Coronary Heart #11 US
40
coronaryheart.com E M P L O Y M E N T Subscribe Free Online Future of Cardiology For Managers Inventory Why peers are a valuable resource Education A review of lifesaving and antithrombotic drugs CRM An extraction evolution Site Visit King’s College Hospital, London (as seen at TCT) Latest News From around the world Employment Time for a change? March / April 2008 Issue 11
-
Upload
cardiologyhd -
Category
Documents
-
view
229 -
download
1
description
Coronary Heart March / April 2008
Transcript of Coronary Heart #11 US

coronaryheart.com
EMPL
OYMENT
Subscribe
Free
Online
Future of CardiologyFor Managers
InventoryWhy peers are a valuable resource
EducationA review of lifesaving and antithrombotic drugs
CRMAn extraction evolution
Site VisitKing’s College Hospital, London (as seen at TCT)
Latest NewsFrom around the world
EmploymentTime for a change?
March / April 2008Issue 11

Coronary Guidewire
TERUMO INTERVENTIONAL SYSTEMS
Proven Terumo coronary guidewire technology NOW AVAILABLE in the U.S.
For more information, call 800.862.4143 to speak to an Inside Sales Customer Care Representative, or visit www.terumois.com
· Exceptional tip shape retention
· Unique DuoCore™ Technology
· Advanced coatings
Precisionyou can feel.
Precision is TERUMO Territory.
118898Adair Greene
Terumo4/c 8.125 x 10.875
118898a
Coronary Heart

March / April 2008
CONTENTS
02 Terumowww.terumois.com
07 Wavemark www.wavemark.net/chm
19 Healthworks www.healthworksonline.cc
20 Braccowww.bracco.com
35 AGFAwww.agfa.com/healthcare
04 Editorial
05 Latest News
08 Future‘Deja vu all over again’
12 Future‘Managing the Future of Cardiology’
15 Future‘Reinvigorating Our Best Plan’
23 Inventory‘Peers are a valuable resource to assist busy labs in evaluating solutions’
25 ECG Quiz
26 Cardiac Site Visit‘Kings College Hospital, London, UK’
29 Education‘Pharmacology - Part 1’
36 CRM‘Leads to the Heart - An Extraction Evolution’
38 Calender & Next Issue
39 Employment
THIS EDITION
ADVERTISERS
Table of Contents
St Peter’s Hospital in New York
Page: 15
CORONARY HEART ™ 3

From The Editor
Disclaimer:Coronary Heart should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from vari-ous companies and contributors, it is not possible to confi rm the accuracy of all statements. Th erefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Coronary Heart Publishing LtdIndependence Wharf
470 Atlantic Avenue, 4th � oorBoston, MA 02210
United States
Email: [email protected]: +1 (617) 273-8012
Visit us online at www.coronaryheart.com
Director / Chief EditorTim Larner
Clinical EditorDr Simon Redwood
Consulting EditorsDr Richard Edwards
Ms Voncile Hilson-MorrowMr Ian Wright
GENERAL ADVERTISING
Brett Goldine:[email protected]
RECRUITMENT ADVERTISING
CIRCULATION
USA edition
8900 Cardiac Professionals
Copyright 2006 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of Coronary Heart Publishing. The publication of an advertisement
or product review does not imply that a product is recommended by Coronary Heart Publishing Ltd.
Subscribe Online to get your own
free copy
EDITORIAL
Special Thanks
The Ever Changing World of Cardiology
It certainly is a busy time of the year. Th e end of March almost seems like confer-ence season with ACC, along with the
two leadership conferences, ACCA, and ACVP. For those of you coming to Chicago for these events, one of the most likely things on your mind is how to come away with an advantage. You will listen to talks from lead-ing departments around the USA, and see what new technologies are on off er, all with the idea of how to make things better in the future.
For this reason we thought we would give you a head start on the conferences and pro-vide you with interesting articles from John Florio, President of ACVP, and Robert Lunt, President of Th e LUNT Group. Both au-thors provide very timely articles as they both look into the future. We also have another great article from the team at St Peter’s Hospital in New York.
Our Site Visit this issue would be familiar for those whom attended TCT in Washing-ton DC in 2007, with the internationally recognized Kings College Hospital which was the host site for one of the live cases telecast. And fi nally our Education section looks at Pharmacology in the cath lab. Written by our education partner Health-works, this article is part one of a two-part series.
I am sure you will enjoy it. As always welcome, and if you have any comments please email me at [email protected].
- Tim Larner
Tim LarnerDirector / Chief Editor
4 CORONARY HEART ™

What’s New?
LATEST NEWSCAUTION: Some products within this magazine may be restricted to specific regional usage, and may not be available in your region. Always check with the manufacturer to determine availability.
Research Shows iPods Do Not Interfere With Cardiac Pacemakers
Over the past twelve months there have been multiple reports that iPods
can interfere with pacemakers after ONE patient experienced dizziness. Now though this theory has been disproved.
Howard Bassen, a researcher with the U.S. Food and Drug Administration led a research team to measure the magnetic fi elds produced by four diff erent iPod models.
Th e cardiologists published their results in the medical journal, Heart Rhythm, and found that all measurements indicated no eff ects on users with cardiac pacemakers.
So now you can expect to see more old folks with pacemakers bopping along down the street listening to their favourite tunes.
DES Perform Better in High Risk Patients
In a recent issue of the New England Journal of Medicine, researchers from the University of Pittsburgh School of
Medicine reported that “Th e use of drug-coated stents in patients with complex heart disease is associated with a lower rate of re-peat procedures without an increased risk of death or heart attacks compared to bare metal stents.”
Th e study was funded by the National Heart, Lung, and Blood Institute.
Endeavor Finally Gets FDA Approval
Although Europe has been using the Endeavor stent from Medtronic for a few
years now, the USA can fi nally see what all of the fuss is about. In early February 2008, the U.S. Food and Drug Administration (FDA) ap-proved the Medtronic Endeavor® Zotarolimus-Eluting Coronary Stent System, and is the fi rst new drug-eluting stent approved by the FDA since 2004.
Th e Endeavor data submitted for approval by the FDA was the largest for a drug eluting stent application, with over 4,100 patients followed up for over four years.
Th e Endeavor stent is available now.
Heart-Check Bed Under Development
There is a project currently un-derway in Europe, funded by the EU and led by Philips to
develop a bed that has sensors that can measure heart rate, breathing rate and body movement while sleeping. But that’s not all. Th e bed will also have a blood pressure monitor and weight
scales. As an extra, the patient could also wear a vest with woven-in elec-trodes to give a full ECG. Th e informa-tion could then be sent down a phone line to a doctors PDA.
Why is this a good idea? It is hoped the bed could reduce the need for emer-gency hospital treatment, helping spot problems several days before they be-come life-threatening.
Th e project, which was reported by the BBC, is expected to run for four years.
Courtesy of Apple
With Cardiac
Howard Bassen, a researcher with the U.S. Food and Drug Administration led a research team to measure the magnetic fi elds produced by
Th e cardiologists published their results in the medical journal, Heart Rhythm, and found that all measurements indicated no eff ects on users with cardiac pacemakers.
So now you can expect to see more old folks with pacemakers bopping along down the street listening to their favourite tunes.
Courtesy of AppleCourtesy of Apple
CORONARY HEART ™ 5

LATEST NEWS
Dual Balloon Catheter to Increase Speed and Improve Safety
Why have two devices when you can combine them into one dy-namic unit. This is just what
Canadian manufacturers Metricath have done with their new Gemini® dual balloon catheter. They have combined the Metri-cath arterial measurement balloon with a
high-perform-ance PTCA balloon.
We agree that the balloon does look rath-er odd however the combina-tion of the two t echno log i e s has a real po-tential of giving doctors the best chance of deploying a perfectly sized stent. This not only saves time in the lab but could reduce patient problems due to over/under sized stents during a case.
So, how do you get your hands on one? Unfortunately they are currently only ap-proved for peripheral use, however we guess it won’t be long before this technology sits alongside your other balloons in the cath lab.
Minnesota Researchers Create Beating Heart in a Lab
Earlier this year researchers from the University of Min-nesota managed to create a beating heart in their labora-tory, By using a process called whole organ decellulariza-
tion. Basically what they did was remove all of the cells from animal cadaver heart -- leaving only the extracellular matrix, the framework between the cells, intact.
This was followed by the hearts being injected with a mixture of progenitor cells that came from neonatal or newborn rat hearts, and then left in a sterile environment to grow (see image right). After only four days contractions were observed. After eight days the heart was actually seen pumping.
“We just took nature’s own building blocks to build a new or-gan,” said Harald C. Ott, M.D., co-investigator of the study and a former research associate in the center for cardiovascu-lar repair, who now works at Massachusetts General Hospital. “When we saw the first contractions we were speechless.”
“We used immature heart cells in this version, as a proof of con-cept. We pretty much figured heart cells in a heart matrix had
to work,” said Doris Taylor, Ph.D., director of the Center for Cardiovascular Repair, Medtronic Bakken professor of medi-cine and physiology, and principal investigator of the research. “Going forward, our goal is to use a patient’s stem cells to build a new heart.”
“It opens a door to this notion that you can make any organ: kidney, liver, lung, pancreas – you name it and we hope we can make it,” she said.
The research was published online in the January 13 issue of Nature Medicine.
Courtesy of M
etricath
Courtesy of the University of Minnesota
6 CORONARY HEART ™

LATEST NEWSCAUTION: Some products within this magazine may be restricted to specific regional usage, and may not be available in your region. Always check with the manufacturer to determine availability.
ETT to Predict Seriousness of MR
A recent study published in the American Journal of Car-diology found that exercise tolerance testing (ETT), may be useful in predicting mitral regurgitation pro-
gression and whether the patient will need surgery.
“Patients with mitral regurgitation who perform well on the treadmill will likely remain healthy and not have to undergo further testing for a number of years. This gives these patients peace of mind,” says principal investigator Dr. Phyllis G. Supi-no, associate research professor of public health in medicine and associate research professor of public health at Weill Cor-nell Medical College.
St Jude’s New Imaging Tool Combines CT with EnSite System
The days of an RT sitting on their hands during an EP study may become a thing of the past after the U.S. Food and Drug Administration
(FDA) cleared the EnSite Fusion™ Registration Module from St Jude. Basically the system works by combin-ing a three-dimensional computed tomography (CT) model with an EnSite System-created chamber model.
The Ensite Fusion also has capability for “dynamic registration” which allows for adjustments fusing the EnSite System-created and CT-derived models, giving physicians a more detailed image of the heart.
“The models produced by EnSite Fusion result in bet-ter, faster care for my patients and more reliable delivery of therapy for complex arrhythmias, such as atrial fibril-lation,” said Andrea Natale, M.D., who is a consult-ing professor at Stanford University and practicing at California Pacific Medical Center. “Because each heart is different, having a tool that helps guide the direction of the therapy through the detailed models is of great value to me.”
chm
Courtesy of the University of Minnesota
CORONARY HEART ™ 7

FUTURE
You’ve probably heard the famous quote by baseball great Yogi Berra, “This is like déjà vu all over again.” In terms of cardiovascular services,
today is déjà vu all over again as the annual membership meetings of the Healthcare Advisory Board are about to begin.
According to its website, the mission of The Advisory Board is to “secure economies of intellect on behalf of member organiza-tions - - discerning “True North,” com-municating these insights and best prac-tices with clarity, and providing innovative services so that our members can set com-pass and elevate performance accordingly.” (www.advisory.com)
In the past, membership meetings focused exclusively on the delivery of cardiovascular
services. This year the content also includes sessions on the future of neurosciences and orthopedics. Does including these disci-plines suggest the once-dominant cardio-vascular service line now has competition? Well, perhaps not competition, but it does mean that hospitals see business opportuni-ties in other services, which may affect the future for cardiovascular services. Just a few years ago annual meetings were almost exclusively cardiovascular in content, but vascular institutes gradually entered the picture. This year, a cardiovascular session called the Future of Cardiovascular Services will look at opportunities. The content in-cludes “impact of next-generation preven-tion and diagnostics, evolution of heart dis-ease treatment, tomorrow’s cardiac surgery volumes, and opportunities at the interven-tional frontier.” Sounds like an interesting meeting, perhaps even a must-attend for leaders from hospitals that belong to the Advisory Board.
As we start the new year, top leaders in our organizations are asking many of us what the future holds for cardiovascular services, and they expect answers.
The Future
French novelist and playwright Marcel Pagnol wrote, “The reason people find it so hard to be happy is that they always see the past better than it was and the present worse than it is, and the future less resolved than it will be.”
The author John M. Richardson, Jr. said, “When it comes to the future, there are three kinds of people: those who let it hap-pen, those who make it happen, and those who wonder what happened.” You can see a leadership theme emerging in his words.
And John Kotter, a Harvard Business School professor, said, “Leaders establish the vision for the future and set the strategy for getting there: they cause change. They motivate and inspire others to go in the right direc-tion and they, along with everyone else, sac-rifice to get there.” Without these visions or our own personal crystal ball, wouldn’t it be wonderful to have a time machine to take us into the future? We could see many of the new advances on the horizon and learn where to invest our resources to insure continued success in what is clearly an uncertain future. Perhaps the insight we gain from a time trip like this
DÉJÀ VU ALL OVER AGAIN
Written by: John Florio, Executive Director, Cardiovascular Services, University of Kansas Hospital, Kansas City, Kansas; President, ACVP
Mr John Florio
- A Fanciful Journey Seeking the Future of Cardiovascular Services
8 CORONARY HEART ™

FUTURE
would help lead our organizations’ cardio-vascular programs move forward into the future.
Time Travel
People have always been fascinated by time travel, as evidenced by the 129 movies and 70-plus television shows that have taken us forward or backward in time. Déjà Vu, the movie starring Denzel Washington, is but the latest. You probably have a favorite of your own.
But you should know there are several prob-lems associated with time travel, including machine design and the fact that not every-one understands the concept. Th ere’s also the fact that many people can survive time travel, but their clothing either doesn’t stay on or fails to change with the time period. And anyone who’s seen a time travel show also knows how diffi cult it is to alter past or future events. Sometimes the traveler is merely an observer and sometimes an actual participant.
In the movie Back to the Future (1985), the question about system design was raised and
answered. Remember the main characters, Marty McFly and Dr. Emmett Brown?
Marty: Wait a minute, Doc, ah, are you telling me you built a time machine out of a DeLorean?
Dr. Brown: Th e way I see it, if you’re gonna build a time machine into a c a r , why not do it with some style?
In Groundhog Day (1993), Phil keeps re-peating the day until he gets it right. He also fi nds that not everyone understands the concept of déjà vu:
Phil: Do you ever have déjà vu, Mrs. Lan-caster?
Mrs. Lancaster: I don’t think so, but I could check with the kitchen.
In Th e Terminator (1984), the question of clothing is addressed as the Terminator ar-rives naked and encounters some punks:
Punk Leader: Nice night for a walk, eh?
Terminator: Nice night for a walk.
Punk: Wash day tomorrow? Nothing clean, right?
Terminator: Nothing clean. Right. Punk Leader: Hey, I think this guy’s a cou-ple cans short of a six-pack. Terminator: Your clothes – give them to me, now. Punk Leader: (Unfortunately, his response cannot be printed).
Needless to say, the Terminator got the clothing he requested.Even though we’re aware of the problems associated with time travel, let’s give it a try. Traveling though time should provide some insight into what the cardiovascular world should look like in the future. Since some of the earlier problems associated with time travel have been solved, we can assume we will arrive properly attired. It should be noted that time machine con-trols are now linked to Internet search en-gines. To operate, simply type in the topic (Future of Cardiovascular Disease) and hit “enter.”
Hmm. Th e search returns more than
FUTUREFUTURE
CORONARY HEART ™ 9

FUTURE
170,000 hits. Pick the “take a chance” icon, and the machine begins to glow and make time travel noises. Hang on!
The Past
True to form, time travel is not perfect. When the light and noise stop, we find our-selves in a large building in Independence, Missouri, in the Midwestern region of the United States, and fortunately with cloth-ing intact. It appears something very of-ficial is going on. The date indicator shows it is July 30, 1965.
We’re in a large auditorium. Seated at an oval wooden table are two men engaged in a ceremonial signing of documents. One is much older than the other, and the younger man seems to be in charge. The men’s wives are standing behind their husbands, and other dignitaries fill the stage.
The distinguished older gentleman accepts two cards from the younger man, takes a pen and signs his name to the cards and other documents, and then pulls out a checkbook and writes a check for three dollars.
At age 81, former President Harry S. Tru-man and his wife have received the first Medicare cards ever issued from then-Presi-dent Lyndon B. Johnson. Johnson is 57 at the time. President Truman had long called for some sort of social system to make sure that older citizens received affordable medi-cal care.
Did our time machine err by taking us into the past when we wanted to look at the fu-ture? Not exactly. Medicare will to con-tinue to play a large part in the future of our business. Already physician practices are worried about predicted Medicare pay-ment reductions for cardiovascular services.
Hospitals always worry about Medicare payments, seeing a continuing shift from hospital admissions to outpatient proce-dures or extended recoveries, which have different payments schemes. Plus the entire Medicare payment system for hospitals is due to change, which could change reim-bursement dramatically.
The Present
Getting back in the time machine, we hit the forward button and come to rest just across the state line in Kansas. The time is January 2, 2008. A man sits across the desk from a government official in the local Social Security office. It’s only the second time in his life that he has met face-to-face with a representative of the U.S. Govern-ment. The first was when he entered the Army in 1968.
In response to a question from the official, he supplies his birth date, information about his mother and father, his military record and employment history. After he swears that all the information is true, she hands him his new Medicare card, which will be-come effective on his upcoming January birthday. Because he has medical insurance from his employer, he elects not to take the optional parts of Medicare at this time.
The time machine is in motion again, and as the scene fades I realize that the man looks very familiar.
Hospitals will continue to track the mix of types of insurance carried by their patients. Most, if not all, will also begin to see an increase in the size of the Medicare popu-lation as its ranks swell with aging baby boomers.
The Not-So-Distant Future
As the time machine moves forward to February 2008, we see a group of people in white coats sitting in a cardiology group practice management meeting. The agenda includes a variety of topics, but the discus-sion quickly turns to the significant decrease in the group’s interventional volumes.
The administrator shares survey data from a national cardiovascular organization that shows interventional volumes are typically down among the groups surveyed. Twenty-six percent have seen volumes decrease by 6 to 12%, and 25% have seen decreases of 13 to 26%.
The physicians are shocked but not com-pletely surprised, and they speculate on the reasons for the decrease. Considerable discussion results from the suggestion that recent data on drug- eluting stents have hurt the business, particularly as the pub-lic becomes aware of some of the problems with stents. One doctor talks about trying to get consent before a procedure from a hospitalized patient while a legal advertise-ment about stents plays on the TV in the background.
The group discusses the literature suggesting that instead of interventional procedures, patients might do as well with aggressive medical management. An older physician says he knows some good internists feel comfortable managing uncomplicated heart disease and have cut back on the number of patients they refer to cardiologists. He mentions a local internal medicine group that’s getting its own stress testing and echo units.
A general cardiologist begins a discussion about the effect that statins may have on patients’ health and notes recent research that describes significant improvements in
DÉJÀ VU ALL OVER AGAIN (cont...)
10 CORONARY HEART ™

cholesterol levels in patients on statins.
Th e administrator shifts the discussion to the group’s plan for its own imaging center, scheduled to be built across the street from the hospital. Th ey hope to gain greater rev-enues from technical fees, particularly those associated with their planned purchase of an advanced CT scanner.
Th e group talks about the limitations of fee-for-services, as indicated by the lack of bonuses for the last two quarters. Th e ad-ministrator brings them up to speed on his recent discussions with the hospital admin-istrator about building a freestanding imag-ing center on land the hospital owns adja-cent to its main campus. Rather than lose the support of the cardiologists, the hospital administrator prefers to have the building on campus and not across the street.
Much discussion ensues, including whether the group should purchase other advanced imaging equipment like an MRI and a PET scanner. Th e administrator reminds the group that the hospital’s off er to buy the group and employ its physicians is still open.
Th e Future, Up Close and Personal
I decide that the best way to learn more about existing and future technology in the cath lab is to visit an interventional cardiol-ogist fi rst-hand. I make the appropriate en-try into the time machine’s system. Almost immediately I fi nd myself in a dark room and feel pressure on my chest. I am cold and try to move my arm but can’t. True to some time-travel laws, my clothes have not made the journey.
I feel very sleepy as the doctor introduces
himself. I ask about future t e chno log i e s and where he sees them go-ing. He laughs and says not to worry about that, but to concentrate instead on the 90% blockage he’s found in my circumfl ex artery. He says he’s going to give me some medicine and then place a stent in the artery after opening it with a balloon.
As I drift in and out of sleep, I hear the sen-ior interventionalist respond to my question about future technology. He is talking to a young physician in training. Most of what he’s discussing concerns the pros and cons of new devices and clinical trials. I make out discussions of chronic total occlusion devices, PFO closure devises, bioabsorbable stents, the next generation of drug eluting stents and angiogenesis.
Th e senior physician says he’s sure admin-istration is not going to be pleased when they discover the cost of some of these technologies, especially when it will almost certainly not add to the profi tability of the labs. Having been trained at the Cleveland Clinic, he mentions some of the technolo-gies on its Top Medical Innovations list, which include dual energy source CTs, new oral anticoagulation drugs, percutaneous aortic heart valves and fl exible intralumenal robotics.
I respond to someone who’s calling my name. It’s the doctor again, and he tells me the pro-cedure was successful, and because the artery was large he used a bare metal stent. I drift back to sleep as I’m moved from the table to a waiting bed. I wake and try to move.
A nurse tells me to
keep my leg straight and try not
to move for the next six hours.
Th e nurse says I must have been dreaming about
time travel. She laughingly asks what I’ve learned in my
travels, and whether I have a better understanding of the fu-
ture. I start to tell her about the growth of the Medicare population and the changes and reductions in payments that will certainly aff ect the bottom line. I talk about the strains on capital budgets as new service lines emerge, as well as potential changes in referral patterns that could result in fewer patients coming to the hospital for interventional procedures.
In the middle of this, I express some fear that there’s really not a lot of information available for administrators to make good decisions. I tell the nurse I’d be totally lost without my network of friends in the CV administrative community who constantly share information and advice. Th e nurse is amused by my ramblings, es-pecially when I elaborate about my time machine and my quest to see what the fu-ture holds for CV services. “Time travel,” she says. “Th at’s funny because I watched a video of Th e Time Machine last evening. Th ere’s a great line that goes, “We all have our time machines, don’t we? Th ose that take us back are memories…and those that carry us forward are dreams.”
Th e nurse reaches for my IV and injects something into the line. I ask what it is, and she replies, “Just something to help you relax a little more, time traveler. Sweet dreams.”
but to concentrate instead on the 90% blockage he’s found in my circumfl ex artery.
A nurse tells me to
keep my leg straight and try not
to move for the next six hours.
Th e nurse says I must have been dreaming about
time travel. She laughingly asks what I’ve learned in my
travels, and whether I have a
FUTURE
CORONARY HEART ™ 11

FUTURE
How well I remember my Respiratory Therapist experience with my first open heart. In 1973 at Wesley Medical Center in
Wichita, Kansas, I helped Cardiac Surgeon Dr. George Farha, remove the intubation tube on his post-op open heart patient. This began his patient’s successful recovery and their next step in care. This patient, along with all the other cardiac surgery and MI patients, stayed many days in the hospi-tal recovering.
In late 1978 I moved on to a new career as a Physician Assistant assisting in open heart surgery. My first presentation as a CV
Administrator, in 1986, was on Developing Effective Product Lines in Cardiology for the American Hospital Association. I fol-lowed with two articles in 1992 on Manag-ing the Cardiology Product Line.
The “Product Line Management” concept emerged in the healthcare industry in the early 1980s as an organizational effort to deal with prospective reimbursement, a tight economic environment and declin-ing revenues, along with intense competi-tion. Hospital executives needed a way to improve the cardiology business line. This management process for cardiology has gone through numerous promotion and role changes. In the late 1980s hospitals became overwhelmed with the assignment of DRGs, Diagnostic Related Groups the rise of managed care, integrated healthcare systems, restructuring, total quality man-agement and cost reduction, along with the need to build volume and thus profit.
Product Line management was not a new theme to the healthcare industry. Johns Hopkins Hospital, Baltimore, Md., turned to product line management in 1974. This
1,380 bed facility created clinical centers and called them “decentralized functional units.” St. Luke’s Hospital, Kansas City, MO., turned to product line management in 1983, when it restructured its departments along specialty lines. Other organizations have followed their product line manage-ment techniques to better meet customer needs. I had administrative responsibility for the product line development at, East Jefferson General Hospital; The Gulf South Heart Centre; Orlando Regional Medical Centre, Orlando, Florida; St. Joseph Re-gional Heart Centre, Albuquerque, New Mexico, and many others across the United States.
Now is the time to discuss the rapid evolu-tion and business success of this most dy-namic service. What unprecedented tech-nological breakthroughs! The business road to success and the increasing demands for service have made this world of cardiology a journey with many turns. The obstacles include increased competition, skyrocket-ing cost, decreasing revenue and the ever growing level of disease along with the new cardiac patients - here we come, the 1950s Baby Boomers.
MANAGING THE FUTURE OF CARDIOLOGY
Written by: Robert D. Lunt, RRT., PA., MBA, President, The LUNT Group, Kansas City
- Past, Present And Future Of Healthcare’s Crown Jewel
Mr Robert Lunt
12 CORONARY HEART ™

FUTURE
In the 90s, as technological advances im-proved diagnostic and therapeutic capa-bilities, smaller hospitals were able to get into the cardiovascular business and com-pete more effectively with the full-service programs. Percutaneous and transcatheter interventions became standard in the 90s. Cardiac ERs and quick response teams in the field with Para-Medics changed the car-diac event. Acute MI to cath times were reduced and more patients were diagnosed needing intervention procedures.
All of these advancements, diagnostic and therapeutic, impacted on the complexity and patient mix of cardiovascular services.
The care model has developed into Path-ways, and we move the CV patients quickly out of the hospital. Length of stays has dropped to amazing levels and the role of CV Product Line manager began to emerge to manage, market and promote their Heart Centre’s capabilities.
Out of the CABG Patch.
2007 marked the 30 years since the father of interventional cardiology, Dr. Andreas Gruentzig, performed the first coronary angioplasty. Today, cardiovascular services delivery represents a $300 billion plus per year industry; cardiovascular care remains the #1 service line of all medical/surgical institutions throughout the US. However, the delivery of cardiovascular care is more complicated to organize that any other type of medical service. Looking back on the evolution of cardiovascular services in the 1990s, we had a growth business on all fronts. As the disease care model increased, so did the number of diagnostic and treat-ment breakthroughs that resulted in tre-mendous programme growth. It used to be that most cardiovascular services were confined to tertiary settings.
2008 Strategic Perspective
Strong Medical Staff leadership is critical. CV service lines need strong medical lead-
ers and champions, physicians willing to go face-to-face with their peers, challenge the status quo and support unpopular de-cisions. The CV service line administrator must develop strong relationships with physicians, sharing information and keep-ing them in the Business Loop.
Facilities
Major investments have been made in the Heart and Vascular Centers for faster serv-ices that achieve economies of scale and centralize CV services. The Heart Hospi-tal, inside or attached to the medical centre, creates and attracts physicians looking for better services delivery and optimized time. Ease of practice and state-of-the-art faculties are also key to attracting clinical staff when there are already critical shortages that are expected to worsen in the future. All one needs to do is look at the new Heart and Vascular Centers that have recently opened or the ones that are on the drawing boards with full plans to be built or redesigned.
CORONARY HEART ™ 13

FUTURE
Human Capital
Attracting and retaining Physicians and Clinical Support Staff will be the most criti-cal element; this major element must be monitored. Product Line managers must watch turnover and burnout. High demand physicians and group changes also are a ma-jor concern. Cardiologist and CV Surgeons are aging just like the rest of the 50s baby boomers. Planning for the CV MD staff-ing is strategic, as attractive new facilities and salary benefits are changing. High de-mand for specialists allied to short supply make this process a key concern that must be planned and managed.
Volume will continue to be the major in-dicator for service and patient mix, and for financial performance. Volume affects skill sets for physicians and staff, supports retention and helps to monitor quality and outcomes. It certainly affects the financial performance and costs.
Running a service line
CV service line managers are not alone now. There are other service-line manag-ers in Orthopedics, Rehabilitation, Wom-en’s Services, Children’s Services, Oncology Services and Neurology Services.
Future of Cardio-Vascular
A CV service provider must become unique. Do not let the past be the guide; it is a new business world of cost control, negative margins and trends. You now need to manage “50,000 ft big picture” perspec-
tives on the enterprise, and a 100 ft focused perspective for managing a service line day to day. It is a tough job. No “one size fits all” model works.
Good data and cost accounting systems should be put in place and costs must be watched. Share data with physicians on outcomes, cost, profit, market data, and referrals. It makes good sense to take CV services and run them as a Product Line. It has become a big business and Key Business Indicators must be monitored.
The new technology evolution:
Cardiovascular Information Systems (CVIS): merging data into images and networking it into CV-PACS. This new comprehensive imaging and information systems is growing and will continue to grow. The need for more interconnected departments that move the CV information along will merge with the imaging needs. All this will help cardiologists and CV sur-geons make clinical decisions through data mining.
The new cardiac leader:
Running a cardiovascular service line re-quires business tools and a tough decision maker to manage and build a business, make tough business decisions, utilize knowledge of market and business strategy and run at a profit. The difficulty with this is often the inability to make difficult but necessary de-cisions, and poor relationship building with physicians. Many organizations have yet to realize the value a good CV service line
manager can bring to the organization. This is reflected in the compensation offered, which is not consistent with the demands of the position. Many organizations also struggle to allow sufficient operating con-trol for the CV manager. Control of deci-sion making is necessary to make a signifi-cant impact. The advantages of Service Line Management are demonstrated by: strong leadership, staying focused on strategy, and looking at both the local and global mar-kets.
The disease is now the whole body…..the baby boomers are coming
Stents vs. Bypass Surgery will be the new review. The financial and clinical usage of stenting is reaching an impasse. The data supporting bypass surgery over stenting will begin to increase. The growing aging popu-lation will overwhelm the industry.
Hospitals will see the “sickest of the sick”. Planning on past performance will not be a good idea. Past growth and margins will not be the future experience. It will be necessary to keep the focused on stra-tegic plans, ensure numbers are realistic, and watch costs and margins, which will be more negative.
It is an exciting time: Welcome to the ever-changing dynamic world of cardiovascular medicine and the CV healthcare market 2008 and beyond.
MANAGING THE FUTURE OF CARDIOLOGY (cont...)
14 CORONARY HEART ™

FUTURE
For years, St. Peter’s Hospital in Albany, New York, has held a strong local reputation as a low-cost provider of excellent health care.
A 442-bed tertiary care hospital and member of Catholic Health Care East, St. Peter’s services are used by physician practices and ancillary medical facilities throughout Northeastern New York.
New York State leads the nation in deaths from cardiovascular disease, the number one cause of death in the United States. According to the American Heart Association, more than one million Americans die an-nually of cardiovascular disease, with care and treatment beyond $350 bil-lion annually.
At St. Peter’s, patient safety and suc-cessful surgical results were among the factors that helped the hospital’s Cardiac and Vascular Center to be named as a national Top 100 cardio-vascular hospital for eight of the past nine years. Only ten of the nation’s 6,000 acute-care hospitals earned this distinction as many times.
St. Peter’s is also the only hospital in New York State to be named a Distinguished Hospital for Patient Safety for each of the past four years – ranking it in the top three percent of hospitals for patient safety each year.
Five years ago, our strong position in local awareness provided the foundation for a marketing campaign to increase physician and pa-tient awareness about St. Peter’s cardiovascular expertise and serv-ices throughout Northeastern New York.
OUR BEST PLAN: - St. Peter’s Hospital builds awareness among patients and physicians
REINVIGORATING
Written By: Elmer Streeter, Director, Corporate Communications, St. Peter’s Health Care ServicesSteve Cameron, Director, Cardiac & Vascular Center, St. Peter’s HospitalJim Banahan, President, Banahan Communications
CORONARY HEART ™ 15

FUTURE
Where we beganTo help us develop a robust marketing strat-egy, a cooperative effort at St. Peter’s linked the hospital’s Senior Leadership Team, the management and physicians of the Cardiac and Vascular Center, and the Corporate Communications department. This part-nership led St. Peter’s to retain Banahan Communications to develop a strategic marketing plan, and a subsequent educa-tion and marketing campaign.
Based in Phoenix, Banahan has a solid track record of aiding large health care organiza-tions to optimize market position. The firm specializes in strategies and action plans that create awareness and enhanced recognition of broad-based cardiovascular programs.
The intent of our campaign was to solidify St. Peter’s position as the leading authority in cardiovascular services in Northeastern New York. We would improve alliances with identified community hospitals, devel-op collaborative relationships with physi-
cians and physician groups, and heighten a firm public perception that St. Peter’s offers the most qualified and caring cardiovascular professionals using the most current tech-nology for the highest quality of care.
Our first step was to create regional mar-keting zones, to better assess and manage unique patient needs in specific areas. A critical component of each zone was the lo-cation of community hospitals. This gave us five identified zones, each served by one or two key community hospitals.
We then conducted a broadly-focused mar-ket analysis that captured both the larger picture and the snapshots of each zone.
Our analysis incorporated patient flow pat-terns, physician groups, demographic and population figures, and referring physician patterns. We also estimated current and potential volume for each zone, and then rated the opportunities to enhance volume in the zones in terms of the probabilities for success.
To thoroughly understand where we were in the market versus where we needed to be for optimum success, we also performed market research to give us a baseline aware-ness/preference analysis. This also gave us a benchmark to aid in deriving a sense of our return on investment in the project.
Cementing our position From these studies, we developed unique planning strategies for each zone, capitaliz-ing on elements that held the most poten-tial to create long-term, synergistic success. A conscious decision to focus on identifying underserved and at-risk populations deter-mined that education about the five major risk factors (personal history, lifestyle, diet, cholesterol and smoking) would become a primary component of our campaign.
While all the action plans were zone-spe-cific, each drew upon a comprehensive framework that included corporate/com-munity health and early disease identifi-cation programs, screenings, educational sponsorships, and advanced communica-tion technology. We also determined that traditional marketing techniques would continue to play a key role in our plans, and that our communications would be both physician and community-directed.
We began with a very public, interactive demonstration that St. Peter’s is, in fact, the preeminent authority, locally and statewide, in the diagnosis and treatment of cardiovas-cular disease.
REINVIGORATING OUR BEST PLAN (CONT...)
16 CORONARY HEART ™16 CORONARY HEART ™

FUTURE
“Celebration of the Heart” was a single-day public symposium in 2004 featur-ing internationally-known cardiovascular professionals as well as regional specialists. More than 2,500 health care professionals and members of the public participated in presentations and discussions, including a question-and-answer panel with physicians from each of our identified zones. Another highlight was a live, televised angioplasty/stent procedures broadcast from St. Peter’s to an audience at Albany’s Palace Theater several miles away.
The symposium generated significant me-dia response, and set the stage for St. Peter’s to take an increasingly active role in leading the region in a campaign to reduce the inci-dence of cardiovascular disease and improve outcomes in treating the disease.
Creating collaborative partnerships and alliancesIn solidifying alliances with community hospitals, we undertook to assist their ef-forts to improve community services and education.
We did this by working with them to gain state approvals for diagnostic service im-provements, such as heart catheterization laboratories. This has a dual benefit, in significantly increasing the community’s abilities to identify at-risk patients earlier and more rapidly, and in providing St. Pe-ter’s with the more complex cases and treat-ments in which we specialize.
We also worked with community hospitals to provide co-branded educational presen-tations and materials for their communi-ties, and used their hospitals names and logos consistently with our own.
Our continuing emphasis rests on estab-lishing a process that provides continuity of care for cardiovascular patients. Collabora-tive relationships with physicians and phy-sician groups are also central to this effort. Improved communication through new technology is the key element in providing physicians with a high-tech system that sig-nificantly aids them in patient care.
Through this advanced electronic system, local physicians can view, in real or recorded time, any procedures their patients undergo at St. Peter’s. The electronic link can be ac-cessed from any of the physicians comput-ers, and can be viewed by the physician or reviewed with the patient. Instant e-mails throughout procedures augment the video record.
In establishing this type of rapid commu-nication specific to patient care, St. Peter’s has realized not just improved communica-tions, but also increased rapport with com-munity physicians and hospitals.
Corporate and community screeningsOur corporate program identifies people at risk for cardiovascular disease, and pro-vides follow-up assistance to help reduce significant risk factors for employees that
are identified.
In this program, employees first complete a health-risk assessment, followed by cho-lesterol, glucose, blood pressure, body mass index, and lung capacity screenings. An immediate consultation with a clinician sets next steps, such as dietary changes, weight-loss programs, and smoking cessation ef-forts.
In cooperation with community hospitals, St. Peter’s also presents more than 100 com-munity events and screenings annually. These include aneurysm, arterial disease, blood pressure and asthma screenings, and lipid profiles.
That these programs have a distinct impact upon our services is illustrated by the results generated by one atrial fibrillation screen-ing of 200 men and women. (About 15 percent of all strokes occur within people with atrial fibrillation.) Sixty-six people from that screening called St. Peter’s, and received treatment, representing $1.3 mil-lion in return.
The intent of our campaign was to solidify St. Peter’s position as the leading authority in cardiovascular services in Northeastern New York.
CORONARY HEART ™ 17CORONARY HEART ™ 17

FUTURE
Partnering for education through mediaThe emphasis on a collaborative approach carried through in our media campaign. All our advertising is carefully crafted with the intent to inform and educate. We actively enlisted our local and regional media in this effort. Because New York State has such a high incidence of cardiovascular disease, presentation of purposeful information af-fords our media partners the opportunity to meet their sense of public service.
Television and print advertising presented clear, simple messages, underscored by our theme: “The more you know about the cause and treatment of heart disease, the better prepared you’ll be to prevent it.”
Another key element of our advertising campaign was the establishment of a toll-free number that can be called to schedule any screening. 1-800-HEART 76 calls are routed through a call center, allowing us to specifically track which programs and advertising generate the most interest and response from our various communities across Northeastern New York.
A look aheadWe believe we see both tangible and intan-gible returns on our investment in build-
ing a broad collaborative coalition publicly committed to reducing the rate of cardio-vascular disease in New York State.
Certainly, our increase in the volume of services provided is a very tangible result, and we have seen a positive change in vol-ume overall in cardiovascular services. We
have also measured awareness in each zone, and can track increases of up to more than 40 percent.
By increasing the availability of certain serv-ices at the community level (such as cath-eterization labs), we are better able to focus on those specialty services which allow us to be the regional authority in cardiovascular care.
On the horizon, we will continue to focus on those services, adding subspecialties such as a pulmonary hypertension center, a lead extraction center, and additional electro-physiology services. We will also continue to acquire leading-edge technology in car-diovascular care.
Our growing reputation and recognition as one of New York’s and, in fact, the nation’s, preeminent cardiovascular centers is an in-tangible, but discernible, result.
We also believe that as we continue to em-phasize collaborative services to provide communities throughout Northeastern New York with a continuity of the high-est-quality care and education, we will af-fect a significant decrease in cardiovascular disease in this region. That’s our vision, and our mission in this campaign.
Our growing reputation and recognition as one of New York’s and, in fact, the nation’s, preeminent cardiovascular centers is an intangible, but discernible, result.
REINVIGORATING OUR BEST PLAN (cont...)
18 CORONARY HEART ™


Visipaque is a trademark of GE Healthcare.
©BDI 2007
Nonionic iodinated contrast media inhibit blood coagulation, in vitro, less than ionic contrast media. Clotting has been reported when blood remains in contact with syringes containing nonionic contrast media. Serious, rarely fatal, thromboembolic events causing myocardial infarction and stroke have been reported during angiographic procedures with both ionic and nonionic contrast media. Therefore, meticulous intravascular administration technique is necessary, particularly during angiographic procedures, to minimize thromboembolic events. As with all injectable contrast agents, the possibility of severe reactions should be borne in mind, regardless of the patient’s pre-existing medical history.
Please see brief summary of Prescribing Information on the following page.
Reference: 1. Solomon RJ, Natarajan MK, Doucet S, et al, and the Investigators of the CARE study. The CARE (Cardiac Angiography in REnally Impaired Patients) study: a randomized, double-blind trial of contrast-induced nephropathy in high-risk patients. Circulation. 2007;115:3189-3196.
The CARE study is the largest, prospective, randomized, double-blind comparison of iso-osmolar iodixanol-320 with low-osmolar iopamidol-370 in high-risk patients.1
Read the CARE study today. Visit CARECIN.comCall Bracco Sales Center at 1-866-282-2895or call Bracco Professional Services at 1-800-257-5181 option #2
We’re shedding more light on CIN.
CARE study: CIN* incidence in at-risk patients1
20
15
10
5
0
% P
atie
nts
With
Incr
ease
in S
Cr
≥25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.43†
9.8%
12.4%
1b.
% P
atie
nts
With
Incr
ease
in S
Cr
≥0.5
mg/
dL
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
20
15
10
5
0
P=0.39†
4.4%
6.7%
1a.20
15
10
5
0
% P
atie
nts
With
Dec
reas
e in
eG
FR ≥
25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.15†
5.9%
10.0%
1c.
* CIN defined as a) an absolute increase 0.5 mg/dL, b) a relative increase 25% in serum creatinine or c) a 25% decrease in eGFR from baseline to 45-120 hours postcontrast.
† P value is not statistically significant.
• There was no statistical difference in the incidence of CIN (SCr 0.5 mg/dL) following iopamidol-370 and iodixanol-320 (see Figure 1a)1
• The rates of SCr increases 25% were not significantly different (see Figure 1b)1
• The rates of eGFR decreases 25% were not significantly different (see Figure 1c)1
New evidence confirms what we’ve known all along.
The CARE study found no statistically significant difference between Isovue® and Visipaque™ in the rate of CIN in high-risk patients undergoing cardiac angiography or PCI.

Visipaque is a trademark of GE Healthcare.
©BDI 2007
Nonionic iodinated contrast media inhibit blood coagulation, in vitro, less than ionic contrast media. Clotting has been reported when blood remains in contact with syringes containing nonionic contrast media. Serious, rarely fatal, thromboembolic events causing myocardial infarction and stroke have been reported during angiographic procedures with both ionic and nonionic contrast media. Therefore, meticulous intravascular administration technique is necessary, particularly during angiographic procedures, to minimize thromboembolic events. As with all injectable contrast agents, the possibility of severe reactions should be borne in mind, regardless of the patient’s pre-existing medical history.
Please see brief summary of Prescribing Information on the following page.
Reference: 1. Solomon RJ, Natarajan MK, Doucet S, et al, and the Investigators of the CARE study. The CARE (Cardiac Angiography in REnally Impaired Patients) study: a randomized, double-blind trial of contrast-induced nephropathy in high-risk patients. Circulation. 2007;115:3189-3196.
The CARE study is the largest, prospective, randomized, double-blind comparison of iso-osmolar iodixanol-320 with low-osmolar iopamidol-370 in high-risk patients.1
Read the CARE study today. Visit CARECIN.comCall Bracco Sales Center at 1-866-282-2895or call Bracco Professional Services at 1-800-257-5181 option #2
We’re shedding more light on CIN.
CARE study: CIN* incidence in at-risk patients1
20
15
10
5
0
% P
atie
nts
With
Incr
ease
in S
Cr
≥25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.43†
9.8%
12.4%
1b.
% P
atie
nts
With
Incr
ease
in S
Cr
≥0.5
mg/
dL
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
20
15
10
5
0
P=0.39†
4.4%
6.7%
1a.20
15
10
5
0
% P
atie
nts
With
Dec
reas
e in
eG
FR ≥
25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.15†
5.9%
10.0%
1c.
* CIN defined as a) an absolute increase 0.5 mg/dL, b) a relative increase 25% in serum creatinine or c) a 25% decrease in eGFR from baseline to 45-120 hours postcontrast.
† P value is not statistically significant.
• There was no statistical difference in the incidence of CIN (SCr 0.5 mg/dL) following iopamidol-370 and iodixanol-320 (see Figure 1a)1
• The rates of SCr increases 25% were not significantly different (see Figure 1b)1
• The rates of eGFR decreases 25% were not significantly different (see Figure 1c)1
New evidence confirms what we’ve known all along.
The CARE study found no statistically significant difference between Isovue® and Visipaque™ in the rate of CIN in high-risk patients undergoing cardiac angiography or PCI.

≤
Rx only
BRACCODIAGNOSTICS
Rx only
Iopamidol Injection 76%
NOT FOR INTRATHECAL USE
ISOVUE®-200Iopamidol Injection 41% ISOVUE®-250Iopamidol Injection 51% ISOVUE®-300
ISOVUE®-300Iopamidol Injection 61% ISOVUE®-370Iopamidol Injection 76%

INVENTORY
≤
Rx only
BRACCODIAGNOSTICS
Rx only
Iopamidol Injection 76%
NOT FOR INTRATHECAL USE
ISOVUE®-200Iopamidol Injection 41% ISOVUE®-250Iopamidol Injection 51% ISOVUE®-300
ISOVUE®-300Iopamidol Injection 61% ISOVUE®-370Iopamidol Injection 76%
Cardiac Cath Lab directors are bombarded with information about new products and serv-ices and so they are turning to
their peers to sift through it all to find about solutions that work and companies that can be trusted. In a recent study by The Aber-deen Group, it was found that 69% of or-ganizations having success with RFID im-plementations relied on their peers to find
an RFID solution. The Alliance of Cardio-vascular Professionals (ACVP) is one such resource where members can network with each other to improve the quality of care and operations of their labs. As the Direc-tor of Cardiovascular Services at University Hospital in Augusta, GA and a member of ACVP, I looked to my peers to find out how they were managing the growing inventory levels and financial commitments associ-ated with high-value, consumable medical supplies.
University Hospital is a 581-bed, Magnet-designated, tertiary care facility, offering in-novative care for the greater Augusta region. In 2006, the Cardiac Cath Lab performed multiple procedures on over 6,000 patients. High-end inventory such as coronary and peripheral balloons, stents and other de-vices priced over $100 account for approxi-mately 80% of the supply budget. Choos-ing the right inventory solution could have a significant impact on reducing expenses. The solution had to address the needs and concerns of every level of the organization: lab management, clinical staff, materials management, finance and administration.
University Hospital had clearly defined ob-jectives and needs, making evaluating op-tions a bit easier.
Provide real-time view of inventory levels
Significantly reduce on-hand inven-tory
Track missing items not accounted for during procedures
Validate that all potential charge/bill-ing opportunities were captured
A better way to manage expired and soon to expire products
Facilitate tracking of items by lot number
Establish par levels that are dynamic, and based on actual usage
After researching solutions and interview-ing peers, University Hospital concluded that RFID technology provided the most efficient means to get accurate, real-time inventory information for reducing supply costs and improving charge capture, with-out impacting current workflow. The lab also benefited from peer advice about ven-dor reliability, trustworthiness, and follow-through. University Hospital implemented an RFID solution in mid-September 2007 in order to achieve the goals outlined at the onset of the project.
•
•
•
•
•
•
•
Peers Are a Valuable Resource to Assist Busy Labs in Evaluating Solutions
Teresa WatersDirector of Cardiovascular Services,
University Hospital, GA
University Hospital, GA
CORONARY HEART ™ 23

INVENTORY
Reducing On Hand Inventory Levels
“With RFID, we were able to safely and effectively reduce our stock of expensive items.” said Chris Lucas, Cath Lab Inven-tory Coordinator at University. “We ana-lyzed our actual usage over time and made adjustments to line-item par levels. So even when we brought in new products, I could keep overall inventory levels down.”
Once the par levels came down, closing
the gap between On Hand Inventory levels and Target Inventory (TI) had significant impact on the department’s financial per-formance “At its highest, we were 72 items over par during the week ending November 17. By using real-time automated replen-ishment, we narrowed this gap to only 10 items over par by the end of January.”
Identifying missing products
One of the surprising benefits that the lab learned from peers during the evaluation
process was the ability of RFID to track the location and disposition of every item – from the time they enter the hospital to usage and even to see if an item has gone missing. With many products carrying a price tag over $1000, missing items can be a significant drain on revenue while poten-tially compromising patient safety. RFID helps eliminate that risk and provide peace of mind to clinical staff that the right prod-uct will always be available and accounted for.
Peers are a Valuable Resource (cont...)
24 CORONARY HEART ™

INVENTORY
Managing expirations and recalled products
In polling peers, University Hospital was in-terested in reports of vastly reduced manual work associated with managing expiration dates. Identifying and removing expired products before they reach the patient is a major concern. Lucas notes, “Without RFID technology, we needed to visually in-spect all of our products at least monthly. With RFID, we are alerted to expired and
short–dated products automatically, and to their location within our department.” Similarly, RFID also improved the ability to execute recalls by showing us where affected lot numbers of product are in inventory, as well as telling us if they had been used dur-ing a case.”
Peer recommendations, discussion groups and professional affiliations have always been a resource for busy lab managers. Effective networks of thought-leaders in the field can
lead to the adoption of best of breed, cut-ting-edge technology solutions that work. Peers are also part of the due diligence proc-ess for selecting the company that offers the product or service. After speaking with peers, University Hospital chose WaveMark CIMS, a web based solution utilizing RFID technology for inventory management in specialty areas. The solution is available on a subscription based, with no capital ex-pense or upfront fees. WaveMark (advert on page 7) is also a member of ACVP.
ECG QUIZ Provided by: Ian Wright, Technical Head EP, St Mary’s Hospital, London, UK
What is the ECG rhythm?
What is the relationship between atrial and ventricular complexes?
1.
2.
Answer: Page 34
CORONARY HEART ™ 25

SITE VISIT
Kings College Hospital
ADDRESS
MAP
Cardiac Cath LabKing’s College HospitalNHS Foundation TrustDenmark HillLondon SE5 9RSUnited Kingdom
Internationally Recognized
Kings College Hospital is recognized internationally as a world leading cardiac facility and is one of London’s largest
and busiest teaching hospitals. Opened in 1840 and today with 950 beds, Kings continues to expand with a new wing opened in 2003 by Her Majesty Th e Queen.
For those whom attended the Transcath-eter Cardiovascular Th erapies (TCT)
conference in 2007, you may have seen the live case telecast from here when the con-sultant cardiologist Dr Philip MacCarthy performed the fi rst coronary angioplasty using the Sprinter Legend Balloon Cath-eter from Medtronic.
Kings is also the fi rst lab in the UK to use the Edwards Lifesciences balloon for aortic valve stenosis. In August 2007, King’s staff carried out the fi rst two successful transapi-cal aortic valve replacements in the UK
and two percutaneous aortic valve replace-ments.
Th e department is also a central hub for patients coming from local district general hospitals and therefore a large portion of patients performed are extra complicated.
Special thanks must be given to Mr Greg Cuickshank, Radiographer Manager of the cath labs for answering the following questions.
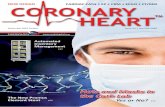
Kings College Cath Lab Team
Starting left foreground: Junior Sister Emma Saunders; Research Sister Michelle Andrews; Specialist Registrar Dr John Byrne; Cardiac Technician Raghunath Behera; Consultant
Cardiologist Dr Phil MacCarthy; Senior Radiographer Matt Trevail; Senior Sister Hannah Kent; Student Radiographer Tudor Kennard; Staff Nurse Zoe Duke; Cardiac Technician Sandip Vias; Junior Charge Nurse Jonathan Breeze; Staff Radiographer Fiona Desmond; Superintendent
Radiographer Greg Cruickshank; Junior Sister Maricel Paguyo; Staff Nurse Cristina Fernandez-Gonzales; Staff Nurse Lucy Barwick; Staff Nurse Rajashree Khandagale.
26 CORONARY HEART ™

SITE VISIT
Size of hospital and department:
King’s College Hospital is a 950 bed teach-ing Hospital in South East London. There are 3 labs; 1 EP and pacing, 2 are diagnos-tic and interventional. There is also mobile unit with floating table used for temporary pacing on our Coronary Care Unit.
Staff Numbers:
9 Nurses (currently only cover 4 on-call)
8 Cardiac Technicians,
1 fulltime Radiographer, 20 rotating Radiographers from Radiology Dept,
1 fulltime Radiography Assistant Practitioner.
Procedures:
Full range of diagnostic and interventional electrical and arterial procedures, as well as trans-apical and trans-femoral aortic valve replacements.
Equipment:
Two Philips Allura Flat Panel labs
1 Siemens Coroskop lab
1 Siemens Cathcor Haemo-dynamic system
2 Axiom Sensis Haemo-dynamic systems
Radi Pressure Wire facilities in both Interventional labs
3 IVUS machines
1 Ziehm Vista Mobile Image Intensifier and mobile floating table top examination couch used in Coronary Care Wing for temporary pacing cases.
•
•
•
•
•
•
•
•
•
•
•
Day Procedures:
Yes, routine elective diagnostic and inter-ventional coronary procedures as well as EP cases.
Procedures performed per year:
Approximately 3600 cases per year, includ-ing 1500 PCI’s, and 240 pacing devices.
Hemostasis Management:
Angioseals, occasionally Star-close, digital pressure and Fem-stops.
New procedures implemented:
Trans-femoral and trans-apical aortic valve replacements.
Cross-Training of staff:
There is overlap between the 3 support staff groups. For on-call purposes, each role can be covered by at least one other Health Pro-fessional or Medic, so we can start urgent cases when Consultant Cardiologist and 3 of the following four staff are in; Special-ist Registrar, Radiographer, Cardiac Tech-nician and Nurse. Note this is done only in the case of absolute necessity – not done routinely.
Inventory Management: Materials management for most products. Drug eluting stents + other irregularly used products are ordered by nursing staff. We use the pen and paper method however will be investigating other options soon.
Cath Lab Control RoomCardiac Tech Sandip Vias (back turned) and Staff Radiographer Fiona Desmond
CORONARY HEART ™ 27

SITE VISIT
Alliances with other hospitals for treatment of patients:
We have close relationships with a number of local district general hospitals and per-form procedures on a treat and return/keep/discharge basis.
Training for new employees:
Radiographers: Full training in all as-pects of Cardiac Radiography from scratch.
Nurses: Cardiac rotation involving all car-diac departments over the course of a week, supernumerary status for two weeks, full
mentorship support until scrubbing inde-pendently, shadow on-calls until compe-tent/confident to do on-call independently.
Continuing education programs for staff: In-house weekly cardiac teaching sessions with Practice Development Nurse, regular morning industry training sessions, access to national conferences/study days, access to KCL post-registration courses/study days, mandatory in-house training, other in-house professional development courses. Also weekly 1 hour talks by SHO’s, and monthly Journal club.
Competency checks for staff:
Radiographers: have bi-annual compe-tency checks signed off in all areas.
Nurses: extensive trust-wide nursing com-petency document that is regularly updated and reviewed. On-call competency check-list.
Challenges:
Recruitment and retention of staff, as London becomes a more expensive place to live.
Big increase in emergency out of hours work over the past two years.
Increase in complexity of cases.
What is the best part of working at your facility?
Friendly department, with a patient focused approach, at the cutting edge of Cardiol-ogy.
•
•
•
Kings College Hospital (cont...)
Staff Nurse Zoe Duke (foreground) and Dr Phil MacCarthy
28 CORONARY HEART ™

EDUCATION
Beep beep beep. It’s 3 am and your pager is going off again. It’s Dr. Bound’s pa-tient in the Emergency Department (ED). You call for a report: 60 year old woman, chest pain 10/10, ST elevations in the ante-rior leads, hemodynamically unstable with a heart rate of 110 and BP of 90/50. She has no previous cardiac history. Th e ED says, “She doesn’t look good, she’s cool and clammy, nauseated and short of breath.”
You know this is a typical presentation for a patient with myocardial infarction. But do you know the physiology behind the presentation? You anticipate the need for blood pressure (BP) support, and you know
dopamine and Neosyn-ephrine® -- aka phenylephrine -- both support BP. But do you know how these drugs work and why one may be a better choice in a given set of cir-cumstances?
Aspirin has been given, but what other an-tithrombotic medications should be used? How do these meds actually work? How does the physician choose among the agents available? And what are the latest Ameri-can College of Cardiology/American Heart Association guidelines for antithrombotic therapy?
By Charlene Shellenberger, BS, RN, Clinical Education Specialist,
Healthworks, Inc.
And The Beat Goes On…
The following article was made possible in part by an unrestricted educational grant from Bracco Diagnostics Inc. For more information, please visit them at www.bracco.com
- A Review of Lifesaving and Antithrombotic Drugs
Part 1 of a Two-Part Series
CORONARY HEART ™ 29

EDUCATION
In a field changing as fast as ours, it’s never been more important to keep up-to-date on the answers to these questions. And that’s the goal of this article: to give members of the cath lab team a better understanding of symptom presentation and the mechanisms of action of the hemodynamic support drugs commonly used in the cath lab. We’ll also review the major antithrombotic medi-cations, their modes of action, and 2007 ACC/AHA recommendations.
To understand the why of the medications we give, we’ll start with a short physiology refresher in Part I. Part II will cover the medications themselves, their actions and indications.
All about the Autonomic Nervous System
The autonomic nervous system (ANS) provides an autoregulatory function to maintain the body’s hemodynamic home-ostasis. These maintenance activities are primarily performed without conscious control or sensation: we don’t need to con-sciously think about breathing or making our hearts beat.
Much of this regulatory function is located in the medulla oblongata in the brain stem. This explains why patients who are declared brain dead continue to have a heartbeat,
and why other elemental body functions re-main intact: they’re regulated by the auto-nomic nervous system and don’t require the higher brain function of conscious thought in order to continue.
The ANS has two opposing (or complimen-tary) divisions: the sympathetic and para-sympathetic systems. The sympathetic sys-tem provides the “fight or flight” response when immediate action is required: it’s the gas pedal. The parasympathetic system is the “rest and digest” mechanism. It calms our nerves and slows things down. It’s the brake pedal.
AND THE BEAT GOES ON (cont...)
Sympathetic Receptors
Alpha
Located in peripheral arteries
Beta 1
Located in the heart
Beta 2
Located in the lungs and arterial walls
Dopaminergic
VasoconstrictionIncrease in heart rate
Bronchiolar dilation arterial vasodilation
Located in coronary arteries, renal & mesenteric blood
vessels
Increase in arterial pressure
Increases contractility,
conduction, and irritability
DilationKidneys
Mesenteric
Figure 1: Sympathetic Receptors
30 CORONARY HEART ™

EDUCATION
All about the Sympathetic Nervous System
The sympathetic nervous system’s “fight or flight“ response is often explained as an evolutionary protective mechanism that de-veloped to help us escape the saber-tooth tigers that were chasing us. Although we’re no longer being chased by tigers, the stres-sors of modern life stimulate our sympa-thetic nervous system and cause catecho-lamine release.
The catecholamines and neurotransmitters of the sympathetic system, noradrenalin (norepinephrine) and adrenalin (epine-phrine) have specific receptor sites and elicit a specific response. The sympathetic receptors are alpha, beta (1 and 2) and dopaminergic. Refer to Figure 1.
Alpha receptors are located in peripheral arteries. When stimulated, they cause vaso-constriction, thereby increasing blood pres-sure and systemic vascular resistance (SVR). Think of water running through a pipe four inches in diameter: if the amount of water remains the same but the pipe is now only two inches in diameter, the water pressure will be greater.
A common cath lab drug that exhibits pure alpha effects is Neosynephrine®(phenylephrine). This is an alpha agonist that raises blood pressure without causing an increase in heart rate. It’s typically the drug of choice in septic shock when the patient has a heart rate of 120 and BP of 80/40.
Other vasopressor agents like dopamine have both alpha and beta 1 properties. They cause an increase in heart rate as well as BP, thereby increasing myocardial oxygen demand. So if our patient is in cardiogenic shock with a heart rate of 40 and a BP of 80/40, dopamine is a logical choice as a va-sopressor since it supports blood pressure and augments the heart’s pumping capabil-ity,
Helpful hint: Before any form of va-sopressor is administered, the patient should be adequately hydrated: it’s counterproductive to squeeze an empty container. Remember: without ad-equate hydration (preload) we can’t at-tain the stretch on the muscle fibers of the heart. And that can lead to inad-equate pumping. Starling’s Law of the Heart states that increasing the stretch on muscle fibers will increase the force of contraction. Think of it as a rubber band: the farther you pull it back (or stretch it) the farther it will fly (and the more it stings if it hits you!).
Beta 1 receptors are located within the myocardial tissues of the heart. Stimula-tion of these receptors causes an increase in heart rate (chronotrophy) and contractility (inotrophy). The increase in heart rate and contractility causes a subsequent increase in cardiac output, with the unwanted side effect of increased myocardial irritability (think arrhythmias).
Isuprel® (isoproterenol hydrochloride) is a medication with pure beta properties to increase heart rate and contractility. It’s commonly utilized as an ectopy stimulating agent in electrophysiology studies, thereby earning its reputation as a “chemical pace-maker.” It also demonstrates the beta 2 properties of vasodilatation, which can lead to a drop in blood pressure.
In contrast, Levophed® (norepinephrine) is a drug with both alpha and beta proper-ties. It increases BP, systemic vascular resist-ance (SVR), cardiac output and heart rate. It provides excellent hemodynamic support in critically ill patients.
Beta 2 receptors, located in the lungs, cause bronchodilatation and arterial dilata-tion when stimulated. Albuterol and terb-utaline -- two types of prescribed inhalers -- are beta 2 agonists used to treat bronchos-
pasm in patients with chronic obstructive pulmonary disease (COPD).
As we’ve already noted, beta 1 stimulation works on the heart. And that’s why, when a patient receives a respiratory treatment, his heart rate increases. In most nebulized agents, the medication contains both beta 1 and beta 2 agonists. So we end up with nicely opened lower airways, but an in-creased heart rate compared to baseline.
Dobutrex® (dobutamine), which is used for heart failure patients, has both beta 1 and beta 2 properties. The beta 1 side increases contractility, or positive inotropic effect, to improve cardiac output, while the beta 2 arterial dilatation effect causes a decrease in preload and afterload. In other words, the two-inch pipe is now four inches.
This reduction in afterload yields less pres-sure for a failed heart to pump against, de-creasing its workload while simultaneously increasing its ability to contract.
Helpful hint for remembering receptor sites: you have one heart: so beta 1. You have two lungs: thus beta 2.
Beta blockers are an entire class of medi-cations dedicated to blocking beta receptor sites. They’re routinely indicated for acute coronary syndrome (ACS) patients. Beta blockers decrease cardiac arrhythmias, heart rate and blood pressure, thereby decreasing myocardial oxygen demand. For this rea-son they’re also used for blood pressure and heart rate control.
Helpful hint: beta blockers should be used with caution in patients with COPD and asthma: remember if you block beta 2, bronchodilitation bronchospasm could be life-threatening in the presence of beta blockade. Beta blockers should not be used in the presence of any atrioventricular (AV) block.
CORONARY HEART ™ 31

EDUCATION
Another example of beta blockade: when one of my friends has to speak publicly, she develops a redness that begins at her chest and incrementally creeps up her neck to her face. It looks as if her heart is literally pounding out of her chest! People like her benefit from prophylactic beta blockade: she took Inderal® (propanolol) before mak-ing speeches and also before her wedding.
Lopressor® (metropolol) is the beta block-er most commonly administered to patients in the cath lab or ED as part of the acute coronary syndrome (ACS) protocol.
Helpful hint for remembering which meds are beta blockers: most end in “lol.”
Now that we’ve explored the sympathetic receptors and actions of alpha and beta stimulation, it’s clear why epinephrine -- a sympathomimetic drug -- is the first-line advanced cardiac life support (ACLS) medication.
Let’s assume your patient has cardiac-ar-rested: there’s no perfusing rhythm, no BP, no cardiac output. Epinephrine will vaso-constrict peripheral arterioles and venules, shunt peripheral blood back to the heart in an attempt to raise blood pressure/sys-temic vascular resistance, and stimulate the beta properties of increasing heart rate and stroke volume.
Epinephrine is also the first-line treatment for anaphylaxis, either in the cath lab for contrast allergy, or as an Epi-Pen® for people who are allergic to bee stings.
Dopaminergic receptors, located in cor-onary arteries and renal and mesenteric blood vessels, cause dilation of kidney and mesenteric arteries.
Inotropin® (dopamine) is one medication with dose-dependent action. At low dose (0.5-2 mcg/kg/min), dopaminergic recep-tors are stimulated and renal perfusion is increased. At median dose range (2-10 mcg/kg/min), Inotropin exerts beta effects of increased heart rate and contractility. At the highest doses,(>10mcg/kg/min), the ef-fect is alpha, with peripheral vasoconstric-
tion that raises blood pressure. At this dose Inotropin will have vasopressor, inotropic and chronotropic effects and may increase myocardial oxygen demands on the heart.
Helpful hint: if an IV line infiltrates with Inotropin it can cause sloughing of the skin due to its alpha peripheral constrictive properties. To prevent tissue necrosis, treat as soon as possible with a Regitine® (phentolamine mesylate) injection around the periphery of the infiltration.
A sympathetic wrap-up. Think about the appearance and vital signs of acute MI pa-tients: they’re afraid they’re going to die, so their “fight or flight” response is stimulated and their sympathetic system is in over-drive.
This is first evidenced by cool, clammy skin caused by alpha stimulation and pe-ripheral vasoconstriction: that’s why their skin is cold, not hot. They may even have a gray or ashen color.
Second, their heart rate (HR) is elevated in part by beta 1 stimulation. The infarcted portion of the myocardium (the ventricular muscle mass) results in a diminished ability to pump effectively, decreasing the stroke volume (SV) and myocardial oxygen sup-ply.
Our bodies work hard to maintain home-ostasis and adequate cardiac output (CO). The equation CO = HR x SV says that or-gan perfusion pressure or blood pressure must remain adequate to perfuse the brain, heart and major organs. If there’s a drop in stroke volume due to myocardium injury, heart rate must increase to compensate for the decreased stroke volume.
Oxygen is required each time the heart beats. A compromised myocardium is al-ready in oxygen deficit, and an increase in
AND THE BEAT GOES ON (cont...)
Generic Brand Name
Metropolol Lopressor®
Labetelol Trandate®
Esmolol Breviblock®
Propanolol Inderal®
Atenolol Tenormin®
Sotalol Betapace®
Figure 2: Commonly Used Beta Blockers
32 CORONARY HEART ™

EDUCATION
heart rate from beta stimulation puts fur-ther oxygen demands on the heart. That’s why your acute MI patient benefits from the administration of a beta blocker like Lopressor®: the beta-blocking action lowers the heart rate, allows for more ventricular filling time, decreases myocardial oxygen demand, improves cardiac output, and may help with arrhythmia suppression.
All about the Parasympathetic Nervous System
The parasympathetic nervous system is the “rest and digest” or “feed and breed” part of the autonomic nervous system. The parasympathetic system innervates the heart via the vagus nerve, or cranial nerve X. The neurotransmitter responsible for parasym-pathetic stimulation is acetylcholine.
This innervation is limited to the sinoatrial (SA) node and the atrioventricular (AV) junction. There’s very little influence on the ventricles or blood vessels. Parasympa-thetic stimulation causes a decrease in heart rate and impulse conduction in the heart. Figure 3 details parasympathetic effects elsewhere in the body.
We see the effect of stimulation of the
The Autonomic Nervous System
Structure Sympathetic Stimulation Parasympathetic Stimulation
Iris (eye muscle) Pupil dilation Pupil constriction
Salivary Glands Saliva production reduced Saliva production increased
Oral / Nasal Mucosa Mucus production reduced Mucus production increased
Heart Heart rate and force increased Heart rate and force decreased
Lung Bronchial muscle relaxed Bronchial muscle contracted
Stomach Peristalsis reducedGastric juice secreted; motility increased
Small Intestine Motility reduced Digestion increased
Large Intestine Motility reduced Secretions and motility increased
LiverIncreased conversion of glycogen to glucose
Kidney Decreased urine secretion Increased urine secretion
Adrenal MedullaNorepinephrine and epinephrine secreted
Bladder Wall relaxed and sphincter closedWall contracted and sphincter relaxed
Figure 3: The Autonomic Nervous System
CORONARY HEART ™ 33

EDUCATION
parasympathetic system in the cath lab and recovery area every day. It may happen when the physician is gaining vascular ac-cess, sheaths are being pulled, or pressure is being applied to the groin. The heart rate drops and BP falls. The patient becomes diaphoretic and nauseated. And we say the patient is having a vagal response.
What should we do first? Administer a drug to block the parasympathetic stimula-tion. The drug of choice is atropine, a para-sympathetic blocker. Atropine is usually dosed at 0.5-1 mg IV per physician’s order (A caution: doses of less than .5 mg or more than 2.5 mg can cause a third-degree heart block).
This is why having atropine readily avail-able at the bedside is part of many institu-tions’ sheath-pulling policies. It should be the first mode of action in a vagal response, followed by placing the patient in Trende-lenburg position and fluids.
Remember groin anatomy of nerve (vagus), artery, vein, ligament. Releasing pressure is not an option until hemostasis is accom-plished. Atropine is indicated in sympto-matic bradycardia, asystole, and pulseless electrical activity (PEA). Patients who re-ceive atropine will experience dry mouth and pupil dilatation.
You’ll be interested to learn that atropine occurs naturally in the deadly nightshade plant, or Atropa belladonna. The plant gets its name from the Italian word for “beau-tiful lady” (bella donna): Renaissance-era women used an extract of its berries to di-late their pupils for cosmetic reasons. And US soldiers carry atropine as the antidote for nerve gas exposure.
In Part II in the next issue we’ll review the major antihrombotic medications, their mode of action, and 2007 ACC/AHA rec-ommendations. And we’ll find out what happened to the patient we talked about at the beginning of this article.
Editor’s Note: The information presented in this article is intended to serve as an educa-tional aid only and provide the reader with a reference; it is not intended to offer medical advice nor substitute medical practice, diag-nosis and/or treatment. The ultimate respon-sibility for patient care resides with the health care professional using his or her professional license, experience, and knowledge of the pa-tient. All products are registered trademarks
by their respective manufacturers, and are ap-proved for use in the United States. Please check with your local government or regula-tory agency for additional information. Dos-ing and/or pricing information is direct from manufacturers; please consult with appropri-ate package inserts or information before ad-ministering any medication or pharmacologic agent listed in this article.
AND THE BEAT GOES ON (cont...)
ECG Quiz Answer from Page 25
The ventricular rate appears at first sight fairly irregular and this could lead to a misdiagno-
sis of atrial fibrillation. Atrial fibrilla-tion is “irregularly irregular” i.e. chaot-ic whereas the QRS complexes in this ECG have an underlying order to them as they are instigated by a regular atrial rhythm. Discrete, identical and repeti-tive atrial depolarisations (marked as F for flutter wave) can be identified. These are conducted to the ventricular in a predominantly one to one fashion but with Wenkebach – occasional flut-ter waves are not conducted as the atri-al rate is just a fraction too fast for the AV node to conduct one to one. There
are groups of regular beats separated by longer intervals – this is sometimes re-ferred to as “group beating”.
One to one (or near one to one) con-duction of flutter usually occurs where the flutter rate is slower than the typi-cal 300 b.p.m. (as in this example). The rate may be slower due to anti-arrhyth-mic medication, slow atrial conduction or a grossly dilated right atrium.
This tachycardia was terminated by ablation of the cavo tricuspid isthmus (CTI) and was demonstrated to be counter clockwise isthmus depend-ent flutter. The patient had right atrial scars from previous surgical incisions but these were not implicated in the arrhythmia.
All references used for this series will appear in Part 2 of this series.
34 CORONARY HEART ™

What if you couldaccess both an angiogram
and a chest x-ray in lesstime than it takes to read
this sentence?
Agfa and the Agfa rhombus are trademarks of Agfa-Gevaert N.V., Belgium, or its affiliates. IMPAX is a trademark of Agfa HealthCare N.V., Belgium, or its affiliates. All rights reserved.
That’s the beauty of integrated medical information. The images and reports you need are at your fingertips and
accessible, whenever and wherever you need them. When seconds matter most, you will be glad that Agfa
HealthCare created the IMPAX® Cardiovascular Suite that facilitates point-of-care data collection and anytime,
anywhere viewing and management of integrated images and information. Our patient-centric approach
consolidates access to secure clinical information, supporting cross-modality and legacy equipment data to help
you improve decisions about patient care. Agfa HealthCare is at work in 1 of every 2 hospitals worldwide, and
because our solution is designed by cardiologists, for cardiologists, you’ll be operating with greater efficiency in
nearly no time at all.
To learn more about our proven healthcare IT solutions,
please visit www.agfa.com/healthcare or booth #18001 at ACC 2008.

CRM
Over the last two years, since the disclosure of safety issues regarding heart defibrillators, device designers, manufac-
turers and the regulators have paid closer attention to tracking device performance once they reach the market.
Pacing leads, which connect pacemakers and defibrillators to the heart, have received particular attention from regulators and the media. These leads are intended to deliver an electric shock, when necessary, to stabi-lise a dangerously erratic heartbeat and as such are a major component to the set-up of a pacemaker or defibrillator.
In Europe over 750,000 leads to pacemak-ers and defibrillators are implanted into patients every year. Of these leads it is es-timated that between 4 and 7 per cent will have to be removed at some point due to damage, infection or the inability to im-plant new leads due to the presence of exist-ing ones.
Since the commercial introduction of im-planted transvenous pacing leads, a wide variety of methods for removing leads have been developed and today the main lead extraction technologies are either laser pow-ered or mechanical.
Evolving Technology and Techniques
In the years following the introduction of chronically implanted transvenous pacing leads, a variety of methods for lead removal were trialled, the simplest being traction, often also called the “drag through” tech-nique. For patients with significant fibrous overgrowth, more aggressive methods had to be developed, including traction applied by weights and elastic bands among other methods.
Nonetheless, complications and difficulties encountered when using traction for lead removal led some investigators to surgical approaches, whereby the heart and great veins were exposed via sternotomy or thora-cotomy allowing extraction of a lead via an incision in the atrium or ventricle. In great-ly experienced hands, these techniques pro-duced high success rates, but required high-ly specialized skills gained through years of training. In addition, these techniques were associated with morbidity and the heavy economic impact of open surgery.
The desire for safe and more economically viable extraction techniques led to the de-velopment of intravascular counter-pres-sure and counter-traction – using telescopic
sheaths made of polymer and /or steel ma-terial, which would slide over the lead body. This technique removes the fibrotic tissue that develops over time and entraps the implanted lead in the veins. As the sheaths are advanced over leads to tear and peel away the encapsulating tissue they achieve a transvenous removal of leads with mini-mised risk to the patient compared with previous methods.
Today’s Choices
The procedure of lead removal has matured into a definable, teachable art with its own specific tools and techniques. Today’s tech-nology offers two main technology options
Leads to The Heart – An Extraction Evolution
In this article, Barry Norlander, Global Marketing Manager for Cook Vascular Strategic Business Unit, outlines current treatments and best practice lead extraction techniques and technology.
36 CORONARY HEART ™

CRM
for surgeons performing extractions – laser and mechanical.
Laser extraction requires a 600 pound (250kg) stand alone unit to interface and power an SLS laser sheath, with each sheath requiring complex calibration before each use. Heavy machinery like this requires support by way of annual maintenance and biomedical inspection as well as the require-ment to employ an on-site laser officer. Put simply, it’s bulky, costly both in terms of operation, training and maintenance. The other option is to use a mechanical ap-proach. This offers benefits in that it requires less surgical finesse and is more intuitive to use than laser powered systems. It is also designed to negotiate chronic, heavily fibro-sed and calcified lesions without requiring the ‘brute strength’ of traction.
An enhanced mechanical extraction ap-proach doesn’t have the forward depth of cut like laser extraction sheaths. With this in mind, mechanical extraction historically
has had a lower adverse event rate than that experienced using powered sheaths.
Today’s mechanical lead extraction technol-ogy has been designed to be as intuitive as possible for the surgeon specialist during a procedure. Lead extraction, which goes a long way in addressing device-related com-plications, has progressed, particularly as clinicians are more aware of the risks and complications associated with some of the techniques previously used. Mechanical techniques allow for greater success rates, thus making the patient’s journey also a much safer and enjoyable one.
Devices like the EVOLUTION® Mechanical Dilator Sheath Set consists of a flexible rotating sheath that succinctly separates fibrous binding sites from the leads that need extracting. The inner, ex-otic braided polymer sheath, shielded by an outer telescoping polymer sheath, connects to a handle, or trigger, which rotates it me-chanically. It’s this mechanical trigger that
allows the user to better feel progress along the lead and through lesions, thereby max-imising physician control.
While extraction of chronically implanted leads has been difficult in the past, this seems to have been addressed with mechan-ical techniques, which have been proven to remove the scar tissue along the vein that is often the primary reason for partial or failed removal of a lead.
An Exciting Evolution
Lead extraction device manufacturers have a responsibility to provide the best, most ver-satile devices that provide safe, timely and effective treatment for the patient, and are easy-to-use devices for surgeons. Addition-ally, the need to reduce the financial burden of acquiring the best possible technology on health organisations has to be reduced. It’s exciting to see the benefits that the lead extraction evolution will deliver to health providers, doctors and patients.
CORONARY HEART ™ 37

CONFERENCECALENDER
March 26 - 28
ACCA 19th Cardiovascular Administrators’ Leadership ConferenceChicago, IL
www.aameda.org
May 14 - 17
Heart Rhythm 2008 - 29th Annual Scientifi c SessionsSan Francisco, CA
www.hrsonline.org
March 27 - 29
ACVP 2008 Cardiovascular Leadership ConferenceChicago, IL
www.acp-online.org
May 28 - 31
SCAI 31st Annual Scientifi c SessionsLas Vegas, NV
www.scai.org
March 29 - April 1
ACC 2008 + i2 SummitChicago, IL
www.acc08.acc.org
July 11 -12
4th Annual Heart & Vascular ConferenceBoyne Falls, MI
www.northernhealth.org/lubdub&splash
April 7 - 10
Concepts in Contemporary Cardiovascular Medicine SymposiumHouston, TX
www.aievolution.com/ccm0801
July 26 - 29
14th World Congress on Heart DiseaseToronto, Canada
www.cardiologyonline.com
May 4 - 6
17th Annual All That Jazz - Nurse/Tech CourseNew Orleans, LA
www.allthatjazz.org
September 10 - 13
9th Annual New Cardiovascular Horizons New Orleans, LA
www.newcvhorizons.com
Upcoming Issues
May / June 2008
Cardiac CT
Contrast Induced Nephropathy
Cardiovascular Pharmacology (Part 2)
Beginner Series (Part 1): Sheaths
Interview: Jeffrey G. Knox, Cardiology Operations Manager, University of Maryland Medical Center
Site Visit: Baton Rouge Cardiology Center, LA
July / August 2008
Mobile Cath Labs
Beginner Series (Part 2): Wires
Cardiac Monitoring Systems
Site Visit: Memorial Hermann Southwest Heart & Vascular Institute, TX
Media Kits available at www.coronaryheart.com
•
•
•
•
•
•
•
•
•
•
38 CORONARY HEART ™

CORONARY HEART ™ 39

WE PRACTICE CARDIAC NURSING ATA HIGHER LEVEL. SARAH’S.Every day Sarah’s able to focus on caring for patients at the bedside, and at the sametime grow her career at Pitt County Memorial Hospital. Nurses like Sarah are part ofour leadership and have made us the region’s healthcare leader.
www.pcmhcareers.com/heartGet the full story of our Nursing family at:
• Exceptional Greenville, NC location
• Magnet certification and clinical ladders
• Flexible shift and schedule options
• Ongoing expansion across our system,which includes the opening of the EastCarolina Heart Institute in 2009
• Training and education at every level
We are diverse talents brought together by a common dedication: EOE.