Current Concepts in Imaging of Small Bowel Obstruction
21
Current concepts in imaging of small bowel obstruction Dean D.T. Maglinte, MD a, * , Darel E. Heitkamp, MD a , Thomas J. Howard, MD, FACS b , Frederick M. Kelvin, MD c , John C. Lappas, MD a a Department of Radiology, Indiana University Medical Center, 550 North University Boulevard, UH0279, Indianapolis, IN 46202-5243, USA b Division of General Surgery, Indiana University School of Medicine, 545 Barnhill Drive, EH523, Indianapolis, IN 46202, USA c Department of Radiology, Methodist Hospital of Indiana, 1701 North Senate Boulevard, Indianapolis, IN 46202, USA Despite recent advances in abdominal imaging, intestinal obstruction remains a difficult disease entity to diagnose accurately and treat [1 – 3]. Small bowel obstruction (SBO) is a common clinical condition, often presenting with signs and symptoms similar to those seen in other acute abdominal disorders. Once intestinal obstruction is suspected based on the patient’s clinical history and physical examination, diagnostic imaging is charged with the task of veri- fying the presence of obstruction and providing cogent information on the site, severity, and probable cause of the obstruction. By providing this broad range of anatomic information, imaging impacts directly on patient management, specifically addressing the cru- cial question of whether a trial of nonoperative therapy should be instituted rather than resorting to immediate surgery because of the possibility of strangulation [4,5]. Because of its ability to provide important anatomic and functional information, radiology has become a vital tool in the clinical decision making of patients with known or suspected SBO. This article examines current concepts in the imaging of SBO. Clinical considerations Small bowel obstruction is responsible for 12% to 16% of admissions to the surgical service in patients with acute abdominal conditions [6]. Establishing the diagnosis in a timely manner is best accomplished by relying on the classic investigational triad of a well-taken history, a careful physical examination, and appropriate ancillary testing. The diagnosis of mechanical SBO is straightforward when the classic findings of crampy abdominal pain, distention, nau- sea, and vomiting are present along with abdominal radiographic (plain film) findings of small bowel distention, multiple air-fluid levels, and decreased colonic gas and stool [4]. In many cases, the dia- gnosis is much more subtle because most patients fail to present with a classic history and often have vague abdominal findings on physical examination. Plain abdominal radiographs have been found not to sup- port the clinical diagnosis of obstruction in nearly one third of surgically proved cases. Based on these observations, after a complete history and physical and abdominal plain films, if the clinical suspicion for intestinal obstruction remains high, further abdominal imaging is often indicated [4,7]. The three most common causes of SBO in the western world are (1) adhesions, (2) Crohn’s disease, and (3) neoplasia [8]. In the past, hernias represented a major cause of SBO in the United States, but improvements in health care availability and the increase in elective hernia repair has led to a sub- stantial decline in the incidence of SBO related to abdominal wall hernias. Hernias, however, still rep- resent the predominant cause of SBO in many devel- oping countries. Crohn’s disease has only recently been acknowledged in the surgical literature as a 0033-8389/03/$ – see front matter D 2003, Elsevier Science (USA). All rights reserved. doi:10.1016/S0033-8389(02)00114-8 * Corresponding author. E-mail address: [email protected] (D.T.T. Maglinte). Radiol Clin N Am 41 (2003) 263 – 283
-
Upload
piterwisely -
Category
Documents
-
view
10 -
download
0
description
fdsfg
Transcript of Current Concepts in Imaging of Small Bowel Obstruction
Current concepts in imaging of small bowel obstruction
Dean D.T. Maglinte, MDa,*, Darel E. Heitkamp, MDa,Thomas J. Howard, MD, FACSb, Frederick M. Kelvin, MDc,
John C. Lappas, MDa
aDepartment of Radiology, Indiana University Medical Center, 550 North University Boulevard, UH0279,
Indianapolis, IN 46202-5243, USAbDivision of General Surgery, Indiana University School of Medicine, 545 Barnhill Drive, EH523, Indianapolis, IN 46202, USA
cDepartment of Radiology, Methodist Hospital of Indiana, 1701 North Senate Boulevard, Indianapolis, IN 46202, USA
Despite recent advances in abdominal imaging,
intestinal obstruction remains a difficult disease entity
to diagnose accurately and treat [1–3]. Small bowel
obstruction (SBO) is a common clinical condition,
often presenting with signs and symptoms similar to
those seen in other acute abdominal disorders. Once
intestinal obstruction is suspected based on the
patient’s clinical history and physical examination,
diagnostic imaging is charged with the task of veri-
fying the presence of obstruction and providing cogent
information on the site, severity, and probable cause of
the obstruction. By providing this broad range of
anatomic information, imaging impacts directly on
patient management, specifically addressing the cru-
cial question of whether a trial of nonoperative therapy
should be instituted rather than resorting to immediate
surgery because of the possibility of strangulation
[4,5]. Because of its ability to provide important
anatomic and functional information, radiology has
become a vital tool in the clinical decision making of
patients with known or suspected SBO. This article
examines current concepts in the imaging of SBO.
Clinical considerations
Small bowel obstruction is responsible for 12% to
16% of admissions to the surgical service in patients
with acute abdominal conditions [6]. Establishing the
diagnosis in a timely manner is best accomplished
by relying on the classic investigational triad of a
well-taken history, a careful physical examination,
and appropriate ancillary testing. The diagnosis of
mechanical SBO is straightforward when the classic
findings of crampy abdominal pain, distention, nau-
sea, and vomiting are present along with abdominal
radiographic (plain film) findings of small bowel
distention, multiple air-fluid levels, and decreased
colonic gas and stool [4]. In many cases, the dia-
gnosis is much more subtle because most patients fail
to present with a classic history and often have vague
abdominal findings on physical examination. Plain
abdominal radiographs have been found not to sup-
port the clinical diagnosis of obstruction in nearly one
third of surgically proved cases. Based on these
observations, after a complete history and physical
and abdominal plain films, if the clinical suspicion for
intestinal obstruction remains high, further abdominal
imaging is often indicated [4,7].
The three most common causes of SBO in the
western world are (1) adhesions, (2) Crohn’s disease,
and (3) neoplasia [8]. In the past, hernias represented
a major cause of SBO in the United States, but
improvements in health care availability and the
increase in elective hernia repair has led to a sub-
stantial decline in the incidence of SBO related to
abdominal wall hernias. Hernias, however, still rep-
resent the predominant cause of SBO in many devel-
oping countries. Crohn’s disease has only recently
been acknowledged in the surgical literature as a
0033-8389/03/$ – see front matter D 2003, Elsevier Science (USA). All rights reserved.
doi:10.1016/S0033-8389(02)00114-8
* Corresponding author.
E-mail address: [email protected] (D.T.T. Maglinte).
Radiol Clin N Am 41 (2003) 263–283

leading cause of SBO, a fact that has long been
suspected in many clinical radiology departments [8].
Controversy still exists surrounding the manage-
ment of patients with adhesive SBO. If the obstruction
is partial or early in the postoperative period ( < 6
weeks from operation), many surgeons recommend a
trial of conservative treatment with intestinal decom-
pression in the belief that, with close patient monitor-
ing, surgery frequently can be avoided altogether
[1,9–12]. Other surgeons advocate early surgical
management for all patients, particularly those with
complete intestinal obstruction, based on the high
complication rate associated with delayed operative
intervention in this group of patients [13–16]. Clinical
experience has shown that simple mechanical obstruc-
tion cannot be reliably differentiated from strangulated
obstruction on the basis of clinical, laboratory, or
abdominal plain film findings [9,15,17–21]. Histor-
ical data in patients with surgically proved strangula-
tion show that the preoperative diagnosis is unreliable
in 50% to 85% of cases [2,9,16,22–24]. The current
mortality rate of patients with adhesive intestinal
obstruction is in the 1% to 2% range [25,26], suggest-
ing that the risks associated with conservative man-
agement may be acceptable as long as emergent
surgery is performed at the first sign of patient deteri-
oration or evidence of incarceration or strangulation is
found. Recent clinical series have shown that even
patients with high-grade mechanical SBO can have a
substantial rate of resolution with conservative nasoin-
testinal decompression, further supporting an even-
handed approach to patients with SBO [11,15,27,28].
Abdominal radiography
Despite its limitations, abdominal radiography
remains the initial imaging study in patients with
abdominal symptoms, particularly in those with pos-
sible intestinal obstruction. Its diagnostic value tends
to be highest in patients with signs or symptoms of
biliary or urinary system calculi, intestinal obstruc-
tion, perforation, or ischemia. Plain films are least
helpful in patients with vague abdominal pain and
nonspecific physical findings. Its role in the evalu-
ation of calculi, perforation, or ischemia has been
replaced by CT.
In the setting of SBO, abdominal radiographs are
diagnostic in 50% to 60% of cases [17–20,29]. In an
analysis of plain film findings reported by experi-
enced gastrointestinal radiologists, a sensitivity of
only 66% was found in proved cases of SBO [7].
Twenty-one percent of patients reported as normal
were in fact obstructed. Of patients whose films were
interpreted as abnormal but nonspecific, 13% had
low-grade and 9% had high-grade obstruction. Addi-
tionally, abdominal radiography has shown a low
specificity for SBO, because mechanical and func-
tional large bowel obstructions can mimic the radio-
graphic findings observed in SBO [30]. Despite these
acknowledged limitations of this examination, plain
film radiography remains an important study in
patients with suspected SBO because of its wide-
spread availability and low cost. Although in many
cases the abdominal radiographs are nondiagnostic,
their findings can be valuable in guiding subsequent
imaging, or following disease progression.
A degree of confusion still exists among radiol-
ogists and clinicians over the meanings of common
descriptors used to identify various intestinal gas
patterns on abdominal radiographs [31,32]. Many
physicians frequently use the term nonspecific bowel
gas pattern to actually mean normal bowel gas
pattern [3]. One survey showed that 70% of radiol-
ogists used the term nonspecific in their interpreta-
tions, with 65% trying to convey a normal or
probably normal bowel gas pattern, 22% meaning
to say that they cannot tell if it is normal or abnormal,
and 13% interpreting this to mean abnormal but
cannot tell if it represents mechanical obstruction or
adynamic ileus. Clearly, the term nonspecific is
imprecise and its use ultimately can lead to serious
errors in patient management. If used at all, it should
be qualified as ‘‘abnormal, but nonspecific,’’ satisfy-
ing a group of plain film findings that fits neither the
‘‘normal’’ nor ‘‘definitely abnormal’’ categories. This
qualification adds its own set of clinical implications
[33]. The use of ambiguous terms, such as ‘‘non-
obstructive gas pattern,’’ which does not indicate
whether the gas distribution is normal or abnormal,
should be abandoned.
The use of well-defined terms for describing bowel
gas patterns is essential for generating understandable
reports for clinicians and other radiologists. (1) The
normal small bowel gas pattern refers to either
absence of small bowel gas or small amounts of gas
within up to four variably shaped nondistended (less
than 2.5 cm in diameter) loops of small bowel. A
normal distribution of gas and stool within a non-
distended colon should also be recognized. (2) Abnor-
mal but nonspecific gas describes a pattern of at least
one loop of borderline or mildly distended small
bowel (2.5 to 3 cm in diameter) with three or more
air-fluid levels on upright or lateral decubitus radio-
graphs. The colonic gas and feces distribution is either
normal or displays a similar degree of borderline
distention. This pattern can also be correctly labeled
‘‘mild small bowel stasis,’’ because many conditions
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283264

can produce it, including low-grade obstruction, reac-
tive ileus, and medication-induced hypoperistalsis. (3)
The probable SBO pattern consists of multiple gas- or
fluid-filled loops of dilated small bowel with a mod-
erate amount of colonic gas. The presence of colonic
gas indicates early complete mechanical SBO, an
incomplete SBO, or nonobstructive ileus. This pattern
can be seen in several acute intra-abdominal inflam-
matory conditions that involve the small bowel (diver-
ticulitis, appendicitis, or mesenteric ischemia). This
diagnosis should trigger further investigation with a
prompt CT enteroclysis in a patient with no objective
clinical findings. (4) The definite SBO pattern shows
dilated gas or fluid-filled loops of small bowel in the
setting of a gasless colon. This constellation of find-
ings is pathognomonic for SBO [4].
Various small bowel gas patterns are shown in
Fig. 1A–N. These patterns should be distinguished
from the distended small bowel occurring secondary to
left-sided colonic obstruction. In this pattern, in addi-
tion to the distended small bowel, a fluid-filled right
colon and fluid and gas distended transverse colon can
also be recognized (Fig. 2). The small bowel distention
seen in this setting is secondary to decompression of
the colonic distention through the ileocecal valve.
Two findings on the upright abdominal radiograph
can help differentiate high-grade obstruction from
lower-grade obstruction: the presence of differential
air-fluid levels in the same bowel loop, and a mean air-
fluid level width of at least 25 mm (see Fig. 1M). The
combined presence or absence of these two radio-
graphic findings has a strong positive (86%) and
negative (83%) predictive value of the degree of
patency of the small bowel lumen [34]. Although
upright radiographs alone are not particularly sensi-
tive for SBO, they may be of value in distinguishing
patients with high-grade or complete obstruction from
those with low-grade or partial obstruction. Because
of its widespread availability, relative low cost, and
high sensitivity in revealing high-grade SBO, the use
of abdominal plain radiographs remains a prominent
imaging tool in the evaluation of suspected SBO [29].
Barium radiography
Because barium does not typically inspissate
within the adynamic gut, it can be used safely to
evaluate SBO [35,36]. Ingested orally, iodinated
water-soluble contrast agents result in poor mucosal
detail on radiography and are quite hypertonic.
Although radiography using water-soluble agents
was once used by some institutions to triage patients
into surgical versus nonsurgical management, the
widespread use of abdominal CT has largely sup-
planted this practice [37–39]. Despite the strong
opinion of a few advocates, the use of water-soluble
contrast has been shown to have no therapeutic effect
in patients with postoperative SBO [40].
Barium evaluation of the small intestine can be
performed by either nonintubation or intubation-infu-
sion techniques [4]. The nonintubation methods
include the retrograde small bowel enema; the per
enterosotomy (colostomy, ileostomy) small bowel
enema; and the small bowel follow-through.
Although the small bowel follow-through is a useful
technique when performed with meticulous fluoros-
copy, it has known limitations in the setting of SBO
[41–43]. In cases of high-grade obstruction, dilution
of barium by fluid in the dilated proximal bowel
typically results in incomplete small bowel opacifi-
cation and poor mucosal detail. The duration of the
small bowel follow-through examination is directly
related to small bowel transit time, both of which are
often markedly prolonged in cases of high-grade
obstruction. Moreover, nonintubation barium tech-
niques are inherently limited in their ability to assess
intestinal distensibility and fixation of small bowel
loops [42]. As a result, they may not detect partially
obstructing lesions that produce only fleeting or
inconspicuous prestenotic dilatations when viewed
under fluoroscopy. Despite these limitations, inter-
mittent fluoroscopic monitoring can often yield
important information making the technique a viable
alternative for radiology departments lacking suf-
ficient expertise in performing enteroclysis [42,43].
Enteroclysis overcomes the limitations of the non-
intubation techniques by challenging the distensibil-
ity of the bowel wall and exaggerating the effects
of mild or subclinical mechanical obstruction (see
Fig. 1B, C). Intubating the small bowel bypasses the
pylorus, enabling delivery of a nondiluted barium or
iodinated contrast bolus directly into the jejunum.
Sequential infusion of barium and methylcellulose or
iodinated contrast during CT enteroclysis promotes
antegrade flow of contrast toward the site of obstruc-
tion despite the presence of diminished bowel peri-
stalsis. The resultant luminal distention facilitates
detection of both fixed and nondistensible bowel
segments. Clinical studies have shown that the
intubation infusion method of small bowel examina-
tion can correctly predict the presence of obstruction
in 100%, the absence of obstruction in 88%, the level
of obstruction in 89%, and the cause of obstruction
86% of patients [7].
SBO is excluded by enteroclysis or CT enter-
oclysis when unimpeded flow of contrast material is
observed within normal-caliber small bowel loops
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 265
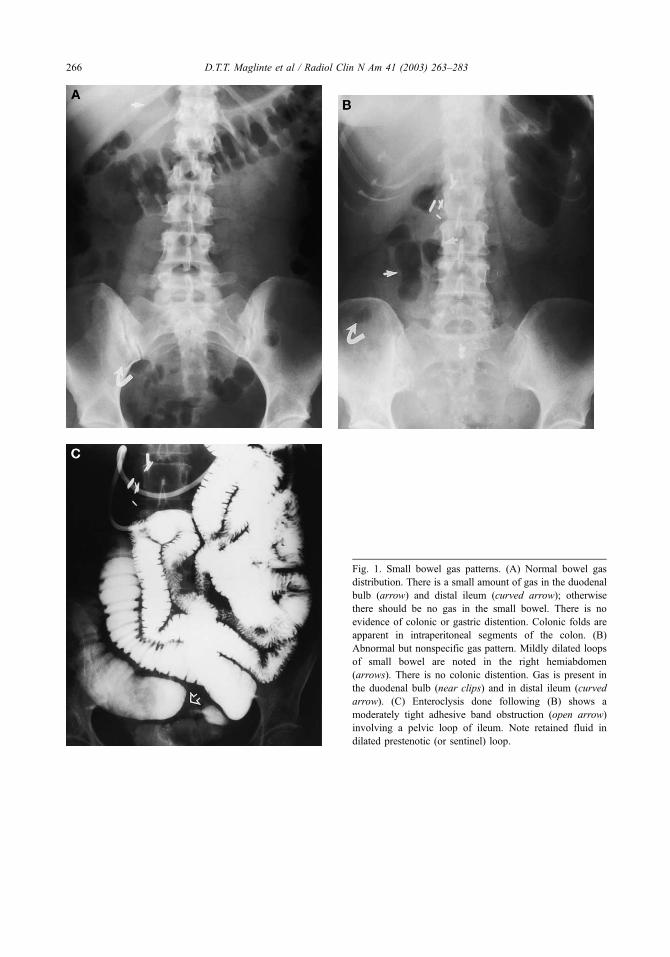
Fig. 1. Small bowel gas patterns. (A) Normal bowel gas
distribution. There is a small amount of gas in the duodenal
bulb (arrow) and distal ileum (curved arrow); otherwise
there should be no gas in the small bowel. There is no
evidence of colonic or gastric distention. Colonic folds are
apparent in intraperitoneal segments of the colon. (B)
Abnormal but nonspecific gas pattern. Mildly dilated loops
of small bowel are noted in the right hemiabdomen
(arrows). There is no colonic distention. Gas is present in
the duodenal bulb (near clips) and in distal ileum (curved
arrow). (C) Enteroclysis done following (B) shows a
moderately tight adhesive band obstruction (open arrow)
involving a pelvic loop of ileum. Note retained fluid in
dilated prestenotic (or sentinel) loop.
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283266

Fig. 1. (D) Abnormal but nonspecific gas pattern. Small
amounts of gas (arrows) are noted in nondistended small
bowel loops in left hemiabdomen and pelvis in addition to
usual gas in distal ileum in chronic renal patient presenting
with abdominal pain, nausea, and vomiting who also had
recent ventral herniorrhaphy and subsequent wound infec-
tion. Note semisolid fecal debris in right colon. This
distribution is also known as small bowel stasis pattern.
(E) Enteroclysis radiography shows no significant distention
proximal to intraluminal filling defects (curved arrow) in
ileum. (F) Further infusion of methylcellulose shows distal
movement of intraluminal filling defects towards cecum
(curved arrow).
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 267

Fig. 1. (G) Infusion radiograph shows that the filling defects
in distal ileum have been flushed into the right colon and the
distal and terminal ileum (arrow) are normal confirming that
the abnormal but nonspecific small bowel gas pattern is
secondary to medication-related hypoperistalsis. The small
bowel stasis pattern is not uncommon in hospitalized patients
on analgesics or sedatives. C, cecum. (H) Probable small
bowel obstruction (SBO) pattern. Upright abdominal radio-
graph shows air-fluid levels in multiple moderately distended
loops of small bowel. Gas and fluid are present in transverse
colon (arrow in a haustrum) and sigmoid. The pattern is
suggestive of mechanical SBO but can be seen in sigmoid
diverticulitis or appendicitis. (I) CT obtained following (H)
shows a lower abdominal anterior parietal peritoneal fixation
of decreased-caliber small bowel loops (arrow) secondary to
dense adhesions. Note dilated small bowel proximal to
adhesions. (From Maglinte DDT, Reyes BL, Harmon BH,
et al. Reliability and the role of plain film radiography and CT
in the diagnosis of small-bowel obstruction. AJR Am J
Roentgenol 1996;167:1451–5; with permission.)
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283268
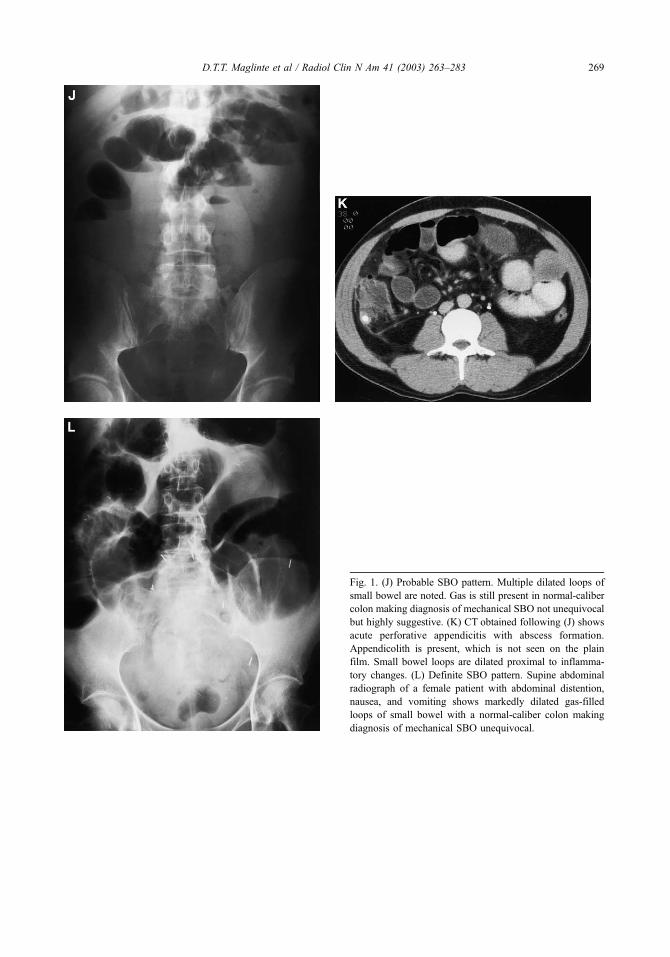
Fig. 1. (J) Probable SBO pattern. Multiple dilated loops of
small bowel are noted. Gas is still present in normal-caliber
colon making diagnosis of mechanical SBO not unequivocal
but highly suggestive. (K) CT obtained following (J) shows
acute perforative appendicitis with abscess formation.
Appendicolith is present, which is not seen on the plain
film. Small bowel loops are dilated proximal to inflamma-
tory changes. (L) Definite SBO pattern. Supine abdominal
radiograph of a female patient with abdominal distention,
nausea, and vomiting shows markedly dilated gas-filled
loops of small bowel with a normal-caliber colon making
diagnosis of mechanical SBO unequivocal.
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 269
from the duodenojejunal junction to the right colon.
The diagnosis of mechanical SBO is confirmed by
the demonstration of a transition zone, defined as a
change in the caliber of the intestinal lumen from a
distended segment proximal to the site of obstruction
to a segment that is either collapsed or decreased in
caliber distal to the site of obstruction [4,5,7,44,45].
By enteroclysis criteria, 3 cm is the upper limit of
normal for the caliber of the jejunal lumen, and 2.5 cm
is the upper limit for the ileal lumen [42]. The level of
obstruction is identified during the single-contrast
phase of the examination, whereas the cause of the
obstruction is best evaluated during the double-con-
trast phase of the study when observation of mucosal
detail is optimal. In partial SBO, enteroclysis has
been shown to be approximately 85% accurate in
distinguishing adhesions from metastases, tumor
recurrence, and radiation damage [46]. Obstructions
can occur synchronously at multiple levels, such that
if dilated fluid- or gas-filled small bowel loops are
encountered distal to a transition zone, additional
downstream obstructions need to be assessed. Enter-
oclysis is particularly helpful in patients about whom
the diagnosis of low-grade SBO is clinically uncer-
tain [47]. Its ability to distinguish low-grade obstruc-
tion from a normal examination makes it an important
tool in this difficult clinical problem [47–51].
Enteroclysis can also objectively gauge the sever-
ity of intestinal obstruction, an important advantage
over other imaging modalities [7,45]. In low-grade
partial SBO there is no delay in the arrival of contrast
to the point of obstruction, and there is sufficient flow
of contrast through the point of obstruction such that
fold patterns in the postobstructive loops are readily
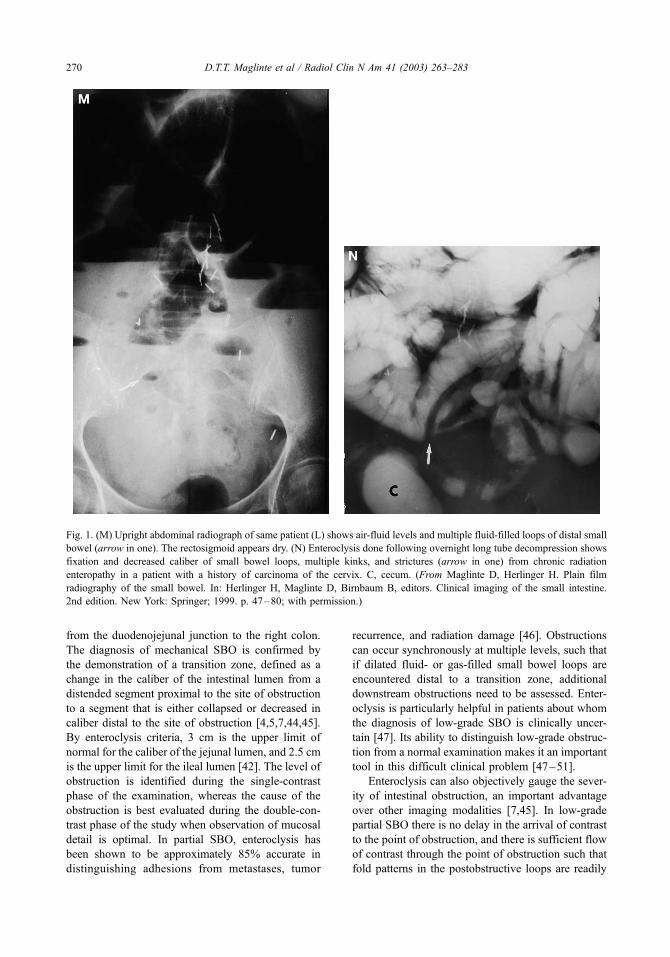
Fig. 1. (M) Upright abdominal radiograph of same patient (L) shows air-fluid levels and multiple fluid-filled loops of distal small
bowel (arrow in one). The rectosigmoid appears dry. (N) Enteroclysis done following overnight long tube decompression shows
fixation and decreased caliber of small bowel loops, multiple kinks, and strictures (arrow in one) from chronic radiation
enteropathy in a patient with a history of carcinoma of the cervix. C, cecum. (From Maglinte D, Herlinger H. Plain film
radiography of the small bowel. In: Herlinger H, Maglinte D, Birnbaum B, editors. Clinical imaging of the small intestine.
2nd edition. New York: Springer; 1999. p. 47–80; with permission.)
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283270
defined. High-grade partial SBO is diagnosed when
the presence of retained fluid dilutes the barium and
results in inadequate contrast density above the site of
obstruction, allowing only small amounts of contrast
material to pass through the obstruction into the
collapsed distal loops. Complete obstruction is diag-
nosed when there is no passage of contrast material
beyond the point of obstruction as shown on delayed
radiographs obtained up to 24 hours after the start of
the examination [7]. The authors have applied this
severity scoring to CT enteroclysis [45]. The term
closed-loop obstruction implies acute obstruction with
a tendency to progress toward infarction and the need
for urgent surgery. If a patient displays clinical signs of
a bowel compromise including localized tenderness,
fever, tachycardia, or leukocytosis, immediate resus-
citation and urgent laparotomy should be done. If
further anatomic information is required in a chal-
lenging patient (ie, multiple prior surgeries, dense
adhesions, or morbid obesity) CT should be the ini-
tial choice of imaging. Further investigation using
barium enteroclysis or positive contrast CT entero-
clysis can provide complementary information about
the obstruction, such as how much contrast material
is moving through the transition zone [29,52]. Partial
closed-loop obstruction has been demonstrated by
enteroclysis in the subacute setting [53].
Because enteroclysis requires conscious sedation,
nasointestinal intubation, and near-constant radiolo-
gist involvement, it can be impractical to perform
adequately in the outpatient clinic setting. Many
institutions also lack individuals with the proper
expertise to perform the study. If expertise is lacking,
a dedicated small bowel follow-through with close
fluoroscopic monitoring is an acceptable substitute,
provided that high-grade obstruction is not present
[41,42]. In patients with complete or high-grade
obstruction, dilution of barium occurs proximal to
the site of obstruction and makes diagnostic evalu-
ation suboptimal. Moreover, barium retained in the
small bowel can degrade the diagnostic quality of
subsequent CT examinations. In the acute setting
where time is of the essence, CT should be the initial
method of examination. In the authors’ department,
CT enteroclysis with positive enteral contrast is now
performed more frequently than barium enteroclysis
for further assessment of clinically stable patients
with SBO.
CT
CT has become important in the preoperative
evaluation of patients with suspected intestinal
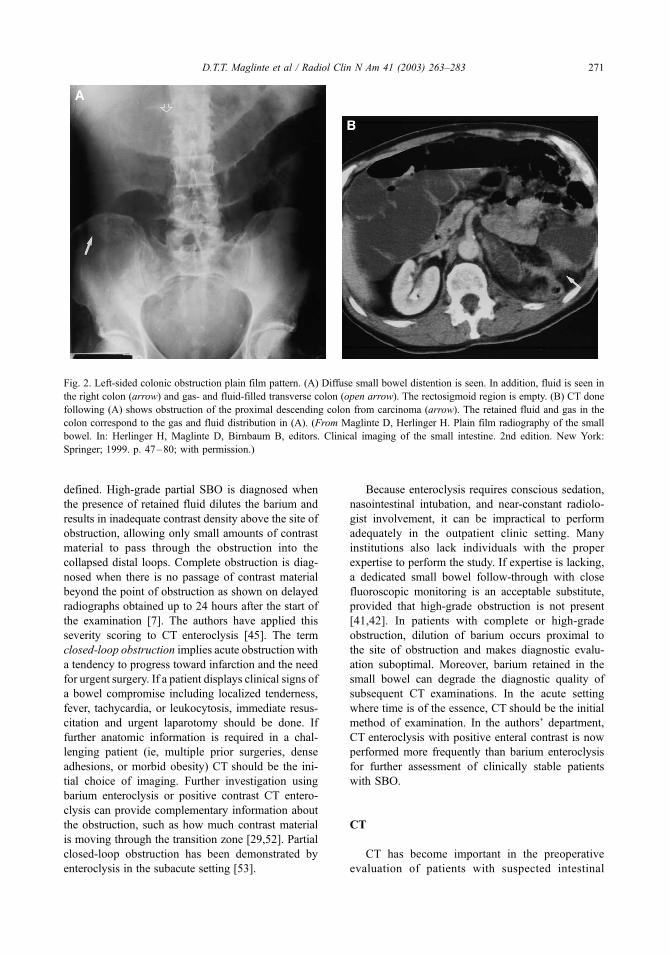
Fig. 2. Left-sided colonic obstruction plain film pattern. (A) Diffuse small bowel distention is seen. In addition, fluid is seen in
the right colon (arrow) and gas- and fluid-filled transverse colon (open arrow). The rectosigmoid region is empty. (B) CT done
following (A) shows obstruction of the proximal descending colon from carcinoma (arrow). The retained fluid and gas in the
colon correspond to the gas and fluid distribution in (A). (From Maglinte D, Herlinger H. Plain film radiography of the small
bowel. In: Herlinger H, Maglinte D, Birnbaum B, editors. Clinical imaging of the small intestine. 2nd edition. New York:
Springer; 1999. p. 47–80; with permission.)
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 271

obstruction. Although some studies report a low
overall sensitivity (63%) of CT for all grades of
SBO, sensitivity improves to 81% when high-grade
obstruction alone is considered. Conversely, sensitiv-
ity worsens to 48% in the detection of low-grade
obstruction [45]. Although CT is accurate for high-
grade SBO, it is not as sensitive for the lower grades
of obstruction that present at the subacute level or in
the outpatient setting [29].
The speed of multidetector row helical CT and its
ability to reveal the cause of obstruction make it
particularly valuable in the acute setting. CT is able to
show the cause of obstruction in 93% to 95% of cases
[29,45,54,55], at the same time revealing the more
serious conditions of closed-loop obstruction and
strangulation [27,56–64]. The exclusion of these
two complications is of great concern to many
surgeons, particularly those who believe a trial of
conservative nonoperative management is warranted
in simple mechanical SBO. Although the specificity
of contrast-enhanced CT for intestinal ischemia is
reported to be as low as 44%, its high sensitivity
(90%) and negative predictive value (89%) [61] are
quite helpful in making decisions concerning contin-
ued nonoperative management versus surgery [11].
Most cases of strangulation occur as complications
of intussusception, volvulus, torsion, or other types of
closed-loop obstruction. Interruption of the blood
supply typically occurs either from twisting of the
bowel on its mesentery or from pressure generated by
markedly distended small bowel loops. Attention to
the course of vascular arcades in the bowel on CTwith
the use of coronal mesenteric vascular mapping may
help identify cases of closed-loop obstruction before
they progress to strangulation. In a recent report [65]
the whirl sign [60], described as the convergence of
mesenteric vessels toward a twisted site [63], and
the reversal of the normal relationship between the
mesenteric artery and vein [66] were identified as the
two most important vascular indicators of closed-
loop obstruction caused by midgut volvulus as seen
on CT. The ability of CT reliably to show signs of
closed-loop obstruction, ischemia, and infarction
likely represents the most important imaging contri-
bution to the management of acute SBO. If CT is used
appropriately, its higher initial cost may result in
overall cost savings within an episode of care by
either expediting surgery or avoiding surgery in
appropriate patients, reducing comorbidities and hos-
pital length of stay.
CT is also useful in differentiating SBO from ileus
or other causes of small bowel dilatation [67,68]. In
cases of high-grade obstruction, CT has a reported
sensitivity of 100% for distinguishing obstruction
from other causes of small bowel dilatation, as com-
pared with 46% for that of plain radiographs [67]. The
literature shows that by differentiating paralytic ileus
from obstruction, CT findings modified management
in 21% of patients either by changing conservative
management to a surgical one (18%) or vice versa. CT
can expedite the need for surgery and also avoid
unnecessary laparotomy, important goals in the man-
Fig. 3. Decompression-enteroclysis catheter. (A) The catheter is introduced transnasally similar to the conventional nasogastric
tube. The black marker (arrow) in the proximal third of the tube when seen at the level of the external nares indicates the tube tip
position in the body of the stomach and allows the tube to be positioned at bedside in the emergency department or hospital ward
without fluoroscopic guidance similar to the positioning of conventional nasogastric tubes. A rubber adapter (1) allows
connection of the decompression lumen (D) (also infusion lumen) to existing suction devices. A small plastic cap (2) prevents
fluid from leaking out of the sump port (S) when suction is disconnected. The balloon (B) is used only during contrast material
infusion and is inflated by first pressing in the balloon inflation one-way valve attachment (curved arrow). (B) A Teflon-coated
stainless-steel braided torque guidewire with interchangeable ends is provided. The straight tip of the guidewire is introduced to
the level of the nasal marker (arrow in A) of the suction-infusion lumen before intubation. The 45% angle proximal to the
opposite tip of the 195-cm long guidewire allows the operator to change the direction of the tube tip when necessary. The angled
tip is used only in occasional situations of difficult directional control and to allow atraumatic nasopharyngeal tube passage in
patients with acute nasopharyngeal posterior wall angulation. The straight tip is all that is necessary to provide torque in most
transgastric intubations.
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283272

agement of adhesive SBO. CT is particularly helpful
and should be used as the primary imaging technique
for patients in whom the obstructive symptoms are
associated with specific medical conditions, such as a
history of a previous malignant abdominal tumor,
known inflammatory bowel disease, palpable abdom-
inal mass, or sepsis [56].
Several caveats need to be considered in the
application of CT to SBO. If the plain radiograph
shows probable or definite SBO, oral contrast should
not be used for the CT, because it often does not reach
the site of obstruction by the time of examination. If it
does, the moderately increased intraluminal attenu-
ation created when bowel fluid dilutes the oral con-
trast bolus can nearly match the attenuation of a
contrast-enhanced bowel wall, making it difficult to
assess the bowel wall for thickening. Administration
of oral contrast in the emergent setting also has the
potential to cause delays in performing the CT exam-
ination. The use of water as an intraluminal contrast
agent is preferred in this setting and in patients with
suspected mesenteric ischemia. Positive oral contrast
in this situation often interferes with vascular recon-
struction algorithms. In the emergent setting, sick
patients are able to tolerate water better than water-
soluble contrast. With multidetector row CT, many
small bowel diseases including inflammatory condi-
tions, obstruction, or masses can be diagnosed with
water as enteral contrast in conjunction with intrave-
nous enhancement. In addition, with the use of water,
further diagnostic investigations are not interfered
with because of residual contrast in the bowel.
Compared with barium enteroclysis or CT enter-
oclysis, abdominal CT is faster, more readily avail-
able, noninvasive, less contingent on technical
expertise, and able to provide a more global evalu-
ation of the abdomen and alimentary tract. This last
advantage is of considerable importance, particularly
in the acute setting when intestinal obstruction rep-
resents only one of many possible etiologies in
patients presenting with acute abdominal conditions.
The CT examination should be monitored closely and
additional sections should be obtained through the
transition zone if the cause of obstruction is unclear
on the initial axial sections. Although identification of
the transition zone is usually not difficult in higher
grades of obstruction, the less distended loops found
with low-grade obstruction can be quite confusing to
follow on axial CT images [69]. When CT results are
equivocal in the search for a transition zone, and
closed-loop obstruction has been ruled out, CT enter-
oclysis or barium enteroclysis can often help establish
the diagnosis by providing volume-challenge disten-
tion of the proximal loops.
Box 1. Suggested instructions for suc-tion with the decompression-enterocly-sis catheter
The following instructions are providedas a guide. This peelable ‘‘suction order’’instruction, which is attached to the cath-eter box cover, can be removed andattached to the physician’s orders sheeton the patient’s chart.
1. Connect decompression (suction)port identified by rubber adapter)to low (___) intermittent (___) con-tinuous suction. Modify as needed.
2. Remove cap from sumping port andinject 2 cc of air into the channel assoon as suction is started. Do notrecap the air channel while suctionis being applied. During section thisport will allow air to enter andbubble back up the suction channelalmost continuously. If ‘‘bubbling’’is not observed, proceed to Step 3.Check that all connections are tight.
3. Irrigate decompression port every4 hours with 20 cc of saline andp.r.n. to prevent clogging of thesuction port.
4. Inject the sumping port with 2 cc ofair every 4 hours and p.r.n. Do notaspirate this port. Steps 3 and 4 canbe done at the same time.
5. Any time the decompression port isdisconnected, reapply caps to boththe decompression and the sumpports to prevent fluid leak. RepeatStep 2 each time the decompressiontube is reconnected for suction.
6. If tube is to be anchored for morethan 2 days, apply Bacitracin orNeosporin ointment to nasal cavityonce daily.
7. Do not use balloon channel. Thisport is used only during enteroclysis.
8. Remove long tube at the discretionof the attending physician. Notifyradiology if there is difficulty inremoving tube.
Signed:________________
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 273
CT enteroclysis has emerged as a promising new
method of investigating the small bowel. In this
technique, water-soluble contrast is infused through
an enteroclysis catheter into the proximal small
bowel, followed immediately by CT cross-sectional
imaging of the distended small bowel loops. Multi-
planar reconstructions of the CT data can be
obtained either routinely or on an as-needed basis
for problem solving in difficult cases. Theoretically,
the volume challenge provided by the intubation-
infusion technique of enteroclysis overcomes the
unreliability of CT for diagnosing low-grade obstruc-
tion, whereas the cross-sectional imaging provided
by CT complements the recognized limitations of
conventional enteroclysis in assessing the gut wall
and providing information on extraintestinal causes
of obstruction. In addition to precise three-dimen-
sional localization of small bowel pathology, CT
enteroclysis allows objective determination of the
severity of SBO as has been previously defined
using standard enteroclysis criteria [70]. Initial
reports indicate that the reliability of CT enteroclysis
is equivalent to that of conventional enteroclysis
(sensitivity 88% and specificity 82%) in patients
suspected of having a low-grade partial SBO
[71,72]. Other reports show that it has greater
sensitivity and specificity (89% and 100%, respec-
tively) than CT alone (50% and 94%, respectively) in
patients suspected of having a partial SBO, a differ-
ence that was even greater when a history of abdom-
inal malignancy was known or suspected [72]. CT
enteroclysis is emerging as a promising tool in the
further work-up of SBO. This topic is reviewed in
detail elsewhere in this issue.
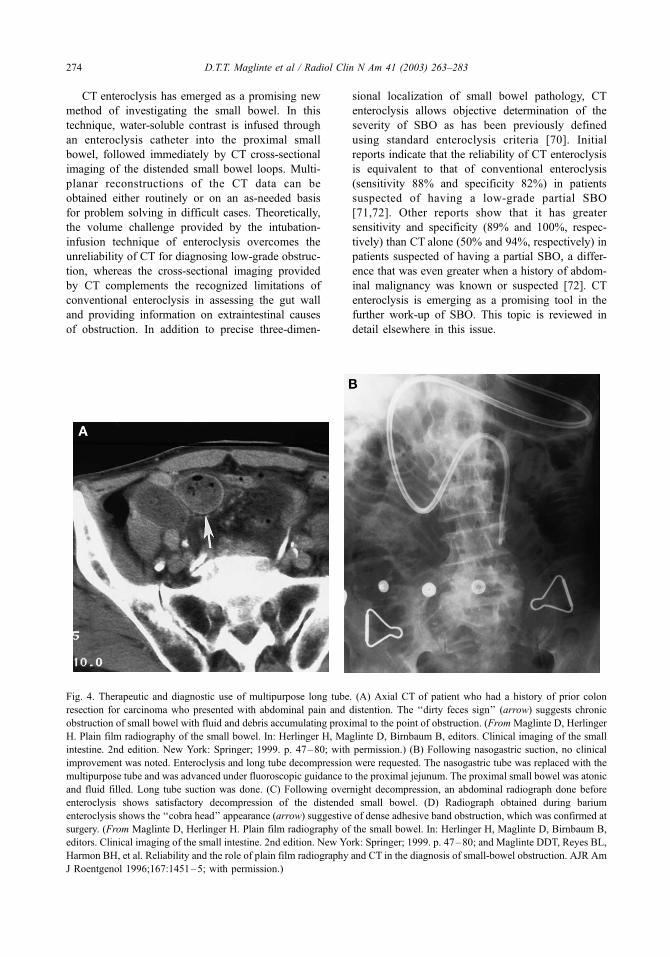
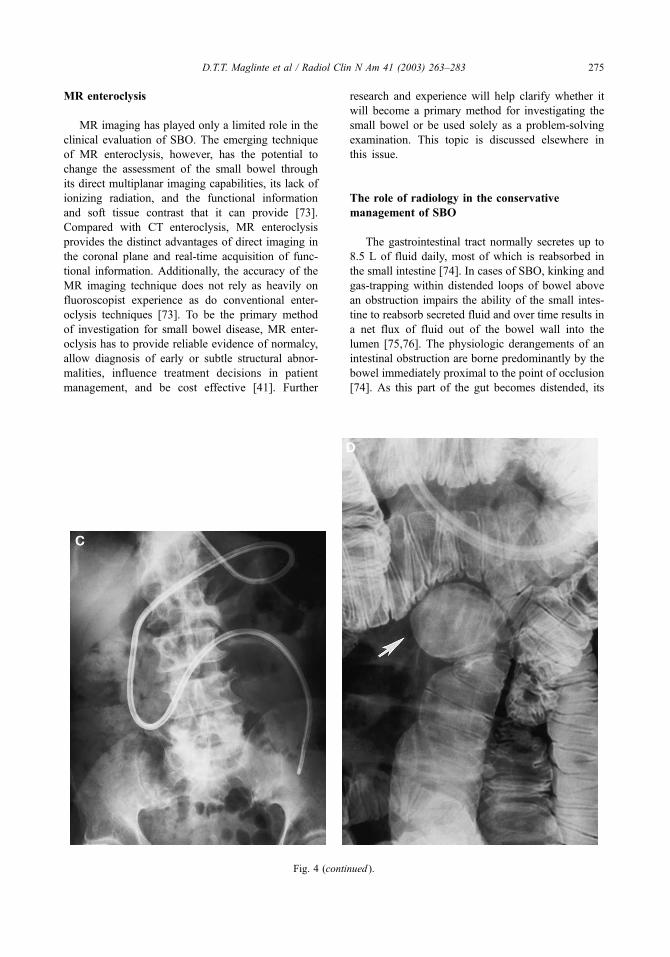
Fig. 4. Therapeutic and diagnostic use of multipurpose long tube. (A) Axial CT of patient who had a history of prior colon
resection for carcinoma who presented with abdominal pain and distention. The ‘‘dirty feces sign’’ (arrow) suggests chronic
obstruction of small bowel with fluid and debris accumulating proximal to the point of obstruction. (FromMaglinte D, Herlinger
H. Plain film radiography of the small bowel. In: Herlinger H, Maglinte D, Birnbaum B, editors. Clinical imaging of the small
intestine. 2nd edition. New York: Springer; 1999. p. 47–80; with permission.) (B) Following nasogastric suction, no clinical
improvement was noted. Enteroclysis and long tube decompression were requested. The nasogastric tube was replaced with the
multipurpose tube and was advanced under fluoroscopic guidance to the proximal jejunum. The proximal small bowel was atonic
and fluid filled. Long tube suction was done. (C) Following overnight decompression, an abdominal radiograph done before
enteroclysis shows satisfactory decompression of the distended small bowel. (D) Radiograph obtained during barium
enteroclysis shows the ‘‘cobra head’’ appearance (arrow) suggestive of dense adhesive band obstruction, which was confirmed at
surgery. (From Maglinte D, Herlinger H. Plain film radiography of the small bowel. In: Herlinger H, Maglinte D, Birnbaum B,
editors. Clinical imaging of the small intestine. 2nd edition. New York: Springer; 1999. p. 47–80; and Maglinte DDT, Reyes BL,
Harmon BH, et al. Reliability and the role of plain film radiography and CT in the diagnosis of small-bowel obstruction. AJR Am
J Roentgenol 1996;167:1451–5; with permission.)
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283274
MR enteroclysis
MR imaging has played only a limited role in the
clinical evaluation of SBO. The emerging technique
of MR enteroclysis, however, has the potential to
change the assessment of the small bowel through
its direct multiplanar imaging capabilities, its lack of
ionizing radiation, and the functional information
and soft tissue contrast that it can provide [73].
Compared with CT enteroclysis, MR enteroclysis
provides the distinct advantages of direct imaging in
the coronal plane and real-time acquisition of func-
tional information. Additionally, the accuracy of the
MR imaging technique does not rely as heavily on
fluoroscopist experience as do conventional enter-
oclysis techniques [73]. To be the primary method
of investigation for small bowel disease, MR enter-
oclysis has to provide reliable evidence of normalcy,
allow diagnosis of early or subtle structural abnor-
malities, influence treatment decisions in patient
management, and be cost effective [41]. Further
research and experience will help clarify whether it
will become a primary method for investigating the
small bowel or be used solely as a problem-solving
examination. This topic is discussed elsewhere in
this issue.
The role of radiology in the conservative
management of SBO
The gastrointestinal tract normally secretes up to
8.5 L of fluid daily, most of which is reabsorbed in
the small intestine [74]. In cases of SBO, kinking and
gas-trapping within distended loops of bowel above
an obstruction impairs the ability of the small intes-
tine to reabsorb secreted fluid and over time results in
a net flux of fluid out of the bowel wall into the
lumen [75,76]. The physiologic derangements of an
intestinal obstruction are borne predominantly by the
bowel immediately proximal to the point of occlusion
[74]. As this part of the gut becomes distended, its
Fig. 4 (continued ).
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 275
increased intraluminal pressure slows capillary blood
flow leading to mesenteric venous congestion putting
this segment of bowel at risk for ischemia, gangrene,
and perforation.
With an intact pylorus, nasogastric tubes cannot
decompress the small bowel until the pressure of
backed-up intestinal fluid and gas is strong enough
to overcome the strength of the pyloric sphincter. The
results of several studies have shown that the efficacy
of decompression is inversely proportional to the
distance between the tube tip and the site of the
blockage, such that advancement of the tube beyond
the pylorus into the small bowel significantly im-
proves decompression efficacy over the standard
gastric positioning [77]. These pathophysiologic prin-
ciples explain why nasointestinal rather than naso-
gastric intubation is considered the optimal method of
decompressing the distended small bowel. An added
advantage to using a long tube is that as soon as the
tube passes the pylorus and begins to decompress the
small bowel, the colicky pain of obstruction is largely
relieved. Because nasogastric tube decompression is
limited to the stomach, a patient’s abdominal pain
persists until either the obstruction is relieved or
effective decompression is achieved, either sponta-
neously or surgically [78].
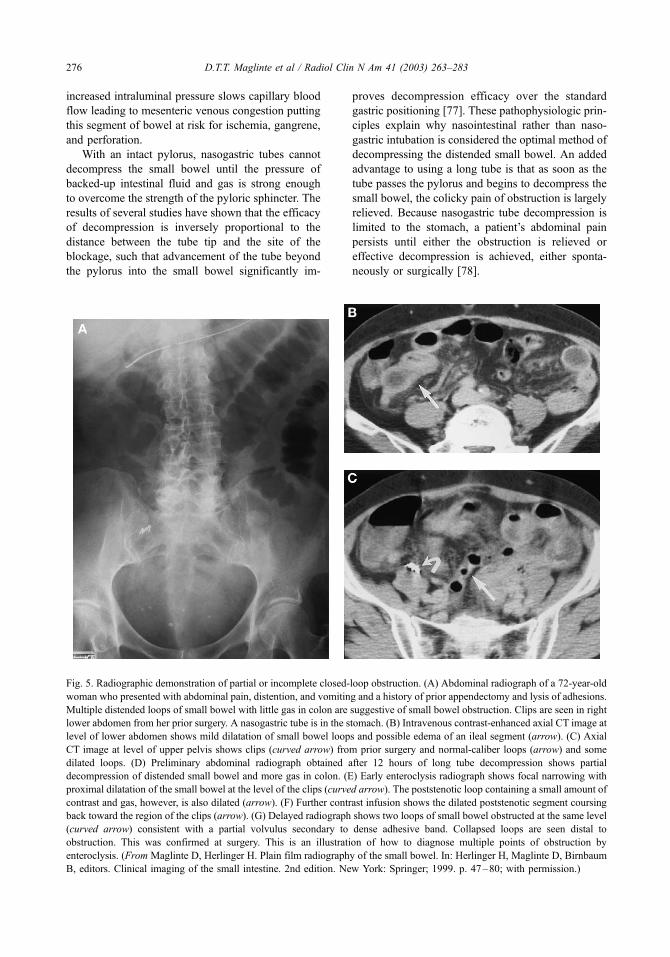
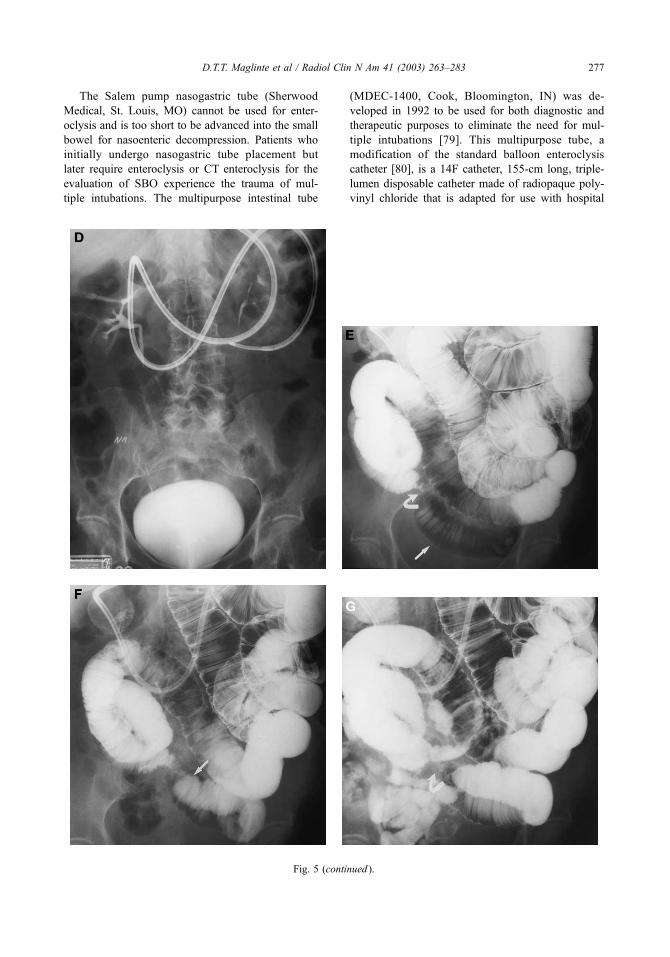
Fig. 5. Radiographic demonstration of partial or incomplete closed-loop obstruction. (A) Abdominal radiograph of a 72-year-old
woman who presented with abdominal pain, distention, and vomiting and a history of prior appendectomy and lysis of adhesions.
Multiple distended loops of small bowel with little gas in colon are suggestive of small bowel obstruction. Clips are seen in right
lower abdomen from her prior surgery. A nasogastric tube is in the stomach. (B) Intravenous contrast-enhanced axial CT image at
level of lower abdomen shows mild dilatation of small bowel loops and possible edema of an ileal segment (arrow). (C) Axial
CT image at level of upper pelvis shows clips (curved arrow) from prior surgery and normal-caliber loops (arrow) and some
dilated loops. (D) Preliminary abdominal radiograph obtained after 12 hours of long tube decompression shows partial
decompression of distended small bowel and more gas in colon. (E) Early enteroclysis radiograph shows focal narrowing with
proximal dilatation of the small bowel at the level of the clips (curved arrow). The poststenotic loop containing a small amount of
contrast and gas, however, is also dilated (arrow). (F) Further contrast infusion shows the dilated poststenotic segment coursing
back toward the region of the clips (arrow). (G) Delayed radiograph shows two loops of small bowel obstructed at the same level
(curved arrow) consistent with a partial volvulus secondary to dense adhesive band. Collapsed loops are seen distal to
obstruction. This was confirmed at surgery. This is an illustration of how to diagnose multiple points of obstruction by
enteroclysis. (From Maglinte D, Herlinger H. Plain film radiography of the small bowel. In: Herlinger H, Maglinte D, Birnbaum
B, editors. Clinical imaging of the small intestine. 2nd edition. New York: Springer; 1999. p. 47–80; with permission.)
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283276
The Salem pump nasogastric tube (Sherwood
Medical, St. Louis, MO) cannot be used for enter-
oclysis and is too short to be advanced into the small
bowel for nasoenteric decompression. Patients who
initially undergo nasogastric tube placement but
later require enteroclysis or CT enteroclysis for the
evaluation of SBO experience the trauma of mul-
tiple intubations. The multipurpose intestinal tube
(MDEC-1400, Cook, Bloomington, IN) was de-
veloped in 1992 to be used for both diagnostic and
therapeutic purposes to eliminate the need for mul-
tiple intubations [79]. This multipurpose tube, a
modification of the standard balloon enteroclysis
catheter [80], is a 14F catheter, 155-cm long, triple-
lumen disposable catheter made of radiopaque poly-
vinyl chloride that is adapted for use with hospital
Fig. 5 (continued ).
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 277
wall suction devices. The important addition of a
sumping mechanism prevents occlusion of the tube’s
side ports from collapse of the bowel wall against the
tube during suctioning, thereby allowing effective
small bowel decompression (Fig. 3) [81]. The multi-
purpose tube kit also includes a preprinted adhesive-
backed order sheet that can be affixed to the orders
page on a patient’s chart (Box 1). This sheet provides
unambiguous instructions to the patient’s caregivers.
In the nonemergent setting, if CT does not answer
all questions relevant to a particular patient’s man-
agement and nasogastric intubation is desired clin-
ically, the multipurpose tube can be positioned in the
stomach for initial gastric decompression. CT enter-
oclysis or barium enteroclysis can then be performed
after advancing the tube, under fluoroscopic guid-
ance, into the jejunum. The long tube can then be
anchored in the proximal jejunum after the study for
further decompression (Fig. 4) [5].
Closed-loop obstruction
Prompt preoperative recognition of closed-loop
obstruction is crucial, because strangulation represents
a dangerous complication that carries a much higher
risk of mortality than simple mechanical SBO. Accu-
rate and early detection of strangulation can expedite
surgery and significantly improve overall patient pro-
gnosis [82,83]. Most closed-loop obstructions result
from entrapment of the small bowel either within an
internal or external hernia. Unless the classic pseudo-
tumor or coffee bean signs are present, plain film
radiography often yields nonspecific and unreliable
results [84]. CT is the imaging modality of choice for
evaluating closed-loop obstruction in the acute setting,
whereas CT or barium enteroclysis serve more com-
plementary roles by establishing the presence of an
incomplete closed-loop obstruction or by helping to
clarify the cause of obstruction (Fig. 5) [37].
The enteroclysis findings of closed-loop obstruc-
tion are similar to those seen in single-band adhesive
obstruction, except that the crossing defect traverses
two adjacent segments of a single loop of bowel [85].
Volvulus is diagnosed if the afferent and efferent
limbs seem to cross or intertwine with twisting of
the folds at the point of obstruction. A separation
between the two obstructed limbs excludes the pres-
ence of volvulus. In patients with moderate to high-
grade obstruction, it may be difficult to exclude
volvulus if the involved limbs appear closely approxi-
mated, tightly compressed, and angulated at the point
of obstruction [85]. It is often impossible to differ-
entiate closed-loop obstructions caused by herniation
through mesenteric defects from those caused by
prolapse of bowel under adhesive bands [40]. If the
constriction is tight, there is usually delayed filling
and delayed emptying of the contrast from the incar-
cerated loop [85].
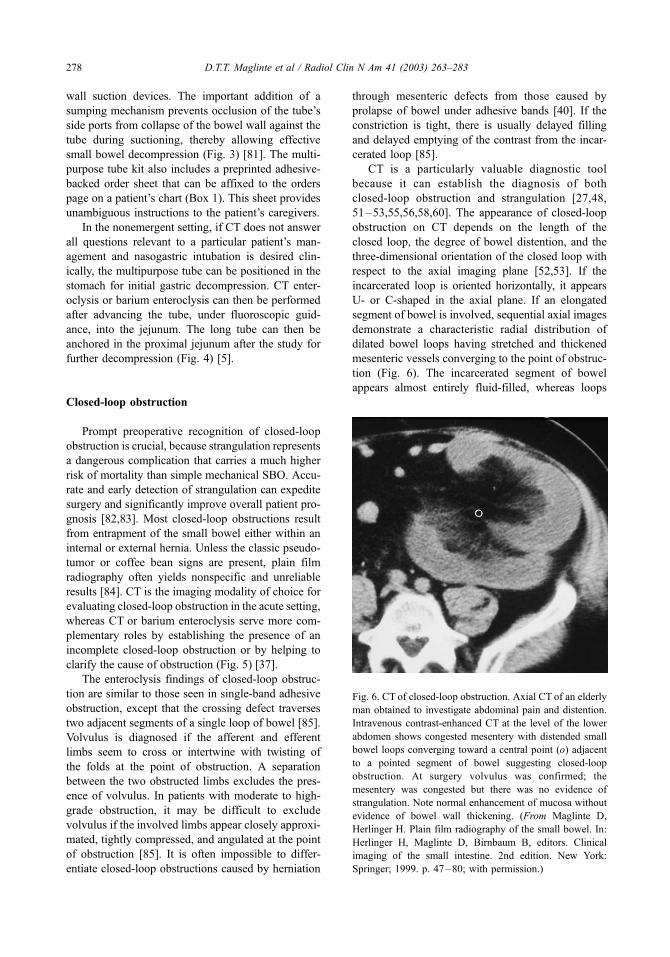
CT is a particularly valuable diagnostic tool
because it can establish the diagnosis of both
closed-loop obstruction and strangulation [27,48,
51–53,55,56,58,60]. The appearance of closed-loop
obstruction on CT depends on the length of the
closed loop, the degree of bowel distention, and the
three-dimensional orientation of the closed loop with
respect to the axial imaging plane [52,53]. If the
incarcerated loop is oriented horizontally, it appears
U- or C-shaped in the axial plane. If an elongated
segment of bowel is involved, sequential axial images
demonstrate a characteristic radial distribution of
dilated bowel loops having stretched and thickened
mesenteric vessels converging to the point of obstruc-
tion (Fig. 6). The incarcerated segment of bowel
appears almost entirely fluid-filled, whereas loops
Fig. 6. CT of closed-loop obstruction. Axial CT of an elderly
man obtained to investigate abdominal pain and distention.
Intravenous contrast-enhanced CT at the level of the lower
abdomen shows congested mesentery with distended small
bowel loops converging toward a central point (o) adjacent
to a pointed segment of bowel suggesting closed-loop
obstruction. At surgery volvulus was confirmed; the
mesentery was congested but there was no evidence of
strangulation. Note normal enhancement of mucosa without
evidence of bowel wall thickening. (From Maglinte D,
Herlinger H. Plain film radiography of the small bowel. In:
Herlinger H, Maglinte D, Birnbaum B, editors. Clinical
imaging of the small intestine. 2nd edition. New York:
Springer; 1999. p. 47–80; with permission.)
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283278
of bowel proximal to the site of obstruction contain
greater amounts of air. Images obtained near the site
of torsion demonstrate progressive, fusiform tapering
of the afferent and efferent limbs manifested as the
beak sign when imaged in longitudinal section. If a
volvulus is present, the whirl sign of a tightly twisted
mesentery may be seen [56]. CT signs of strangula-
tion are related to the appearance of the incarcerated
bowel wall and its mesentery [52,53]. Ischemia is
suggested by the presence of circumferential wall
thickening, increased mural attenuation, and the tar-
get or double halo sign seen on the intravenous
contrast-enhanced examination. In the setting of
examinations without intravenous contrast, increased
bowel wall attenuation is suggestive of ischemia.
Pneumatosis intestinalis may be seen with advanced
ischemia and infarction. Mesenteric congestion
and hemorrhage are important findings whose pres-
ence increases the specificity of the CT diagnosis
of strangulation.
Optimizing the imaging investigation of SBO
Open communication among radiologists, primary
care physicians, and surgeons is essential in the work-
up and management of SBO [86]. The selection of
imaging is based on knowledge of the patient’s
history, physical examination, laboratory results,
and abdominal plain film findings. The dilemma that
radiologists face is not the use of one technique over
the other, but the decision of which examination to
use first in the context of the clinical presentation and
abdominal plain film findings [56,85].
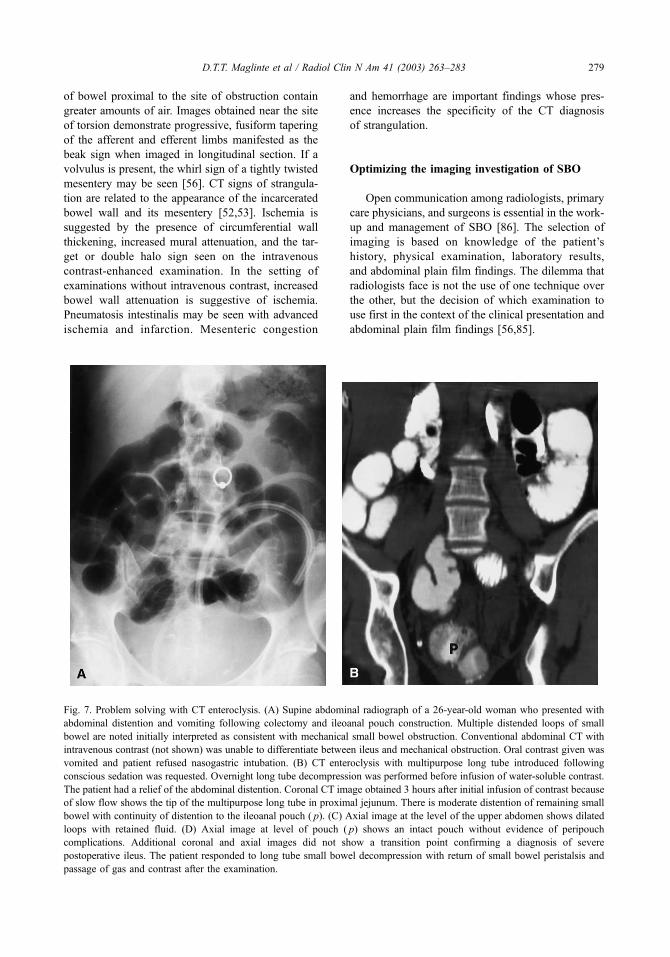
Fig. 7. Problem solving with CT enteroclysis. (A) Supine abdominal radiograph of a 26-year-old woman who presented with
abdominal distention and vomiting following colectomy and ileoanal pouch construction. Multiple distended loops of small
bowel are noted initially interpreted as consistent with mechanical small bowel obstruction. Conventional abdominal CT with
intravenous contrast (not shown) was unable to differentiate between ileus and mechanical obstruction. Oral contrast given was
vomited and patient refused nasogastric intubation. (B) CT enteroclysis with multipurpose long tube introduced following
conscious sedation was requested. Overnight long tube decompression was performed before infusion of water-soluble contrast.
The patient had a relief of the abdominal distention. Coronal CT image obtained 3 hours after initial infusion of contrast because
of slow flow shows the tip of the multipurpose long tube in proximal jejunum. There is moderate distention of remaining small
bowel with continuity of distention to the ileoanal pouch ( p). (C) Axial image at the level of the upper abdomen shows dilated
loops with retained fluid. (D) Axial image at level of pouch ( p) shows an intact pouch without evidence of peripouch
complications. Additional coronal and axial images did not show a transition point confirming a diagnosis of severe
postoperative ileus. The patient responded to long tube small bowel decompression with return of small bowel peristalsis and
passage of gas and contrast after the examination.
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 279

Definitive SBO on plain film radiography con-
firms the clinical diagnosis and opens the door for a
decision on whether to perform surgery or use a trial
of conservative nonoperative management. Factors
that favor early surgical exploration include no prior
history of abdominal surgery; clinical signs of bowel
compromise; incarcerated hernia; or the presence of a
complete SBO (obstipation). Factors that favor initial
conservative management include the presence of a
partial SBO; history of resected abdominal tumor;
prior radiation therapy; history of inflammatory
bowel disease; and early ( < 6 weeks) postoperative
obstruction (see Fig. 1M, N). When initial conserva-
tive management is entertained, CT examination is
helpful in evaluating the presence and extent of
neoplastic or inflammatory disease and in excluding
a strangulated obstruction. Postsurgical patients pre-
senting early after operation with abdominal disten-
tion and no signs of bowel compromise (tachycardia,
leukocytosis, localized tenderness, or fever) are
treated conservatively for several days, with CT
advised only if the clinical findings and abdominal
plain films do not improve, or if signs of sepsis or
bowel compromise develop. CT enteroclysis with
positive enteral contrast is a good problem-solving
tool and is easier to perform than barium enteroclysis
particularly in the postoperative patient or those who
are clinically ill (Fig. 7). CT enteroclysis should be
used after the conventional CT study only if addi-
tional management questions are left unanswered
[29,53]. In departments where CT enteroclysis is
not practical, barium enteroclysis is the preferred
investigation [5].
If the abdominal plain film shows colonic disten-
tion in addition to small bowel dilatation, a CT or
contrast enema should be performed. In this clinical
setting, CT is preferred in elderly or infirm patients,
patients with a clinical suspicion of abscess or diver-
ticulitis, and in patients with a history of previously
resected colon carcinoma. CT is also necessary in the
acute setting in patients with poor anal sphincter tone
(see Fig. 2) [82]. Where CT is not readily available,
the contrast enema is the method of choice.
Discordance between the clinical presentation and
plain film findings often requires additional radiologic
imaging. In patients with acute abdominal symptoms
who have normal or abnormal but nonspecific bowel
gas pattern on abdominal plain films, CT is recom-
mended (see Fig. 1J, K). CT is not only reliable in
showing many of the acute abdominal conditions that
Fig. 7 (continued ).
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283280
can mimic SBO, but it also has a high sensitivity for
high-grade or complete SBO and can reveal closed-
loop and strangulating obstruction. When the CT
examination is not diagnostic, enteroclysis (CT,
barium, or MR) or a fluoroscopy-based barium small
bowel study can be performed as a complementary
examination. CT enteroclysis is the best initial
imaging technique in patients with a history of lap-
arotomy who complain of mild intermittent abdominal
pain and have few physical findings and a normal or
abnormal but nonspecific abdominal plain film. Low-
grade intermittent obstructions and intraluminal
tumors can be detected and evaluated better using this
technique. Barium enteroclysis can be performed later
if the CT enteroclysis does not provide enough
mucosal detail to detect small ulcerations or mild
inflammatory changes. MR enteroclysis can also give
additional information, particularly in patients with
inflammatory bowel disease.
The specific indications for diagnostic imaging
procedures are receiving intense scrutiny because of
the need to control health care costs. Radiologic
services are now being evaluated by criteria that
assess whether the use of a particular diagnostic
method influences clinical management, improves
patient outcome, or lowers medical costs. [83,84].
Unfortunately, erroneous application of imaging stud-
ies is frequent in clinical practice. Recent improve-
ments in CT and enteroclysis technology have
changed the approach to the evaluation of patients
suspected of having SBO [86]. These modalities are
complementary and serve as essential adjuncts to
abdominal plain film radiography in the diagnosis
and management of SBO.
References
[1] Mucha Jr. P. Small intestinal obstruction. Surg Clin
North Am 1987;67:597–620.
[2] Otamiri T, Sjodhal R, Ihse I. Intestinal obstruction
with strangulation of the small-bowel. Acta Chir Scand
1987;153:307–10.
[3] Suh RS, Maglinte DDT, Lavonas EJ, et al. Emergency
abdominal radiography: discrepancies of preliminary
and final interpretation and management relevance.
Emerg Radiol 1995;2:1–4.
[4] Herlinger H, Maglinte DDT. Small bowel obstruction.
In: Herlinger H, Maglinte DDT, editors. Clinical radi-
ology of the small intestine. Philadelphia: WB Saun-
ders; 1989. p. 479–507.
[5] Maglinte DDT, Balthazar EJ, Kelvin FM, et al. The
role of radiology in the diagnosis of small bowel ob-
struction. AJR Am J Roentgenol 1997;168:1171–80.
[6] Welch JP. General consideration and mortality in bow-
el obstruction. In: Welch JP, editor. Bowel obstruction:
differential diagnosis and clinical management. Phila-
delphia: WB Saunders; 1990. p. 59–95.
[7] Shrake PD, Rex DK, Lappas JC, et al. Radiographic
evaluation of suspected small-bowel obstruction. Am J
Gastroenterol 1991;86:175–8.
[8] Miller G, Boman J, Shrier I, et al. Etiology of small
bowel obstruction. Am J Surg 2000;180:33–6.
[9] Bizer LS, Leibling RW, Delany HM, et al. Small-
bowel obstruction: the role of nonoperative treat-
ment in simple intestinal obstruction and predictive
criteria for strangulation obstruction. Surgery 1981;
89:407–13.
[10] Brolin RE, Krasna MJ, Mast BA. Use of tubes and
radiographs in the management of small –bowel ob-
struction. Ann Surg 1987;206:126–33.
[11] Seror D, Feigin E, Szold A, et al. How conservatively
can postoperative small-bowel obstruction be treated?
Am J Surg 1993;165:121–6.
[12] Wolfson PJ, Bauer JJ, Gelernt IM, et al. Use of the long
tube in the management of patients with small-intesti-
nal obstruction due to adhesions. Arch Surg 1985;120:
1001–6.
[13] Becker WF. Acute adhesive ileus: a study of 412 cases
with particular reference to the abuse of tube decom-
pression in treatment. Surg Gynecol Obstet 1952;95:
472–6.
[14] Hofstetter SR. Acute adhesive obstruction of the small
intestine. Surg Gynecol Obstet 1981;152:141–4.
[15] Sarr MG, Bulkey GB, Zuidema GD. Preoperative rec-
ognition of intestinal strangulation obstruction: pro-
spective evaluation of diagnostic capability. Am J
Surg 1983;145:176–82.
[16] Snyder EN, McCranie D. Closed-loop obstruction of
the small-bowel. Am J Surg 1965;111:398–402.
[17] Barnett WO, Petro AB, Williamson JW. A current ap-
praisal of problems with gangrenous bowel. Ann Surg
1976;183:653–9.
[18] Laws HL, Aldrete JS. Small-bowel obstruction: a re-
view of 465 cases. South Med J 1976;69:733–4.
[19] Lefall LD, Syphax B. Clinical aids in strangulating
intestinal obstruction. Am J Surg 1970;120:756–9.
[20] Nadrowski LF. Pathophysiology and current treatments
of intestinal obstruction. Rev Surg 1974;31:381–407.
[21] Silen W, Hein MF, Goldman L. Strangulation obstruc-
tion of the small intestine. Arch Surg 1962;85:137–45.
[22] Davis SE, Sperling L. Obstruction of the small intes-
tine. Arch Surg 1969;99:424–6.
[23] Frazee RC, Mucha Jr. P, Farnell MB, et al. Volvulus of
the small intestine. Ann Surg 1988;208:565–8.
[24] Shatila AH, Chamberlain BE, Webb WR. Current sta-
tus of diagnosis and management of strangulation ob-
struction of the small-bowel. Am J Surg 1976;132:
299–303.
[25] Peetz Jr. DJ, Gamelli RL, Pilcher DB. Intestinal intu-
bation in acute mechanical small-bowel obstruction.
Arch Surg 1982;117:334–6.
[26] Snyder CL, Ferrell KL, Goodale RL, et al. Nonoper-
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 281
ative management of small-bowel obstruction with en-
doscopic long intestinal tube placement. Am Surg
1990;56:587–92.
[27] Taourel PG, Fabre VM, Pradel JA, et al. Value of CT in
diagnosis and management of patients with suspected
acute small-bowel obstruction. AJR Am J Roentgenol
1995;165:1187–92.
[28] Turner DM, Croom III RD. Acute adhesive obstruction
of the small intestine. Am Surg 1983;49:126–30.
[29] Maglinte DDT, Reyes BL, Harmon BH, et al. Reliabil-
ity and the role of plain film radiography and CT in the
diagnosis of small-bowel obstruction. AJR Am J
Roentgenol 1996;167:1451–5.
[30] Maglinte DDT, Herlinger H. Plain film radiography. In:
Herlinger H, Maglinte DDT, editors. Clinical radiology
of the small intestine. Philadelphia: WB Saunders;
1989. p. 54–65.
[31] Marcus JB, Somers S, Franic SE, et al. Interobserver
variation in the interpretation of abdominal radio-
graphs. Radiology 1989;171:69–71.
[32] Patel NH, Lauber PR. The meaning of a nonspecific
abdominal gas pattern. Acad Radiol 1995;2:667–9.
[33] Maglinte DDT. Nonspecific abdominal gas pattern: an
interpretation whose time is gone [guest editorial].
Emerg Radiol 1996;3:93–5.
[34] Lappas JC, Reyes BL, Maglinte DDT. Abdominal ra-
diography findings in small-bowel obstruction: rele-
vance to triage for additional diagnostic imaging.
AJR Am J Roentgenol 2001;176:167–74.
[35] Frimann-Dahl J. The administration of barium only in
acute obstruction: advantages and results. Acta Radiol
1954;42:285–95.
[36] Nelson SW, Christoforides AJ. The use of barium sul-
fate suspensions in the study of suspected mechanical
obstruction of the small intestine. AJR Am J Roent-
genol 1967;101:367–78.
[37] Blackmon S, Lucius C, Wilson JP, et al. The use of
water-soluble contrast in evaluating clinically equiv-
ocal small bowel obstruction. Am Surg 2000;66:
238–42.
[38] Chen SC, Lin FY, Yu SC, et al. Water-soluble con-
trast study predicts the need for early surgery in ad-
hesive small bowel obstruction. Br J Surg 1998;85:
1692–4.
[39] ChungCC,MengWC,Yu SC, et al. A prospective study
on the use of water-soluble contrast follow-through ra-
diology in the management of small bowel obstruction.
ANZ Journal of Surgery 1996;66:598–601.
[40] Feigin E, Seror D, Szold A, et al. Water-soluble
contrast material has no therapeutic effect on post-
operative small-bowel obstruction: results of a pro-
spective, randomized clinical trial. Am J Surg 1996;
171:227–9.
[41] Maglinte DDT, Kelvin FM, O’Connor K, et al. Re-
view: current status of small bowel radiography. Ab-
dom Imaging 1996;21:247–57.
[42] Maglinte DDT, Lappas JC, Kelvin FM, et al. Small
bowel radiography: how, when, and why? Radiology
1987;163:297–305.
[43] Taverne PP, van der Jagt EJ. Small bowel radiography:
a prospective comparative study of three techniques in
200 patients. Fortschr Rontgenstr 1985;143:293–7.
[44] Herlinger H, Rubesin SE. Obstruction. In: Gore RM,
Levine MS, Laufer I, editors. Textbook of gastrointes-
tinal radiology. Philadelphia: WB Saunders; 1993.
p. 931–66.
[45] Maglinte DDT, Gage SN, Harmon BH, et al. Obstruc-
tion of the small intestine: accuracy and role of CT in
diagnosis. Radiology 1993;186:61–4.
[46] Caroline DF, Herlinger H, Laufer I, et al. Small-bowel
enema in the diagnosis of adhesive obstructions. AJR
Am J Roentgenol 1984;143:1133–9.
[47] Maglinte DDT, Peterson LA, Vahey TN, et al. Enter-
oclysis in partial small-bowel obstruction. Am J Surg
1984;147:325–9.
[48] Maglinte DDT, Burney BT, Miller RE. Lesions missed
on small-bowel follow-through: analysis and recom-
mendations. Radiology 1982;144:737–9.
[49] Maglinte DDT, Miller RE. Intubation infusion method:
reliability in diagnosis of mechanical partial small-bow-
el obstruction. Mt Sinai J Med 1984;51:372–7.
[50] Nolan DJ, Marks CJ. The barium infusion in small
intestinal obstruction. Clin Radiol 1981;32:651–5.
[51] Sellink JL, Miller RE. Ileus-fusion-bands-volvulus-in-
tussusceptions-incisional hernia. In: Sellink JL, Miller
RE, editors. Radiology of the small-bowel. Hingham
(MA): Nijhoff; 1982. p. 413–48.
[52] Dehn TCB, Nolan DJ. Enteroclysis in the diagnosis of
intestinal obstruction in the early postoperative period.
Gastrointest Radiol 1989;14:15–21.
[53] Maglinte DDT, Herlinger H, Nolan DJ. Radiologic
features of closed-loop obstruction: analysis of 25 con-
firmed cases. Radiology 1991;179:383–7.
[54] Fukuya T, Hawes DR, Lu CC, et al. CT diagnosis of
small-bowel obstruction: efficacy in 60 patients. AJR
Am J Roentgenol 1992;158:765–9.
[55] Megibow AJ, Balthazar EJ, Cho KC, et al. Bowel
obstruction: evaluation with CT. Radiology 1991;
180:313–8.
[56] Balthazar EJ. CT of small-bowel obstruction. AJR Am
J Roentgenol 1994;162:255–61.
[57] Balthazar EJ, Bauman JS, Megibow AJ. CT diagnosis
of closed-loop obstruction. J Comput Assist Tomogr
1985;9:953–5.
[58] Balthazar EJ, Birnbaum BA, Megibow AJ, et al.
Closed-loop and strangulating intestinal obstruction:
CT signs. Radiology 1992;185:769–75.
[59] Cho KC, Hoffman-Tretin JC, Alterman DD. Closed-
loop obstruction of the small-bowel: CT and sono-
graphic appearance. J Comput Assist Tomogr 1989;
13:256–8.
[60] Fisher JK. Computed tomographic diagnosis of volvu-
lus in intestinal malrotation. Radiology 1981;140:
145–6.
[61] Frager D, Baer JW, Medwid SW. Detection of intesti-
nal ischemia in patients with acute small-bowel ob-
struction due to adhesions or hernia: efficacy of CT.
AJR Am J Roentgenol 1996;166:67–71.
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283282

[62] Ha HK, Park CH, Kim SK, et al. CT analysis of intes-
tinal obstruction due to adhesions: early detection of
strangulation. J Comput Assist Tomogr 1993;17:
386–9.
[63] Jaramillo D, Raval B. CT diagnosis of primary small-
bowel volvulus. AJR Am J Roentgenol 1986;147:
941–2.
[64] Shaff MI, Himmelfarb E, Sacks GA, et al. The whirl
sign: a CT finding in volvulus of the large bowel.
J Comput Assist Tomogr 1985;9:410.
[65] Ha HK, Rha SE, Kim JH, et al. CT diagnosis of stran-
gulation in patients with small-bowel obstruction: cur-
rent status and future direction. Emerg Radiol 2000;7:
47–55.
[66] Ha HK. CT in the early detection of strangulation in
intestinal obstruction. Semin Ultrasound CT MR 1995;
16:141–50.
[67] Frager D, Medwid SW, Baer JW, et al. CT of small-
bowel obstruction: value in establishing the diagnosis
and determining the degree and cause. AJR Am J
Roentgenol 1994;162:37–41.
[68] Gazelle GS, Goldberg MA, Wittenberg J, et al. Effi-
cacy of CT in distinguishing small-bowel obstruction
from other causes of small-bowel dilatation. AJR Am J
Roentgenol 1994;162:43–7.
[69] Maglinte DDT, Reyes BL. Computed tomographic di-
agnosis of partial small-bowel secondary to anterior
peritoneal adhesions: relevance to laparoscopic chole-
cystectomy. Emerg Radiol 1996;3:84–6.
[70] Bender GN, Maglinte DDT, Kloppel VR, et al. CT
enteroclysis: a superfluous diagnostic procedure or val-
uable when investigating small-bowel disease? AJR
Am J Roentgenol 1999;172:373–8.
[71] Bender GN, Timmons JH, Williard WC, et al. Com-
puted tomographic enteroclysis: one methodology. In-
vest Radiol 1996;31:43–9.
[72] Walsh DW, Bender GN, Timmons JH. Comparison of
computed tomography-enteroclysis and traditional
computed tomography in the setting of suspected partial
small bowel obstruction. Emerg Radiol 1998;5:29–37.
[73] Maglinte DDT, Siegelman ES, Kelvin FM. MR enter-
oclysis: the future of small-bowel imaging? [editorial].
Radiology 2000;215:639–41.
[74] Adams MB, Condon RE. Fluid and electrolyte therapy.
In: Condon RE, Nyhus LM, editors. Manual of surgical
therapeutics. 5th edition. Boston: Little, Brown; 1981.
p. 171–202.
[75] Paine JR. The hydro-dynamics of the relief of disten-
tion in the gastrointestinal tract by suction applied to
inlaying catheters. Arch Surg 1936;33:995–1020.
[76] Sheilds R. The absorption and secretion of fluids and
electrolytes in the obstructed bowel. Br J Surg
1965;52:774–6.
[77] Cantor MO. Intestinal decompression tubes in use to-
day. In: Cantor MO, editor. Intestinal intubation.
Springfield (IL): Thomas; 1949. p. 100–15.
[78] Gowen GF, Aufses A. Short versus long tubes [letter].
Am J Surg 1996;171:543–4.
[79] Maglinte DDT, Kelvin FM, Micon LT, et al. Nasoin-
testinal tube for decompression or enteroclysis: expe-
rience with 150 patients. Abdom Imaging 1994;19:
108–12.
[80] Maglinte DDT, Stevens LH, Hall RC, et al. Dual-pur-
pose tube for enteroclysis and nasogastric-nasoenteric
decompression. Radiology 1992;185:281–2.
[81] Maglinte DDT, Kelvin FM, Rowe MG, et al. Small-
bowel obstruction: optimizing radiologic investigation
and nonsurgical management. Radiology 2001;218:
39–46.
[82] Chapman AH, McNamara M, Porter G. The acute con-
trast enema in suspected large bowel obstruction: value
and technique. Clin Radiol 1992;46:273–8.
[83] Royal HD. Technology assessment: scientific chal-
lenges. AJR Am J Roentgenol 1994;163:503–7.
[84] Hillman BJ. New imaging technology and cost con-
tainment. AJR Am J Roentgenol 1994;162:503–6.
[85] Maglinte DDT, Herlinger H, Turner WW, et al. Radio-
logic management of small bowel obstruction: a prac-
tical approach. Emerg Radiol 1994;1:138–49.
[86] Bender GN, Maglinte DDT. Small bowel obstruction:
the need for greater radiologist involvement [editorial].
Emerg Radiol 1997;4:337–9.
D.T.T. Maglinte et al / Radiol Clin N Am 41 (2003) 263–283 283