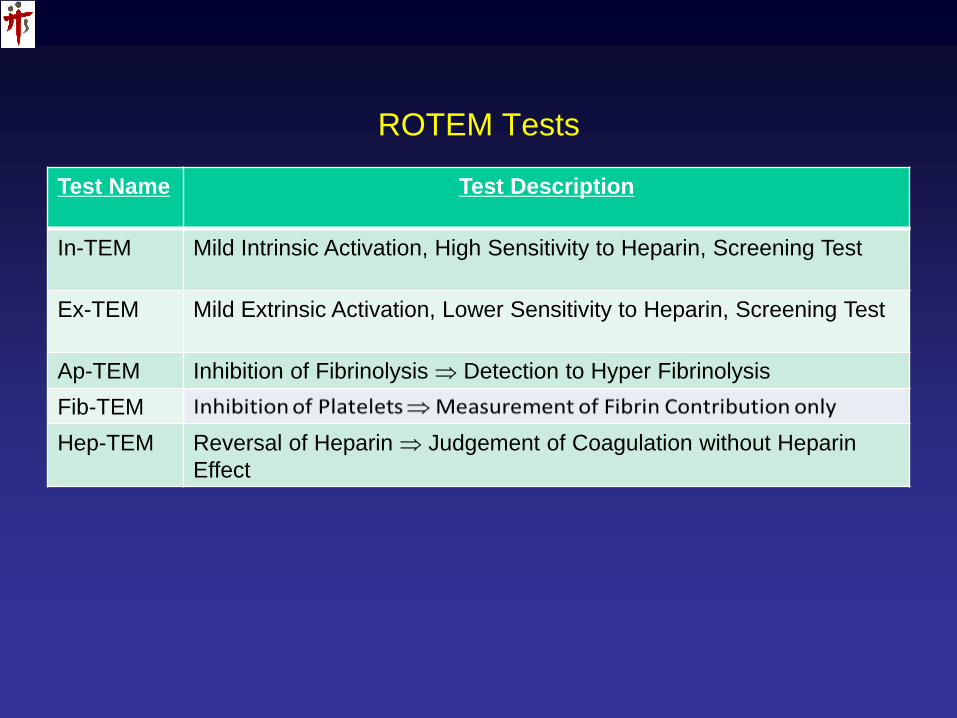
ROTEM Tests
Test Name Test Description
In-TEM Mild Intrinsic Activation, High Sensitivity to Heparin, Screening Test
Ex-TEM Mild Extrinsic Activation, Lower Sensitivity to Heparin, Screening Test
Ap-TEM Inhibition of Fibrinolysis Detection to Hyper Fibrinolysis
Fib-TEM
Hep-TEM Reversal of Heparin Judgement of Coagulation without Heparin
Effect
A need for Point-of-Care evaluation of
Coagulation
• Where does the ROTEM/TEG fit into our MTP?
• How do we use the results?
• What are the limitations?
• How do we get the whole picture?
• Stat!
Algorithm?

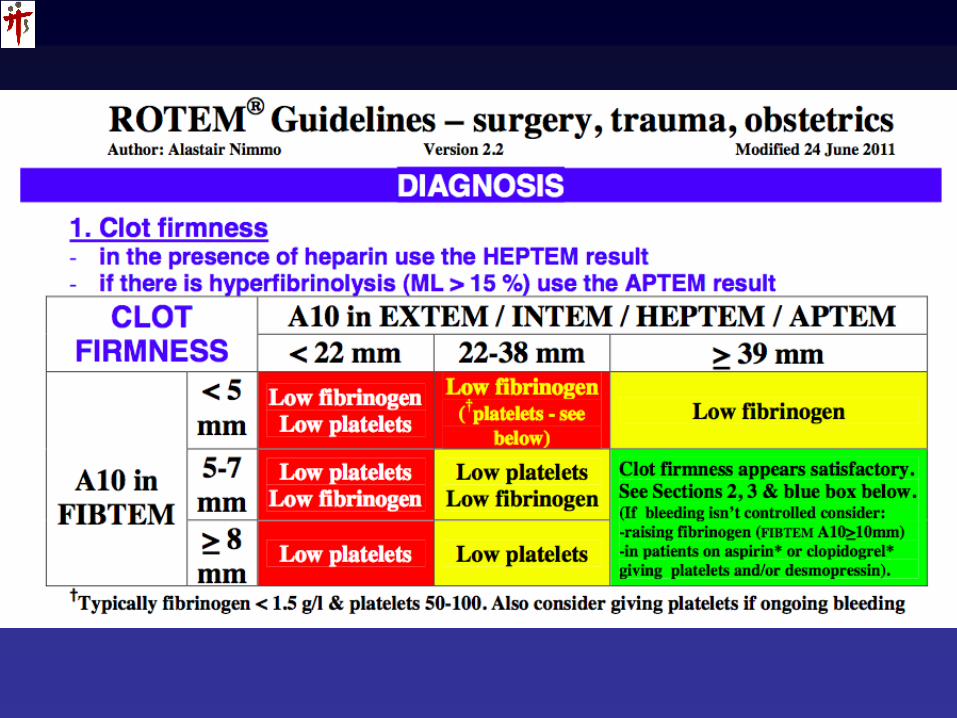
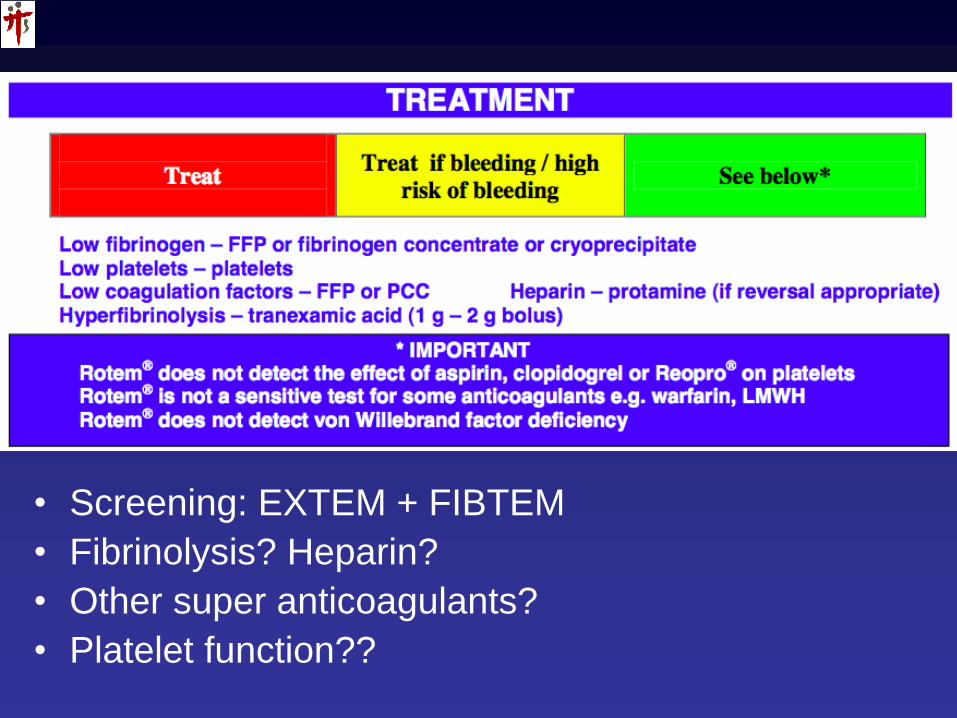
• Screening: EXTEM + FIBTEM
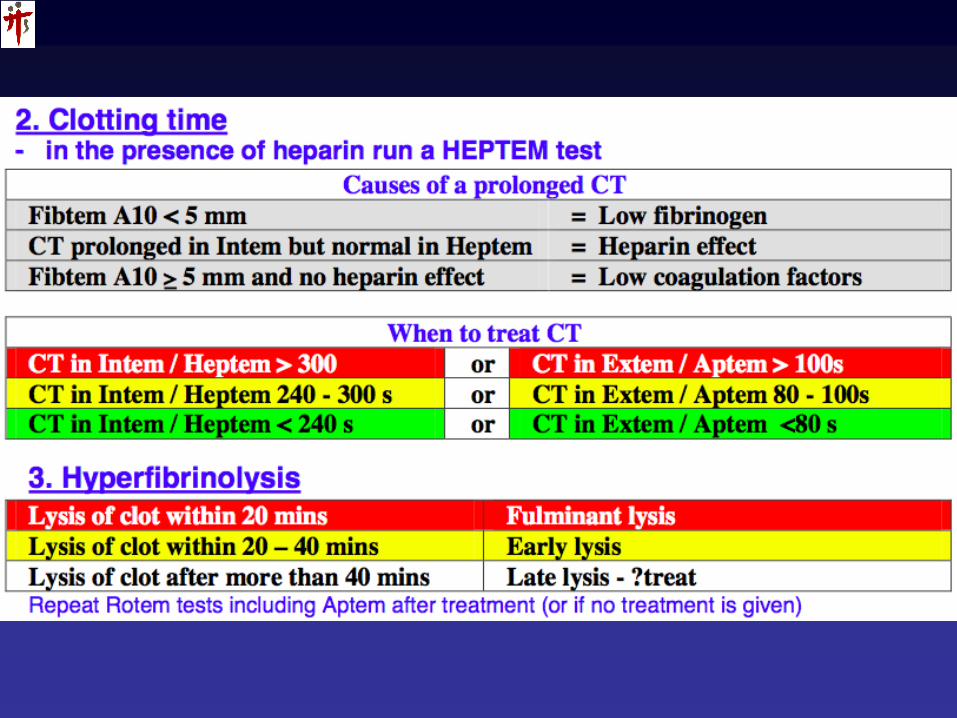
• Fibrinolysis? Heparin?
• Other super anticoagulants?
• Platelet function??
Platelet Function!!??



Platelet Function Assessment
Bleeding Time
TEG + Platelet Mapping
Roche Multiplate
ROTEM….
Reagents detecting defect in platelet function wrt AA, ADP, Collagen, 2b-3a interactions…
Paucity of data and evidence
Big Blind spot that will kill our patients!

Platelet Function Assessment
For which patient?
Trauma
TBI
Antiplatelet drugs
Renal Failure
Coronary Artery disease; stenting
Ischaemic strokes
My ICU patient…
Everyone??!!??

DDAVP
1-deamino-8-D-arginine vasopressin
Enhances platelet adherence and platelet aggregate growth on endothelial surface
0.3ug/kg or 20U
Von Willebrand factor disease
Head Bleeds with antiplatelet effects
Prevents the development of hypothermia-induced impairment of primary haemostasis and significantly increases platelet aggregation during hypothermia and acidosis.
Ng KF et al: Low-dose desmopressin improves hypothermia-induced impairment of primary haemostasis in healthy volunteers. Anaesthesia 2011, 66:999-1005.468. Hanke AA, Dellweg C et al:Effects of desmopressin on platelet function under conditions of hypothermia and acidosis: an in vitro study using multiple electrode aggregometry*. Anaesthesia 2010, 65:688-691.

TEG/ROTEM/VHAs
Shown to save money and reduce unneccessary transfusions
May save lives
Use of VHAs endorsed by European and British Transfusion guidelines
Differentiate medical vs surgical bleeding. (Cardiac literature)
Used with Platelet Function Assay

TEG/ROTEM/VHAs
Will not identify “super” anticoagulants
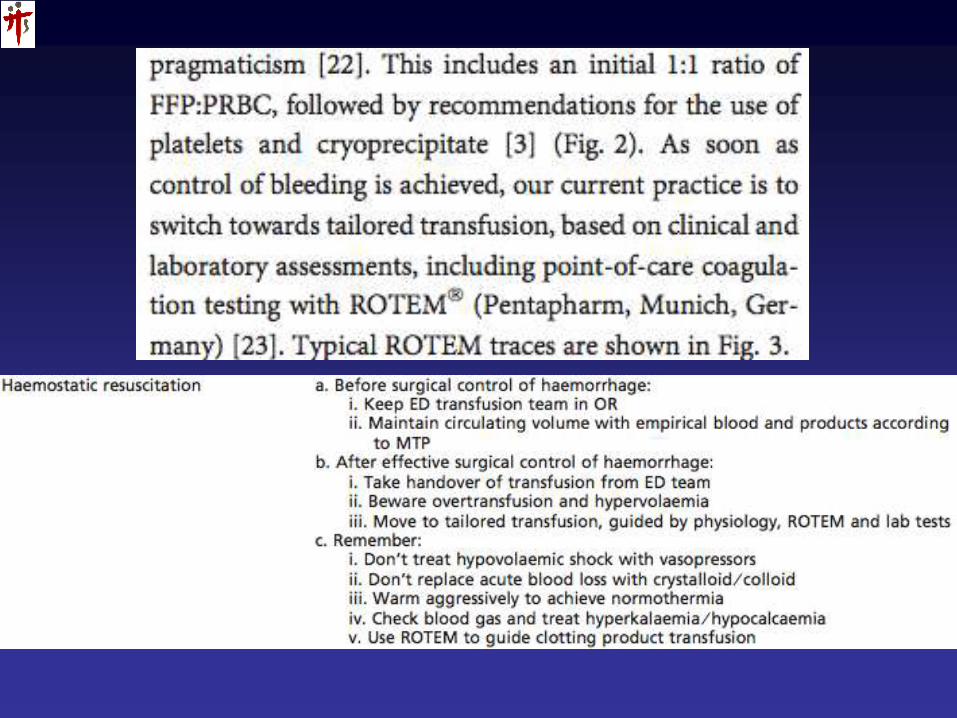
As part of Haemostatic Resuscitation Protocol
After exsanguinating bleeding plugged
Localised, Specific, to the instituition and patient
It will NOT stop the bleeding!

Beyond Blood
Restore circulating vol 1:1:1, limit crystaloid
Warm
Check: Rotem, ABG, Temp
Correct… Ca, K, Lactate…
Directed coagulopathy and Hb correction
Quick reminder: tranexamic acid; rFVIIa

rFVIIa
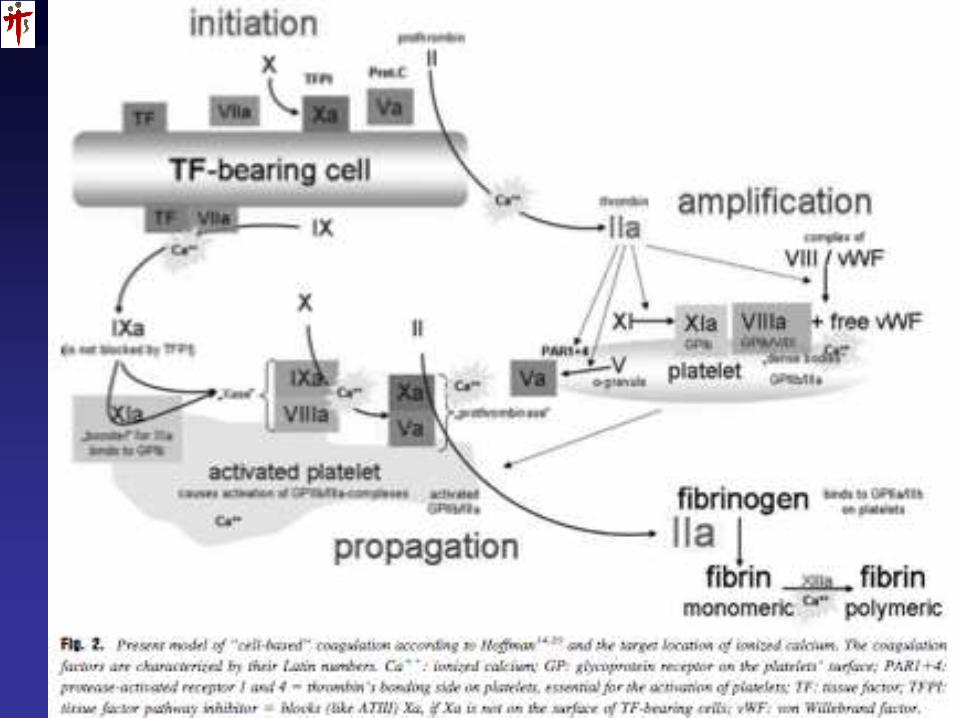
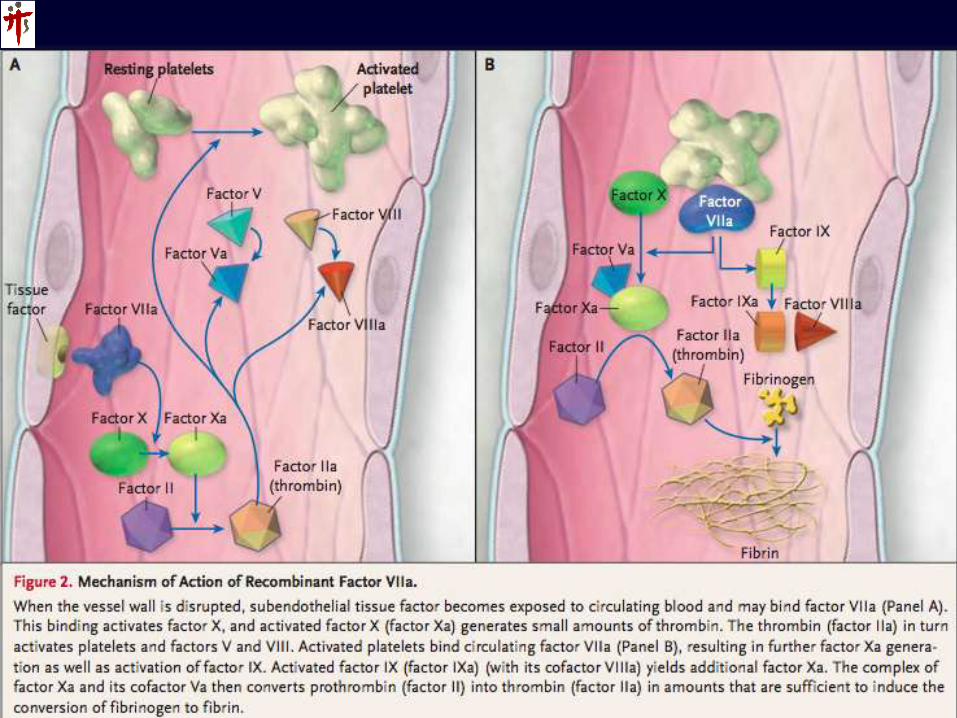
Mode of Action
• Tissue Factor dependent pathway
• Tissue factor independent pathway:
Binds directly to activated platelets &
activates Xa on platelet surface. Initiates
thrombin burst.
• Rate and amount of thrombin generation
is paramount in clot stability and
resistance.
• ?Localized to site of injury without
systemic activation??

rFVIIa… Does it work?
Yes!
Haemophilia
Platelet Defects
Qn is…..
Does it work in Trauma??

rFVIIa… Evidence?
Kenet et al 1999, Lancet 354:1879
Numerous Case series; Registries; guidelines; own anecdotal success?
RCTs: Trauma, ICH
Boffard et al, J Trauma 2005: Reduction in RBCs transfused, ARDS, MODS in blunt trauma. Safety.
Phase 2. Safety. Efficacy.
Explosion of off label use in trauma.
rFVIIa in Trauma: Issues
Efficacy; Conditions for optimum effect
Timing
Safety
Dosing
Off label use implications
Cost
“Last-ditch” to Salvage to Optimum outcome improving??
Definitive RCT?.....
Was meant to be the ONE!!
J Trauma Sept 2010,Vol69,(3);489-500
150 Hospitals, 26 Countries
Aug 2005 – Sept 2008
Clinical management guidelines
Inclusion
18-70yr
< 4Hrs Injury to admission
Active Haemorrhage: Acidosis &/or
Hypotension; Ongoing volume loading
1st dose trial drug between 4U & 8U
RBC
Injury to 1st dose completed max
12hrs
Exclusion: futile, Time exclusions.

Intervention
3 doses of rFVIIa: 200ug/kg T0,
100ug/kg T1hr and T3hr.
Placebo
Randomized 1:1
Randomization: Random permuted
blocks

Results
Interim analysis: Blunt trauma mortality far lower. Power too low.
Trial stopped early due to high likelihood of futility.
Total 573 enrolled
481 blunt, 92 penetrating
Baseline demographics statistically same. (ISS, pH, Hb, Vitals, lactate, GCS)

Blunt Trauma Gp
30 day mortality 11.0% Rx v 10.7%
Durable morbidity rates no diff.
Trend towards decreased MOF in rFVIIa gp 45% v 53% p=0.06
Significant reduction in blood pdts used.
RBC 6.9 vs 8.1, FFP 4.7 vs 6.9 at 24hrs
48hrs total allogenic blood transfused 19 vs 23.5
No diff: Platelet, Cryo use.
Blunt Trauma Gp: Safety
Total number of Significant Adverse
Events same
Thrombotic events: 16.1% (rFVIIa) vs
13.2% placebo. p=0.38
SAFE…. ?

Penetrating gp
Mortality rFVIIa grp 18.2% vs 13.2%
p=0.4.
No diff in secondary endpoints
FFP use reduced in rFVIIa gp. 3.8U v
5.7U p=0.04
No diff in SAE, with venous thrombosis
higher in placebo grp. p=0.04
Post hoc analysis combining both grps
less ARDS in rFVIIa grp (8 vs 22
events) p=0.022
CONTROL Trial: Discussion
rFVIIa: Proven haemostatic agent
Modest reduction in RBC use. Is reduction of 1-1.5U of blood transfused clinically significant??
Safety: Combination of 2 RCTs in trauma, total of 837pts: No increased thrombotic risk. ?Young pt population?
Benefits: Reduction in ARDS? Both trials show benefit??
Discussion
Compliant Use of patient management protocols: improved “standard care”?
See appendix of study for details: DCS, Resus targets,colloid use guidelines, Ventilation strategy…
Safety of rFVIIa in RCTs
NEJM Nov 4, 2010. 363;(19). 1791-1800
35 RCTs (9 in healthy volunteers) spanning 12 years, heterogenous disease states. CONTROL trial NOT included.
4119 patients, 349 healthy volunteers
Arterial Thromembolic events 5.5% rFVIIa, 3.2% placebo. P=0.003
Venous events no diff.
Factors for increased risk: Neuro-events, Age (esp >65), higher rFVIIa doses, concomitant haemostatic agent used
• ANZHR 386 trauma pts, 45 with triad
• Triad: INR>1.5, pH<7.2,Core temp<35
• Use of rFVIIa assoc with survival in 31%
of patients
• Use in pH<6.91 appears futile
Cannot recommend as 1st line agent
Use as part of a haemostatic protocol; bundle of measures
TTSH rFVIIa guidelines
Used as part of MTP
pH>7.2; Temp>34; iCa >0.9
90-100ug/kg; 2nd dose at hour 2
Off label use implications & Cost: inform family; fill forms
“Last-ditch” to Salvage to Optimum outcome improving??
THINK of it!
Tranexamic Acid
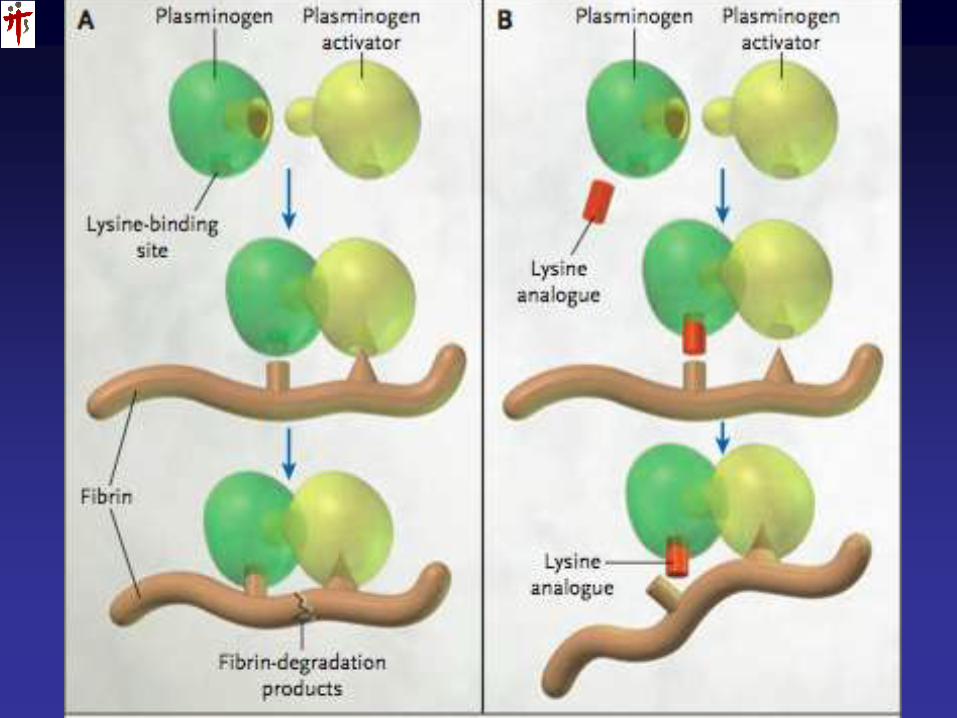
Tranexamic Acid
Antifibrinolytic agent
Lysine analogue; Competitive inhibition
Plasma T1/2 120min
Prevents Plasmin activation
Dose? Cardiac surgery? Trauma?: Large
variation.
Cave! Dose accumulation with Renal failure.
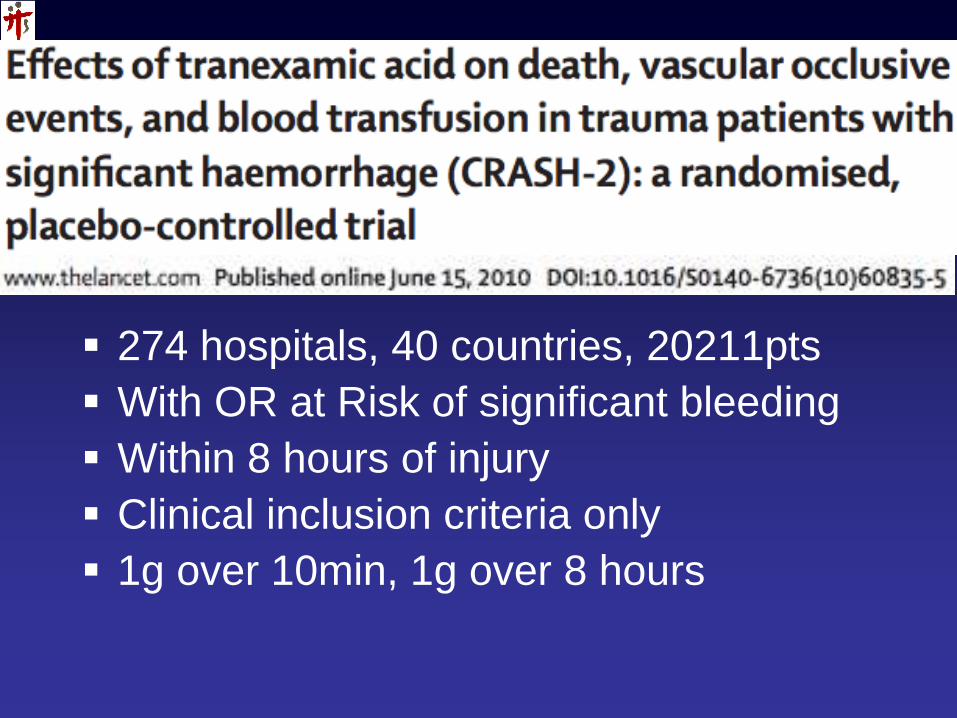
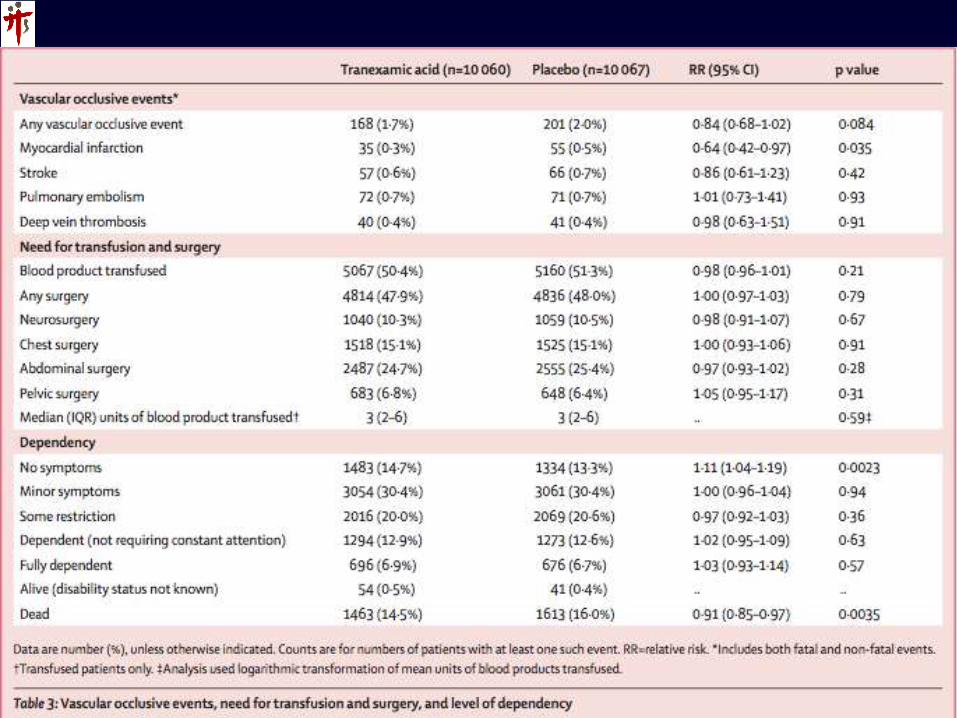
274 hospitals, 40 countries, 20211pts
With OR at Risk of significant bleeding
Within 8 hours of injury
Clinical inclusion criteria only
1g over 10min, 1g over 8 hours
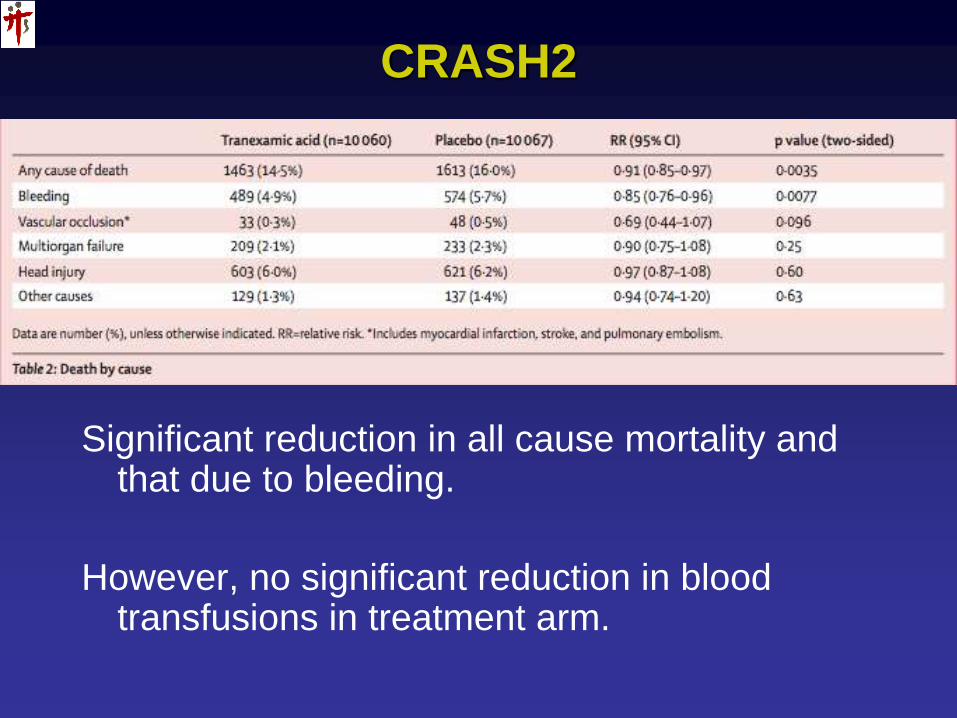
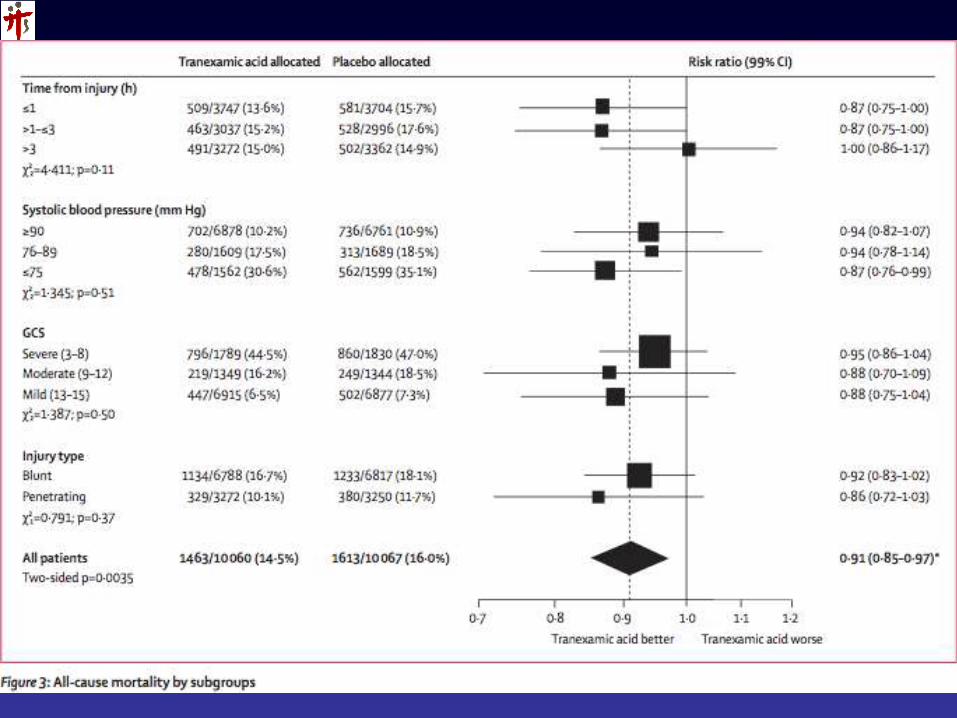
CRASH2
Significant reduction in all cause mortality and that due to bleeding.
However, no significant reduction in blood transfusions in treatment arm.
Tranexamic Acid
Issues…
8 Hours from injury: Prehospital influences?
Lack of precision of inclusion criteria?
Fibrinolytic assays?
Safety: Vascular occlusions? Seizures?
Dosing
ISS not presented for groups
Blood component ratios in both groups?
Issues…
No difference in transfusion: was benefit due to other properties of Tranexamic acid or reduced Plasmin proinflammatory effects?
How??
Wait for it………
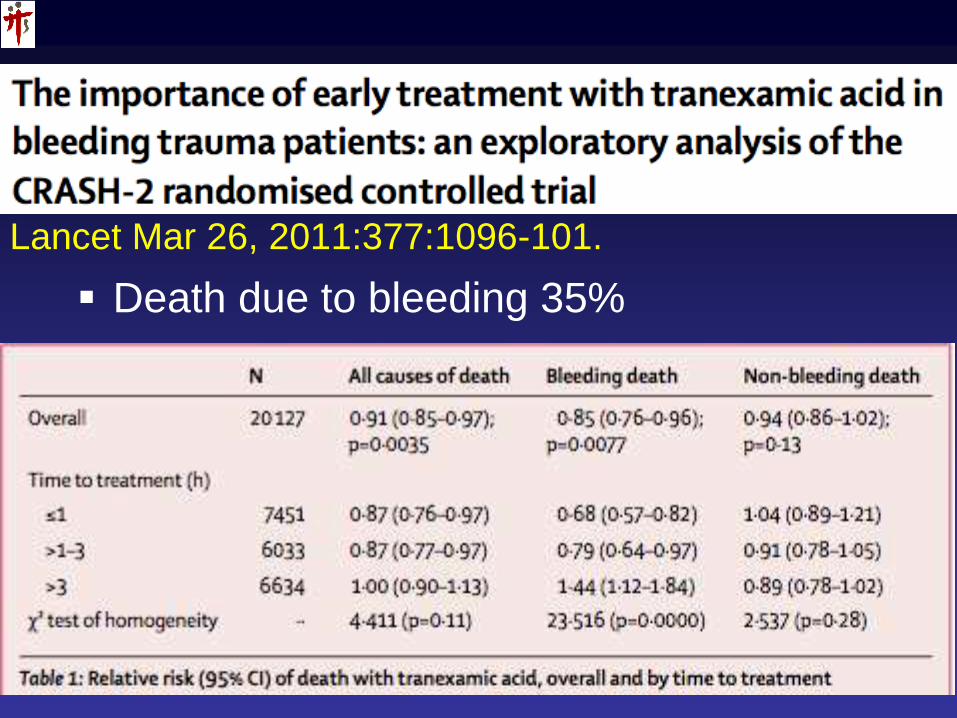
Lancet Mar 26, 2011:377:1096-101.
Death due to bleeding 35%
Discussion
Used in dose and manner prescribed:
Reduced all cause mortality, esp death due to bleeding.
Give it early! < 3 hours post injury
?? Given > 3 hours, increased risk of death.
Editorial comment re availability of coagulant blood pdts and benefit of tranexamic acid, esp in pre hospital care.
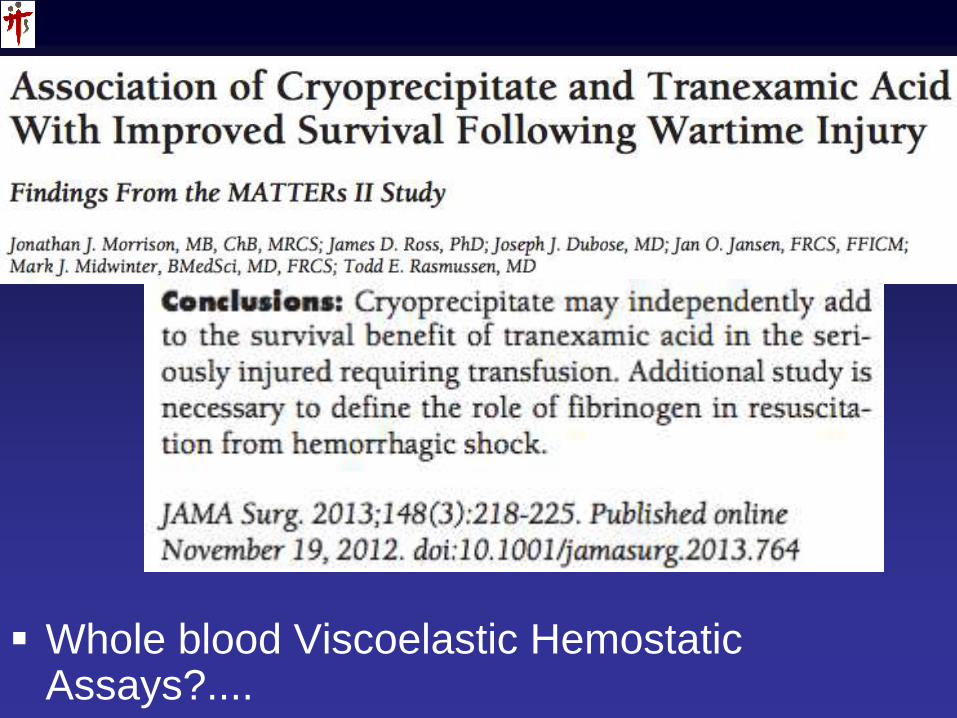
Whole blood Viscoelastic Hemostatic Assays?....

Conclusion
Stopping the Bleeding: Interventionalist’s job
Making the blood clot: YOUR job.


















