Jurnal Annisa - Bowel Obstruction

of 5
-
Upload
annisa-febrieza-zulkarnaen -
Category
Documents
-
view
222 -
download
0
Transcript of Jurnal Annisa - Bowel Obstruction
-
8/12/2019 Jurnal Annisa - Bowel Obstruction
1/5
29 1
0361-8 03 X /93/161 2 -0291 A m erica n R oen tge n R a ySocie ty
W e searched the m edical records of 1 770 patients for those w ith proved m echanicadynam ic bow el obstruction. T he search included all patients hospitalized at our instit
D iagnos is o f B ow el O bs truc tionon P la in A bdom ina l R ad iographs :Sign ificance of A ir-F lu id Levels a t
D iffe ren t H eigh ts in the Sam e Loop ofB o w e l
C urtis L.Harlow1Robert L. G . Stea rs1
Bernard E . Zeligm an1Philip G . A rc he r2 3
R ece ive d Ja nua ry 2 6, 1 99 3; a cce pte d a fte r re vi-sio n M a rch 16, 199 3.
1 D e pa rtm en t of R ad iology, B ox A0 3 0, U n iv e rs i-
ty of C olorado S chool of M edicine, D enver, C O80262. A ddress correspondences to C . L H arlow .
2D epartm e nt o f P re ve nta tive M e dic ine , U n ive r-sity of C olorado S chool of M edicine, D enver, C O80262.
3 D ep ar tm e nt o f B io m et ric s,U nivers ity o f C ob-ra do Schoo l of M ed icine , D enver, C O 802 62 .
O B JE C T IV E . D ifferen tia l air-flu id levels aretw o d istin ct air-flu id in terfaces o n h o ri-zo n tal-b eam ab d o m in al rad io g rap h s th at are at d ifferen t h eig h ts b u t w ith in th e sam e
lo o p o f b o w el. D ifferen tial air-flu id levels h ave b een co n sid ered b y m an y to b e stro n
evid en ce o f m ech anical b o w el o b stru ctio n , b u t o th ers have fo u n d th is s ig n u n reliab lefo r d ifferen tiatin g m ech an ical fro m adyn am ic o b stru ctio n s . N eith er op in io n is su pported b y evid ence from larg e series o f p atien ts . A ccord ing ly , w e d eterm ined th e efcacy of d ifferentia l a ir-flu id levels fo r d is ting uish ing m ech anical fro m ad ynamb o w el o b st ru c ti on .
M A TER IA LS A N D M ETH O D S. W e Iden tified p atien ts w ho had a to ta l of 62 ep iso f p ro ved m ech an ical b o w el o b s tructio n an d 38 ep Iso d es o f ad yn am ic o b s tru ctio n
th ro u g h a co m pu ter search o f m ed ical reco rd s an d rad io grap hic files . O n h o rizo n tal-b eam ab d o m in al rad b o graph s o f th ese p atien ts , th e p resen ce an d h eig h t o f in testin al
d ifferen tia l air-flu id levels w ere d eterm in ed b y th e co n sen su s o ftw o experiencedrad io lo gis ts . Th ese d ata w ere then sta tis tica lly analyzed to determ in e the u sefu lnesso f d ifferen tia l air-flu id levels fo r d is tin g u ish in g b etw een m ech an ical an d ad yn am ic
b o we l o b st ru c ti on s.R ESU LTS. Pla in film s sh ow ed differen tia l a ir-flu id levels in 32(5 2 %) o f th e 62 ep l-
sodes o f m ech anical ob stru ctio ns com pared w ith 11 (29 ) of th e 38 ad yn am ic ob stru
tio n s , g iv in g a sen sftivfty fo r m ech an ical o b stru ctio n o f 0 .52 an d aspecificity o f 0 .71 .A s the m inim um signfficant height of diffe rential air-fluid levels increased , spin creased an d sen s itivity d ecreased . T h e p o s itive p red ictive valu e also In creased ad ifferentia l a ir-flu id level h eigh ts in creased , reachin g a level o f 086 o r greater a t 20 m
C O N CLU SIO N . The presen ce of d ifferentia l a ir-flu id levels is an insen sItive m eto f determ in ing if a b o w el o b s tru ctio n is m ech an ical, b ecau se o n ly a sm all p ro p o rtio n
o f m ech an ical o b s tructio n s h ave d ifferen tia l air-flu id levels . In o u r p o p u latio np atien ts , h o w ever, a d ifferen tial air-flu id level o f 20 m m or g reater w as m o d eratelysug g estive that a bo w el ob stru ctio n w as m echan ical in nature .
AJ R 1993;161:291-295
Differentia l a ir-flu id levels can be defined as tw o dis tinct a ir-flu id in terfaces
horizonta l-beam abdom inal radiograph that are at d ifferent heights but with in
sam e loop of bow el. Traditiona lly , such fluid levels have been cons ideredevidence of m echanical obstruction [1], a lthough m ost authorities now dis
th is notion [2-5]. This finding has been known for decades, but little scientificdence supports beliefs concerning its s ignificance . Accordingly, w e studiedpla in abdom inal radiographs of patien ts w ho had proved m echanical bobstruction and adynam ic obstruction to determ ine the efficacy of the findin
dis tinguishing between m echanical and adynam ic obstructions.
M ateria ls and M eth od s
-
8/12/2019 Jurnal Annisa - Bowel Obstruction
2/5
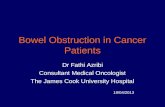
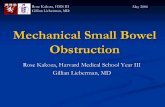
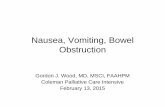
Fig. 2.-85 -ye ar-old w om a n w ith pne um onia and a dyna m ic obs truc tion prove d at a u-to psy. A bd om in al radio grap h o btain ed w ith p atien t in lateral d ecu bitu s p ositio n sh ow sI 7 -m m stra ig ht a rro ws an d 19 -m m c uried arrow s d iffe re ntia l a ir-flu id le ve ls .
292 H AR LO W ET A L. R :161, A ugus t 1993
betw een January 1, 1988, and January 1, 1990, with the diagnosisof bow el obs truction . W e also searched files of patients w ho had
pla in abdom inal nadiognaphs after cholecystectom y and cesareansectio n be cause these p roced ure s often re su lt in a dyna m icbow e l
obstruction . T he author not involved in in terpretation of radiographspreview ed hospita l charts. P atien ts w ere included in the study only if
they w ere m ore than 1 2 years old, m edical records w ere available,
bow el dila ta tion appeared on abdom inal nadiographs, a horizonta l-beam abdom inal radiograph show ed air-flu id levels, and diagnosisw as m ade on the bas is of surgery, contrast exam inations of bow el,autopsy, or reasonable clin ical d iagnosis .
S everal patien ts had m ultip le episodes of m echanical obstructionor adynam ic obstruction , on both , dunng the study period , and eachof these situations w as categorized as a different episode on thebasis of c lin ica l inform ation . F or exam ple , a sm all-bow el obstructioncaused by adhesions occurring m onths after an obstructing abdom i-nal m ass w as rem oved w as considered an independent episode.
T w o radiologis ts w ho had no know ledge of the inform ation in
patients m edical records together review ed the radiographs . F in
ings on film s w ere scored by consensus. W hen m ore than one filw a s a va ila ble for a given episode, the results w ere pooled as thoughthey w ere a s ingle exam ination. F ilm s w ere evaluated for the pre
ence and heights of differential air-flu id levels.
D ifferentia l air-fluid levels w ere m easured in 1 -m m increm ents.flu id levels w ere not scored as differential unless they w ere unequivo
cabby with in a single loop of bow el (Figs. 1-4). W hen m ore than onfenentiab air-fluid bevel w as identified , the greates t height w as usedsta tis tic al a na lysis. To s tu dy th e e ffe ct th at d iffe re ntia l a ir-fluid le vgreater heights w ould have on predicting m echanical obstruction ,threshold of a diagnostic d ifferential air-flu id level w as variably defiby increasing the m inim um height requirem ent in 5-m m increm entT hese data w ere analyzed for sensitivity, specificity, and positivenegative predictive values for m echanical obstruction , and a receioperator-characteris tic (R O C) curve w as constructed [6 , 7].
Fig. 1 .-3 9-ye ar-o ld w om anwith m ec ha nic al s ma ll-bow el obstruction pro ve d by con tra st e xa m ination o fsm all b o w el. A h ys terecto m y h ad b eenperformedma n y y ea rs ea rlie r. P laina bd om ina l ra diograph ob -tam ed w ith pa tie nt up right show s 26-m m diffe ren tia la ir -f lu id l ev el a rrows .
Fig. 3 .-42 .yea r-o ld m a n w ith re -m ote h is tory o f abdom ina l s urge rya nd m e chan ica l bow el obs truc tionproved s urgic a lly . A bdom inal radio-g raph obta ine d w ith pa tie nt up righ ts ho ws 5 -m m d iffere ntia l a ir-flu id le ve l
a r r o w s .
Fig . 4.-47-ye ar-old w om a n w ithre -m o te h is tory o f abdom inal s urgeryand m ec ha nica l bow el obs truc tionproved su rgica lly . P la in abdom ina l ra -
diog raph ob ta ined w ith patient up rights ho ws 13 -m m d ifferen tia l air-flu id 1 ev -el ar rows) .
-
8/12/2019 Jurnal Annisa - Bowel Obstruction
3/5
FrC
qUC
ncy
1-5 5-10 10-15 15-20 20-25 25-30 X l-35 35-40 40+
O A R . Height (m m )
I - S.nsd y
.-.-. PR y
. NP y
p
I I O 2 5 35 40
D AF L H eig ht (mm l
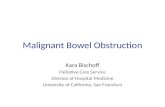
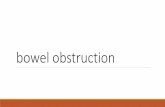
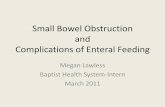
F ig . 6 .-S tatistical an alys is as m in im um th resh old h eigh t o f d bfterentia l air-flu id lev el (D AF L) In crea se s. P PV= positive p re dictiv e v alu e, N PV= ne ga tive p re dictive va lu e.
A JR :1 61 , A ug us t1993 AIR-FLU ID LEVELS IN BO W EL O BSTR U CTIO N 29 3
Results
O f 100 episodes am ong 75 patients m eeting the study cm i-
tenia, 62 w ere m echanical obstructions and 38 w ere adynam ic
obstructions . Am ong all episodes, 42% had diagnostic proofby surgery , contras t exam inations of bow el, or autopsy (ana-
tom ic proof), and 58% had reasonable proof on clin ica lgrounds (Table 1). As expected, m ore m echanical obstruc-tions than adynam ic obstructions had anatom ic proof (60% vs
13% ) because m ost adynam ic obstructions do not requiresurgica l in tervention . W ith the m inim um significant height for a
differential air-fluid level set at anything grea ter than 0 m m, 32of the 62 m echanical obstructions had differentia l a im -flu id 1ev-
els and 11 of the 38 adynam ic obstructions had differ-entia laim -flu id levels (Table 2). As the m inim um significant height of
differentia l a ir-fluid levels w as increased , the frequency andpercentage of m echanical obstructions and adynam ic
obstructions w ith differentia l a ir-fluid levels declined (Table 2and Fig . 5). S tatistical ana lysis(Table 3 and Fig. 6) revealedtha t specificity for m echanical obstruction increased and sen-
sitivity decreased as the threshold height defin ing a differen-tia l a im -flu id level w as increased . Positive predic tive value also
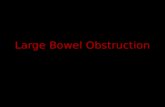
g ene rally in cre ase d w ith incre as ing spe cificity.An R O C curve w as cons truc ted (Fig . 7). P lotting sens itiv-
ity (true-positive fraction) vs 1- s pe cific ity ( fa ls e-p os itiv efrac tion) as the threshold differential air-fluid level height val-ues changed from 0 to 40 m m allow ed generation of a curvetha t illustra tes the usefulness of differentia l a ir-flu id levels in
discrim inating betw een adynam ic obstruction and m echani-
TA B LE 1 : M etho ds o f Proo f fo r M echan ical O bstruction an dA dynam ic O bstruction Episo des
N o. of Situations (% )Type of Clin ica l S urgery C ontrast Autopsy
O bstruction B I
Examinations
Mechanical n = 62) 25 (40) 34 (55) 3 (5) 0Adynamic n = 38) 33 (87) 2 (5) 2 ( 5) 1 (3)Mechanical + adynamic
n = 1 00) 55 (58) 36 (36) 5 (5) 1 (1)
TA BLE 2: Freq uen cy of D ifferentia l A ir-F lu id Levels asT hresh old H eigh t C han ges
N o. (% ) of C ases w ith D ifferentia lThreshold H eight Air-Flu id Levels
(m m ) M echanical A dynam ic
Obstruction n = 62) O bstruction n = 38)
>0 35 (52) 11 (29) 5 30 (48) 9 (24)
1o 20 (32) 8 (21)
15 19 (31) 4 (11) 20 1 4 (23) 2 (5) 25 13 (21) 2 (5)
30 7 (11) 1 335 6 1 0 1 340 2 (3) 0
Fig . 5 .-F req uen cy d istrib utio n o f d ifferen tia l air-flu id levels (D AF L)th resh old h eig ht. M O= m ec han ic al o bstru ctio n, A O= a dy na mic o bs tru c-tbon .
1 L: :: ii ::
z z2 0 _ _
10
S ..
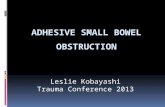
cal obstruction . The farther the arc of a plo tted set of valueis from the m iddle diagonal line , the higher are the sensitivand specificity of a test for a given problem . The m iddle dional line on the RO C curve, representing those circum
stances in w hich the sum of sensitiv ity and specificity equaone, can be thought of as representing a test that has a random chance of predicting abnorm ality . To com pare our tw ith that of random chance, we calcula ted the area unde
the curve created by using m ethodology equivalent to tW ilcoxon rank sum tes t [8]. The area under the differentair-flu id level curve equals 0 .63 , while the area underm iddle diagonal line is 0 .50 (p< .02).
Discussion
Although C T has recently show n som e prom ise , p la
abdom inal m adiographs rem ain the first im aging procedureevaluation of bow el obstruction [9-li]. The im portance offlu id levels and dila ted bow el for diagnosing bow el obstructio
on pla in abdom inal m adiogm aphs w as recognized early in
-
8/12/2019 Jurnal Annisa - Bowel Obstruction
4/5
TA B LE 3: SensitIv ity , Specific ity , an d Pred ic tive Values ofD ifferen tia l A ir-Flu id Levels for M ech anical O bstru ctio n an dR ela tio nsh ip to Th resh old H eigh ts
Note. -DAFL = d iffe re ntia l a ir-flu id le ve ls .
CYrusPositiveFrac t ion
294 HA RLO W E T AL. AJR:161 , Augus t1993
D AF L H eig ht(m m )
S ensitivity S pecific ityPositive
PredictiveValue
NegativePredictive
Value
>0 0.52 0.71 0.74 0.47
as 0 .48 0.76 0.77 0.48 1o 0.32 0.79 0.71 0.42
a15 0.31 0.89 0.83 0.44a20 0.23 0.95 0.88 0.43a25 0.21 0.95 0.87 0.42 30 0.11 0.97 0.88 0.40a35 0.10 0.97 0.86 0.40a40 0 . 03 1 .0 1 .0 0 .39
-
08 -.-
-.-.
0.7
06 -..
- - - -
-
:! 1 3 E,,
E E E E01 20.1
0
4
4-
....L..I.,.
0.1 0.2 0 .3 0 .4 0 .5 0.6 0.7 0 .8 0 .9
1 Spec#{225}ficity(FalsePositive Fract ion)
F ig . 7.-R ec eiv er-o pe ra to r-c ha ra cte ris tb c c urv e. A rea u nd er m id dle d l-ag on ai lin e= 0 .50. A rea under lin e d eriv ed fro m re su fts= 0.63. Dots rep-re se nt increa sin g th resh o ld h eig h ts o f d ifferen tial air-flu id levels(DAFLs) .
century [12, 13]. In 1919, Kloiber [14] reasoned that the pres-
ence of differentia l a ir-flu id levels on upright abdom inal radio-graphs confirm ed the diagnosis of m echanical obstruction .
M ore recently, Frim ann-D ahI [1] popularized the im portance of
differentia l a ir-flu id levels for d istinguishing betw een m echani-ca l obstruction and adynam ic obstruction and proposed that
ongoing perista lsis against a m echanical b lockage was them echanism of differentia l a ir-flu id level form ation . M ost con-
tem porary published reports sta te that d ifferentia l a ir-flu id 1ev-
els are not unique to m echanical obstruction and m ay occur inadynam ic obstruction as well [2-5]. This conclusion , how ever,
is based on evidence of clin ica l im pressions and on a reportby G am m ill and N ice [1 5], who reported two patients w ith ady-
nam ic obstruction w ho had differentia l a im -flu id levels on
upright abdom inal radiographs. A nalyses of differentia l a ir-fluid levels in large num bers of patien t w ith proved diagnoses
and rigorous sta tis tical analysis are lacking .The diagnosis in 58% of our episodes w as based on m ea-
sonable clin ica l evidence and outcom e rather than anatom icproof. A lthough this s itua tion is not ideal, defin itive proof ofm any m echanical obstructions and m ost adynam ic obstruc-tions is im possib le , because surgery, contrast exam inations
of bow el, and autopsy often are not perform ed. W e m inm ized the effects of th is situa tion by elim inating episodesw hich the final d iagnosis w as unclear. Another lim ita tion
th is study is that som e episodes of bow el obstruction m ahave been excluded from this study if bowel gas w as insufcient to produce air-flu id levels, a lthough this situa tion co
occur in either m echanical or adynam ic obstruction .The R O C curve shows the trade-offs betw een sensitiv ity
and specificity for m echanical obstruction by changing
threshold defin ition of a differentia l a ir-flu id level. The farthe R O C curve lies above the m iddle diagonal, the better t
test d iscrim inates for the diagnosis of in terest. The R O
curve of our results d iffers significantly from the m ain dianal line of essentia lly random choice (area under the curve=
0.63 vs 0 .50 , p< .02 [8J). The sensitivity is greatest a t the
low est threshold (any m easurable differentia l), but eventh is low level only about half of m echanicalobstructions
w ould be detected and alm ost a th ird of adynam ic obstructions would be m isdiagnosed. As the threshold increases ,
few er adynam ic obstructions are m isclassified , but m ore am ore m echanical obstructions are m issed . Although the R Ocurve indicates that using differentia l a ir-flu id levels to predthat an obstruction is m echanical produces better than ra
dom results, a t every potentia l threshold the com binations
sensitiv ity and specificity are too low to be clin ica lly usef
For exam ple , a t a threshold of 1 m m , the poin t a t w hich tRO C curve is farthest from the diagonal, nearly half tm echanical obstructions w ould be m issed (sensitivity= 0.52),
and about a th ird of adynam ic obstructions would be fa lseclassified as m echanical obstructions (specificity= 0.71).
Table 3 , how ever, illus tra tes that som e of the positive pr
dic tive values look im pressively high . For exam ple , a thresold of 20 m m gives a positive predictive value of 0 .88 . Thata prediction of a m echanical obstruction for every differentia ir-flu id level greater than 20 m m w ould be correct 88% oftim e. How ever, th is inform ation should not be used to inthat patien ts w ho have differentia l a ir-flu id levels sm aller t20 m m have obstructions that are not m echanical, because
77% of m echanical obstructions have differentia l a ir-flu idels sm aller than that (sensitiv ity= 0.23). N evertheless , posi-
tive predictive values do provide som e useful inform ation
although three caveats should be noted . First, inferencesshould be lim ited to popula tions sim ilar in re levant w ays topatients included in th is study. S econd, predictive value ifunction not only of specificity and sensitivity but a lso of
prevalence of the condition studied . The prevalencem echanical obstruction in our series w as 62% . A low er prevlence w ould decrease the positive predictive value . Third ,
have reported point estim ates only for a ll the proportionscited, som e of which are based on sm all num bers. For exam
pIe , the positive predic tive value at a threshold of 20 m m
based on the frac tion 1 4/1 6= 0.875. The 95% confidencein terval for th is estim ate is 62-98% [16]. S im ilarly, the a
under the RO C curve is 0 .63 , but th is estim ate has a standarderror of 0 .056, from w hich a 95% confidence in terval fortrue area is 0 .52-0 .74 . Arithm etic calcula tion w ith the mextrem e value of 0 .74 indicated that even if th is w ere the trarea , the available a lternatives of sensitiv ity and specific itrem ain fa irly unattractive for c lin ica l applica tion .
-
8/12/2019 Jurnal Annisa - Bowel Obstruction
5/5
A JR :161, A ugus t 1 993 A IR -FLU ID LEVE LS IN B O W EL O BS TR U CTIO N
Conclus ions
Although no radiographic sign should be used to the
exclusion of other findings, it is instructive to know how help-fu l or m isleading an isola ted diagnostic s ign is so that its
presence or absence will be used appropria te ly. W e havesh o w n th at reliance on the presence or absence of the differ-entia l a ir-flu id level sign to differentia te betw een types ofb ow el o bs tru ctio n is only slightly better than a randomguess. In our popula tion , how ever, positive predictive valueswere reasonably high for a ll d ifferentia l a im -flu id level heights
but w ere especia lly high at d ifferentia l a ir-flu id levels 20 m mor greater in height. Therefore , the presence of differentia l
a ir-flu id levels a t or above th is threshold height was m oder-
a te ly suggestive that the obstruction was m echanical.
REFERENCES
1 . F nm ann-D ahl J .R oen tgen exarn ina tions in a cu te ab dom inal d ise ases ,2 nd e d. S prin gfie ld , IL : T ho ma s, 1 96 0:1 12 -1 18
2. S cartz 55 . T he differentia l d iagnosis of in tes tinal obs truction .SerninRoentgenol 1973;8:323-3383. Eisenbe rg R L G astrointe stina l ra dio logy: a pa tte rn a pproa ch,2nd ed.
P hila de lp hia : U pp in co tt, 1 99 0:4 11 -4 29
4. M indelzun R E ,M C C O rt JJ. A cute a bdom en . In: M argu lis A R , B unhe nne Heds. A lim en ta ry tra ct ra dio lo gy .2 nd ed . S t. L ou is: M os by,1973:291-361
5. B aker S R .The a bdom ina l pla in film .Norwalk, C T: A ppleton & Lange,1990:155-241
6. M e tz C E. B as ic p rincip lesof R O C analysis. Se rn in N ucI M e d1978;8:283-298
7 . H erm an se n M . B io sta tistics : so me ba sic co ncepts.P atte rso n, N Y: C ad u-ce us M edical P ub lish ers, 1 990 :1 69 -17 4
8. H a ne ly JA , M cN eil B J .Th e meaning an d u se o f t he a re au nd er a r ec eiv ero p er at in g c ha ra ct er is ti c (R O C ) curve . Radiology 1982;143:29-36
9. M egibow M, B aitha za rE J , C ho K C , M e dw id SW ,B im baum B A , N oz M E.
B o we l o b st ru ct io n : e valua tio n w ith C T.Radiology 1991180:313-31810. F ukuya T , H aw es D R , Lu C C , C hang P J,Barboon TJ. C T diagnosis of
sm all-bow e l obs truction: efficacy in 60 patients.AI R 1992;158:765-769
11 . S tew art E li C T d ia gn osis o f sm all-bo wel o bstru ctio n.A IR 1992;158:771-772
12 . Schw arz G . D ie Erkennung den tiefere n D unndarm stenose m itte ls desRontgenverfahrens . W ie n K im W och en sch r 1911 40:1386-1390
13 . A ssm ann H . Zur R on tge nd iagnostik d e r D u n nd a rm s te n os e n.Otsch ZNervenheilkunde 1 91 3;4 7:1 -9
14. K boiber H . D ie R ontgendiagnose des bus ohne K ontnas tm itteb .A rch K imC h i r 1919;112:513-591
15. G a m m ill S I, N iceC M . A ir flu id le vels: the ir occurrence in no rm al pa tien ts
an d the ir rob e i n the a na ly sis of ile us.Surgery 1972;71:771-78016 . D iem K , ed.D ocum e nta G e igy: sc ie ntific tab les ,6 th ed . A rdsle y, N Y :G e igy P ha rm ace utica ls, 1962:85