
Curricullum Vitae - Official Website of Andalas … · Curricullum Vitae Dr. Isman Firdaus, SpJP...
37
Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: [email protected] Qualification : o GP – 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist 2011 - present Possition : • Consultant of Cardiovascular Intensivist in Emergency Instalation and Intensive Cardiovascular Care Unit, Harapan Kita Hospital • Critical Care Cardiology Division, Departement Cardiology and Vascular Medicine, University of Indonesia SymCARD 2013 Padang-West Sumatera 17- 19 Mei 2013
Transcript of Curricullum Vitae - Official Website of Andalas … · Curricullum Vitae Dr. Isman Firdaus, SpJP...

Curricullum VitaeDr. Isman Firdaus, SpJP (K), FIHAEmail: [email protected]
Qualification :
o GP – 2001 (FKUI)
o Cardiologist 2007 (FKUI)
o Cardiovascular Intensivist 2010 - present
o Cardiovascular Intervensionist 2011 - present
Possition :
• Consultant of Cardiovascular Intensivist in Emergency Instalationand Intensive Cardiovascular Care Unit, Harapan Kita Hospital
• Critical Care Cardiology Division, Departement Cardiology and Vascular Medicine, University of Indonesia
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Post Cardiac Arrest Care in ACS: Role of Therapeutic Hypothermia
Isman Firdaus, MD, FIHA
Critical Care Cardiology Sub Division
Intensive Cardiovascular Care Unit of National Heart Center, Harapan Kita Hospital
Departement Cardiology and Vascular Medicine, University of Indonesia
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Chain of Survival
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Cardiac arrest in the ICU
• Causes of arrest
– Metabolic disturbances 29%
– Shock 26%
– Hypoxemia 23%
– Cardiac ischemia 15%
– Brain death 7%
– PE 2%
• Initial rhythms
– Asystole 47%
– Brdycardia followed by asystole 29%
– PEA 18%
– V Fib/V Tach 6%
Hospital survival is 11% Critical care, 2001
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Cardiopulmonary Resuscitation on TV
• 97 episodes of ER, Chicago Hope and Rescue 911 reviewed
• 60 incidents of Cardiac arrest observed• Etiology of cardiac arrest 55% trauma,28% cardiac• 75% of patients survived the immediate arrest• 68% survived to hospital discharge• 10 cases had miraculous recovery when physicians
gave up hope.• Almost all patients surviving had normal neurolgic
and functional outcome.
NEJM 1996 :334 (1578-82)SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Outcome of in-hospital cardiac arrest
• National Registry of Cardiopulmonary Resuscitation (NRCPR) of 14720 in-hospital arrests with 17% hospital discharge.
– 16% of patients had V Fib as initial rhythm with 34% hospital discharge
• 105 patients with in-hospital arrests reviewed.44% survived the arrest and 22% survived to discharge
• Better prognosis
– Cardiac etiology
– V Tach or V Fib
Internal Medicine Journal 34 ; 398 - July 2004SymCARD 2013 Padang-West Sumatera 17-
19 Mei 2013

Critical care medicine 1999
Survival According to Initial Rhythm
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Can the outcome of cardiac arrest be improved ??
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Benson et al,Anesth Analg 1959; 38: 423-8.
• Comatose survivors
• Asystole or VF
• 31-32°C
• Cooling until neurologic recovery(3 hours to 8 days)
• Water-filled blanket
0
10
20
30
40
50
60
Favorable neurologic
recovery
%
Hypothermia (n=12)
Normothermia (n=7)
The Use of Hypothermia After Cardiac Arrest
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Mild Therapeutic Hypothermia to Improve the Neurologic Outcome After Cardiac Arrest (HACA)
• Patients with witnessed cardiac arrest from VF or pulseless VT, 18-75 years of age, estimated 5-15 minutes to attempted resuscitation, and less than 60 minutes from collapse to restoration of spontaneous circulation (ROSC).
• 275 patients of 3,551 cardiac arrests screened were eligible for the study (8%)
• 137 patients randomized to receive hypothermia (32-34°c) for 24 hours
Dr. Fritz Sterz, Vienna, Austria, and The Hypothermia After Cardiac Arrest
Study Group, N Engl J Med 2002; 346:549-556SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

HACA Study Group
• Randomized trial 2002 -Hypothermia vs Normothermia
• Methods
– Inclusion - CA due to VF
– Exclusion – cardiogenic shock
• Hypothermia group
– 32°C - 34°C
– Cooled for 24 hrs
– Rewarming over 8 hrs
Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549-556.
3351assessed
3246ineligible
30Not included
275enrolled
137hypothermia
138normothermia
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013
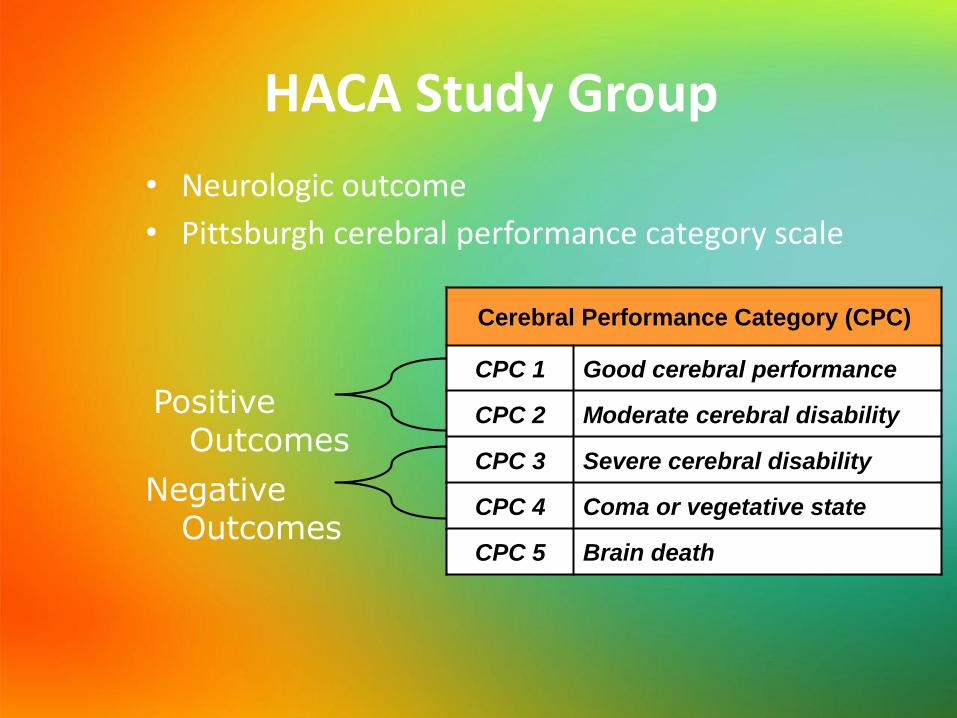
HACA Study Group
• Neurologic outcome
• Pittsburgh cerebral performance category scale
Cerebral Performance Category (CPC)
CPC 1 Good cerebral performance
CPC 2 Moderate cerebral disability
CPC 3 Severe cerebral disability
CPC 4 Coma or vegetative state
CPC 5 Brain death
Positive Outcomes
Negative Outcomes

Hypothermia for Coma After Cardiac Arrest
Hypothermia
Normothermia
P 0.02
Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549-556.SymCARD 2013 Padang-West Sumatera 17-
19 Mei 2013

Mild Therapeutic Hypothermia to Improve the Neurologic Outcome After Cardiac Arrest (HACA)
• Mortality at 6 months was 41% in the hypothermia group and 55% in the normothermia group
• 55% of hypothermia group and 39% of normothermia group had a favorable neurologic outcome (good recovery or moderate disability) p value 0.009
• Complication rate did not differ significantly between the two groups
Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549-556.SymCARD 2013 Padang-West Sumatera 17-
19 Mei 2013

Treatment of Comatose Survivors of Cardiac Arrest with Induced Hypothermia
• Survival was 21/43 of the hypothermia group (49%) vs. 9/34 treated with normothermia (25%) p = 0.01
• Good outcome (normal or with minimal or moderate disability) was 49% in hypothermia group and 26% in the normothermia p = 0.046
Bernard et al. (Australia), N Engl J Med 2002; 346:557-563SymCARD 2013 Padang-West Sumatera 17-
19 Mei 2013

Favorable Neuro Outcome :All three studies combined
• Benson 1959– 50% with Hypo (12)
– 15% with Normo (7)
• HACA 2002– 55% with Hypo (137)
– 39% with Normo (138)
• Bernard 2002– 49% with Hypo (43)
– 25% with Normo (34)
Total patients:
Hypo = 192
Normo = 179
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Combined Data (3 studies)
• Favorable Neuro
– Hypothermia = 53% (102/192)
– Normothermia = 35% (63/116)
Chi Square Testing:
p < 0.0005
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Cooling Experience in Indonesia ??
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013
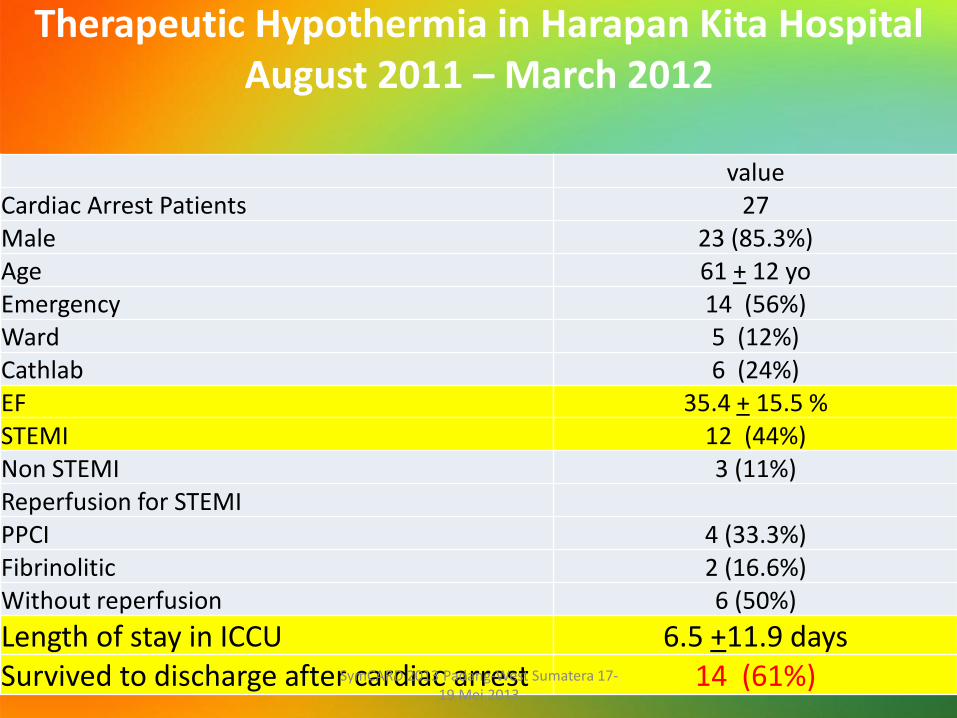
Therapeutic Hypothermia in Harapan Kita HospitalAugust 2011 – March 2012
valueCardiac Arrest Patients 27Male 23 (85.3%)Age 61 + 12 yoEmergency 14 (56%)Ward 5 (12%)Cathlab 6 (24%)EF 35.4 + 15.5 %STEMI 12 (44%)Non STEMI 3 (11%)Reperfusion for STEMIPPCI 4 (33.3%)Fibrinolitic 2 (16.6%)Without reperfusion 6 (50%)
Length of stay in ICCU 6.5 +11.9 daysSurvived to discharge after cardiac arrest 14 (61%)SymCARD 2013 Padang-West Sumatera 17-
19 Mei 2013

SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

AHA guidelines for ACLS and post CPR care
• In a select subset of patients who were initially comatose but hemodynamicaly stable after a witnessed VF arrest of presumed cardiac etiology, active induction of hypothermia was beneficial. Thus, unconscious adult patients with ROSC after out-of-hospital cardiac arrest should be cooled to 32°C to 34°C for 12 to 24 hours when the initial rhythm was VF (Class IIa). Similar therapy may be beneficial for patients with non-VF arrest out of hospital or for in-hospital arrest (Class IIb).
2005 AHA guidelines, Circulation
2010 AHA guideline, ACLS Updated SymCARD 2013 Padang-West Sumatera 17-
19 Mei 2013

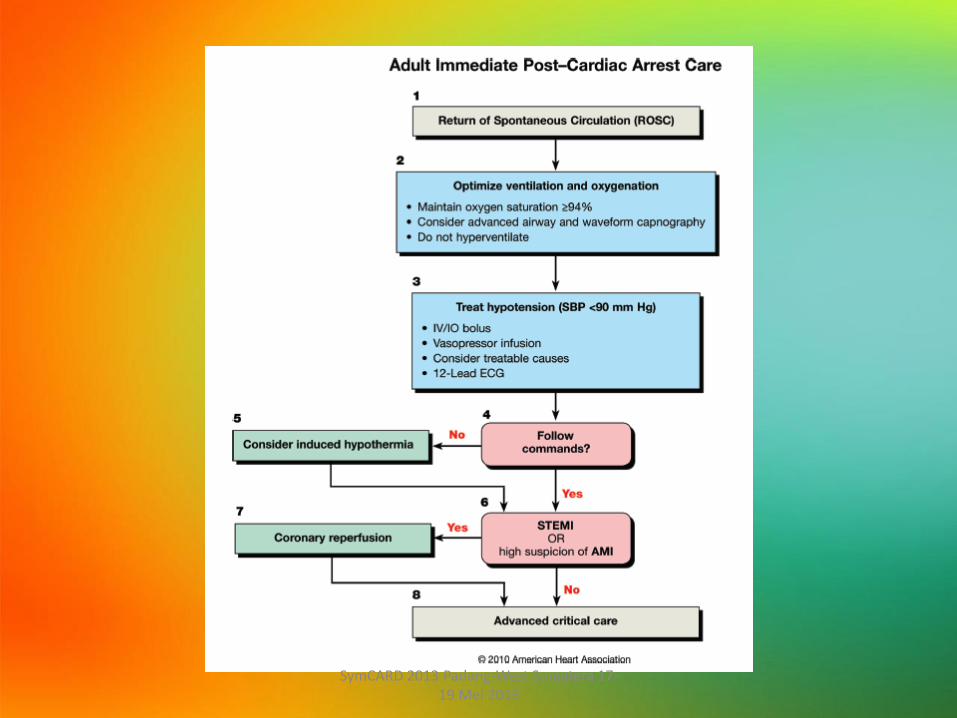
Post– Cardiac Arrest Care ProgramAHA Guideline 2010
• Therapeutic hypothermia
• Optimization of hemodynamics and gas exchange
• Immediate coronary reperfusion when indicated
• Glycemic control
• Neurological
• Diagnosis, management, and prognostication.
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

How to apply hypothermia ??
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Four Modes of Heat Transfer
• Conduction– Cold water immersion
• Radiation– Cold room
• Convection– Fans (do not use for infection control purposes)
• Evaporation– Sweating
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Basics of Therapeutic Hypothermia: Three phases of treatment
– Induction• Rapidly bring the temperature to 32-34C• Sedate with propofol or midazolam during TH• Paralyze to suppress heat production
– Maintenance• maintain the goal temperature at 33C• Standard 12-24 hours (optimal duration is
unknown)• Suppress shivering
– Rewarming• Most dangerous period: hypotension, brain swelling, • Goal is to reach normal body temperature over 12-
24h• Stop all sedation when normal body temperature is
achieved
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Induction: How to Cool
• Commercial cooling devices– Servo mechanism varies temperature of
circulating water or air (prevents overcooling)
– External (surface cooling) systems• Hydrogel heat exchange pads
• Cold water circulating through plastic “suit”
• Cold water immersion – awaiting safety data
– Invasive (catheter based) systems• Heat exchange catheter in SVC or IVC
• Plastic or metalic heat-exchange catheter
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Cooling Devices
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Management of shivering
• Neuromuscular blockade– Vecuronium bolus 0.1mg/kg prn BSAS>2
– Cisatricurium in renal failure
• Propofol
• Alpha blockade– Dexmedetomidine infusion or clonidine
• Scheduled acetaminophen, buproprion
• Meperidine or fentanyl
• Focal counterwarming
• Magnesium infusion (serum level 3mg/dl)
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Re-warming
If using surface cooling: Use passive re-warming
Remove Ice packs
Stop cold Iv fluids
If using endovascular cooling: set temperature rise at 0.3-0.5 degrees per hour
Avoid rapid re-warming
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Maintainance: how to cool
• Monitor core temperature– Bladder, esophagus, or central venous/pulmonary
arterial
• Ice packs and cooling mats– Effective, but difficult to control rate of
temperature change
– Overcooling is dangerous
• Endovascular cooling allows for gradual reduction in temp, maintainence at desired temp and prevents over cooling
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Take home messages
• Strong evidence that mild hypothermia is neuro-protective after return of spontaneous circulation
• Hypothermia is underutilized so far but should be included in post resuscitaion care of cardiac arrest victims
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

...The Last but not Least...
كل نفس ذائقة الموت...Setiap yang hidup pasti akan mati...
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013

Hypothermia Questions
• How to monitor cooling?– Bladder, rectal or blood temperature? Brain temperature?
• How should we manage shivering? – If use NMB, need to monitor EEG
– Sub-clinical seizures may be more common than clinically recognized – should we load with anticonvulsants?
• How to adjust medications in the hypothermic patient
• Are there useful biomarkers?
SymCARD 2013 Padang-West Sumatera 17-19 Mei 2013


















