Current approaches in the treatment of HCV GT 1b patient...
53
Current approaches in the treatment of HCV GT 1b patient with extrahepatic manifestations Clinical case Olga Sagalova St. Petersburg 03.06.2016 г.
Transcript of Current approaches in the treatment of HCV GT 1b patient...

Current approaches in the treatment of
HCV GT 1b patient with extrahepatic
manifestations
Clinical case
Olga Sagalova St. Petersburg 03.06.2016 г.

2
Complaints in May 2016 г.: pain throughout the body, musculoskeletal pains in the area
below head, pain in the lumbar and lower thoracic spine region (more intensive at
inclinations), numbness in the hands at the night, feeling that hands “were pumped”,
hands hoot for fatigue, knee joint pains, tearfulness, irritability, weakness and hands
pains (impossibility of exact movements), sensitivity violations, dryness of a mucous
mouth, nose, eyes.
Anamnesis vitae:
1977 - the urolithic disease was diagnosed. A stone of the left kidney, the lithotomy is carried out.
1978 - acute pyelonephritis of left kidney, complicated by peritonitis, left nephrectomy was carried out.
Hemotransfusions
1982 - reflux in the stump of the ureter, resection of the stump.
1991 - the recurrence of renal colic on the right. Repeatedly hospitalized in urology department with a
diagnosis of urolithiasis. A single stone of the right kidney.
1994 – suspicion of acute pyelonephritis of right kidney complicated by sepsis. 03.1994 г. – right kidney
decapsulation.
During the next 10 years condition was stable.
F, 59 years
old, BMT – 24,9
HCV
GT1b
F3 pegIFN/RBV
treatment in
2008 – D/C
before EOT due
to AEs

3
Case history
0 5 10 15 20 25 30
Arthralgia
Years
1999 – HCV antibodies
Lichen planus
dryness of a mucous mouth, nose, eyes,
paresthesia
Liver biopsy: F1 (2008 г.) Antiviral treatment failed:pegintron/RBV 05.11.2008 –
24.12.2008 г. D/C due to AEs
2011: scleroderma, Sjogren syndrome
2015 г.: severe pain, polyneuropathy of the hands*, Lyrica 300 mg QD with a strong
temporary effect
* Electromyography in 2015 г.: signs of bilateral demyelinating lesions of sensory and motor fibers of the median nerve in the
distal no signs of damage at the level of the carpal channel.

4
Patient B, May 2016 г.: lichen planus of oral mucosa, inactive
phase

5
Laboratory findings in May 2016
F, 59 years
old
HCV
GT1b
F3 pegIFN/RBV
treatment in
2008
Parameter Meaning
Total bilirubin, µmol/l 8.7
Direct bilirubin, µmol/l 3.0
ALT, U/l 116
ASТ, U/l 110
GGTP, U/l 78.7
Ureа, µmol/l 5.7
Creatinine, µmol/l 81
Creatinine clearence, ml/min 61
МНО 1,01
Albumin, g/l 39.7
C-reactive protein, mg/l 7.5 (N = 0.0 – 5.0)
Crioglobulines Not detected
Hb, g/l 117
Plt, х 109/l 165
WBC, х 109/l 5,42
Results of instrumental
methods
Fibroscan 11.08.2015 г. - 11,8
kPa
MSCT of the abdomen
14.03.2016:
Liver has a normal size, shape,
with clear contours. The spleen is
not enlarged, cysts of the spleen..
CT features of a state after left
nephrectomy, scarring in the left
psoas muscle after drainage of
the hematoma, the vicar zoom,
nephrolithiasis (multiple
concretions from 3 to 9 mm in
diameter), a moderate expansion
of the CPPS of the right kidney..

6
Diagnosis: CHCV (GT 1b, IL-28B CT), minimal activity, F3 Metavir ( Fibroscan 11,8 kPa ).
Extrahepatic manifestations: Systemic scleroderma, a chronic course, limited form, minimal
activity with skin lesions (the"mask-like" face, a symptom of a "tobacco pouch"), blood vessels
(Raynaud's syndrome), joints (arthralgia), myalgia, gastrointestinal tract (esophagitis, chronic
hypokinetic colitis with constipation), cardiovascular system (incomplete intra-artrial blockade),
polyneuropathy of the upper extremities. Secondary Sjogren's syndrome (xerostomia,
xerophthalmia). Lichen planus of the oral mucosa, an inactive phase.
Co-morbidities: Urolithiasis. Chronic pyelonephritis of the one right kidney, the active
phase, CRF 0. CKD 2. Cyst of the retroperitoneal space. Percutaneous drainage in Sept 2015.
Osteoporosis without fractures T - 3.3. Scoliotic deformation of the spine. Osteochondrosis,
aggravation. Lumbalgia.
Hypertension, the risk 2. Bronchial asthma, mild persistent current, controlled current.
Respiratory failure 0.
Peptic ulcer of duodenum without exacerbation.
F, 59 years
old
HCV GT1b F3 pegIFN/RBV
treatment in
2008

7
Some of the extrahepatic manifestations of HCV infection
Mixed cryoglobulinemia syndrome Autoimmune mechanisms
Skin:
- cutaneous necrotising vasculitis;
- erythema nodosum;
- urticaria;
Renal:
- membranoproliferative glomerulonephritis.
Hematologic:
- non-Hodgkin's lymphoma.
Neuromuscular and joint:
- peripheral polyneuropathy;
- myopathic syndrome;
- arthritis, arthralgia
Skin:
- lichen planus (1,9%)
- porphyria cutanea tarda.
Endocrine:
-thyroiditis;
- diabetes mellitus etc.
Hematologic:
-autoimmune thrombocytopenia;
- aplastic anemia.
Autoimmune and other:
scleroderma and CREST syndrome;
- Sjogren's syndrome (2-11,9%)

8
1. Ombitasvir/paritaprevir/ritonavir (25/150/100 mg QD)
and dasabuvir (250 mg BD) 12 weeks
2. Simeprevir 150 mg + sofosbuvir 400 mg QD 12 weeks
3. Sofosbuvir 400 mg + daclatasvir 60 mg QD 12 weeks
4. Daclatasvir 60 mg + asunaprevir 100 mg QD 24 weeks
Which of the IFN- free regimens would you
prefer?
‡

9
Which factors should be taken into account while
choosing the antiviral treatment?
1. Stage of fibrosis.
2. Efficacy of antiviral treatment regimen
3. Potential drug-drug interactions.
4. Renal disease.
5. Extrahepatic manifestations

10
Efficacy of IFN-free regimens in HCV GT 1b pts
without cirrhosis
1. Kwo P, et al. 50th EASL; 2015. Abstract LB14
2. Dieterich D. et al, EASL, 2014, P0755
3. Colombo M. et al., 2014 AASLD, Abstract #1931
4. Zuckerman E. et al. EASL 2016. Abst. PS004
5. Sulkowski M. et al. N. Engl. J. Med. 2014; 370(3): 211-221
6.Pol S, et al. EASL 2015. L03
7.Kao JH. et al, Liver Int. 2015 Dec 18. doi: 10.1111/liv.13049. [Epub ahead of print]
8.Shuhei H. et al., EASL 2016, Abstract SAT 261
97 91
86,4
0
20
40
60
80
100
SOF+SIM 3D SOF+DAC DAC+ASV
clinical trials
real-world data
1
8
SV
R 1
2 ,%
2*
* including SOF+SIM+RBV regimen
** SVR 4 for pts without cirrhosis
3 4 5 6**
7 98 98.6 99 100 100
‡

11
Which factors should be taken into
account while choosing the antiviral
treatment?
1. Stage of fibrosis.
2. Efficacy of antiviral treatment regimen
3. Potential drug-drug interactions.
4. Renal disease.
5. Extrahepatic manifestations

12
Current treatment:
-pregabalin (Lyrica) 300 mg QD,
- verapamil 120 mg QD,
- osteogenon 840 mg QD.
- tramadol ½ tablet QD
- risperidon 0,5 mg QD in the evening
F, 59 years
old
HCV GT1b F3 pegIFN/RBV
treatment in
2008

13
Potential drug-drug interactions
Drug SOF DAC SIM OBV/PTV/
r + DSV
ASV
Pregabalin - - - - -
Verapamil - + + + +
Tramadol - - + + +
Risperidon - - + + +
Osteogenon - - - - -
«-» - drug interactions are not expected
«+» - drug interactions are possible www.drugs.com/drug_interactions.html

14
Which factors should be taken into
account while choosing the antiviral
treatment?
1. Stage of fibrosis.
2. Efficacy of antiviral treatment regimen
3. Potential drug-drug interactions.
4. Renal disease.
5. Extrahepatic manifestations

15 Dumortier, AASLD, 2015, 1158
SOF-Based Therapy in HCV Patients with Severe Renal Failure
Retrospective study of SOF-based therapy in 50 patients with CHC with severe
renal failure (GFR < 35 mL/min) in France
France
n=50
Male, n (%) 36 (72)
Mean age, years 60.5±7.5
GT 1, n (%) 28 (56)
Cirrhosis, n (%) 27 (54)
Hemodialysis, n (%) 35 (70)
History of kidney transplantation, n (%) 17 (34)
History of liver transplantation, n (%) 11 (22)
On waiting list for kidney transplant, n (%) 27 (54)
Treatment naïve, n (%) 14 (28)
SOF+RBV, n (%) 7 (14)
SOF+PegIFN+RBV, n (%) 2 (4)
DCV+SOF±RBV, n (%) 30 (60)
SMV+SOF±RBV, n (%) 11 (22)
‡
90 88
0
20
40
60
80
100
SVR4 SVR12
Virologic Response (Interim Analysis)
Vir
olo
gic
resp
on
se,
%
Safety Results
GFR was not significantly modified
during treatment
Baseline: 29.6±6.2 mL/min
EOT: 27.9±6.5 mL/min
No cases of severe anaemia and
renal-related AE

16
Which factors should be taken into
account while choosing the antiviral
treatment?
1. Stage of fibrosis.
2. Efficacy of antiviral treatment regimen
3. Potential drug-drug interactions.
4. Renal disease.
5. Extrahepatic manifestations

17
Does successful antiHCV treatment with DAAs entail with reduction of extrahepatic manifestations?
Lichen planus:
– There are no published data regarding DAAs usage 1.
– Data regarding use of pegIFN/RBV are controversial 1
• Sjogren's syndrome:
There are no published data regarding DAAs usage.
Positive effect of pegIFN/RBV regimen has been registered in the limited number of observations 2
Scleroderma: There are no published data regarding DAAs usage
1. Sherman A .& Sherman K. Curr HIV/AIDS Rep (2015) 12:353–361
2. Doffoel-Hantz V. et al. La Revue de medecine interne / fondee
par la Societe nationale francaise de medecine interne. 2005;26:88–94.
18
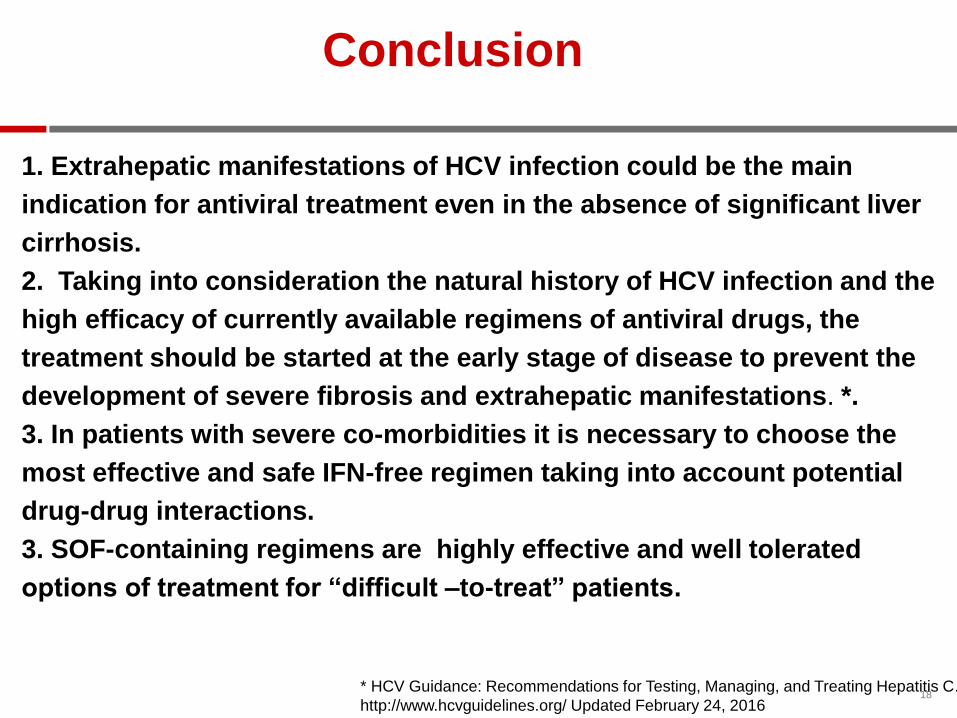
1. Extrahepatic manifestations of HCV infection could be the main
indication for antiviral treatment even in the absence of significant liver
cirrhosis.
2. Taking into consideration the natural history of HCV infection and the
high efficacy of currently available regimens of antiviral drugs, the
treatment should be started at the early stage of disease to prevent the
development of severe fibrosis and extrahepatic manifestations. *.
3. In patients with severe co-morbidities it is necessary to choose the
most effective and safe IFN-free regimen taking into account potential
drug-drug interactions.
3. SOF-containing regimens are highly effective and well tolerated
options of treatment for “difficult –to-treat” patients.
* HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C.
http://www.hcvguidelines.org/ Updated February 24, 2016
Conclusion

19
Thanks for your
attention

HCV genotype 2 infection: A case report
Professor Е. Esaulenko Saint-Petersburg State Pediatric Medical University

Genotype 2 is found worldwide, but is less common than genotype 1 and 3
Prevalence (Viremic)
0.0%-0.6%
0.6%-0.8%
0.8%-1.3%
1.3%-2.9%
2.9%-7.8%
North America Europe, Western Europe, Central Europe, Eastern Asia, Central Asia Pacific, High Income Asia, South
Asia, Southeast
Asia, East
Australasia
Sub-Saharan Africa, West Sub-S Africa, Southern Sub-S Africa, Central North Africa/Middle East Latin America, Andean Latin America, Southern
Latin America, Tropical
Latin America, Central
Caribbean
Razavi H, Gower E, Estes C, Hindman S. Global HCV Genotypes. Poster presented at: AASLD: The Liver Meeting 2013; 2013 Nov 1-5; Washington, DC, United States.

Prevalence of HCV genotype 2 in Russia
Country/Region %
Russia ~ 8,1% Pimenov et al., 2012
Russia ~ 4,4% Shustov et al., 2005
Russia, Moscow ~ 5,5% Vedernikov et al., 2010
Russia, Primorsky
region
~ 20% Sklyar et al., 2005
Russia, Saint-
Petersburg
~ 7,2% Zhebrun et al., 2011
3

In March 2016, patient was referred to the Clinical
Infectious Hospital named after Botkin, Saint- Petersburg, with:
1. high elevated liver enzymes: AlAT 350 U/L (reference range <
30 U/L);
2. positive HCV antibodies
3. PCR HCV +
4
Case report

Patient history & Examination in November 2015
County Russia
City St. Petersburg
Date of Birth 20/10/1952
Age, yr 63
Date anti-
HCV
15/11/2015
Reason for
testing: investigations
before surgery
Time of infection
and route of
transmission is
unknown
:
ALT 400 МЕ/L
Bilirubin 14 μmol/L
PCR HCV +
Genotyping and viral load were
not available
In November 2015 the patient
underwent cholecystectomy, which
was complicated by common bile duct
stricture.
5

Patient history & Examination in March 2016
ALT 350 МЕ/L
Bilirubin 12μmol/L
PCR HCV +
viral load
(HCV RNA
quantitative)
4x106 IU/mL
Genotype 2
Fibroscan F0
hemoglobin 110 g/L
platelet count 180x106 /L
Diagnosis:
Chronic hepatitis C,
replicative phase, GT2,
high cytolytic activity, F0
(Metavir)
6

Comorbidities
Chronic pancreatitis. Cholelithiasis. Choledocholithiasis, Bile duct stricture.
Arterial hypertension
– Losartan
Depressive Disorder
– Self-treatment with herbal OTC drugs
7

Will you treat this patient immediately or wait & monitor?
1. Treat now
2. Wait & monitor
8

EASL Recommendations on Treatment of Hepatitis C 2015
EASL Recommendations on Treatment of Hepatitis C 2015
In this case: the patient decided to start antiviral
treatment
9

Which treatment regimen would you choose in this GT2 HCV patient?
1. Pegylated IFN alpha 2 + Ribavirin
2. Pegylated IFN alpha 2 + Ribavirin +Sofosbuvir
3. Sofosbuvir + Ribavirin
4. Sofosbuvir + Daclatasvir
5. Daclatasvir + Asunaprevir
10

Treatment options recommended by EASL for patients with genotype 2 HCV infection:
•Daily sofosbuvir (400 mg) and weight-based RBV (1000-1200
mg) for 12 weeks);
• This regimen may be extended up to 16 or 20 weeks for
patients with cirrhosis, especially if treatment experienced
•Daily daclatasvir (60 mg) plus sofosbuvir (400 mg) for 12 weeks,
In Russia, Peg IFN + RBV for 24 weeks is still a standard of care
in GT2 HCV patients
11

97
78
98
8291
62
0
20
40
60
80
100
SV
R12 (
%)
No cirrhosis Cirrhosis Overall
58/59 44/54 10/11 8/13 68/70 52/67
SOF+RBV 12 weeks PEG-IFN+RBV 24 weeks
Error bars represent 95% confidence intervals
GT 2 Treatment-Naïve SOF+RBV vs PEG-IFN+RBV
FISSION
Lawitz E, et al. N Engl J Med. 2013;368:1878–87. 12

Zeuzem S, et al. N Engl J Med 2014;370:1993–2001.
93
68/73 212/250
Overall
97 100 94 78
Naïve, Non-cirrhotic
Experienced, Non-cirrhotic
29/30 2/2 7/9 30/32
SV
R12 (
%)
Naïve, Cirrhotic
Experienced, Cirrhotic
0
20
40
60
80
100 Overall
Non-cirrhotic
Cirrhotic
HCV GT 2 TN and TE SOF + RBV for 12 Weeks
VALENCE
13

Thank you for attention!
14

Treatment of Chronic Hepatitis C with DAA in decompensated cirrhotic patient
with Wilson disease
T.Rozina
Lomonosov Moscow State University
I.M.Sechenov First Moscow State University

Wilson disease
Rare congenital condition with impaired copper metabolism, leading to metal accumulation and damage of the target organs
Orphan disease
Disease gene (АТР7В) is located in chromosome 13
Prevalence is 1:30 000 inhabitants1,2
Carrier frequency 1: 90, 1:1001,2
Autosomal recessive inheritance
1.Scheinberg H., Sternlieb I. Wilson's disease. In: Smith L.H. Jr., ed. Major problems in Internal Medicine. -Vol. 23. -WB Saunders Company. -Philadelphia, -1984. 2.Roberts E.A., Schilsky M.L. A practice guideline on Wilson disease.// Hepatology. -2003. -Vol. 37. -N 6. -P. 1475-92.
Target organs:
Eyes
Heart
Kidney
Liver Brain
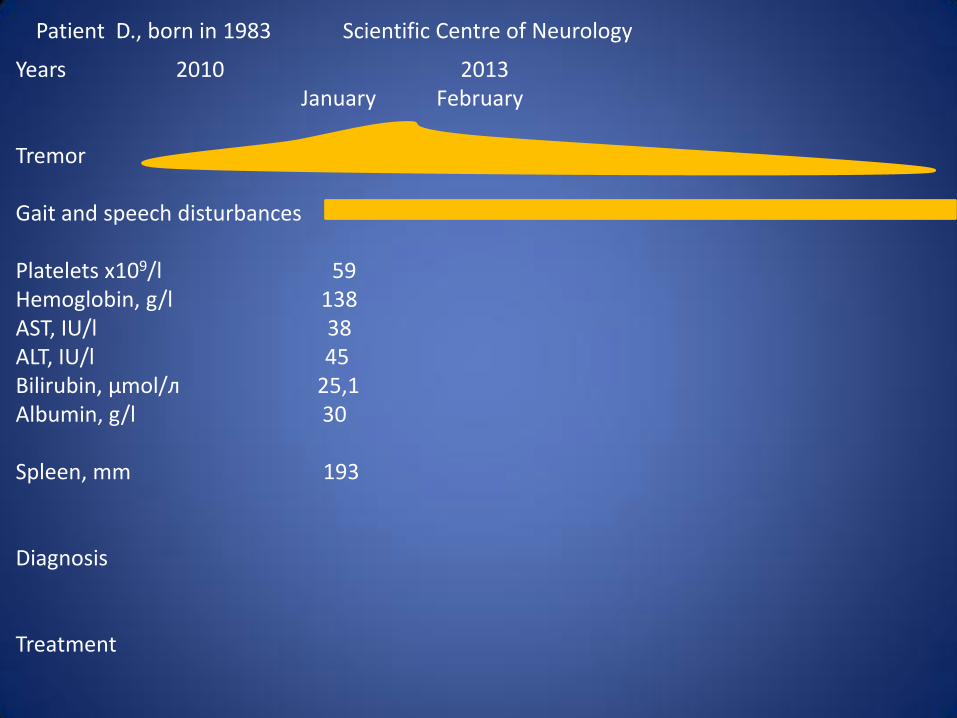
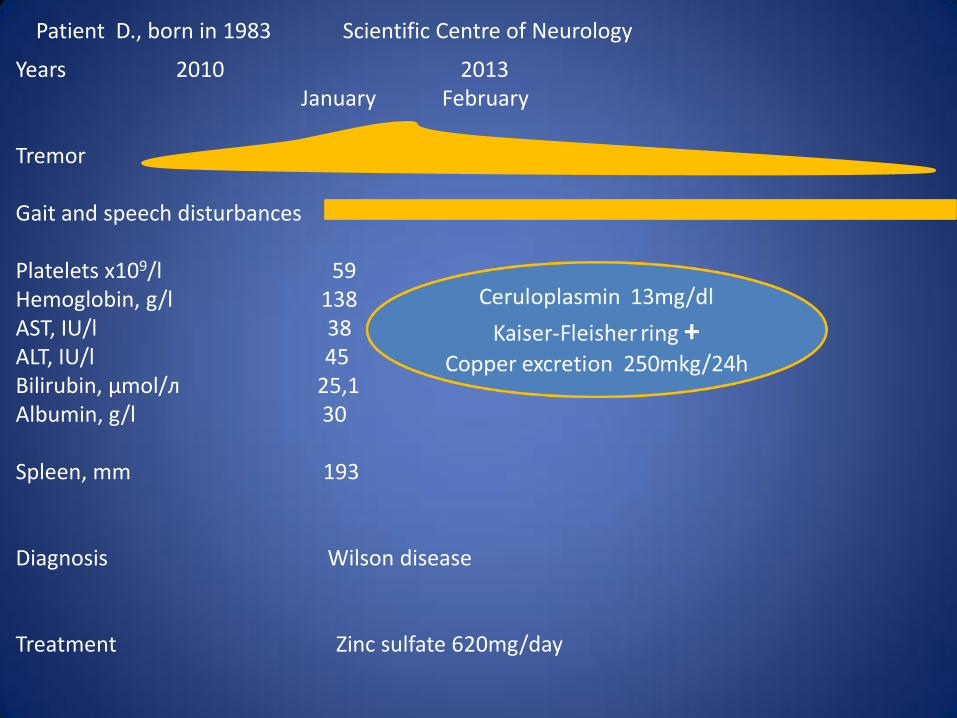
Patient D., born in 1983 Scientific Centre of Neurology
Years 2010 2013 January February Tremor Gait and speech disturbances Platelets х109/l 59 Hemoglobin, g/l 138 AST, IU/l 38 ALT, IU/l 45 Bilirubin, μmol/л 25,1 Albumin, g/l 30 Spleen, mm 193 Diagnosis Treatment
Patient D., born in 1983 Scientific Centre of Neurology
Years 2010 2013 January February Tremor Gait and speech disturbances Platelets х109/l 59 Hemoglobin, g/l 138 AST, IU/l 38 ALT, IU/l 45 Bilirubin, μmol/л 25,1 Albumin, g/l 30 Spleen, mm 193 Diagnosis Wilson disease Treatment Zinc sulfate 620mg/day

Patient D., born in 1983 Scientific Centre of Neurology City Hospitals N 52, 20
Years 2010 2013 2014 January February September January Tremor Gait and speech disturbances Platelets х109/l 59 61 Hemoglobin, g/l 138 134 AST, IU/l 38 63 ALT, IU/l 45 91 Bilirubin, μmol/л 25,1 26,4 Albumin, g/l 30 39 Spleen, mm 193 Diagnosis Wilson disease Treatment Zinc sulfate 620mg/day
Traumat i c Brain Injury

Patient D., born in 1983 Scientific Centre of Neurology City Hospitals N 52, 20
Years 2010 2013 2014 January February September January February Tremor Gait and speech disturbances Platelets х109/l 59 61 Hemoglobin, g/l 138 134 - 68 - 90 AST, IU/l 38 63 44 ALT, IU/l 45 91 55 Bilirubin, μmol/л 25,1 26,4 Albumin, g/l 30 39 Spleen, mm 193 Diagnosis Wilson disease Variceal bleeding Treatment Zinc sulfate 620mg/day Blood transfusions
Traumatic
brain Injury
GIB
Ligation
of
Varices
ASCITES
HBsAg – Anti-HCV –

Patient D, born in 1983 Tareev named Clinic of Sechenov First Moscow State Medical University
Years 2014 March April Tremor Gait and speech disturbances Ascites Hgb, g/l 87 AST, IU/l 47 ALT, IU/l 56 Bilirubin, μmol/l 18 Albumin, g/l 29 Prothrombin, % 78 Diagnosis Wilson disease: liver cirrhosis Child B, portal hypertension (ascites, splenomegaly, variceal bleeding, ligation of esophageal varices) Treatment Zinc sulfate 620 mg/day D-penicillamine 250 mg/day

Patient D, born in 1983 Tareev named Clinic of Sechenov First Moscow State Medical University
Years 2014 March April Tremor Gait and speech disturbances Ascites Hgb, g/l 87 95 AST, IU/l 47 520 ALT, IU/l 56 536 Bilirubin, μmol/l 18 43,6 Albumin, g/l 29 36 Prothrombin, % 78 Diagnosis Wilson disease: decompensated liver cirrhosis Treatment Zinc sulfate 620 mg/day D-penicillamine 250 mg/day

Patient D, born in 1983 Tareev named Clinic of Sechenov First Moscow State Medical University
Years 2014 March April Tremor Gait and speech disturbances Ascites Hgb, g/l 87 95 AST, IU/l 47 520 334 ALT, IU/l 56 536 385 Bilirubin, μmol/l 18 43,6 40 Albumin, g/l 29 36 38 Prothrombin, % 78 46 Diagnosis Wilson disease: decompensated liver cirrhosis Acute Hepatitis С Treatment Zinc sulfate 620 - 372 mg/day D-penicillamine 250 – 500 mg/day
HAV, HEV – HBV –
HCV RNA +, genotype 3

Which strategy would you prefer?
1. Symptomatic treatment
2. Increasing of Penicillamine dosage
3. To stop Penicillamine, because transaminases elevation can be caused by Penicillamine (DILI)
4. Immediate start of antiviral treatment
5. Wait 12 weeks for spontaneous HCV-clearance, than antiviral treatment if viremic

Patient D, born in 1983 Tareev named Clinic of Sechenov First Moscow State Medical University
Years 2014 2015 March April May July March June September Tremor Gait and speech disturbances Ascites Hgb, g/l 87 95 117 139 146 148 160 AST, IU/l 47 520 334 105 55 42 448 414 315 296 208 ALT, IU/l 56 536 385 137 64 49 598 583 376 464 396 Bilirubin, μmol/l 18 43,6 40 21 24 34,7 42 37 53 39 Albumin, g/l 29 36 38 40 42 45 41 45 Prothrombin, % 78 46 48 46 55 Diagnosis Wilson disease: decompensated liver cirrhosis Chronic Hepatitis С Treatment Zinc sulfate 620 - 372 - 248mg/day Stopped D-penicillamine 250 – 500 – 750 – 1000 – 1500 - 1500 - 1500mg/day
HAV, HEV – HBV –
HCV RNA +, genotype 3
HAV, HEV – HBV, CMV, EBV –

Database of Tareev named Clinic (1985-2016)
• 181 patient • 140 (77,3%) – liver cirrhosis, 79 (43,6%) –
decompensated liver cirrhosis • No cases with concomitant chronic HBV-infection • 3 patients with concomitant HCV-infection
1. Chronic hepatitis С, genotype 2, relapse after IFN + RIB 24 weeks. Now takes SOF + DAC
2. Acute hepatitis С, treated with SOF + RIB 24 weeks, SVR 3. Clinical case
In literature: Nałecz A. et al 1995, Lembowicz K. et al. 1999.

Patient D, born in 1983 Tareev named Clinic of Sechenov First Moscow State Medical University
Years 2014 2015 March April May July March June September Tremor Gait and speech disturbances Ascites Hgb, g/l 87 95 117 139 146 148 160 AST, IU/l 47 520 334 105 55 42 448 414 315 296 208 ALT, IU/l 56 536 385 137 64 49 598 583 376 464 396 Bilirubin, μmol/l 18 43,6 40 21 24 34,7 42 37 53 39 Albumin, g/l 29 36 38 40 42 45 41 45 Prothrombin, % 78 46 48 46 55 Diagnosis Wilson disease: decompensated liver cirrhosis Chronic Hepatitis С Treatment Zinc sulfate 620 - 372 - 248mg/day Stopped D-penicillamine 250 – 500 – 750 – 1000 – 1500 - 1500 - 1500mg/day
HAV, HEV – HBV –
HCV RNA +, genotype 3
HAV, HEV – HBV, CMV, EBV –
AVT

Which type of treatment would you prefer?
1. PegIFN + Ribavirin 24 week
2. PegIFN + Ribavirin + Sofosbuvir 12 weeks
3. Sofosbuvir + Daclatasvir 12 weeks
4. Sofosbuvir + Ribavirin 24 weeks
5. Sofosbuvir + Daclatasvir 24 weeks
6. Sofosbuvir + Daclatasvir + Ribavirin 24 weeks

Which type of treatment would you prefer?
1. PegIFN + Ribavirin 24 week
2. PegIFN + Ribavirin + Sofosbuvir 12 weeks
3. Sofosbuvir + Daclatasvir 12 weeks
4. Sofosbuvir + Ribavirin 24 weeks
5. Sofosbuvir + Daclatasvir 24 weeks
6. Sofosbuvir + Daclatasvir + Ribavirin 24 weeks

EASL Guideline for Cirrhotic Patients
European Association for the Study of the Liver (EASL). Recommendations on Treatment of Hepatitis C 2015, Journal of Hepatology, Vol. 63, Issue 1, p199–236
SOF + PEG-RBV
SMV + PEG-RBV
SOF + RBV
SOF + LDV
PAR/р + OMB +
DAS
PAR/р + OMB
SOF + SMV
SOF + DCV
GT 1а 12 w
12 w (naives or relapsers)
or 24 w (partial or null responders)
No 12 w with RBV or 24 w w/o RBV or 24 w with RBV in
negative predictive factors ответа
24 w with RBV No 12 w with
RBV or 24 w w/o RBV
12 w with RBV or 24
w w/o RBV
GT 1b No 12 w with RBV No
GT 2 12 w No
12 w (naives or
relapsers) or 24 w
(partial or null responders)
No No No No 12 w w/o RBV
GT 3 12 w No No No No No No 24 w with RBV
GT 4 12 w
12 w (naives or relapsers)
or 24 w (partial or null responders)
No
12 w with RBV or 24 w w/o RBV or 24 w with RBV in
negative predictive factors ответа
No 24 w with RBV
12 w with RBV or
24 w w/o RBV
12 w with RBV or
24 w w/o RBV
GT 5-6 12 w No No
12 w with RBV or 24 w w/o RBV or 24 w with RBV in
negative predictive factors ответа
No No No

Drug-drug interactions
www.hep-druginteractions.org

Lab Tests during Antiviral Treatment
Week 0 Week 4 Week 12 Week 24 Follow up
Week 4 Follow up Week 12
AST 208 33 30 33 36 32
ALT 396 38 29 28 31 36
Hgb 160 134 130 129 144 145
Bilirubin 42 42 37 46 19 49
HCV RNA 2,2 x 104 IU/ml
0 0 0 0 0
2015 2016

Conclusions:
• SVR 12 achieved
• Drug-drug interactions between Penicillamine with Sofosbuvir and Daclatasvir are not expected
• No clinically significant AE
• Cirrhosis compensation achieved due to concomitant treatment with Penicillamine and DAA

Long-term Prognosis in Wilson Disease
Study N Duration of
follow up, years Stable course Survival
Merle U et al., 20071
Germany 163 17 (1-51) 76% 98%
Svetel M et al., 20092 Serbia
142 11 79% 80%
Lowette KF, 20103 Belgium
24 15 92% 92 %
Bruha R, 20114 Czech Republic
117 12 (1-41) 82% -
1 Merle U et al. Gut. 2007;56(1):115-20; 2 Svetel M et al. Eur J Neurol. 2009;16(7):852-7; 3 Lowette KF et al. Eur J Gastroenterol Hepatol. 2010 May;22(5):564-71. 4 Bruha R et al. Liver Int. 2011;31(1):83-91