Coronary Heart #12 US
40
coronaryheart.com E M P L O Y M E N T Subscribe Free Online coronaryheart.com Special Feature Drastic Cuts in Medicare Reimbursement Would Close Cath Labs Interview Jeffrey Knox University of Maryland Medical Center Management Cardiac CT - Benefit or Risk Education A review of lifesaving and antithrombotic drugs (Part 2) Site Visit Baton Rouge Cardiology Center, LA Contrast Media Contrast-induced Nephropathy May / June 2008 Issue 12
-
Upload
cardiologyhd -
Category
Documents
-
view
237 -
download
4
description
Coronary Heart May / June 2008
Transcript of Coronary Heart #12 US

coronaryheart.com
EMPL
OYMENT
SubscribeFree
Online
coronaryheart.com
Special FeatureDrastic Cuts in Medicare Reimbursement Would Close Cath Labs
InterviewJeffrey KnoxUniversity of Maryland Medical Center
ManagementCardiac CT - Benefi t or Risk
EducationA review of lifesaving and antithrombotic drugs (Part 2)
Site VisitBaton Rouge Cardiology Center, LA
Contrast MediaContrast-induced Nephropathy
May / June 2008Issue 12

That’s the beauty of integrated medical information. The images and reports you need are at your
fingertips and accessible, whenever and wherever you need them. When seconds matter most,
you will be glad that Agfa HealthCare created the IMPAX® Cardiovascular Suite that
facilitates point-of-care data collection and anytime, anywhere viewing and management of
integrated images and information. Our patient-centric approach consolidates access to secure
clinical information, supporting cross-modality and legacy equipment data to help you improve
decisions about patient care. Agfa HealthCare is at work in 1 of every 2 hospitals worldwide, and
because our solution is designed by cardiologists, for cardiologists, you’ll be operating with
greater efficiency in nearly no time at all.
To learn more about our proven healthcare IT solutions, please visit
www.agfa.com/healthcare
Agfa and the Agfa rhombus are trademarks of Agfa-Gevaert N.V. or its affiliates. All rights reserved.
PROJECT INFORMATION FILE INFORMATION PRINTING INKS INTERNAL APPROVALSTARGETS/TINTS
Client:
Project:
Docket #:
Live Area:
Final Size:
Print Process:
Colours Available:
Line Screen:
Pre-press/Printer:
Agfa
Access Ad Resize
AGFA2178
N/A
8.125” x 10.875”
Litho
4-CMYK
N/A
Coronary Heart
File Name:
Job Folder Name:
Software/version:
Fonts Used: BosisforAgfa, CharterITCforAgfa
Client is responsible for checking all copy before project prints. Colour separators, pre-press service bureaus and/or printers are responsible for verifying all technical/mechanical specifications, including but not limited to tolerances, registration, accuracy of measurements and construction details before film and plates/cylinders are generated. Any changes to accommodate print requirements must be submitted to client for approval. Milestone makes every reasonable effort to ensure all artwork is error-free; however, we cannot be held responsible for any errors present once client provides final sign-off.
Cyan
101 King Street West, Cambridge, Ontario Canada N3H 1B5 T 519.653.2654 F 519.653.5941 milestoneadvertising.com
M I L E S TO N E A D V E R T I S I N G / D E S I G N
Magenta Yellow Black
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000C
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
Pantone0000 C
(Process Target)
MILESTONE TEAMADDITIONAL INFORMATION PRODUCTION FILE HISTORY PROOF NUMBER
Production Artist:Production Manager:Proofreader:Designer/Creative Director:Account Director:
October 11, 2007
October 11, 2007
October 11, 2007 2
Artwork Approved:
Production Artist:
Production Manager:
Proofreader:Designer/Creative Director:
Account Director:
Y/N DateInitials
Start Date:
Date Last Modified:
Date Released:
TomDianeDianeHeather/LauraJohn
• This is a digital colour mechanical, no traps have been made. Trapping to be applied by separator.• This proof/PDF is for colour break and content only and may not accurately reflect final printed inks.• Do not open this file with software and version other than that specified.
NOTES:
• This mechanical artwork has been prepared size as - 100%
AGFA2178_AccessAd_CH.ai
AGFA2178 Access Ad Resize
Adobe Illustrator CS3, Macintosh
©2007

May / June 2008
CONTENTS
02 AGFAwww.agfa.com/healthcare
0� Wavemarkwww.wavemark.net/chm
11 Healthworkswww.healthworksonline.cc
18 Braccowww.bracco.com
40 RADIwww.radi.se
04 Editorial
0� Latest News
08 Special Feature‘Drastic Cuts in Medicare Reimbursements Would Close Cath Labs’
12 Management‘Cardiac CT - Bene� t or Risk for Cardiovascular Programs’
14 Interview‘Je� rey Knox - University of Maryland Medical Center’
21 Contrast Media‘Contrast-Induced Nephropathy’
24 Site Visit‘Baton Rouge Cardiology Center, LA’
2� Education‘A Review of Lifesaving and antithrombotic drugs (Part 2)’
38 Calender & Next Issue
3� Employment
THIS EDITION
ADVERTISERS
Table of Contents
Baton Rouge Cardiology Center, LA
Page: 24
CORONARY HEART ™ 3

From The Editor
Disclaimer:Coronary Heart should never be regarded as an authoritative peer reviewed medical journal. Coronary Heart has been designed as a guide only, to inform readers who work in the cardiology environment about latest news stories and the diff erent techniques used by others around the world. Whilst all care is taken in reviewing articles obtained from vari-ous companies and contributors, it is not possible to confi rm the accuracy of all statements. Th erefore it is the reader’s responsibility that any advice provided in this publication should be carefully checked themselves, by either contacting the companies involved or speaking to those with skills in the specifi c area. Opinions expressed by contributors are their own and not necessarily those of their institution, Coronary Heart Publishing Ltd or the editorial staff .
Coronary Heart Publishing LtdIndependence Wharf
470 Atlantic Avenue, 4th fl oorBoston, MA 02210
United States
Email: [email protected]: +1 (617) 273-8012
Visit us online at www.coronaryheart.com
Director / Chief EditorTim Larner
Clinical EditorDr Simon Redwood
Consulting EditorsDr Richard Edwards
Ms Voncile Hilson-MorrowMr Ian Wright
GENERAL ADVERTISING
Brett Goldine:[email protected]
RECRUITMENT ADVERTISING
CIRCULATION
USA edition
9031 Cardiac Professionals
Copyright 2006 by Coronary Heart Publishing Ltd. All rights reserved.
Material may only be reproduced by prior arrangement and with due acknowledgment of Coronary Heart Publishing. The publication of an advertisement
or product review does not imply that a product is recommended by Coronary Heart Publishing Ltd.
Subscribe Online to get your own
free copy
EDITORIAL
Special Thanks
Door to Balloon
I must be honest that when I fi rst heard of a door to balloon time of 90min a while back, I thought that it would be an easy target. However with speaking to many at the con-ferences it is actually quite diffi cult for some. You see where I trained in Australia we con-sistently had a D2B of less than 30min which I thought was normal. How did we achieve it?
Firstly the paramedics would call into our emergency department stating they had an MI on route. Straight away the oncall team were called, in which we had 30min to arrive. Any person whom lived further away were not able to cover call. Two nurses, one radiographer, and a tech were called, and each knew how to turn each others equipment on, enter details, or get the drug keys. Th is saved valuable time. We weren’t generic trained but had knowledge of the basics to get by before the patient arrived, or even before other staff members arrived.
Upon arrival normally the patient directly bypassed the emergency department, or briefl y stopped to see the cardiologist, and brought straight to the cath lab where we were waiting with slide board ready and emergency names in the system to be fi lled in correctly later. Th is worked extremely well, and as a result I think our department had a great success rate. Our cardiologists were brilliant to work for and coped well under pressure which is important when working often under extremely diffi cult cir-cumstances, as it is one less thing to worry about, allowing you to concentrate and work faster.
Although I produce this publication I still often can be found working in various departments around London. Th e amazing sense of teamwork and compassion, and the thrill of working in emotionally diffi cult situations defi nitely brings the best out of us, which I am sure you all understand.
- Tim Larner
Mr Tim LarnerDirector / Chief Editor
4 CORONARY HEART ™

LATEST NEWS
Coronary Heart spoke with Dr Liam Hughes, Consultant Cardiologist at Norfolk and Norwich University Hospital after returning from his teams record breaking row across the Atlantic Ocean.
What was the reason for doing the row?Nearly 2 years ago the planned expansion of the cardiac unit at the Norfolk & Nor-wich NHS Trust was put on hold due to a financial shortfall in the Trust. Frustrated by this we brokered a deal whereby the Trust would provide £ 1.7 million if a further £1 million could be raised by charitable dona-tions. I co-founded an appeal and decided I should make a personal contribution to raise money and came up with the idea of rowing the North Sea. I achieved this in July 2007 and was then approached by an internation-al team attempting to break the 15 year old transatlantic rowing record. At the age of 54 being given an opportunity to break such a record was too tempting to turn down. My wife was very supportive but it took an
enormous amount of wrangling to get the unpaid leave from my Trust. Some reward for raising £900,000 so far but such is the brave new NHS!!
How much fundraising do you require?We hope to reach our £1 million target in the summer and the second lab is already operational if not officially opened.
What was it like to row across the Atlantic?The row was as hard as one might imagine with a 2 hours on 2hours off rota round the clock for the entire crossing. Despite being held up in a storm for 3 days we took 2 days off the French held record.
What is the current situation of your department?We now have 2 cath labs here which are situ-ated 10 metres from the 10 bedded CCU. We are starting a rescue service in the near
future and hope to have a primary PCI serv-ice before too long. Our geographical posi-tion slap bang in the middle of the region makes us an ideal site.Our aim is for 1,000 PCI’s pa by 2009.
What was the biggest lesson you learnt from the trip?There were so many lessons from the cross-ing but a recurring thought is that a lot of people might benefit from spending some time in a small boat in a big ocean with only their own resources to get them home. I am thinking politicians and policy makers be-cause being out there concentrates the mind on what matters and what doesn’t.
For more details visit www.balloons4hearts.co.uk
UK Cardiologist Breaks World Record to Raise Money for Cardiac Unit
We are pleased to announce that Ian Wright, our Clinical Editor for EP and his wife Ria have become parents.
Their new daughter Deia Nell Wright was born on 14th January 2008. We wish them all the best for the future.
Congratulations
CORONARY HEART ™ �

LATEST NEWS
Outgoing President’s Message
First and foremost I must say it has been a privilege to represent you as the President of the SICP. It is with mixed feelings that
I write my last message to you. I am a little sad that my two years have gone by so fast, but very excited about the impact and energy that Todd Chitwood brings to the position.
The last two years have been a whirlwind of ac-tivity and growth for our Society. The progress we have made is incredible. Collaboration with Industry has been a big focus. We have built relationships that will continue to support our mission and goals. The chapter initiative will continue to build a strong foundation for our profession. As more chapters form, more people will get involved and influence how the invasive cardiovascular profes-sional will practice.
As I thought about what my last President’s mes-sage would be, I remembered an essay I wrote several years ago about professionalism in the face of a changing environment. As I read it, I realized that we are facing yet another big change in healthcare. Back then, the changes were managed care and hospital mergers creat-ing huge corporations. Today, it is more regula-tory involvement (National Patient Safety Goals, Compliance, etc.!) and the division of roles in our environment. It is our responsibility to keep up with the changes, while making sure that we keep quality care and excellent patient outcomes as our primary focus.
Change is always an opportunity for growth. We are in the perfect position to impact how our profession will evolve to keep up with these changes. By effectively advancing ourselves to a position that has the ability to make a difference, we will shape our own future. As our profession continues to advance, each of us will determine how we will respond to increasing demands.
As a strong voice, we have the ability to set the standards. By positioning ourselves as the au-
thority in our own unique environment, we will maintain what we have evolved into, an in-tegrated and cohesive mix of professionals that each contribute their expertise in the care of the patient undergoing invasive procedures.
As procedures evolve to less invasive techniques, we will find ourselves collaborating with even more disciplines. This is already happening with the emergence of hybrid rooms in operating and radiology departments. Again, this is an oppor-tunity for growth. We must remember that, as the experts in our field, we are compelled to set the standards for patient care.
I admire those of you who have chosen to get involved with your society during the last few years. Your success in building chapters prove there is a need for educational opportunities as well as networking and fellowship. You are impacting not only patients and peers, but your communities.
So….my challenge to you is to continue to take care of patients and each other. Get involved ei-ther locally or nationally with your society. The SICP exists because of you!
July 31-August 2, 2008
FeaturingDr. Morton J. Kern,
MD, FSCAI, FAHA, FACCClinical Editor, Clinical Professor of Medicine
Associate Chief CardiologyUniversity of California Irvine
Hemodynamics in the Cath LabAngiographic Challenges
FFR complications… and more!
Dr. David E. Allie, MD, FACS, FACC, FACA, FCCP
Chief of Cardiothoracic and Endovascular Surgery, Cardiovascular
Institute of the South, Lafayette, LA
Diagnostic Imaging for PVDCritical Limb Ischemia (CLI): The Current
Status of Interventional Therapies The “CLI Tool Box”
Detailed Program Information Coming Soon!
Please call 800-901-5188 or 888-458-8471 to make hotel reservations and refer to the group code when making your reservations. The SICP group code is SHSIC8, and the cut-off is Monday, June 30, 2008. Harrah’s has also created this internet link for Online booking:
https://www.harrahs.com/CheckGroupAvailability.do?propCode=LAS&groupCode=SHSIC8
www.sicp.com
Lynne Jones RN, RCIS, FSICP
� CORONARY HEART ™

LATEST NEWS
chm
Imagine this – your enjoying a normal day when with-out warning you pass out and wake up in a hospital. You are informed that your heart rate is in the 30’s
and to live you will need a pacemaker. However you live in a developing country and have very limited resources. You cannot afford the device that would save your life or the life of your child or spouse. One to three million times per year this story is someone’s reality.
Heartbeat International, a Florida based non-profit or-ganization, answers this call for life by providing new car-diac pacemakers, as well as implantable defibrillators and cardiac resynchronization devices, and all of the related physician and hospital expenses – all at no charge! That’s right – the procedure that can cost $60,000 in the U.S. is free for needy patients in developing countries.
Over 9,000 lives have been saved since Heartbeat Inter-national began its mission in 1984. It is not difficult to imagine that in addition to saving lives, providing futures and returning loved ones to family and friends, Heartbeat International uses Pacemakers as Peacemakers; fostering international understanding, goodwill and friendship.
In March 2008 Coronary Heart officially endorsed the non-profit organization Heartbeat International. Over the next twelve months we will bring you patient stories and how you can become involved.
Janeth Belmores Colungo Life saved May 13, 2002
[email protected] www.heartbeatintl.org
CORONARY HEART ™ �

SPECIAL FEATURE
Drastic Cuts in Medicare Reimbursement Would Close Cath Labs
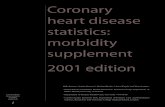
Fed up after waiting days for a cardi-ac catheterization, John G. walked out of the hospital in his Arkansas hometown. He drove three hours
to the Little Rock Cardiology Clinic for the procedure. John (not his real name) arrived at the clinic, and over the next few hours not only underwent cardiac catheterization, but all the other diagnostics needed to plan the endarterectomy he needed for an oc-cluded carotid.
Unfortunately, John and tens of thousands of patients like him each year may soon lose the benefits of such rapid service and lower costs of non-hospital cardiac catheterization labs. A proposed drastic cut in Medicare re-imbursement would render most of the 80 to 100 such labs uneconomic, forcing them to close, said clinic administrators.
The problem first arose in 2006, when the Centers for Medicare and Medicaid Serv-ices (CMS) of the Department of Health and Human Services proposed to change how Medicare reimburses for a number of diagnostic procedures, including non-hospital outpatient cardiac catheterization. The CMS administers Medicare and other federal health-related programs and works with the state government to administer Medicaid.
“I am concerned that the severe reimburse-ment cuts initiated by CMS for non-hos-pital outpatient cardiac catheterization lab procedures in 2008 to 2010 will threaten access and quality of care for the Medicare beneficiaries in my state and throughout the nation. I believe that CMS should review the extensive materials that the Cardiovas-cular Outpatient Center Alliance (COCA), a national organization representing the labs, has provided to them and establish reasonable reimbursement that will allow these important patient care facilities to stay in business,” said U.S. Senator Mary Landrieu (D-La.).
Cardiology clinic administrators criticize the new CMS reimbursement rules as un-realistic, because they would eliminate the category of more skilled, higher-paid tech-nologists and nursing staff needed to oper-ate cardiac cath labs. Also, the new rules do not allow for the sophisticated infrastruc-ture, equipment and supplies needed for such procedures, said the administrators. In essence, the new rules treat cardiac cath labs more like physician’s offices, rather than so-phisticated diagnostic facilities.
“The support that a cath patient needs is far more elaborate than an office-based proce-dure,” pointed out Karen Engelhardt, exec-utive director of Louisiana Cardiology As-
sociates, in Baton Rouge, LA. “It’s not just a case of a nurse walking in and doing an assessment and walking out. The nurse may have to examine or pull a catheter sheath, or monitor the patient’s groin to make sure there is no hematoma or bleeding. And this monitoring is continuous, sometimes up to 17 hours.”
Under the rules, to be phased in by 2010, Medicare compensation for cardiac cath procedures would drop by about half, said Steve Blades, president of COCA.
“If these draconian cuts go through, cardiac caths will be reimbursed at a level several hundred dollars less than they cost to per-form,” he said. “This means that firstly, the clinics can’t afford to do Medicare cases anymore; and then if the commercial insur-ance companies follow the reimbursement, outpatient cath labs will be put out of busi-ness.
“The CMS has made us a square peg in a round hole, and they’ve shaved so much off trying to get us to fit, that they will have cut us down below our cost of providing the service,” said Blades. Blades said that re-imbursement for the non-hospital cath labs
8 CORONARY HEART ™

SPECIAL FEATURE
has already been cut by about 20 percent as of January 2008.
Dan Caldwell, CEO of the Little Rock Car-diology Clinic, said his facility exemplifies the squeeze facing the non-hospital clinics.
“We are already down 15 percent in our revenues for cardiac cath this year, and the payment cuts scheduled for next year will put us close to break even. The final 2010 cuts will put us below our costs. It would put us out of the catheterization business,” said Caldwell.
Even those facilities that managed to keep their cath labs open would lose a key finan-cial base, said Engelhardt.
“Since our cath lab offers expanded services such as device implants and stent placement, it would not close,” she said. “However, we would find ourselves having to support the lab through those procedures.”
Blades estimated that the forced closure of non-hospital clinics would drive 100,000 cardiac cath procedures annually to hospi-tals ill-equipped to handle the load.
“The hospital cath labs are already over-burdened, and it would only get worse,” he said. “The impact on patients would be severe. They would no doubt suffer long delays, not only because of the case load, but because hospital labs appropriately give precedence to emergency patients.”
“In contrast, our outpatient cath labs compared to a hospital lab are much like a birthing center compared to a maternity ward,” said Blades. “We give our patients an accessible, quiet environment that meets their needs.”
Caldwell pointed out that such accessibil-ity is particularly important for cardiac pa-tients.
“Many cardiac patients are older, and be-cause cardiac disease usually is a chronic disease, they tend to be sicker, and many are not well-to do,” he said. “In our state, they have to drive from one to three hours to see a cardiologist, so they really need to get as much done in a single visit as possible.”
Left to right: Fred H. Petty, M.D., F.A.C.C., F.S.C.A.I. – Cardiologist & Tim Derouen, BSRT, (R) at Baton Rouge Cardiology Center, LA
CORONARY HEART ™ �

SPECIAL FEATURE
However, he said, closing cardiac cath labs such as Little Rock’s would force patients to schedule cath procedures separately and endure more long trips, greater travel expense, and extended waits at hospitals. What’s more, since co-payments are higher at hospitals, patients would incur more out-of-pocket medical costs, said Caldwell. Physicians are also better served by the less hectic environment of the non-hospital clinics, he said. “The slower pace and more relaxed atmos-phere means that doctors have more time to spend with patients, to show them the results of their studies and discuss options,” said Caldwell. Engelhardt pointed out that the non-hospi-tal labs also serve physicians by giving them rapid service. “Basically, we’re a one-stop shop,” she said. “We offer all the tools clinicians need to expedite their diagnoses, besides offering patients considerable convenience. For example, in one patient with coronary ar-tery disease his doctor was worried that the vessel might have re-occluded. The doctor
called us in the morning, and we were able to insert that patient into the cardiac cath schedule by noon. In a hospital, the wait would have been many hours, if not over-night.”
The federal health care system also will also incur greater costs because of closures, said Blades. “Cutting reimbursement to non-hospital labs is a false economy,” he said. “The in-creased use of more expensive hospital cath labs resulting from the closure of non-hos-pital labs will cost the federal government millions of dollars in increased health care spending.”
Concluded Martin (Bubby) Fischer, practice administrator for Baton Rouge Cardiology Center in Baton Rouge, LA, “The simple reality is, if CMS does not fix this problem quickly, outpatient cath labs may be forced to close. With looming health care crises in this country, it is more important than ever that our government supports logical, rational choices and delivery systems. The way this issue is currently being handled, there will be millions in increased tax dol-
lars allocated to fund the provision of these same health care services. It is just illogi-cal to increase health care spending, while at the same time limiting patient access for these services, creating longer length of stay for these patient services, increasing out-of-pocket expense to patients, and incurring less desirable patient outcomes. This is why many members of Congress have asked CMS to address this issue,” he explained. Given the many benefits of the non-hospital labs, Blades said that he hopes that “CMS will come to understand that we are an anomaly, and that the rules used for office-based procedures really don’t apply to out-patient cath labs. What we are really seeking is fair and reasonable reimbursement, rather than cutting payments to the point where they are below cost and there is no other choice than to close these labs down.”
For more information on the Cardiovascu-lar Outpatient Center Alliance (COCA), please visit www.cocaheart.org or email Steve Blades, COCA President at [email protected].
Drastic Cuts in Medicare Reimbursement (cont...)
“If these draconian cuts go through, cardiac caths will be reimbursed at a level several hundred dollars less than they cost to perform”
10 CORONARY HEART ™


MANAGEMENT
In life there are always two sides to eve-rything. For most of life’s events, a simple question represents this truth – “Would you like the good news or
the bad news?” For cardiovascular pro-fessionals, we have historically lived in a world with only one side – an ever increas-ing number of Americans stricken with cardiovascular disease. Each year we have seen more disease, more deaths and more opportunity for cardiovascular profession-als to educate and assist in modifying per-sonal choices that increase risk. Add to this the explosion in technology and this has
translated into increased volumes and strong fi nancial margins for cardiovas-cular departments.
In 2007, the good news turned as we saw major reductions in incidence rates and deaths due to cardiovascular disease. Th e National Institutes of Health announced a signifi cant decline in deaths among women down to 1 in 3 from 1 in 4 in recent years. Overall, the American Heart Association announced a 23% decline in deaths among all demographics. Th ese statistics are the direct result of the prevention and early detection programs provided by cardiovas-cular programs, physicians and hospitals. Great results for the American public (good news) and not so great result for hospitals (bad news).
In a direct corollary, cardiac catheterization laboratories, heretofore a source of volumes and revenues, have seen a decline of ap-proximately 20% nationwide in the past year alone. Th is signifi cant decline has gen-erated negative operating margins in both the cardiovascular programs and the overall hospital fi nancial performance.
In the midst of this decline, a new non-in-vasive technology, cardiac CT, has entered the forefront of discussions in cardiovascu-lar programs. Understanding the potential benefi ts and impact of this technology drive many conversations among the manage-ment ranks. Clinical benefi ts have been
proven such as the negative predictive val-ue of 99% while the potential risk looms as well – is this just another force driving volumes out of the cardiac catheterization laboratory?
Cardiologists, in preparation for the poten-tial risk, are moving quickly to adapt to this technological change; attending courses to become credentialed to interpret these stud-ies. Th e result: another cardiology – radiol-ogy “turf” battle over the reading privileges. And so the stage is set for the next challenge to cardiovascular managers – when to enter this market and what will be the impact of this latest non-invasive technology?
Th e answer to the question of ‘when’ is sim-ple: NOW (preferably before the competi-tion). Th e benefi ts of the implementation of cardiac CT are many:
Expansion of current services 1.
Courtesy of G
E Healthcare
saw major reductions in incidence rates and deaths due to cardiovascular disease. Th e National Institutes of Health announced a signifi cant decline in deaths among women down to 1 in 3 from 1 in 4 in recent years. Overall, the American Heart Association announced a 23% decline in deaths among
Cardiac CT – Benefit Or Risk For Cardiovascular Programs?
Tina Brinton is a partner in Cenergy a Washington based consulting company
specializing in the implementation of physician alignment strategies and the strategic development of service lines.
12 CORONARY HEART ™

MANAGEMENT
Enhancement of capabilities such as rule out coronary disease for Heart At-tack programs
Direct consumer marketing opportu-nity for calcium scoring
Platform for physician alignment strat-egy
Physician alignment is key to successful implementation of cardiac CT due to the multidisciplinary capabilities for interpreta-tion. Providing a combined panel of radiol-ogy and cardiology with a common set of credentials and protocols is a fundamental element in a successful cardiac CT service. Secondarily, the ability for economic align-ment by way of joint venture, purchased services and other models provides a second level of alignment between physicians and potentially the hospital.
Therefore, implementing the service is a proven strategy for growing volumes, en-hancing early diagnosis in acute settings and
2.
3.
4.
in aligning multiple physicians to work col-laboratively toward a common goal. With these benefits, why not pursue this immedi-ately? That answer lies in understanding the second component of this equation – what is the impact of the implementation on my cardiac catheterization laboratory and on my program?
On initial glance, it might appear that the implementation of cardiac CT will further reduce the volume of cardiac catheteriza-tion procedures by replacing traditional coronary angiography with CT angiogra-phy. Although strides have been made in this non-invasive technology, traditional coronary angiography remains the ‘gold standard’. Coronary CTA is most useful to determine whether symptoms of chest pain may be caused by a coronary block-age, particularly in individuals that may be at risk, such as those with a family history of cardiac events, diabetes, high blood pres-sure, smokers, and/or those with elevated cholesterol. This benefit allows for quick rule out and rapid mobilization of the acute
interventional team. A significant clinical benefit and a strong marketing tool result-ing in a potential increase in the number of patients through the chest pain center.
The cardiovascular program overall receives several benefits from coronary CT rang-ing from the improved marketing for the chest pain patients through the continued opportunities resulting from the physician alignment strategy. Bringing together the multi-disciplinary team of radiology and cardiology lays the foundation for further collaboration in areas such as endovascular procedures.
Implementing a cardiac CT service opens the door for new services (calcium scor-ing), assists in rapid detection of coronary blockage in the acute setting and provides the framework for a radiology – cardiology collaborative model. With decreasing vol-umes in cardiovascular programs across the country, the tactical deployment of cardiac CT provides a real opportunity to recapture market share.
Courtesy of Siemens Medical Systems
CORONARY HEART ™ 13

INTERVIEW
Cardiology managers are generally a tough lot who have accomplished much. Jeff Knox, by my standards, does not fit into this mould. Yes, he has accomplished much over the course of his 20 year healthcare career, but somehow he has maintained a fun lov-ing disposition and a caring attitude. He told me in this interview he tries to kill with kindness.
Organizational Overview
The University of Maryland Medical Center is a 689-bed teaching hospital in downtown Baltimore, founded in 1823 as the Balti-more Infirmary; the University of Maryland Medical Center is one of the nation’s oldest academic medical centers.
The Maryland Heart Center - located within the University of Maryland Medical Center
- is nationally known for leading the way in diagnosing and managing complex heart disease. The Heart Center’s cardiologists and cardiac surgeons use the most advanced technology and medical therapies to diag-nose and treat the full range of heart prob-lems. The Heart Center was one of the first in the nation to combine minimally inva-sive bypass surgery with stented angioplasty at the same time in a specially outfitted operating room. This “hybrid” procedure enables patients with multiple vessel block-ages to receive the best treatment for each blockage in an efficient way. The cardiolo-gist and cardiac surgeon work side by side and the University of Maryland Medical Center were among the first in the nation to institute this approach. It means patients get the best treatment for their individual needs, with the convenience of having only one procedure.
Jeff please provide an overview of your area of responsibility.
I am the Maryland Heart Center’s cardiol-ogy operations manager. Before taking on this newly developed role three years ago, I had been the cath lab supervisor for 12 years and a cath lab CV tech for the previ-ous five years. My current area of responsi-bility includes cardiac cath, electrophysiol-ogy, echo, EKG, and the Cardiology prep and recovery unit.
There are five supervisory FTEs that assist me in managing our total cardiology work-force of 95 FTEs. We perform approxi-mately 4,000 cardiac caths, 1,000 electro-physiology procedures, 10,000 echos, and over 48,000 EKGs annually.
Cardiac Interview
Jeffrey G. Knox, M.S., R.T. (R) (CV)Cardiology Operations Manager
University of Maryland Medical Center
14 CORONARY HEART ™

INTERVIEW
Describe the impact you have had on your department.
My current role was created to align all areas of cardiology into one collaborative group. With my longevity at University of Mary-land Medical Center and my positive and collaborative attitude, I have been able to infl uence positive changes throughout my department and create strong relationships with my peers throughout the institution. I do everything in my power to have good, positive interactions with everyone. People respect that, even when you may not get it in return. After a while, all people can give back to you is positive, because you have killed them with kindness. I realize this is easy to say and hard to practice. I am hu-man. And, of course, I can’t say it is what I do everyday with every person, but it does work for me on almost every occasion. When it doesn’t, you have to just know you have done your best.
I have tried diff erent ways of orienting new staff in my areas to give them the best tools to succeed. We have tried diff erent ap-proaches to training from our own orien-tation programs internally, to a partnership with a community college for non-invasive and invasive CV programs, and recently, a Healthworks program. In collaboration with the Healthworks educational team we customized a program to meet the needs of several diff erent staff members (RN, RT, and RCIS) to help accelerate their under-standing of the cath lab. We arranged 80 hours of on-site didactic training in two day increments over several weeks. Th is was an extremely successful way to help our staff pursue professional development. Study af-ter study tells us that quality staff education builds the skills, moral and loyalty of your nursing and technical staff .
How would you characterize the morale and working environment of your organization and your area of responsibility?
I play a very important role for my manage-
ment staff in that I am the buff er between the upper administration and my group. I often soften the blow for unexpected changes and diffi cult messages by putting a positive spin on my messages to achieve the greatest outcome. People who don’t know what I can bring to the table may have a hard time knowing what to do with me. I am not one to sit by and be told what to do. I question everything. Often, I have been viewed as “just a tech” by other disci-plines—as I know many technologists and other smaller disciplines can relate to this feeling. Everyone has a voice. I am proud of my accomplishments and always want to project a positive image of my profession. I am a Radiologic technologist with a mas-ter’s degree in Health Administration.
We have a great working environment with-in my management group. I am honored and proud to work with each and every one of them. Th ey are a very talented and skilled group, each bringing something diff erent to the table. We continue to learn a lot from each other. I can honestly say I have a great time with them all. We have a great deal of fun together as we continue to build our group as a highly eff ective team.
Jeff as a leader what is your view of the team concept and the role you play?
A true team is one in which all players par-ticipate. Th e team must be interactive and be true to their convictions. To create this, a high level of trust must be established with-in the team. It is my role as the manager of my group to encourage brainstorming and decision making collaboratively. I thrive on participation in an eff ective team. Th is is where I get my most satisfaction. It is my duty to be the visionary and to introduce the concepts and ideas. Th e toughest part is to manage all the personalities in the group to allow true participation from everyone. Of course, remember you are not the only one with the ideas. Your staff has excellent ideas that need to be heard. Th ey live the issues and have excellent ideas for solutions.
Most importantly, they need to be recog-nized and rewarded for what works best.
Accomplishments and Expertise
What significant accomplishments have been achieved at your direction?
Being in a management position for 15 years, you are bound to come up against huge capital purchases. Th e one that I am most proud of was completely renovating two cath labs and adding our third [at that time]. What I had learned previously was the simplest and most eff ective thing we all know, but often fail to do—involve the ones whom truly matter—the staff . My technical and nursing staff worked with me on every aspect. We walked every step of each lab. I had the contractors spray paint every item on the concrete fl oors before anything was built. Some staff did not want to partici-pate. So I mandated the participation. We had mock codes to make sure that we knew how far the defi brillator was going to be from the patient. We fi gured out how many steps that would take and what would be in the way. Each room was created identical so that whichever room you were in, you could fi nd the stopcock in the same drawer in the same bin on the same side of the room. Th e staff as a group was very proud of the fi nal product.
As our volume grew—like most institu-tions—our physical space did not grow at the same rate. Our recovery area was moved four fl oors up and into a diff erent building from the cath lab as we built our fourth room. Th is created communication issues. We tried resolving it by using the telephone and then tried spectra link charge phones. Due to budgetary constraints, we were un-able to purchase an interactive scheduling software package. So I dealt with what we had—as we all do—I developed procedural room schedules in GroupWise.
Th e scheduling system we developed al-
Interviewed by Ms Voncile Hilson-MorrowCEO Baltimore/Washington Division of Healthworks, Inc.Previous Director of Invasive Cardiology at Washington Heart at the Washington Hospital Center
CORONARY HEART ™ 1�

INTERVIEW
lowed us to all look at the same schedule—cath, EP, EKG, echo, and our Cardiology Prep & Recovery. It also allowed anyone to be granted proxy rights. The first applica-tion gave Maryland ExpressCare (our ambo transportation department) the ability to read and write within the system enabling them to schedule 24/7. This was a great scheduling tool for the outside physicians using our services. At the same time, we de-veloped a color-coded system for the com-munication of the patient status. By looking at the schedule, we know where the patient is physically located and what point they are in their procedural stay without a phone call. GroupWise scheduling has made a huge impact on the overall flow resulting in patient and staff satisfaction.
I have now been working on a much larger visionary plan to create our integrated Car-diology Information System which I find very exciting. We have installed new ver-sions of software in every area of Cardi-ology in the last two years. We now have Witt in the cath lab, Pruka in EP, ProSolv in echo and Muse in EKG. We have been integrating each system with Cerner Pow-erChart. Several systems have gone on our Citrix servers to gain greater access images and reports as we slowly move all images to our enterprise solution with our Radiol-ogy PACS. As you get people to work to-gether and appreciate what each can add to the whole, you have the most success. The process has been extremely successful. Of course, the growing pains are always a factor, but the long-term goal and product make the process worthwhile.
Views and Opinions
Are you a visionary?
Yes, I am the visionary guy. I am the one that is looking for ways to make the to-tal patient experience better as they move through our system. I had been a front line supervisor for many years and understand clearly how to get things done.
I have registered patients, answered phones, scheduled patients, managed a budget, pur-chased large capital expenditures, as well as given excellent patient care as a cardiovas-cular radiologic technologist. I have slowly worked my way up through the ranks, not as someone who necessarily wanted to climb the corporate ladder, but someone who was prepared to take the next step when it came my way. I have been a patient with a poten-tially life threatening illness—all things that have made me the person I am, and want to project to others.
I am able to identify with many different people’s perspectives—a patient, a front desk receptionist, a clinician, a manager, and most importantly, simply a [hopefully] good human capable of seeing the diversity in the world and how to motivate people to do the right thing.
I very much enjoy using my life experiences to create a better, easier world for us all to live. It is important for a patient to have a seamless transition from one clinician to the next.
Left: The Weinberg Atrium
Jeffrey G. Knox - Cardiology Operations Manager Interview (cont...)
1� CORONARY HEART ™

INTERVIEW
Career
What are the “drivers’ in your career?
What drives me has changed as I have gotten older and hopefully wiser. I became a Radiologic Technologist in a hospital-based program in Rockford, Illinois. After gradu-ation, I quickly sought out my next step—the cath lab. I moved to Baltimore, Mary-land and went to the Advanced Imaging Program at Johns Hopkins Medical Center. I was then just 22 years old and wanted to do everything. I had an excellent knowledge base established at Johns Hopkins. The Car-diovascular Diagnostic Laboratories as it was called then performed every procedure
from the neck down—Interventional Radi-ology and Cardiology. What a great experi-ence it was at the time. In 1990, when I moved across the city to the University of Maryland in Baltimore, I became special-ized in cardiac cath only. Once I became the supervisor of the cath lab, I learned a great deal about myself and how to interact with many different professional levels. When I began to realize that I was getting ready for my next step it was apparent that I needed to further my education. I went back to school at the age of 35 and vowed to myself that I would finish my bachelor degree by the time I was 40. It became a very personal goal that I had hoped would pay off in the end. I became obsessed with success in my program. I worked extremely hard and did
well. My strength and confidence grew by leaps and bounds. I went directly into my master’s program and finished both with my five-year goal. What a struggle that was, but what an incredible experience with a group of very professional, wonderful individuals that expanded my mind tremendously. One of the most important things that I need to learn to control is my expectations of oth-ers. This is a true weakness for me. I often have such high expectations of myself that I project those upon others. I know that in order to truly grow and motivate people to their highest potential, I need to allow them to be who they want to be and allow them to aspire to the level they themselves wish to attain.
Cardiologists in the electrophysiology laboratory at the University of Maryland Medical Center correct complicated heart rhythm disorders by using detailed 3-D imaging and robotics, which enhance accuracy and patient safety.
All photos courtesy of U
niversity of Maryland M
edical Center
CORONARY HEART ™ 1�

Visipaque is a trademark of GE Healthcare.
©BDI 2007
Nonionic iodinated contrast media inhibit blood coagulation, in vitro, less than ionic contrast media. Clotting has been reported when blood remains in contact with syringes containing nonionic contrast media. Serious, rarely fatal, thromboembolic events causing myocardial infarction and stroke have been reported during angiographic procedures with both ionic and nonionic contrast media. Therefore, meticulous intravascular administration technique is necessary, particularly during angiographic procedures, to minimize thromboembolic events. As with all injectable contrast agents, the possibility of severe reactions should be borne in mind, regardless of the patient’s pre-existing medical history.
Please see brief summary of Prescribing Information on the following page.
Reference: 1. Solomon RJ, Natarajan MK, Doucet S, et al, and the Investigators of the CARE study. The CARE (Cardiac Angiography in REnally Impaired Patients) study: a randomized, double-blind trial of contrast-induced nephropathy in high-risk patients. Circulation. 2007;115:3189-3196.
The CARE study is the largest, prospective, randomized, double-blind comparison of iso-osmolar iodixanol-320 with low-osmolar iopamidol-370 in high-risk patients.1
Read the CARE study today. Visit CARECIN.comCall Bracco Sales Center at 1-866-282-2895or call Bracco Professional Services at 1-800-257-5181 option #2
We’re shedding more light on CIN.
CARE study: CIN* incidence in at-risk patients1
20
15
10
5
0
% P
atie
nts
With
Incr
ease
in S
Cr
≥25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.43†
9.8%
12.4%
1b.
% P
atie
nts
With
Incr
ease
in S
Cr
≥0.5
mg/
dL
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
20
15
10
5
0
P=0.39†
4.4%
6.7%
1a.20
15
10
5
0
% P
atie
nts
With
Dec
reas
e in
eG
FR ≥
25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.15†
5.9%
10.0%
1c.
* CIN defined as a) an absolute increase 0.5 mg/dL, b) a relative increase 25% in serum creatinine or c) a 25% decrease in eGFR from baseline to 45-120 hours postcontrast.
† P value is not statistically significant.
• There was no statistical difference in the incidence of CIN (SCr 0.5 mg/dL) following iopamidol-370 and iodixanol-320 (see Figure 1a)1
• The rates of SCr increases 25% were not significantly different (see Figure 1b)1
• The rates of eGFR decreases 25% were not significantly different (see Figure 1c)1
New evidence confirms what we’ve known all along.
The CARE study found no statistically significant difference between Isovue® and Visipaque™ in the rate of CIN in high-risk patients undergoing cardiac angiography or PCI.

Visipaque is a trademark of GE Healthcare.
©BDI 2007
Nonionic iodinated contrast media inhibit blood coagulation, in vitro, less than ionic contrast media. Clotting has been reported when blood remains in contact with syringes containing nonionic contrast media. Serious, rarely fatal, thromboembolic events causing myocardial infarction and stroke have been reported during angiographic procedures with both ionic and nonionic contrast media. Therefore, meticulous intravascular administration technique is necessary, particularly during angiographic procedures, to minimize thromboembolic events. As with all injectable contrast agents, the possibility of severe reactions should be borne in mind, regardless of the patient’s pre-existing medical history.
Please see brief summary of Prescribing Information on the following page.
Reference: 1. Solomon RJ, Natarajan MK, Doucet S, et al, and the Investigators of the CARE study. The CARE (Cardiac Angiography in REnally Impaired Patients) study: a randomized, double-blind trial of contrast-induced nephropathy in high-risk patients. Circulation. 2007;115:3189-3196.
The CARE study is the largest, prospective, randomized, double-blind comparison of iso-osmolar iodixanol-320 with low-osmolar iopamidol-370 in high-risk patients.1
Read the CARE study today. Visit CARECIN.comCall Bracco Sales Center at 1-866-282-2895or call Bracco Professional Services at 1-800-257-5181 option #2
We’re shedding more light on CIN.
CARE study: CIN* incidence in at-risk patients1
20
15
10
5
0
% P
atie
nts
With
Incr
ease
in S
Cr
≥25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.43†
9.8%
12.4%
1b.
% P
atie
nts
With
Incr
ease
in S
Cr
≥0.5
mg/
dL
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
20
15
10
5
0
P=0.39†
4.4%
6.7%
1a.20
15
10
5
0
% P
atie
nts
With
Dec
reas
e in
eG
FR ≥
25%
Isovue®-370(iopamidol injection)
n=204
VisipaqueTM 320(iodixanol injection)
n=210
P=0.15†
5.9%
10.0%
1c.
* CIN defined as a) an absolute increase 0.5 mg/dL, b) a relative increase 25% in serum creatinine or c) a 25% decrease in eGFR from baseline to 45-120 hours postcontrast.
† P value is not statistically significant.
• There was no statistical difference in the incidence of CIN (SCr 0.5 mg/dL) following iopamidol-370 and iodixanol-320 (see Figure 1a)1
• The rates of SCr increases 25% were not significantly different (see Figure 1b)1
• The rates of eGFR decreases 25% were not significantly different (see Figure 1c)1
New evidence confirms what we’ve known all along.
The CARE study found no statistically significant difference between Isovue® and Visipaque™ in the rate of CIN in high-risk patients undergoing cardiac angiography or PCI.

≤
Rx only
BRACCODIAGNOSTICS
Rx only
Iopamidol Injection 76%
NOT FOR INTRATHECAL USE
ISOVUE®-200Iopamidol Injection 41% ISOVUE®-250Iopamidol Injection 51% ISOVUE®-300
ISOVUE®-300Iopamidol Injection 61% ISOVUE®-370Iopamidol Injection 76%

CONTRAST MEDIA
One of the leading causes of renal failure for both in-patients and outpatients is contrast-induced nephropathy (CIN) following diagnostic and interventional procedures. As imaging modali-
ties continue to evolve, more patients will be treated and diagnosed with contrast enhanced imagery. CIN varies from 5% to 38% depending on the patients risk factors. So in perspective, a lab performing 1000 plus cases a year puts almost 400 patients at risk for CIN. As cardiovascular professionals working in the lab we rarely see the latent eff ects of our patients once they leave, and their intervention is complete. So we are unlikely to ever see the renal damage that can occur 48 – 72 hours following these cases. Th e only eff ects we may ever encounter would be a case with anaphylactic response, cardiac arrhythmia or arrest. What can we do to help decrease the inci-dence of CIN and preserve the renal function of our patients?
CIN is defi ned as a 25% or greater increase in serum cre-atinine, or a decrease in calculated creatinine clearance in the appropriate clinical setting: exposure to intra-venous or intra-arterial contrast, a rise in creatinine within 24-48 hours within contrast exposure, and the absence of other explanations for acute renal failure such as nephrotoxins, hypotension, and urinary obstruction. CIN occurs with much greater frequency and is more insidious, with eff ects that may not be visible. At this point it is believed that contrast agents stimulates vasoconstriction in the kidneys and decreas-es the kidneys ability to vasodilate. Some agents appear to cause ischemia by causing an increase of calcium ions into the renal vascular smooth-muscle cells. Th is in turn lowers the glomerular fi ltration rate (GFR). Contrast Medias are also known to irritate erythrocytes which increase blood viscos-ity reducing oxygen delivery. Because CIN takes several days to develop, patients might
≤
Rx only
BRACCODIAGNOSTICS
Rx only
Iopamidol Injection 76%
NOT FOR INTRATHECAL USE
ISOVUE®-200Iopamidol Injection 41% ISOVUE®-250Iopamidol Injection 51% ISOVUE®-300
ISOVUE®-300Iopamidol Injection 61% ISOVUE®-370Iopamidol Injection 76%
ne of the leading causes of renal failure for both in-patients and outpatients is contrast-induced nephropathy (CIN) following diagnostic and interventional procedures. As imaging modali-
ties continue to evolve, more patients will be treated and diagnosed with contrast enhanced imagery. CIN varies from 5% to 38% depending on the patients risk factors. So in perspective, a lab performing 1000 plus cases a year puts almost 400 patients at risk for CIN. As cardiovascular professionals working in the lab we rarely see the latent eff ects of our patients once they leave, and their intervention is complete. So we are unlikely to ever see the renal damage that can occur 48 – 72 hours following these cases. Th e only eff ects we may ever encounter would be a case with anaphylactic response, cardiac arrhythmia or arrest. What can we do to help decrease the inci-dence of CIN and preserve the renal function of our patients?
CIN is defi ned as a 25% or greater increase in serum cre-atinine, or a decrease in calculated creatinine clearance in the appropriate clinical setting: exposure to intra-venous or intra-arterial contrast, a rise in creatinine within 24-48 hours within contrast exposure, and the absence of other explanations for acute renal
Written by: Erik Benson RT (R)NorthBay Medical Center Heart and Vascular Lab Fairfield, CA
What do you know about contrast-induced nephropathy and how can you help protect your patients from it?
CORONARY HEART ™ 21

CONTRAST MEDIA
Contrast Nephropathy (cont...)
be discharged before any symptoms are evident. It should be taught on discharge that the patient be aware of any sings and symptoms and to contact their physician if they appear. Oral hydration is impera-tive and should be emphasized (provided that their overall health condition does not contraindicate increased fluid intake as in congestive heart failure). Patients should be instructed to watch for weight gain (>1kg or 2lbs per day), edema or if other signs appear the first days following their procedure. By the time symptoms of renal failure appear their renal function is decreased by as much as 75%. Some patients function will recover and could re-turn to normal over time (unless additional contrast studies are needed). So it is clear that we not only need to be aware of the potential of CIN, but we must be prepared to reduce the likely hood of occurrence.
Recognizing which of our patients are high risk and have the potential for contrast-induced acute renal failure is the key to improving our patient’s outcomes. There are many factors that may predispose a patient’s incidence of CIN. Pre-existing decreased renal function puts them in the high risk factor. The lower their function the higher their risk. We should as well be aware of any other comorbities, particular-ly diabetes and impaired cardiac function. Patients with diabetes and pre-existing renal insufficiency have the greatest risk of CIN. When patients in this group develop CIN they more than often develop oliguria as well. Screening for any contrast related problems would be the simplest approach. Check the blood urea nitrogen and creati-nine levels prior to procedure to assure that they are within normal limits. Calculat-ing the patients glomerular filtration rate (GFR) or creatinine clearance is another way to recognize any potential issues.
The normal ranges of GFR, adjusted for body surface area, are:
• Males: 70 ± 14 mL/min/m2 • Females: 60 ± 10 mL/min/m2
Estimation using creatinine clearance
In clinical practice, however, creatinine clearance is used to measure GFR. Creati-nine is an endogenous molecule, synthe-sized in the body, which is freely filtered by the glomerulus (but also secreted by the renal tubules in very small amounts). Creatinine clearance is therefore a close approximation of the GFR. However, the approximation of the GFR calculation is best measured by the evaluation and visualization of the frequency and duration of urination. The GFR is typically recorded in units of volume per time, e.g. milliliters per minute (ml/min).
Example: A person has a plasma creatinine concentration of 0.01 mg/ml and in 1 hour he excretes 75 mg of creatinine in the urine. The GFR is calculated as M/P (where M is the mass of creatinine excreted per unit time and P is the plasma concen-tration of creatinine).
Modification of Diet in Renal Disease (MDRD) formula
The most commonly used formula is the “4-variable MDRD” which estimates GFR using four variables: serum creatinine, age, race, and gender. The original MDRD used six variables with the additional vari-ables being the blood urea nitrogen and albumin levels. The equations have been validated in patients with chronic kidney disease; however both versions underes-timate the GFR in healthy patients with GFRs over 60 mL/min. The equations have not been validated in acute renal failure (see figure 1).
There was a presentation given at the CTO Summit this past year by Dr. Roxana Mehran in reference to CIN prevention, causes and treatments. A “scheme to de-fine CIN risk” was introduced along with a scoring system that incorporated a series of risk factors predicting the potentional for CIN (see Figure 2).
Prevention is key and should focus on lim-iting risk factors. Hydration is imperative to preventing CIN. The Cardiovascular Research Foundation Columbia Uni-versity Medical Center conducted a trial comparing the efficacy of 0.9% Saline and 0.45% Sodium Chloride in 1383 patients to help determine an optimal hydration regimen. The study showed that 0.45% Sodium Chloride had an increased inci-dence by 2% where 0.9% Saline only had an increased incidence of less than 1%. In addition to hydration NAC (N-acetyl-cysteine) also proves to be very effective in the prevention of CIN. A prospective randomized study at Columbia University Medical Center took 83 high risk patients with a CrCl < 50 ml/min gave them NAC 600 Bid X 2 days prior to 75ml of low osmolar contrast followed by hydration with 0.45% @ 1 ml/kg/h X 24 h. The end resulted in the control group (42) having a 21% increase incidence of CIN compared to a 2% increase in patients (41) that received NAC. A meta-analysis of 13 ran-domized placebo controlled trials showed that 4 of the 13 trials reported statistically significant reduction in CIN after NAC. Sodium Bicarbonate is also being used in conjunction with NAC helping to decrease the incidence of CIN. The REMEDIAL trial compared saline + NAC with Bicarbo-nate + NAC as well as Saline + AA + NAC. Out of 326 patients about a hundred in each group Bicarbonate + NAC showed
GFR = 186 x Serum Creatinine-1.154 x Age-0.203 x 1.21 if Black x 0.742 if Female
Figure 1
22 CORONARY HEART ™

CONTRAST MEDIA
only a 1.9% incidence in CrCl increase where saline + NAC resulted in 9.9% and saline + AA + NAC at 10.3%.
Limiting the amount of contrast given to patients with reduced renal function has been the historical standard of care for angiography. The damage associated with contrast agents can be minimized also by using lower doses of contrast medium and by using low-osmolal or iso-osmolal noni-onic contrast agents. Iso-osmolal nonionic agents have shown the lowest incidence of contrast-induced nephropathy. The type and amount of contrast agent is important. High osmolar, ionic agents were suggested to be highly nephrotoxic, whereas low-osmolar, non-ionic contrast agents where
not. A meta-analysis of 39 studies found that patients with renal insufficiency had a reduced incidence of CIN when low-os-molar agents were used. No difference in CIN was noted in those with normal renal function. One recent study compared iodixanol (non-ionic dimmer, iso-osmolar) with iohexol (non-ionic monomer, low osmolar) in patients with renal impair-ment and diabetes. This high risk group, iodixanol was associated with a signifi-cantly lower rate of CIN as compared with iohexol. Studies have found that a single agent in high risk patients undergoing cardiac catheterization or peripheral angi-ography suggest that both iodixanol and iopamidol may have a lower rate of CIN compared with iohexol. Additionally, the
volume of contrast is important. There is a thought that the risk of CIN is propor-tional to the volume infused. There is a retrospective study (the tadros study) that investigated the association between the volume of iso-osmolar agents and CIN. In this study the mean dose of contrast (84.3 +/- 67 ml in 117 patients) was not associ-ated with higher incidence of CIN. So the real question is, is the type of contrast agent important? Current evidence says that iso-osmolar contrast, in high risk pa-tients reduces the incidences of CIN. An ongoing, prospective study (VALOR trial) may provide additional evidence in favor of iodixanol.
Eventually we may find that iodixanol will provide better outcomes for all patients with decreased renal function. Compared to low-osmolar, iodixanol needs to be studied for cost effectiveness. But the opti-mism that the Tadros study promises could defiantly improve the safety and improve the outcomes of our patients in the future.
References:
Solomon R. The role of osmolality in the incidence of contrast induced nephropathy: a systematic review of angiographic con-trast media in high risk patients. Kidney Intl. 2005;68:2256-2263.Rudnick MR, Kesselheim A, Goldfarb S. Contrast-induced nephropathy: how it develops, how to prevent it. Cleve Clin J Med. 2006;73:75-80, 83-7.Stone GW, McCullough PA, Tumlin JA, et al. Fenoldopam mesylate for the prevention of contrast-induced nephropathy: A randomized controlled trial. JAMA 2003;290:2284–2291.Tadros GM, Malik JA, Manske CL. Iso-osmolar radio contrast iodixanol in patients with chronic kidney disease. J Invas Cardiol 2005;17:211–215.9 Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation 2002;105:2259–2264Aspelin P, Aubry P, Fransson S-G, et al. Nephrotoxic effects in high-risk patients undergoing angiograSolomon R, Werner C, Mann D, D’Elia J, Silva P. Effects of saline, mannitol, and furo-semide to prevent acute decreases in renal function induced by radiocontrast agents. N Engl J Med 1994;331:1416-1420phy. N Engl J Med 2003;348:491–499.Rich MW, Crecelius CA. Incidence, risk factors, and clinical course of acute renal insufficiency after cardiac catheterization in patients 70 years of age or older. A prospective study. Arch Intern Med 1990;150:1237-1242McCullough PA, Wolyn R, Rocher LL, Levin RN, O’Neill WW. Acute renal failure after coronary intervention: inci-dence, risk factors, and relationship to mortality. Am J Med 1997;103:368-375Caro JJ, Trindade E, McGregor M. The cost-effectiveness of replacing high-osmolality with low-osmolality contrast media. AJR Am J Roentgenol 1992;159:869-874Cindy Kohtz, EdD, RN, CNE, and Maren Thompson, PharmD Preventing Contrast Medium Induced Nephropathy AJN September 2007 Vol. 107, No. 9
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Scheme to define CIN risk score
Risk Factors Integer Score
Hypotension 5IABP 5CHF 5Age >75 4Anemia 3Diabetes 3Contrast media volume 1 for each 100cc3 Serum creatine > 1.5mg/dl 4
Or
2 for 40-60eGFR <60ml/min/1.73 m2 4 for 20-40
6 for <20
The total calculated score will give you the percentage of risk your patient faces.
Risk Score Risk of CIN Risk of Dialysis ≤ 5 7.5% 0.04%6 to 10 14% 0.12%11 to 16 26.1% 1.09%≥ 16 57.3% 12.6%
Figure 2
CORONARY HEART ™ 23

SITE VISIT
Baton Rouge Cardiology Center
ADDRESS
FAST FACTS
Baton Rouge Cardiology Center�231 Brittany DriveBaton Rouge, LA �0808United States of America
MAP
Free-Standing Outpatient Cath Lab
Over 30 years trusted cardiac service in the com-munity
Cardiac and Peripheral Cases
•
•
•
Baton Rouge Cardiology Center (BRCC), located in Baton Rouge, Louisiana, is the trusted leader in the community for
heart and vascular care.
Established in 1978 by cardiologists’ James Calvin, M.D., T.R. Kilpatrick, M.D. and Boyd E. Helm, M.D., Baton Rouge Cardiology Center (formally the “Cardi-ology Clinic”) has grown to the current, 13 physician practice, which includes (11 cardiologists, 1 electrophysiologist, 1 inter-ventional radiologist).
Boyd E. Helm, M.D., F.A.C.C., F.S.C.A.I. – Cardiologist
Joseph M. Cefalu, M.D., F.A.C.C. – Cardiologist
•
•
Kevin L. Kilpatrick, M.D., F.A.C.C. – Cardiologist
Terry L. Zellmer, M.D., F.A.C.C. – Cardiologist
Daniel T. Fontenot, M.D., F.A.C.C. – Cardiologist
Harold G. Clausen, Jr., M.D., F.A.C.C., F.S.C.A.I. – Cardiologist
Fred H. Petty, M.D., F.A.C.C., F.S.C.A.I. – Cardiologist
Henry C. Patrick, M.D., F.A.C.C. – Cardiologist/Electrophysiologist
•
•
•
•
•
•
From Left (front row): Sadie Edwards; Kathy Simmons, RN; Beverly Myrick, RN; Audrey Williams;
From Left (back row): Terry L. Zellmer, M.D., F.A.C.C.; Harold G. Clausen, Jr., M.D., F.A.C.C., F.S.C.A.I.; Evens Rodney, M.D., F.A.C.C.; Darrin M. Breaux, M.D., F.A.C.C.; Venkat R. Surakanti, M.D., F.A.C.C., F.S.C.A.I.; Daniel T. Fontenot , M.D., F.A.C.C.; Dana Politz, RN, Director
24 CORONARY HEART ™

SITE VISIT
Venkat R. Surakanti, M.D., F.A.C.C., F.S.C.A.I. – Cardiologist
Evens Rodney, M.D., F.A.C.C. – Car-diologist
Darrin M. Breaux, M.D., F.A.C.C. – Cardiologist
Jonathan W. Tronolone, M.D. – Car-diologist
Boyd M. Helm, M.D., Vascular & Interventional Radiologist
In 1993, Baton Rouge Cardiology Center opened its “outpatient cath lab.” Work-ing in conjunction with local hospitals, our main goal was to provide quality patient care in a cost effective manner. Our outpatient cath lab provides patients’ with comprehensive care all in one setting - admission, diagnosis, treatment, and recovery. This comprehensive care results in convenience and shorter length of stay for our patients.
Today, Baton Rouge Cardiology Center’s outpatient cath lab, along with 60+ ad-ditional outpatient cath labs around the country, is facing reimbursement chal-lenges from the Centers for Medicare and Medicaid (CMS). These reimbursement changes could result in the closing of the majority of outpatient cath labs in the U.S., as well as forcing patients who now benefit from improved access and lower health care costs into more acute and expensive settings.
BRCC Cath Lab Site Visit Interview:
(The following questions were answered by Baton Rouge Cardiology Center’s physi-cians and cath lab staff.)
What are the benefits to having an outpatient cath lab?There are a variety of reasons and benefits
•
•
•
•
•
From Left: Dana Politz, RN, Director , Anthony Pocorello, RN; and Randi Deaton, RN, Assistant Director
CORONARY HEART ™ 2�

SITE VISIT
Baton Rouge Cardiology Center (cont...)
to having our own cath lab, including improved work efficiency and enhanced patient satisfaction.
Because all of our cases are elective, the outpatient cath lab procedures are not interrupted by emergency procedures (i.e. Acute MIs) from the ER. The duration of our cases are short and predictable. All la-bwork, paperwork and registration is com-pleted at the time the patient’s procedure is scheduled, which is an added convenience for our patients.
Our patients appreciate the friendly décor, the shorter length of stay, as well as the laid back atmosphere in our cath lab. In addition, because the recovery rooms are located near the procedure room, patients are not transferred through elevators or multiple floors in a facility. Our patients are able to stay in our large, spacious recovery areas.Our patients receive personalized, conven-ient, and rapid service, which results in superior patient satisfaction.
Is your cath lab accredited?Yes. The outpatient cath lab received accreditation with Commendation from the Joint Commission on Accreditation of Healthcare Organizations (JCAHO). The Joint Commission is the leader in ac-creditation and certification of health care organizations, such as hospitals, surgery centers and ambulatory care facilities.
Because Joint Commission standards are regarded as the most rigorous in the indus-try, this shows our labs’ extraordinary com-mitment to provide safe, high quality care and a willingness to be measured against the highest standards of performance.
Has the practice formed an alliance with other hospitals for treating patients?Yes. Our physicians and staff have excel-lent relationships with hospitals in the community. In the rare occurrence of an emergency, we have entered into trans-
fer agreements to have full access to all hospital services (including surgery, ICU, OR, etc.)
Does owning an outpatient lab affect your relationship with the hospitals?Yes, in a positive manner. Our physicians and staff work in collaboration with the hospitals to provide an on-going continu-ity of care for the patient. Also, the elective cases in the outpatient cath lab offset the increased volume that acute care facilities face, thereby decreasing delays in treat-ment. The hospital recognizes having the outpatient cath lab on campus as a benefit to the community.
What is the size of the cath lab facility?
1 cath lab6 patient rooms3 holding bays
The outpatient cath lab admits patients, performs procedures, recovers and dis-charges patients in one setting.
How many staff work at your lab? What are their roles?Our physicians are personally and directly responsible for managing the cath lab, which includes training and maintain-ing competency of staff. By working in collaboration with the staff, we are able to work efficiently and effectively.
We currently have 14 full-time cath lab employees including:
1 Cath Lab Director1 Assistant Director (works in the lab & nurses unit)7 RNs (works in the lab & nurses unit)
•••
••
•
In cath lab: Fred H. Petty, M.D., F.A.C.C., F.S.C.A.I.; and Tim Derouen, BSRT, (R);In control room: Kathy Simmons, RN, RCIS
2� CORONARY HEART ™

SITE VISIT
3 RTs (works in the lab & nurses unit)1 Receptionist1 Nursing Assistant
Our night staff includes:4 Polysomnography StaffPart-time Contracted Night Staff
Types of procedures?Diagnostic & Interventional Cardiac / Pe-ripheral Procedures, Electrical Cardiover-sions, Transesophageal Echo’s, Pacemakers & ICD/Bi-V Implants
•••
••
Types of equipment used (eg. X-ray, IVUS, Pressure Wire)MIS X-ray equipment, Mennen / Clini-base Database, Spacelabs monitoring, and Computerized Scheduling
Are patients performed as day cases?Yes, all cases in our outpatient cath lab are performed during the day. Patients who have had an intervention may spend the night. This is when our night shift comes in from 7pm – 7am.
How many procedures are performed in the outpatient cath lab per year?2026 patients/yr.; 4,192 procedures/yr.
Is your staff cross-trained? Yes. Our outpatient cath lab staff is dedi-cated to our facility. In order to maximize the use of our staff, they are cross-trained to be able to handle all functions in the cath lab and recovery areas. Our RNs circulate. RNs, RTs & CVTs scrub and monitor. All of our staff are cross-trained to work in the nurse’s unit. We have at least one RN in nursing unit at all times.
Outpatient Cath Lab Staff (Pictured from left to right):Randi Deaton, RN, Assistant Director; Dana Politz, RN, Director; Tammy Gascon, RT(R); Johnny Johnson, RT(R); Kathy Simmons, RN; Audrey Williams; Nancy Marionneaux, RN; Sadie Edwards; Babette Bartholomew, RCIS; Cathy Sims, RN; Tim Derouen BSRT(R); Beverly Myrick, RN; Elsie Byouk, RN. (not pictured: Barb Pittenger, RN; Anthony Pocorello, RN
CORONARY HEART ™ 2�

SITE VISIT
What are the main roles for the RTs, CVTs and Nurses? Do you have any other job roles onsite?RNs, RTs and CVTs are involved in the daily operations of cath lab procedures. They are also involved in Performance Improvement (i.e. call backs for patient satisfaction, ordering supplies, input of daily charges, maintaining database of imaging equipment, and maintaining lab responsibilities for COLA certification.)
Is surgical back-up available in the cath lab? If not, where does the patient get transferred?Yes, surgical backup is available 24/7, if needed. In the rare instance that a patient needs emergency surgery, we are able to provide the most efficient and quality care as our cath lab is located on a hospital campus.
What new procedures have you implemented into the department recently?Polysomnography (Sleep Studies)
How is your inventory managed?PAR levels are maintained for general and special supplies, and medications.
How does the lab handle hemostasis?Manual pressure 98% and Angioseal 2%
What measures has the lab implemented to cut costs?To cut costs, we make bulk purchases of DES, staff schedules according to cath lab needs and maintain PAR levels for supplies and medications.
What kind of training can new employees expect to receive?For new employees, initial orientation to the cath lab and the nursing unit is a three month process. There is a dedicated preceptor for each role that the preceptee is in (i.e. circulating, scrub, or monitoring in the cath lab.) An RN orients new employ-ees to the nurse’s unit.
What types of continuing education programs are available to staff?In order to attend educational programs pertinent to job responsibilities, staff are provided workshop days each year. In-service training with continuing education hours are also provided in the cath lab.
What types of competency checks does staff undergo once employed?
Annual videos and safety programModerate Sedation Test for all RNsSurgical Fire Prevention TestLab competencies for all RNsRadiation and charting in-service training annuallyAutoclave CompetencyCultural Diversity
Is the department used as a training facility for cardiac fellows? No.
Please outline the Department Management structure.
Governing Board: 2 Co-ChairsAdministrators: 2 Co-Administra-tors
•••••
••
••
DirectorAssistant DirectorRNs, RTs, CVTsSecretary Nursing AssistantPolysomnography Staff Contracted Night Staff
How do you deal with late finishing of cases? For example staggered working hours or just staff overtime?Blocked scheduling. Last case starts at 3:45 p.m. If cases run late, we have staff to stay over. We also have staggered shifts, which helps to decrease overtime. There is night staff at 7 p.m., if needed for over-night patients.
What is your policy for company reps within the labs?Limited to cath lab specific in-service training.
What is the best part of working at your facility?The best part of working at our outpatient cath lab is the excellent TEAMWORK of physicians and staff! We have experi-enced personnel of 10 years or greater. Of course, an added plus to working in our outpatient cath lab is that we are closed on weekends and holidays… and we do not have call!
•••••••
Baton Rouge Cardiology Center (cont...)
28 CORONARY HEART ™

EDUCATION
And The Beat Goes On…
A little background. A 60 year old woman presents in the ED with chest pain 10/10, ST elevations in the anterior leads, hemodynami-cally unstable with a heart rate of 110, BP of 90/50 and no previous cardiac history. Th e ED says, “She doesn’t look good, she’s cool and clammy, nauseated and short of breath.”
In Part l of this series (See our March/April 2008 issue), we talked about the physiology behind this typical presentation for a patient with myocardial infarction. In Part ll, we review the major antihrom-botic medications, their modes of action, and 2007 ACC/AHA recommendations. And we fi nd out what happened to our ED patient.
Antithrombotic Pharmacology
Here’s a sobering statistic: over 1.5 million people are hos-pitalized in the US every year with acute coronary syndrome (ACS). And within a year of an initial MI, 38% of women and 25% of men will die. 1
Th e good news is that new technologies and treatment strategies have decreased mor-tality and morbidity rates over the last few decades. Pharmacologic and invasive thera-pies aimed at safe and eff ective reperfusion are constantly evolving based on evidence-based standards of care.
In 1960, when my grandfather developed chest pain, “take two aspirin and call me in the morning” was close to the defi nitive treatment. Th e 1980’s saw the introduction of thrombolytics or clot busters in the
The following article was made possible in part by an unrestricted educational grant from Bracco Diagnostics Inc. For more information, please visit them at www.bracco.com
- A Review of Lifesaving and Antithrombotic Drugs
Part 2 of a Two-Part Series
By Charlene Shellenberger, BS, RN, Clinical Education Specialist, Healthworks, Inc.
CORONARY HEART ™ 2�

EDUCATION
AND THE BEAT GOES ON (cont...)
form of streptokinase for coronary arterial reperfusion.
In 1989 a new recombinant form of tissue plasminogen activator (t-PA) was intro-duced. By 2002, early invasive interven-tion was the standard of care. And overall in-hospital death rates for acute myocardial infarction fell from 25% in 1970 to 8% in 2002. 2
Pharmacologic antithrombotic therapy is a hot topic of debate and investigation today. Included are anticoagulants, antiplatelets and thrombolytic agents. When and why are each of these agents used, and how do they function?
To find the answers, let’s revisit what we know about normal clotting in the body. The ability to achieve hemostasis – the physiologic process by which bleeding is halted - is essential to life. The clotting cascade is a detailed, multistep process that we’ll look at in its simplest form.
The primary focus is on the star player of hemostasis: the platelet. Any disruption in the endothelium of the blood vessel, whether due to a cut in the skin or a rup-tured plaque in a coronary artery, causes the release of collagen and tissue factors into the bloodstream.
Platelets circulating in the bloodstream, which in their normal inactive state are smooth and discoid in shape, become acti-vated in the presence of collagen and tissue factor. The platelets change shape and send out spicules that resemble a sea anemone (see Figure 1).
Activated platelets adhere to the site of in-jury. Thrombin is produced and recruits more circulating thrombin and coagula-tion factors, setting the stage for large-scale thrombin production. Thrombin converts fibrinogen to fibrin, which leads to clot for-mation as red blood cells are caught up in a fibrin mesh.
This is great for a cut finger but not so good as a response to a ruptured coronary artery plaque: the thrombus may eventually block flow in that artery completely. Initially this is seen on EKG as ischemia and T-wave inversion, followed by ST segment eleva-tion indicating injury, and -- if not resolved -- myocardial infarction evidenced by a Q wave, coupled with crushing chest pain and feelings of impending doom.
Here’s the order of events:
Vasoconstriction (to reduce blood loss) —->
Platelet adhesion (to seal the injury site) —->
Platelet activation (change of shape, transformers) —->
Platelet aggregation (recruit friends for help) —->
Clot formation (fibrin mesh where red blood cells and platelets “stick” together) —->
Mission hemostasis accomplished! —->
Possible occlusive thrombus in coronary arteries —->
Myocardial infarction
As you can see in Figure 2, there are many pathways to platelet activation.
Platelet aggregation can be inhibited by:
Inhibitors of thromboxane 2 (TXA2) production, including aspirin and non-steroidal anti-inflammatory drugs (NSAIDs).
Inhibitors of P2Y12 receptors of ad-enosine diphosphate (ADP) like Plavix® (clopidogrel), Ticlid® (ticlo-pidine), prasugrel and cangrelor.
Direct thrombin inhibitors like Angi-omax® (bivalirudin), argatroban, lepirudin and desirudin. These drugs also inhibit plasma coagulation where thrombin plays a key role.
Inhibitors of glycoprotein llb/llla re-ceptors like ReoPro® (abciximab), Integrilin® (eptifibatide) and Aggra-stat® (tirofiban).3
The key event in the final stages of blood coagulation is the conversion of fibrinogen to fibrin by the serine protease enzyme thrombin, which is produced in the final stages of coagulation from prothrombin by the action of the enzyme prothombinase. Fibrin is then cross-linked to factor XII to form a blood clot.
•
•
•
•
Figure 1: Inactive platelets (left) and activated platelets (right).
Figure 2: Pathways to platelet activation
30 CORONARY HEART ™

EDUCATION
The principal inhibitor of thrombin in normal blood circulation is antithrombin III. Antithrombotic pharmacological therapy may prevent clot formation or ex-tension, inhibit platelet aggregation, or break down or “bust” the existing fibrin mesh of a clot. 4
Anticoagulants prevent clot formation and prevent the extension of an existing thrombus. These include heparin in the form of unfractionated heparin (UFH), low molecular weight heparins (LMWHs) like Lovenox® (enoxaparin), Arixtra® (fon-daparinux), and Coumadin® (warfarin), the last of which is not used in the cath lab. Direct thrombin Inhibitors (DTI) like An-giomax® (bivalirudin) and argatroban are also included in the anticoagulants.
Unfractionated heparin (UFH) is derived from the mucosal tissues of meat animals, including pig intestines and bovine lungs. One unit of heparin is the quantity required to keep 1 ml of cat’s blood fluid for 24 hours at 0 degrees Celsius.5
Heparin binds to the enzyme inhibitor an-tithrombin III (AT-III) and causes a shape change that results in its active site being ex-posed. The activated AT-III then inactivates thrombin and other proteases involved in blood clotting, predominantly factor Xa.
Heparin is given as an anticoagulant in the cath lab setting for percutaneous coronary intervention (PCI). UFH is indicated for use with glycoprotein receptor site inhibitor (GPI) drugs like ReoPro® (abciximab), In-tegrilin® (eptifibatide) and Aggrastat® (ti-rofiban) as well as with thrombolytic medi-cations like Activase® (alteplase).
Heparin has a short biological half-life of one hour. Its effects are measured in the lab by partial thromboplastin time (aPTT), or the time it takes blood plasma to clot, and activated clotting time (ACT). 2007 AHA/ACC guidelines recommend an ACT of 200-250 as therapeutic during PCI.6
Patients who receive heparin are at risk for developing heparin induced thrombocy-topenia syndrome (HITS). The effects of heparin can be reversed with protamine.
Heparin was in the news in November 2007 when actor Dennis Quaid’s twelve-day-old twins were mistakenly given 1,000 times the requested dosage of heparin. The drug received more negative press recently due to tainted heparin batches traced to manufac-turing facilities in China.
Lovenox® (enoxaparin) is a low molecular weight heparin derived from pig intestine mucosa. Its anticoagulant effect can be directly correlated to its ability to inhibit factor Xa. Lovenox was originally used to treat deep vein thrombosis (DVT) and pulmonary embolus (PE). It’s now used in acute coronary syndrome (ACS) and fre-quently administered in the ED.
Lovenox has no effect on INR, aPTT, PT or ACT, as these tests are insensitive to altera-tions in factor Xa. Its half-life is 4.5 hours. There is a reduced risk of HITS with Lov-enox compared to heparin. Protamine will reverse the effects of Lovenox, but only by 66%. 7
The ExTRACT-TIMI 25 trial compared the outcomes of patients undergoing PCI who received Lovenox with patients who received UFH. There was a 23% relative risk reduction in the primary composite endpoint of death or nonfatal MI for pa-tients receiving Lovenox compared with those receiving UFH.8
Arixtra® (fondaparinux) is the newest anti-coagulant approved for use in ACS patients. It’s a synthetic pentasaccharide and a factor Xa inhibitor that selectively binds to anti-thrombin.
Arixtra has been successfully used to pre-vent thromboembolic complications in or-thopedic surgery and has shown short-term efficacy similar to Lovenox in preventing ischemic events in Non-ST-Elevation Myo-
cardial Infarction (NSTEMI) patients.9
The 2007 ACC/AHA guideline update rec-ognizes Arixtra as an anticoagulant agent to be used in conjunction with fibrinolytic agents. It has a predictable anticoagulant response, although it has no effect on INR, aPTT, PT or ACT. The half life of Arixtra is 17 to 21 hours. Trials have shown de-creased bleeding complications compared to heparin. There is no antigenicity and very limited risk of HITS.10
The OASIS-6 randomized, double blind trial evaluated the efficacy of Arixtra com-pared with standard anticoagulant therapy in patients with acute ST-elevation myo-cardial infarction (STEMI). Arixtra was superior to UFH in patients who did not undergo PCI, but patients who underwent PCI and received Arixtra had an increased risk of coronary complications, abrupt closure, no reflow, dissection, new angio-graphic thrombus, perforation and catheter thrombosis.
In patients treated with conservative therapy, the preferred anticoagulants may be Arixtra, Lovenox for 8 days or for the duration of hospitalization, or UFH for 48 hours, in that order. 6 Angiomax® (bivalirudin) is a direct thrombin inhibitor anticoagulant. Its ac-tive substance is a synthetic peptide that uses hirudin, a natural protein in the sali-vary gland of leeches, as a prototype.11
This is a potent, highly specific, reversible bivalent inhibitor of thrombin and can in-activate both circulating and clot-bound thrombin. It has fast on and fast off ac-tivity, with a half-life of 25 minutes. There is no reversal agent.
Angiomax is indicated for patients with unstable angina undergoing percutaneous transluminal angioplasty (PCTA) and for PCI with provisional use of GPIIb/IIIa. It’s also indicated for patients with or at risk of HIT/HITTS who are undergoing PCI.
CORONARY HEART ™ 31

EDUCATION
AND THE BEAT GOES ON (cont...)
Dosing is weight-based. Angiomax is in-tended for use with aspirin. Sheath removal is possible in 1 to 2 hours after discontin-uing the infusion.12
Helpful hint: If the patient has received UFH, wait 30 minutes before starting An-giomax. if the patient has received LMWH, wait 8 hours before starting Angiomax.
In PCI, Angiomax demonstrated proven ef-ficacy plus fewer bleeding complications for improved outcomes. It was also shown to reduce major hemorrhagic events by 41 to 61% in the ACUITY ACS trial.
In HORIZONS-AMI, Angiomax mono-therapy compared to UFH plus GP llb/llla inhibitor was associated with a 24% reduc-tion in the 30-day primary endpoint of net adverse clinical events (all cause death, reinfarction, ischemic target vessel revas-cularization, or stroke and major bleeding non-CABG). There was also a 40% reduc-tion in 30-day primary endpoint of major bleeding. 13
Finally, data from the REPLACE-2 and ACUITY trials determined that Angi-omax provides cost reductions compared to heparin+GPIIb/IIIa and can be considered an economically attractive antithrombotic medication.
Argatorban is a direct thrombin inhibitor indicated for use as prophylaxis or treatment of thrombosis in patients with heparin-induced thrombocytopenia syndrome (HITS). It’s also indicated for patients undergoing PCI who are at risk for HITS and is an effective alternative to heparin in HITS patients. The anticoagulant effect is seen immediately and is monitored with aPTT. Therapeutic aPTT levels are seen in about three hours. Its half-life is 39 to 51 minutes. 14
Antiplatelet medications decrease platelet aggregation and inhibit thrombus forma-
tion. They’re effective in arterial circulation where anticoagulants have little effect. An-tiplatelet drugs are classified according to which platelet receptor site is inhibited.
Acetylsalicylic acid (aspirin) is a cyclooxy-genase inhibitor. Adenosine diphosphate (ADP) receptor inhibitors include Plavix® (clopidogrel) and Ticlid® (ticlopidine). Glycoprotein llb/llla inhibitors include ReoPro® (abciximab), Integrilin® (epti-fibatide) and Aggrastat® (tirofiban). Ad-enosine reuptake inhibitors include Persan-tine® (dipyridamole).15
Acetylsalicylic acid (ASA) is the one drug used to treat cardiac patients whose value is undisputed. Its appropriate dosing regime is currently being debated, however. Its derivatives have been in medical use since antiquity. Sources of salicylic acid can be found in willow bark, myrtle leaves and meadowsweet (Spiraea ulmaria).
In 1835, salicylic acid was successfully synthesized in the laboratory, enabling mass production. Its side effects included mouth, throat and stomach irritation. In 1897 Felix Hoffmann, a German pharma-ceutical graduate working for the Bayer Company, invented acetylsalicylic acid, a new formulation without the unpleasant side effects of its predecessor. In 1899, ASA was given the brand name of aspirin, The “A” stood for acetyl, the “spir” came from Spiraea ulmaria, and where the “in” came from is unknown.16
Today aspirin is the most widely used car-diac medication, is available without a pre-scription, and is by far the least expensive. It also provides the greatest return in terms of long-term cardioprotective benefit. A new twist on an old saying: an aspirin and an apple a day keep the doctor away!
Aspirin irreversibly inhibits COX-1 (cy-clooxygenase) and modifies the activity of COX-2. This gives it the ability to suppress prostaglandin and thromboxane produc-tion. Thromboxanes are responsible for
the aggregation of platelets that form blood clots. Low-dose, long-term aspirin use ir-reversibly blocks the formation of throm-boxane A2 in platelets, producing an inhib-itory effect on platelet aggregation. 17
Because heart attacks are primarily caused by blood clots, their reduction with the in-troduction of small amounts of aspirin has been seen as an effective medical interven-tion.
The 2007 ACC/AHA guidelines recom-mend that ASA be administered to patients with ACS as soon as possible and continued indefinitely. Patients with unstable angina and non-ST elevation MI (UA/NSTEMI) who are treated medically without stenting should receive aspirin indefinitely and Plavix for one to 12 months.
Patients with UA/NSETMI who are treated with bare-metal stents should receive aspirin for at least one month and then indefinitely at lower dose as well as Plavix for one to 12 months. 18
For patients undergoing coronary artery bypass grafting (CABG), aspirin should be continued while Plavix should be stopped five to seven days before surgery. In UA patients, ASA should be chewed, not swal-lowed, to hasten its effects in the blood-stream.19
Plavix® (clopidogrel), a thienopyridine, is an antiplatelet aggregate medication whose beneficial effects are undisputed. It’s used in combination with aspirin as dual an-tiplatelet therapy in the majority of cardiac and stroke patients.
Plavix irreversibly blocks the adenosine di-phosphate (ADP) receptor site on platelet cell membranes (P2Y12). It’s a prodrug that requires metabolism by the liver for ac-tivation. Platelet inhibition can be demon-strated two hours after single-dose adminis-tration, but the onset of action is slow, so a loading dose is usually administered. 20
32 CORONARY HEART ™

EDUCATION
The hot topic here is not “Should Plavix be given?” but “What dose of Plavix is best?” Debate centers on when to administer the drug, at what dose and for how long. The answers depend on variables of patient pres-entation (diagnostic case turned interven-tional or UA/STEMI) and treatment (con-servative pharmacological support, invasive plain old balloon angioplasty (POBA), bare-metal or drug eluting stent).
In the CURE trial, pre-treatment with Plavix 300mg at least 24 hours prior to pro-cedure showed a 20% relative risk reduction (RRR) in the primary end points of death, MI, stroke and severe ischemia. Because Plavix must be withheld for five to seven days before surgery, clinicians must weigh the risks and benefits of an early loading dose.
Researchers in the ARMYA-2 trail evalu-ated whether a 300mg or 600mg loading dose is superior. Patients receiving 600mg at least eight hours prior to PCI had a 50% RRR in periprocedural MI.21
For patients treated invasively, the 2007 ACC/AHA guidelines recommend that the duration of Plavix therapy be extended for at least one year after drug-eluting stent placement and ideally up to one year after bare-metal stent placement or medical therapy. ACC/AHA guidelines support the 600mg loading dose, citing more prompt and reliable platelet inhibition.22
In 2005, Plavix was reported to be the world’s second-highest selling pharmaceu-tical, with sales of $5.6 billion US. A one-month supply -- thirty 75mg tablets -- costs around $160 without insurance.23
Its high price is a factor for clinicians to consider in making treatment decisions: can the patient afford the medication, and how compliant will he or she be? The pa-tient should not have to choose between food and Plavix.
Just like Cinderella’s slipper, this is not a
one-size-fits-all situation. Decisions are multifactorial and need to be evaluated in terms of risk-benefit ratio on an individual basis.
Ticlid® (ticlopidine) is in the same class of medications as Plavix and may be used for patients who are allergic to Plavix or aspirin. Its half-life is 12 hours with a single dose and four to five days with repeated dosing.
CORONARY HEART ™ 33

EDUCATION
AND THE BEAT GOES ON (cont...)
The downside of Ticlid – and the reason Plavix is the preferred drug in this class -- is the reported increase in the risk of throm-botic thrombocytopenic purpura (TPP) and neutropenia. Plavix also has a much lower hemorrhagic risk than Ticlid.24
Glyoprotein IIb/IIIa inhibitors include ReoPro® (abciximab), which blocks the GP llb/llla receptor and thereby blocks the interaction of fibrinogen with the receptor, the final common pathway to platelet ag-gregation.
ReoPro is manufactured from chimeric monoclonal murine proteins. What’s that, you ask? A chimera is a human-engineered or in vivo mutated protein that is encoded by a nucleotide sequence made by splicing together two or more complete or partial genes from two different species.25 Wow! Among other things, this is a labor-inten-sive process, which explains why ReoPro is sooo expensive.
ReoPro is dosed by the patient’s weight with no adjustments for renal impairment. A 100kg patient receives a 12.5 cc bolus and an infusion of 17 cc/hr. This patient needs four vials: one for the infusion and three for the 12.5 cc bolus.26 At $470 per vial, cost of treatment is $1,880.27
Helpful hint: ReoPro vials should be refriger-ated and should not be shaken. Inspect the vial visually for particulate matter prior to administration. A non-pyrogenic, low protein binding 0.2 micron filter is used to prepare ReoPro boluses and infusions. Withdraw the contents from the vials with a standard needle, then attach the filter for injection. Don’t pull the drug through the filter: push it through the filter into the IV line (for the bolus dose) or bag.
What subset of patient benefits most from ReoPro administration? As with any drug, efficacy must be evaluated in terms of risk-
benefit ratio. There’s a saying in the cath lab that “ReoPro makes it (blood) flow.” There’s a good reason for this: blood does indeed flow in the coronary vessel. But there are also more bleeding risks associated with ReoPro than with other anticoagulant agents.
ReoPro has a demonstrated ability to di-minish freshly-formed platelet aggregates, causing the outermost platelets to break away from the collected aggregates and the thrombus to diminish. This distinction sets it apart from other anticoagulants or an-tiplatelet agents. 28
ReoPro binds to platelets for the life of the platelet, which is approximately 10 days. If the patient develops bleeding, HITS, or must go immediately to bypass surgery, platelet infusion would be necessary to help reverse the effects of ReoPro.
High-risk STEMI patients who have visible clots and are diabetic should definitely slip their feet into the ReoPro “slipper.” This was demonstrated in the EPISTENT trial.
ACC/AHA guidelines recommend a GP llb/llla inhibitor if an early invasive strategy is used. ReoPro is more enthusiastically rec-ommended in intermediate- to high-risk patients and in combination with aspirin and Plavix in patients who were not pre-treated with a GP llb/llla inhibitor and were proceeding to PCI .29
Integrilin® (eptifibatide) is an antithrom-botic agent that reversibly inhibits platelet aggregation by preventing binding of fi-brinogen to the GP lla/lllb receptor. In-tegrilin helps prevent occlusion of the coro-nary arteries, thus reducing the incidence of ischemic events.
This is a cyclic hepapeptide derived from a protein found in the venom of the south-eastern pygmy rattlesnake. It has a short half-life of 2.5 hours. It’s the third inhibitor of GPllb/llla to find wide acceptance after ReoPro and Aggrastat. 30
Integrilin is always used in combination with aspirin and/or Plavix and UF or LMW heparin. In patients with UA/STEMI and those undergoing PCI, it has been shown to drive down the risk of ischemic events: clinical trials have demonstrated significant risk reduction before, during and long after PCI. The PURSUIT and ESPRIT trials were pivotal in supporting Integrilin use in PCI, UA/NSTMI and STEMI.31
Integrilin is dosed based on patient weight and creatine clearance (CrCl). Infusion is recommended for a minimum of 12 hours. Integrilin comes in premixed bottles for bolus and infusion administration and should be kept refrigerated.32
This is the only PCI medication for which there is no mixing involved and two bo-luses are given. Sometimes the first bolus and infusion are initiated in the ED and the second bolus in the cath lab.
Helpful hint: Administer weight-based heparin and monitor ACTs to achieve a level of 200-250 during PCI, per the latest ACC/AHA guidelines.
Cost of treatment with Integrilin lies be-tween bivalirudin and abciximab. Our 100kg patient with normal CrCl will re-ceive two boluses of 9cc and an infusion of 16cc/hr. This translates into two small vials at $76 each and two 100ml infusion bottles at $230 each to complete the recommended 12 hours of infusion, for a grand total of $612.33
Integrilin has been investigated in multiple clinical trials and has been demonstrated to play an important role in conservative and invasive UA/NSTMI management. Data from the CAPTURE, PRISM, and PAR-AGON B trials suggest that GPIs are more effective in reducing mortality and MI in non-ST-segment elevation ACS (NSTE-ACS) patients with elevated troponin levels,
34 CORONARY HEART ™

EDUCATION
but not in patients with normal troponin levels. 34
Integrilin has been the most widely used PCI medication in the past, providing ex-cellent results at a fair price: like vanilla ice cream, almost everybody likes it. Where abciximab is expensive and reserved for high-risk patients and bivalirudin came into the marketplace as an alternative to heparin in patients at risk for HITS and has been gaining acceptance as a first line drug in PCI and now STEMI, Integrilin has a universal appeal rooted in evidence-based medicine.
Aggrastat® (tirofiban) is another GP llb/llla inhibitor. It’s a modified version of an anticoagulant found in the venom of the saw-scaled viper Echis carinatus. ACC/AHA guidelines for Aggrastat reflect those of eptifibatide.35
Thrombolytic therapy includes the use of drugs to break up or dissolve blood clots -- the main cause of heart attack and stroke -- and reestablish flow. The suffix “lytics” and the term “clot-buster” reflect the action of these drugs.
Thrombolytic medications have saved countless lives. They act on the fibrinolytic system, which is activated by the conversion of plasminogen to the enzyme plasmin (fi-brinolysin). This is the enzyme that breaks down the fibrin mesh of clots (Fibrinolysin means “to loosen”).
Streptokinase (SK) and tissue plas-minogen activator (tPA) are the most widely used thrombolytic agents for heart attack and stroke.
The key to successful thrombolytic reper-fusion therapy is early implementation. Time is muscle, as reflected in the concept
of “door to needle time,” the time between a patient’s first symptoms and the first dose of thrombolytic.
One trial showed that patients who re-ceive thrombolytics and subsequently had blood flow restored within one hour had a 1% mortality rate over the next 30 days. Waiting another 30 minutes raised the 30-day mortality rate to 6.4%. After three hours, 80% of benefits were lost, and after 4 hours thrombolytics had virtually no ef-fect in reducing mortality.36
Thus the clinical goal is to administer t-PA or streptokinase within 90 minutes of the onset of symptoms. Accomplishing this re-quires patients to recognize the early onset of symptoms and call for help immediately.
But even with rapid thrombolytic treat-ment, about 60% of heart attack patients
CORONARY HEART ™ 3�

EDUCATION
need more intervention to restore blood flow completely. This group requires inva-sive mechanical intervention in the form of PCI.37
Streptokinase -- so named because it was isolated from the streptococcus bacterium -- was the first thrombolytic used in heart attack patients. Introduced in the 1970’s, it made its mark in terms of declining death rates from heart attack.
SK activates both the plasminogen bound to a fibrin clot and the normally inactive plasminogen circulating in the bloodstream, forming plasmin throughout the body. As a result, it both dissolves clots and predis-poses bleeding in other organs and tissues. This systemic activity represents the major drawback to SK as a thrombolytic: un-wanted and potentially lethal bleeding. 38T-PA, or tissue plasminogen activator, converts plasminogen to plasmin. Re-combinant rt-PA began clinical trials in 1980 and won FDA approval in 1987. It has several advantages over streptokinase. First, t-PA acts almost exclusively on the plasminogen bound to a fibrin clot. In other words, its activity is relatively fibrin-specific: it dissolves clots only and carries a lower risk of systemic bleeding.
All antithrombotic medications carry bleeding risks. Thrombolytics fall in the highest risk category, and there are a number of contraindications to their use. Absolute contraindications for fibrinolysis in STEMI include prior intracranial hem-orrhage, suspected aortic dissection, active bleeding, significant closed-head or facial trauma within three months, and known structural cerebral vascular lesion.39
The patient’s age, sex, body weight and renal function influence bleeding risk as well. Bleeding events are associated with poorer long-term outcomes. Invasive reperfusion strategies carry fewer bleeding risks.
Heparin UF, bolus and infusion, is recom-mended in combination with either t-PA or streptokinase.
Choosing among therapies There’s an in-creased emphasis today on the concept that pharmacological and interventional strate-gies should be risk-directed.
The goals for management of NSTEMI patients are rapid and accurate risk strati-fication, appropriate and institution-spe-cific triage to interventional versus medical strategies, and optimal pharmacological therapy.
High-risk features that direct the clinician toward PCI as the preferred modality in-clude:
Elevated cardiac markers (troponin and/or CK-MB)
Elevated inflammatory markers (CRP >3)
age >65
Presence of ST-T wave changes
Diabetes
TIMI risk score >5
Clinical instability in suspected NSTE-ACS. 40
2007 ACC/AHA guidelines suggest that prompt mechanical revascularization is as-sociated with the best clinical outcomes. Choosing the most appropriate reperfusion strategy -- PCI or fibrinolysis -- depends on the physician’s assessment of patient risk, the time since the onset of symptoms, and the availability of appropriate PCI and sur-gical facilities.
However, the potential mortality benefit as-sociated with PCI might be lost if door-to-balloon time is delayed by more than one hour compared to door-to-needle time for fibrinolytic therapy. For every ten-minute delay in performing PCI, there’s a 1% re-
•
•
•
•
•
•
•
duction in the mortality benefit that PCI confers relative to fibrinolysis.41
A final thought about our patient So what happened to our patient -- the 60 year old woman, chest pain 10/10, ST elevations in the anterior leads, hemodynamically un-stable with a heart rate of 110 and BP of 90/50? The one who “doesn’t look good, is cool and clammy, nauseated and short of breath”?
How her story ends is in many ways deter-mined by where it begins: in other words, on the availability of first-line care. Let’s say she comes to a high-volume interventional cardiology tertiary care center where she receives prompt invasive revascularization with adjunctive pharmacological support and her door-to-device time is 55 minutes.
In this best-case scenario, her EKG returns to normal, she’s pain-free and discharged two days later. In fact she feels so good that she and her husband go ahead and book that cruise they’ve been dreaming of. Sounds like a storybook ending, and it is.
But what if her symptoms present while she’s on that cruise? Her outcome could be very different. Time is muscle, and it takes time to arrange transport from the ship to the nearest hospital. And the hos-pital may or may not have a cath lab, which means revascularization would come in the form of noninvasive pharmacotherapy with thrombolytics.
Let’s say the patient has an undiagnosed ulcer and develops a GI bleed, is hemody-namically compromised and unstable. In this case she’s transferred to the mainland the next day for cardiac cath, a stent is placed, and her EF is 30%. Not a story-book ending at all.
And that brings us back to the point of this article. Medication management in today’s cardiac cath lab is challenging, exciting and demanding, with new meds, equipment and procedures being introduced constantly and
AND THE BEAT GOES ON (cont...)
3� CORONARY HEART ™

EDUCATION
ACC/AHA guidelines changing frequently to reflect evidence-based medicine.
Keeping up to date on the why and how of what we do is critical. This knowledge makes it possible for us to understand, em-brace and anticipate the pharmacological management of all our cath lab patients.
References:
www.ClinicalMedicineToday.com, p. 4.
http://www.fasebj.org/cgi/content/full/19/6/671e. Clot Busters!! Discovery of Thrombolyt-ic Therapy for Treating Heart Attack & Stroke.
www.reopro.com.
http://www.fasebj.org/cgi/content/full/19/6/671e.
http://enwikipedia.org/wiki/heparin-e.
Cohen M, Diez J et al. Pharmacoinvasive Management of Acute Coronary Syndrome: Incorporating the 2007 ACC/AHA Guide-lines. The CATH (Cardiac Catheterization and Antithrombotic Therapy in the Hospital) Clinical Consensus Panel Report-III. Journal of Invasive Cardiology, Vol.19, No.12, December 2007, p.530.
www.lovenox.com.
www.theheart.org. Recent clinical trial data on adjunctive pharmacology in ACS patients undergoing PCI.
www.ClinicalMedicineToday.com. Manag-ing Patients with Acute Coronary Syndromes: Evidence Based Approaches to Improve STEMI and UA/NSTEMI Outcomes, p. 8.
Cohen M, Diez J et al. Pharmacoinvasive Management of Acute Coronary Syndrome: Incorporating the 2007 ACC/AHA Guide-lines. The CATH (Cardiac Catheterization and Antithrombotic Therapy in the Hospital) Clinical Consensus Panel Report-III. Journal of Invasive Cardiology, Vol. 19, No. 12, December 2007, p. 529.
Cohen D et al. Economic evaluation of bivalirudin with provisional glycoprotein llB/lllA inhibition versus heparin with routine glycoprotein llB/lllA inhibition for percutane-ous coronary intervention: Results from the REPLACE-2 trial. Journal of the American College of Cardiology, November 2004: 44, pp. 1792-1800.
www.angiomax.com.
Cohen M, Diez J et al. Pharmacoinvasive Management of Acute Coronary Syndrome:
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Incorporating the 2007 ACC/AHA Guide-lines. The CATH (Cardiac Catheterization and Antithrombotic Therapy in the Hospital) Clinical Consensus Panel Report-III. Journal of Invasive Cardiology, Vol.19, No. 12, December 2007, p. 533.
http://www.argatroban.com/about/arga-troban_htm.
http://en.wikipedia.org/wiki/Antiplatelet_drug.
http://starryskies.com/articles/dln/1-01/asprin.html. The Science of Aspirin and Willows.
http://en.wikipedia.org/wiki/Aspirin.
Cohen M, Diez J et al. Pharmacoinvasive Management of Acute Coronary Syndrome: Incorporating the 2007 ACC/AHA Guide-lines. The CATH (Cardiac catheterization and Antithrombotic Therapy in the Hospital) Clinical Consensus Panel Report-III. Journal of Invasive Cardiology, Vol.19, No. 12, December 2007, p. 532.
www.ClinicalMedicineToday.com. Manag-ing Patients with Acute Coronary Syndromes: Evidence Based Approaches to Improve STEMI and UA/NSTEMI Outcomes, p. 9.
http://en.wikipedia.org/wiki/Clopidogrel.
www.ClinicalMedicineToday.com. Manag-ing Patients with Acute Coronary Syndromes: Evidence Based Approaches to Improve STEMI and UA/NSTEMI Outcomes, p. 8.
Cohen M, Diez J et al. Pharmacoinvasive Management of Acute Coronary Syndrome: Incorporating the 2007 ACC/AHA Guide-lines. The CATH (Cardiac Catheterization and Antithrombotic Therapy in the Hospital) Clinical Consensus Panel Report-III. Journal of Invasive Cardiology, Vol.19, No. 12, December 2007, p. 53.
Cost information supplied by Eastern Shore Pharmacy, Salisbury, Maryland, February 2008.
http://en.wikipedia.org/wiki/Ticlid.
http://en.wikipedia.org/wiki/Chimera_%28pro-tein%29.
http://reopro.com/news_information/faqs.jsp.
Peninsula Regional Medical Center, pharmacy cost list, 2007.
http://www.reopro.com/pdf/AB39432_926252_2.28.06.pdf.
Cohen M, Diez J et al. Pharmacoinvasive Management of Acute Coronary Syndrome: Incorporating the 2007 ACC/AHA Guide-lines. The CATH (Cardiac Catheterization and Antithrombotic Therapy in the Hospital) Clini-cal Consensus Panel Report-III. Journal of Invasive Cardiology, Vol.19, No. 12, December 2007, p. 529.
http://en.wikipedia.org/wiki/Integrilin.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
http://www.integrilin.com/efficacy_introduc-tion.html.
http://www.integrilin.com/full_prescribing_in-formation.html.
Peninsula Regional Medical Center, pharmacy cost list, 2007.
www.ClinicalMedicineToday.com. Managing Patients with Acute Coronary Syndromes, p. 10.
http://en.wikipedia.org/wiki/Aggrastat.
Bergman SR, Learch RA, Fox KA et al. Temporal dependence of beneficial effects of coronary thrombolysis characterized by positron tomography. American Journal of Medicine, June 1982: 73, pp. 573-58.
www.ClinicalMedicineToday.com. Managing Patients with Acute Coronary Syndromes, p. 3.
http://www.fasebj.org/cgi/content/full/19/6/671e. ClotBusters!! Discovery of Thrombolytic Therapy for Treating Heart Attack & Stroke.
http://www.madsci.com/manu/ches_thr.htm.
www.ClinicalMedicineToday.com. Managing Patients with Acute Coronary Syndromes, p. 3.
www.ClinicalMedicineToday.com. Managing Patients with Acute Coronary Syndromes, p. 3.
Editor’s Note: The information presented in this article is intended to serve as an educational aid only and provide the reader with a reference; it is not intended to offer medical advice nor substitute medical practice, diagnosis and/or treatment. The ultimate responsibility for patient care resides with the health care pro-fessional using his or her professional license, experience, and knowledge of the patient. All products are registered trademarks by their re-spective manufacturers, and are approved for use in the United States. Please check with your local government or regulatory agency for additional information. Dosing and/or pric-ing information is direct from manufacturers; please consult with appropriate package in-serts or information before administering any medication or pharmacologic agent listed in this article.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
CORONARY HEART ™ 3�

CONFERENCECALENDER
May 4 - 6
17th Annual All That Jazz - Nurse/Tech CourseNew Orleans, LA
www.allthatjazz.org
May 13 - 16
EuroPCR with 2-Day Nurse and Technician Programme
Barcelona, Spain
www.europcronline.com
May 30 - 31
Emergency CV Care 2008Fairmont Hotel, Washington, D.C.
www.acc.org
July 11 -12
4th Annual Heart & Vascular ConferenceBoyne Falls, MI
www.northernhealth.org/lubdub&splash
July 26 - 29
14th World Congress on Heart DiseaseToronto, Canada
www.cardiologyonline.com
July 28 - 30
Recent Advances in Invasive and Noninvasive ImagingMiami, Florida
www.register-crf.org/imaging08.aspx
August 30 - September 3
European Society of Cardiology (ESC) Congress 2008Munich, Germany
www.escardio.org
September 5 - 6
Mechanics of an EP Study, CEU# 13South Austin Hospital, Austin, TX
www.tcainstitute.com
September 10 - 13
9th Annual New Cardiovascular Horizons New Orleans, LA
www.newcvhorizons.com
October 12 - 17
Transcatheter Cardiovascular Therapeutics (TCT 2008)Washington, D.C.
www.tct2008.com
Next Edition
July / August 2008
Mobile Cath Labs
Cardiac Monitoring Systems
Site Visit: Memorial Hermann Southwest Heart & Vascular Institute, TX
For advertising contact:Brett Goldfi ne Leonard Media Group Phone: 215-675-9133 Ext. 226 E-mail: [email protected]
Write for us
Share your expertise with your fellow workers by contributing an article to Coronary Heart. All topics related to the cath lab are welcome.
For more information and a copy of Coronary Heart’s author guidelines, email the Clinical Editor Tim Larner at [email protected]
•
•
•
CONFERENCES
38 CORONARY HEART ™

CORONARY HEART ™ 3�
EMPLOYMENT ADVERTISING
WE PRACTICE CARDIAC NURSING ATA HIGHER LEVEL. SARAH’S.Every day Sarah’s able to focus on caring for patients at the bedside, and at the sametime grow her career at Pitt County Memorial Hospital. Nurses like Sarah are part ofour leadership and have made us the region’s healthcare leader.
www.pcmhcareers.com/heartGet the full story of our Nursing family at:
• Exceptional Greenville, NC location
• Magnet certification and clinical ladders
• Flexible shift and schedule options
• Ongoing expansion across our system,which includes the opening of the EastCarolina Heart Institute in 2009
• Training and education at every level
We are diverse talents brought together by a common dedication: EOE.

LAD LCXLCX
ON YOUR MARK,GET SET, AND GO!IN ONLY 90 MINUTESWITH FEMOSTOP®.
CONSISTENT PRESSURESINCE 1992
Femostop® has been providing consistent pressure since 1992. Used on over 5 million patients, the controlled pressure provided by Femostop® provides safe, rapid and effective ambulation as an alternative to manual compression.
FemoStop® is proven to ambulate patients faster, while maintaining a low rate of complications. A recent report from Freeman Hospital shows overall vascular complications of less than 1%when FemoStop® is used in diagnostic patients ambulated after 90 minutes1.
1. Gall, S.1, Natarajan, A.1, Zaman, A.1. “Rapid ambulation after coronary angiography via femoral artery access: A prospective study of 1000 patients.”1 Freeman Hospital, Newcastle, UK. The Journal of Invasive Cardiology, March 2006 issue.
www.radi.se