
dacremont2_oct202011
25
Management of malaria and non-malaria febrile illnesses Valérie D'Acremont Swiss Tropical & Public Health Institute Global Malaria Programme, WHO Seattle, 20 Oct 2011
-
Upload
center-for-disease-dynamics-economics-policy -
Category
Documents
-
view
213 -
download
0
description
http://cddep.org/sites/cddep.org/files/dacremont2_oct202011.pdf
Transcript of dacremont2_oct202011

Management of malaria
and non-malaria febrile illnesses
Valérie D'Acremont
Swiss Tropical & Public Health Institute
Global Malaria Programme, WHO
Seattle, 20 Oct 2011

2
Background
Prescription of antimicrobials for children underfive
in Dar es Salaam, Tanzania
Antimalarials AntibioticsAND
Routine microscopy
(or no malaria tests)
Rapid Diagnostic Tests
75%
15%
57%79%

3
Dar Es Salam
3 mio d’habitants
Ifakara, 50.000 hab.
To determine the etiology of fever episodes
in children living in urban and rural Tanzania
Objective

4
Methodology
• Prospective study including children
attending two outpatient clinics
(one urban and one rural) in Tanzania
• Inclusion criteria:
- aged 2 months - 10 yrs
- temperature > 38°C
- no antimicrobials for > 1week
• Full clinical assessment
• Investigations based on pre-defined algorithms:
FBC; ALT; creat.; RDT for malaria, typhoid, strepto A,
adeno/rotavirus; BS malaria and borrelia; urine dipstick;
amoeba in stool; blood/urine/stool cultures; chest X-ray

5
Diarrhea (>3 stools/day):
POS
NEGRapid test
Rota/adeno
Amoebic
GASTRO-ENTERITIS
Viral
GASTRO-ENTERITIS
Possible bacterial
GASTRO-ENTERITIS
Metronidazole
POS
NEGCiprofloxacine
Follow-up
Day 7
Blood
culture
Investigation
for diarrhea
Stool
examination
for amoeba
TYPHOIDPOS
NEGFollow-up
Day 7
Ciprofloxacine
Rapid Test
for Typhoid
2)
1)
3)
No antibiotic
STOP
STOP
STOP
Methodology
Example of a pre-defined algorithm:

6
Methodology
• Real-time (RT-)PCR of naso-pharyngeal swabs for 15 virus:
FLUAV, FLUBV, RSV, HMPV, HPIV 1/3,
PIC (rhino, entero, coxsackie), HBoV,
HCoV OC43 229E NL63 HKU1, HAdV
• Real-time PCR on blood:
Dengue, Chikungunya, West Nile, Rift Valley
HHV6, parvovirus B19
• Serologies on blood :
EBV, CMV, Toxoplasma, Rickettsia, Coxiella, Leptospira
Computer-based diagnosis with levels of probability

7
Baseline characteristics
From April to December 2008:
• 1005 children were included (informed consent, 2 refusals)
507 in Dar es Salaam and 498 in Ifakara
• median age was 18 months
• 49% were females
• 78 (8%) children were admitted in the ward
• 133 (13%) had WHO criteria for severe disease (4 deaths)

8
Skin infection
TyphoidMalaria
Fever?
Systemic infections
Gastroenteritis
Acute
respiratory
infectionUrinary tract infection
50%
13%
8%
5%
1%
11%
0.2%3%
9%Meningitis
Etiologies of fever in 1005 Tanzanian children
1212 diagnoses

9
Overlap of diseases
ARI52.8%
Clinical pneumonia*
14.6%
0.2%
4%
3.6
%
Gastro-
enteritis5.9%
Malaria6.7%
19.6% had 2 or more diagnoses of high probability
*Pneumonia as defined by WHO
(documented or not by chest X-ray)

10
Skin infection
TyphoidMalaria
Fever?
Systemic infections
Gastroenteritis
ARI
Urinary tract infection
50%
13%
8%
5%
1%
11%
0.2%3%
9%Meningitis
Etiologies of Acute Respiratory Infections (ARI)

11
ARI
50%
URTI
Clinical
pneumonia
Bronchiolitis
Radiological pneumonia
Viruses
5%
22%
7% 65%
Etiologies of Acute Respiratory Infections (ARI)
81%

12
ARI
50%
URTI
Clinical
pneumonia
Bronchiolitis
Radiological pneumonia
5%
22%
7% 65%
Influenza
RSV
Metapneumovirus
Parainfluenza 1/3
RhinovirusEnterovirus
Coronavirus
Bocavirus
Adenovirus
Etiologies of Acute Respiratory Infections (ARI)
81%

13
Seasonality of influenza
0%
10%
20%
30%
40%
50%
Apr May Jun Jul Aug
Influenza A
Influenza B
0%
10%
20%
30%
40%
50%
Jul Aug Sep Oct Nov
Dar es Salaam
Ifakara

14
Skin infection
TyphoidMalaria
Fever?
Systemic infections
ARI
Urinary tract infection
50%
13%
5%
1%
11%
0.2%3%
9%Meningitis
Etiologies of gastroenteritis
Gastroenteritis
8%

15
Amoeba
Rotavirus
Adenovirus
Salmonella
Shigella
Unknown
pathogen
8%
Gastroenteritis
51%
4%
28%
18%
Etiologies of gastroenteritis

16
Skin infection
TyphoidMalaria
Fever?
Gastroenteritis
ARI
Urinary tract infection
50%
13%
8%
5%
0.2%3%
9%Meningitis
Etiologies of systemic infections
Systemic infections
11%

17
8%
11%
Systemic infections
Viruses
75%
Etiologies of systemic infections
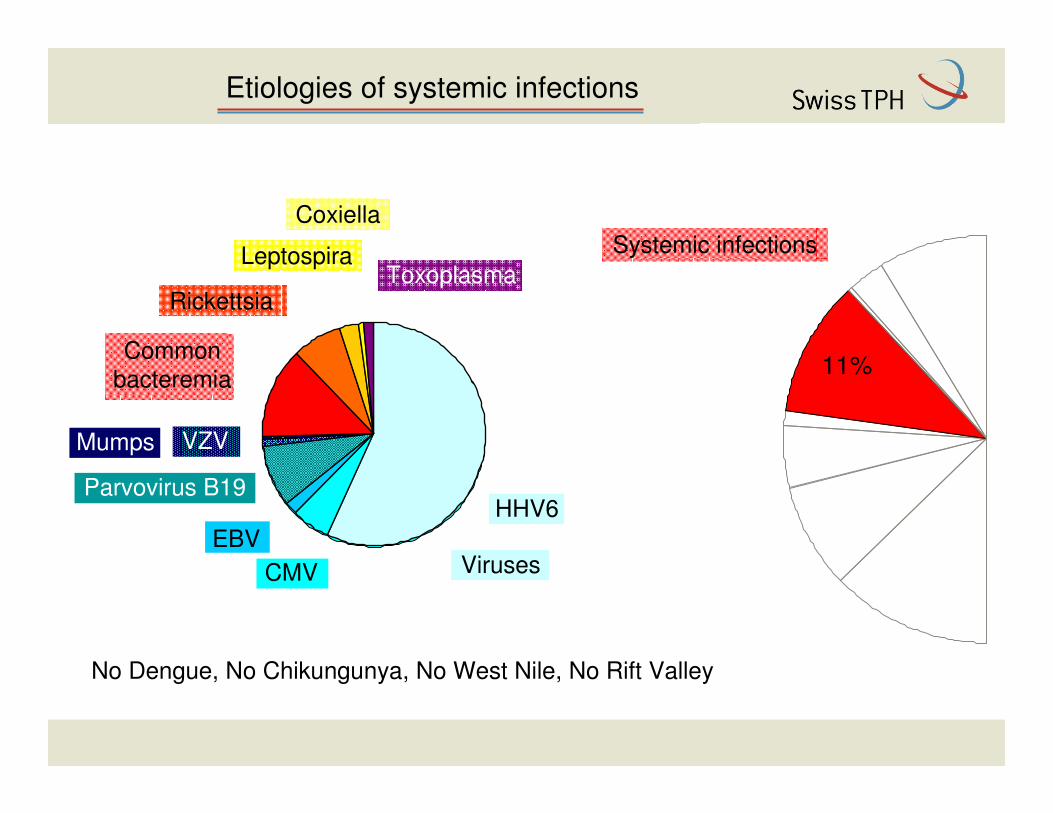
18
8%
11%
Systemic infections
Viruses
HHV6
CMV
EBV
Parvovirus B19
VZVMumps
Common
bacteremia
Rickettsia
Leptospira
Coxiella
Toxoplasma
75%
No Dengue, No Chikungunya, No West Nile, No Rift Valley
Etiologies of systemic infections

19
Summary of findings
• In Tanzanian children, half of fevers are due to acute respiratory
infections (ARI)
• A quarter of ARI were due to influenza
• 81% of the children were infected with one or more viruses
• Malaria (9%), urinary tract infection (5%) and typhoid (3%) were
much less prevalent than clinicians think
• In children: cosmopolitan >>> tropical vector-borne pathogens
• Children rarely had more than one significant diseases at a time
• 47% of severe patients were not admitted to the ward

20
Guidelines: IMCI and iCCM
NO
Blood in stool
Malaria Dysentery
ACT
Fever
<7 days Cough
Pneumonia
Diarrhea
Cold
Fast breathing
‘Watery’ diarrhea
Amoxicillin
Antimalarials and antibioticsYES
NO
No drug Ciprofloxacin ORS+
Zinc
Ear pain
Amoxicillin
YES NO YES NO
REFER
Acute otitis
media
Danger signs
Malaria test
No drug
POS NEG
Salbutamol

21
The way forward
• In our study, only 27% had a disease that needs antibiotics
• If we had applied the IMCI algorithm to these children, 25% would
have received antibiotics, BUT:
Our study IMCI13%12%15%

22
ALMANACH
How can we improve the IMCI clinical algorithm with available tools?
1) including the clinical predictors found in the fever study
2) adding diagnostic tests to RDT for malaria :
- RDT for influenza or RSV (cough) ?
- chest Xray (clinical pneumonia) ?
- urine dipstick (children <2 years) ?
- RDT for typhoid (children >2 years) ?
The way forward in diagnostics
Our study 17%18%9%

23
We need a rapid and portable test that detects
(malaria and) ONLY patients in need for antibiotics:
BUT who are they?
� All patients who have no respiratory virus?
� All patients who have a ‘respiratory bacteria’?
� All patients who have a bacteria in blood (including typhoid)?
NO, so what?
Biomarkers of severity…
… with a clever combination of the above.
The ‘fever stick’

24
Implications for treatment of febrile illnesses
Based on what we are presently able to diagnose:
(excluding severe and immunosuppressed children)
• Amoxicillin for clinical pneumonia and acute otitis media
• Oseltamivir for influenza (children <2 years, chronic condition)
• Inhaled salbutamol + spacer for wheezing
• ORS + Zinc for diarrhea
• Ciprofloxacin for UTI, bloody diarrhea (and typhoid)
• Cloxacillin for significant skin infection
• Tetracyclin eye ointment + vitamine A for measles
64%18%

25
DSM City Medical Office of Health, Tanzania
Judith Kahama (co-researcher)
Ndeniria Swai (research assistant)
Gerumana Mpawa (logistics and data entry)
Ministry of health and Welfare, Tanzania
Deo Mtasiwa (Chief Medical Officer)
Ifakara Health Institute, Tanzania
Hassan Mshinda (ex-director)
Amana and St Francis hospital, Tanzania
Willy Sangu and P. Kibatala (directors)
Swiss Tropical and Public Health Institute
Blaise Genton and Christian Lengeler
Hôpitaux Universitaires de Genève
Laurent Kaiser, Pascal Cherpillod, Yves Thomas, C. Tapparel
Financial support from the Swiss National Science Foundation
Acknowledgements
Special thanks to lab
technicians who
performed 28’352
microbiological tests
…


















