926277 Coronary Heart Disease
72
M Chadi Alraies 1 Coronary Heart Coronary Heart Disease Disease M Chadi Alraies M.D. M Chadi Alraies M.D.
-
Upload
aditya-gore -
Category
Documents
-
view
222 -
download
0
Transcript of 926277 Coronary Heart Disease

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 1/72
M Chadi Alraies 1
Coronary HeartCoronary Heart
DiseaseDisease
M Chadi Alraies M.D.M Chadi Alraies M.D.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 2/72
2M Chadi Alraies
The main reason to invest in prevention is The main reason to invest in prevention isto promote health and extend life, improveto promote health and extend life, improvefunctioning and prevent suffering.functioning and prevent suffering.
"The Role of Prevention in Health Reform", Russell,"The Role of Prevention in Health Reform", Russell,Louise B., Ph.D., The New England Journal of Medicine,Louise B., Ph.D., The New England Journal of Medicine, July 29, 1993;329 (5):352 July 29, 1993;329 (5):352--354.354.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 3/72
3M Chadi Alraies
General considerationsGeneral considerations
number one killer in thenumber one killer in theUnited States andUnited States and
worldwide. worldwide.
Every minute,Every minute, anan American dies of American dies of coronary heart disease.coronary heart disease.
Coronary heart diseaseCoronary heart diseaseafflicts overafflicts over 1313 millionmillion Americans. Americans.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 4/72
4M Chadi Alraies
The estimated cost for cardiovascular disease in The estimated cost for cardiovascular disease in
1994 by the American Heart Association is1994 by the American Heart Association is 128 128
billion dollarsbillion dollars..

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 5/72
5M Chadi Alraies
An 82 An 82--yearyear--old woman presents for her annual examination. Sheold woman presents for her annual examination. Shehas hypertension and is on chronic has hypertension and is on chronic --blocker therapy. She deniesblocker therapy. She deniesall cardiac symptoms. She takes a daily 1all cardiac symptoms. She takes a daily 1--mile walk, and hermile walk, and her
exercise tolerance has not changed during the past year.exercise tolerance has not changed during the past year. Physical examination shows a blood pressure of 138/86 mm Hg,Physical examination shows a blood pressure of 138/86 mm Hg,
a regular pulse of 80/min, and a respiratory rate of 16/min. Hera regular pulse of 80/min, and a respiratory rate of 16/min. Herjugular venous pressure is 10 cm H2O, her carotid upstrokes arejugular venous pressure is 10 cm H2O, her carotid upstrokes arenormal, and her lungs are clear. Cardiac examination reveals anormal, and her lungs are clear. Cardiac examination reveals a
normal S1, a single S2, and a grade 3/6 early systolic murmur atnormal S1, a single S2, and a grade 3/6 early systolic murmur atthe upper left sternal border that radiates to her carotids.the upper left sternal border that radiates to her carotids. Abdominal examination is benign, and there is 1+ peripheral Abdominal examination is benign, and there is 1+ peripheraledema. Laboratory data are remarkable for a total cholesterol of edema. Laboratory data are remarkable for a total cholesterol of 210 mg/dL (5.43 mmol/L), with an LDL cholesterol of 110210 mg/dL (5.43 mmol/L), with an LDL cholesterol of 110mg/dL (2.84 mmol/L).mg/dL (2.84 mmol/L).
Her echocardiogram from 2 years ago showed moderate calcificHer echocardiogram from 2 years ago showed moderate calcificaortic stenosis, with a maximum aortic velocity of 3.6 m/saortic stenosis, with a maximum aortic velocity of 3.6 m/s(normal, <1.5 m/s) a mean gradient of 30 mm Hg (normal, <5(normal, <1.5 m/s) a mean gradient of 30 mm Hg (normal, <5mm Hg) and a valve area of 1.2 cm2 (normal, >2 cm2) withmm Hg) and a valve area of 1.2 cm2 (normal, >2 cm2) withnormal left ventricular systolic function. Echocardiography now normal left ventricular systolic function. Echocardiography now shows a maximum aortic jet velocity of 4.2 m/s, mean gradientshows a maximum aortic jet velocity of 4.2 m/s, mean gradientof 44 mm Hg, and a valve area of 1.0 cm2.of 44 mm Hg, and a valve area of 1.0 cm2.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 6/72
6M Chadi Alraies
W hich is the most appropriate next step? W hich is the most appropriate next step?
A Reassurance A Reassurance
B Begin a cardiac rehabilitation programB Begin a cardiac rehabilitation program C Begin hydrochlorothiazideC Begin hydrochlorothiazide
D Start statin therapy D Start statin therapy
E Refer for aortic valve replacementE Refer for aortic valve replacement
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 7/72
7M Chadi Alraies
R isk factorsR isk factors
Abnormal lipids Abnormal lipids
Smoking Smoking
HypertensionHypertension
Diabetes mellitusDiabetes mellitus
Abdominal obesity Abdominal obesity
Psychosocial factorsPsychosocial factors
Consumption of too few fruitsConsumption of too few fruits
and vegetables.and vegetables.
Too much alcohol Too much alcohol
Lack of regular physical activity.Lack of regular physical activity.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 8/72
M Chadi Alraies 8
What is the number one What is the number one preventable cause of preventable cause of
cardiovascular diseasecardiovascular disease worldwide? worldwide?
SMOKING!SMOKING!

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 9/72
M Chadi Alraies 9
1 1 year after quitting, the year after quitting, the
risk of coronary heartrisk of coronary heart
disease decreases bydisease decreases by 5050%%
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 10/72
M Chadi Alraies 10
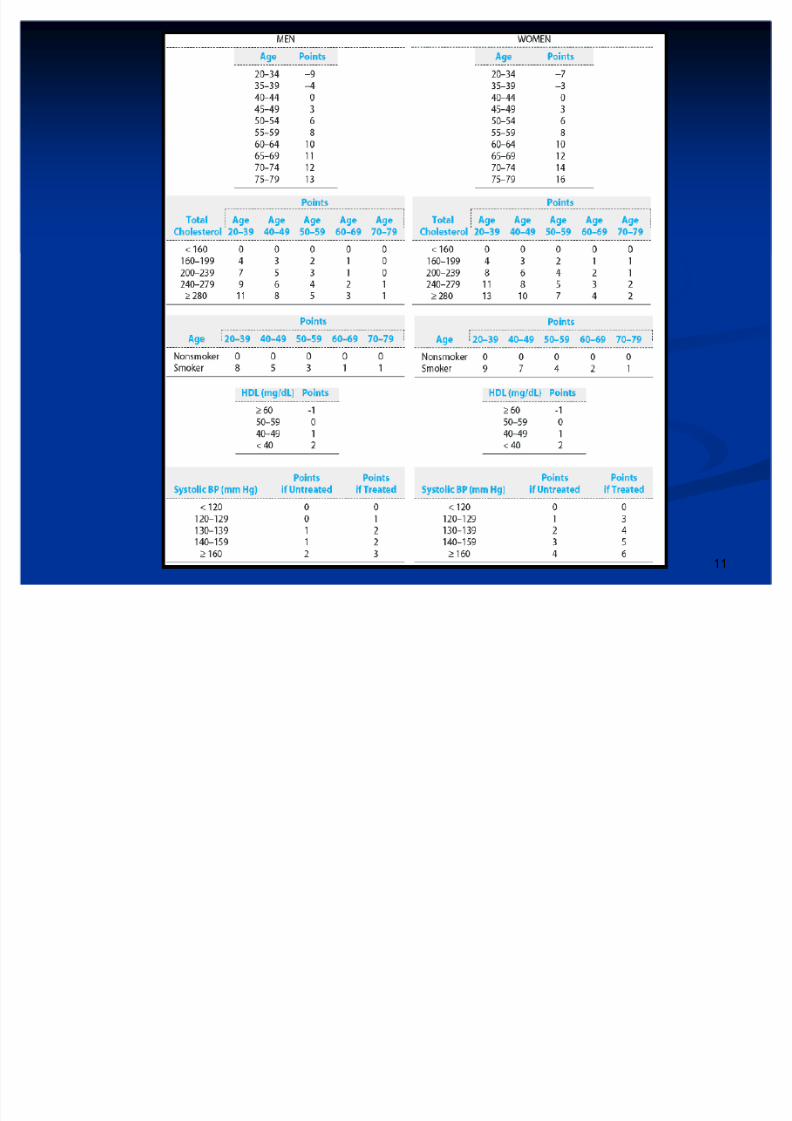
Framingham scoreFramingham score
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 11/72
11M Chadi Alraies
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 12/72
12M Chadi Alraies
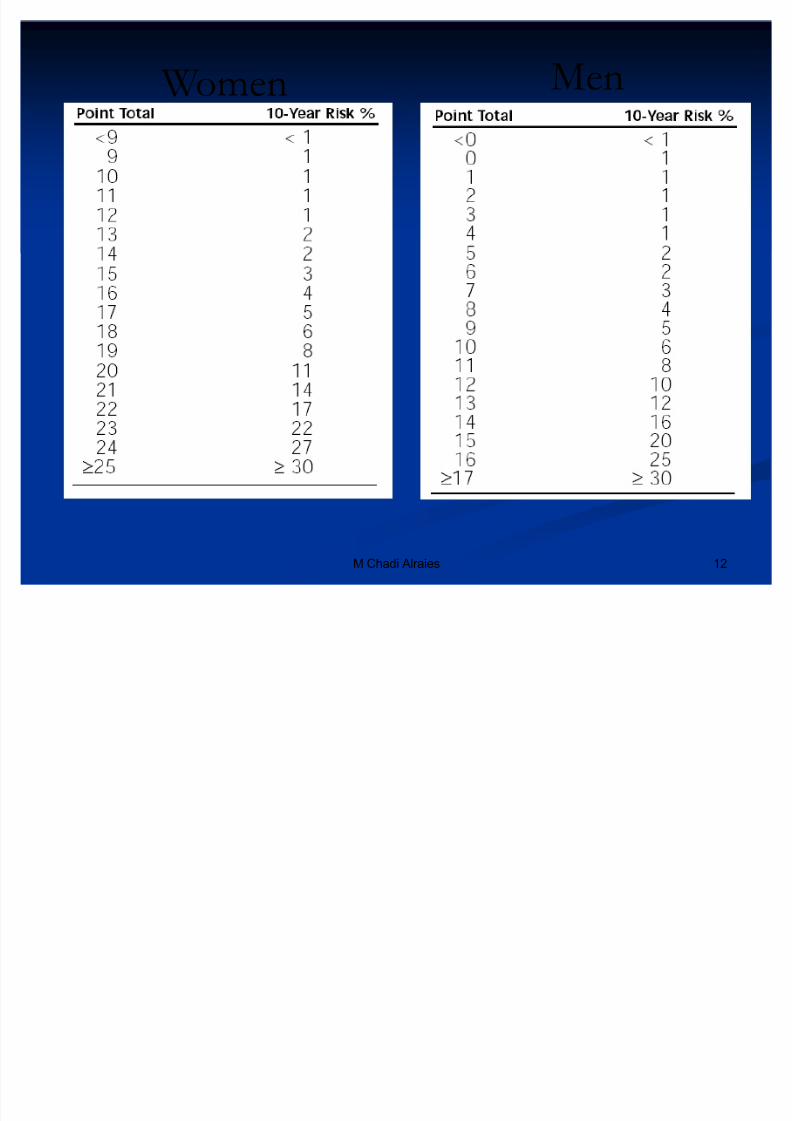
W omen Men
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 13/72
M Chadi Alraies 13
Define the metabolicDefine the metabolic
syndrome?syndrome?
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 14/72
14M Chadi Alraies
The metabolic syndrome The metabolic syndrome
Three or more of the following: Three or more of the following:
Abdominal obesity Abdominal obesity
Triglycerides
Triglycerides 150150 mg/dLmg/dL
HDL cholesterol <HDL cholesterol < 4040 mg/dL for men and <mg/dL for men and < 5050mg/dL for womenmg/dL for women
Fasting glucoseFasting glucose 110110 mg/dLmg/dL
Hypertension.Hypertension.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 15/72
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 16/72
16M Chadi Alraies
A A 7272--yearyear--old woman is seen for a routine office evaluation toold woman is seen for a routine office evaluation toestablish care. Past medical history includes only hypertension,establish care. Past medical history includes only hypertension,
hyperlipidemia, and a familial history of coronary artery disease.hyperlipidemia, and a familial history of coronary artery disease.She does not smoke. She is active and walks daily and deniesShe does not smoke. She is active and walks daily and deniesangina, dyspnea, fatigue, and edema.angina, dyspnea, fatigue, and edema.
Physical examination reveals a blood pressure of Physical examination reveals a blood pressure of 128128//7070 mmmmHg. There are no carotid bruits. There is a normal SHg. There are no carotid bruits. There is a normal S11 and aand a
physiologically split Sphysiologically split S22. There is a grade. There is a grade 22//66 midsystolic murmurmidsystolic murmurthat does not radiate and is best heard at thethat does not radiate and is best heard at the 22nd right intercostalnd right intercostalspace. The rest of the physical examination is unrevealing.space. The rest of the physical examination is unrevealing.
W hich of the following diagnostic tests is most appropriate at W hich of the following diagnostic tests is most appropriate atthis time?this time?
A No further testing at this time A No further testing at this time B Transthoracic echocardiography B Transthoracic echocardiography
C ElectronC Electron--beam C T beam C T
D Treadmill stress echocardiogramD Treadmill stress echocardiogram
EE 2424--hour ambulatory electrocardiographic monitoring hour ambulatory electrocardiographic monitoring
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 17/72
M Chadi Alraies 17
PathophysiologyPathophysiology

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 18/72
18M Chadi Alraies
Lipid metabolism in relation toLipid metabolism in relation to
formation of atherosclerotic lesionsformation of atherosclerotic lesions
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 19/72
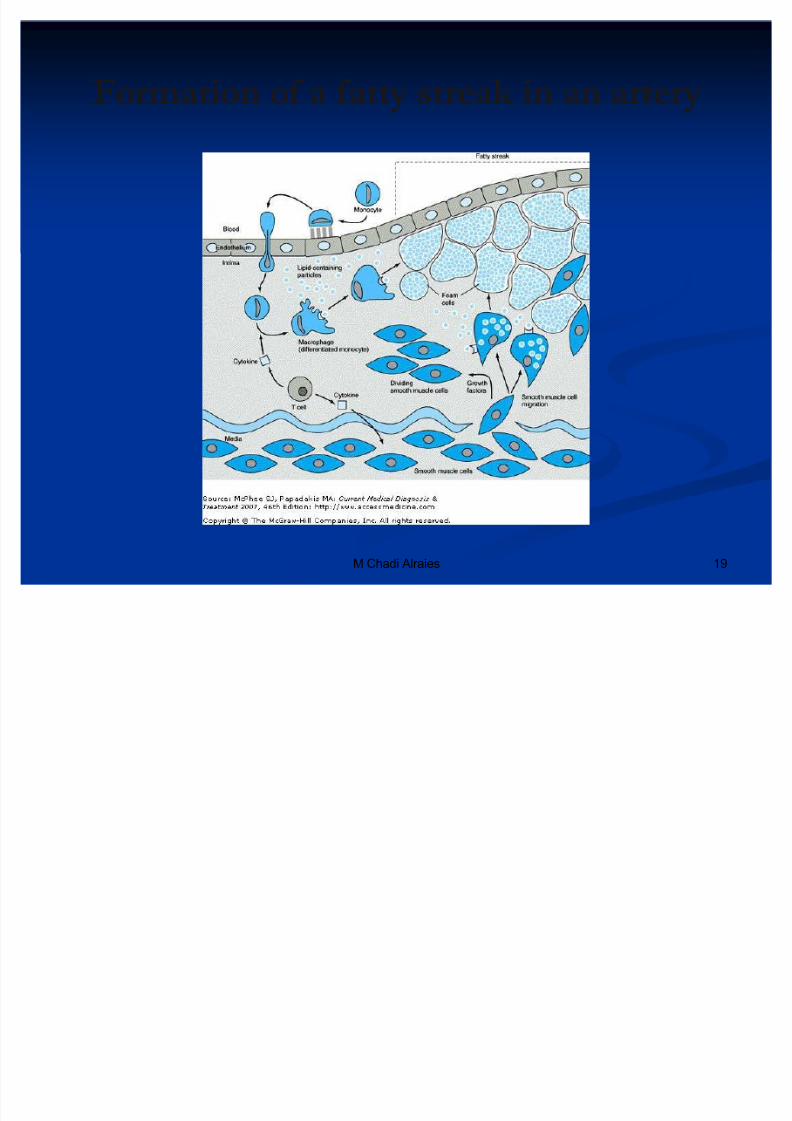
19M Chadi Alraies
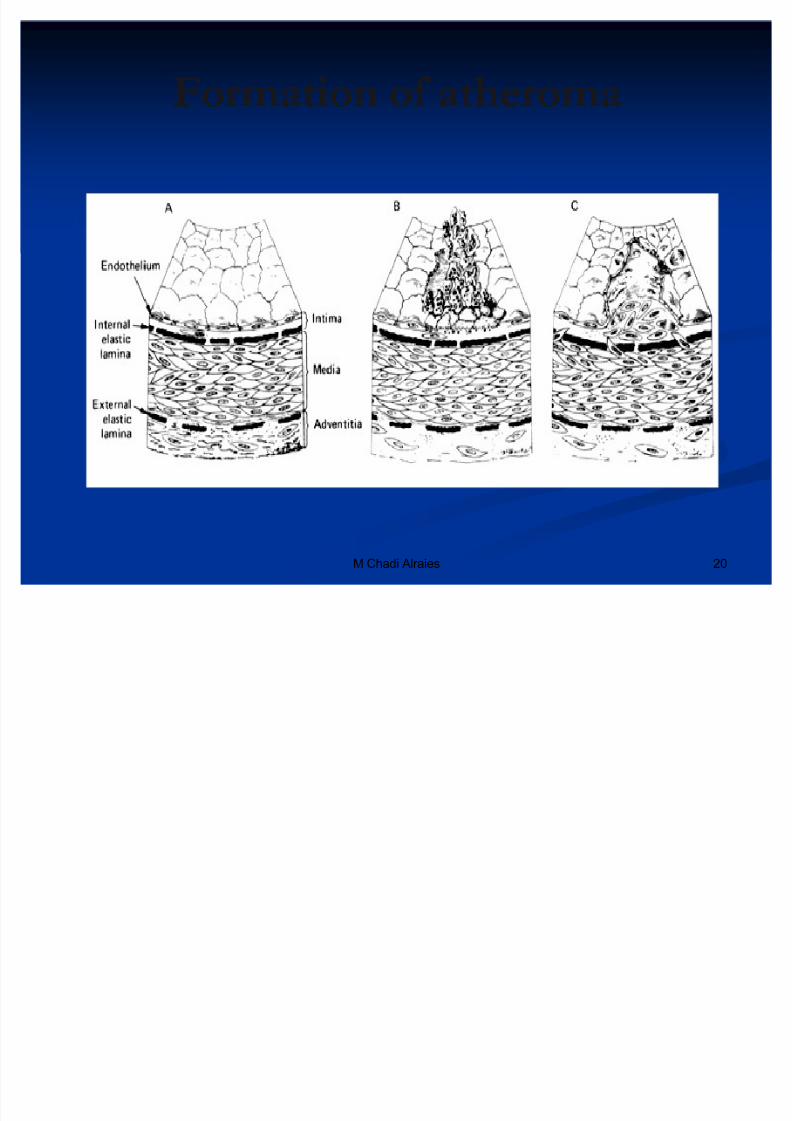
Formation of a fatty streak in an arteryFormation of a fatty streak in an artery
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 20/72
20M Chadi Alraies
Formation of atheromaFormation of atheroma
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 21/72
21M Chadi Alraies
Plaque rupturePlaque rupture
Many atherosclerotic plaques remain stable orMany atherosclerotic plaques remain stable or
progress only gradually.progress only gradually.
Rupture, often related to the inflammatory Rupture, often related to the inflammatory process.process.
The rupture causes« The rupture causes«
Turbulent flow Turbulent flow
Extrusion of lipids and fatty gruelExtrusion of lipids and fatty gruel
Exposure of tissue factorExposure of tissue factor
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 22/72
22M Chadi Alraies
Plaque rupturePlaque rupture
All result in a cascade of events culminating in All result in a cascade of events culminating inintravascular thrombosis.intravascular thrombosis.
The outcome of these events is« The outcome of these events is«
Complete vessel occlusion.Complete vessel occlusion. Partial vessel occlusion (causing the symptoms of unstablePartial vessel occlusion (causing the symptoms of unstable
angina or myocardial infarction)angina or myocardial infarction)
Restabilization often with more severe stenosis.Restabilization often with more severe stenosis.
Transient occlusion and/or embolization of platelet and
Transient occlusion and/or embolization of platelet andthrombin debris, which may result in elevation in serumthrombin debris, which may result in elevation in serum
troponin, predispose to clinical events and portend atroponin, predispose to clinical events and portend a worse prognosis. worse prognosis.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 23/72
M Chadi Alraies 23
Plaque rupturePlaque rupture
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 24/72
24M Chadi Alraies
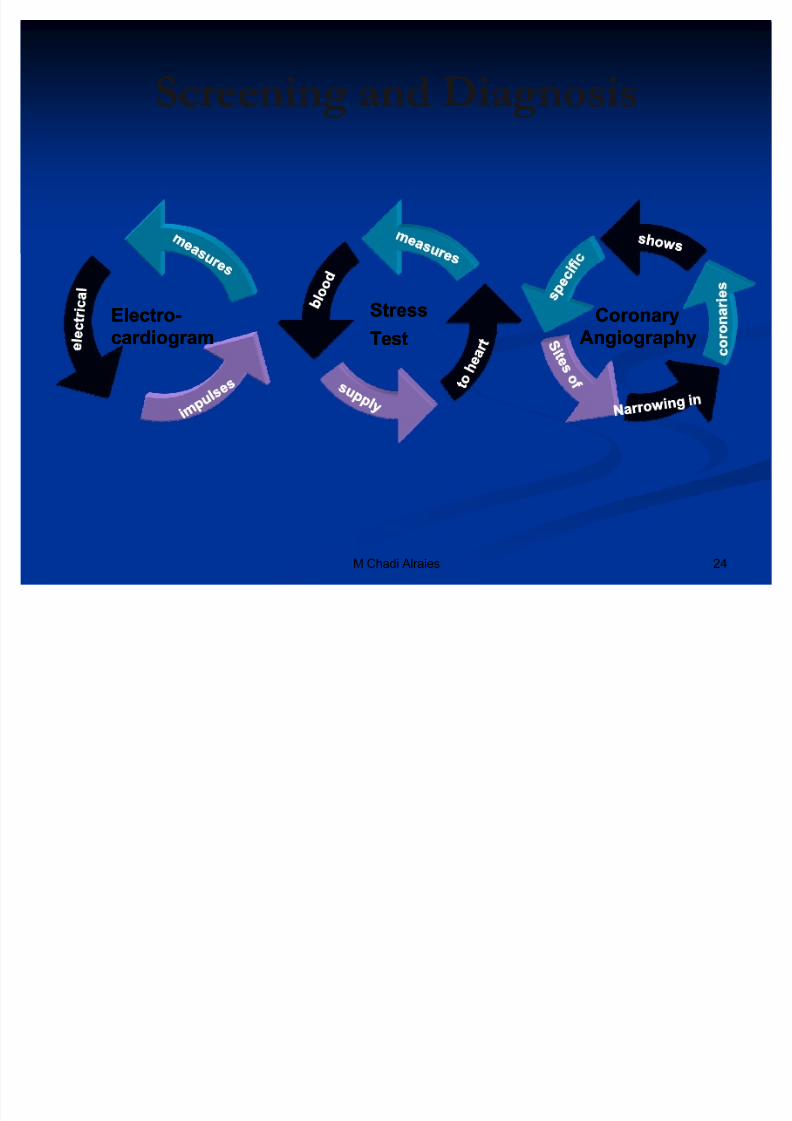
Screening and DiagnosisScreening and Diagnosis
StressStress
TestTest
CoronaryCoronary
AngiographyAngiography
ElectroElectro--
cardiogramcardiogram
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 25/72
25M Chadi Alraies
A A 2222--yearyear--old women who isold women who is 1616 weeks pregnant is evaluated for weeks pregnant is evaluated foraa 22--hour history of severe anterior chest pain radiating to herhour history of severe anterior chest pain radiating to hermid back. She is a tall, thin woman with a pectus abnormality of mid back. She is a tall, thin woman with a pectus abnormality of
her chest and long, thin fingers. Her blood pressure isher chest and long, thin fingers. Her blood pressure is 140140//8080mm Hg, her pulse ismm Hg, her pulse is 9494/min and regular, and her respiratory rate/min and regular, and her respiratory rateisis 2424/min. Her chest wall is diffusely mildly tender to palpation./min. Her chest wall is diffusely mildly tender to palpation.Her lungs are clear to auscultation. Cardiac auscultation shows aHer lungs are clear to auscultation. Cardiac auscultation shows anormal Snormal S11, a physiologically split S, a physiologically split S22, and a grade, and a grade 22//66 diastolicdiastolic
decrescendo murmur at the left sternal border. There is nodecrescendo murmur at the left sternal border. There is noperipheral edema. Her electrocardiogram shows only nonspecificperipheral edema. Her electrocardiogram shows only nonspecificS TS T-- T changes. Oxygen saturation by pulse oximetry on room air T changes. Oxygen saturation by pulse oximetry on room airisis 9999%. Her D%. Her D--dimer level is mildly elevated.dimer level is mildly elevated.
W hich is the most likely cause of her chest pain? W hich is the most likely cause of her chest pain? A Pulmonary embolus A Pulmonary embolus
B Acute myocardial infarctionB Acute myocardial infarction
C Aortic dissectionC Aortic dissection
D CostochondritisD Costochondritis
E PericarditisE Pericarditis

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 26/72
M Chadi Alraies 26
Primary & SecondaryPrimary & Secondary
Prevention of CoronaryPrevention of Coronary
Heart DiseaseHeart Disease
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 27/72
M Chadi Alraies 27
A H A/A CC Secondary A H A/A CC SecondaryPrevention for PatientsPrevention for Patients
With Coronary and Other With Coronary and Other Vascular Disease Vascular Disease
20062006 UpdateUpdate
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 28/72
28M Chadi Alraies
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 29/72
29M Chadi Alraies
Coronary and Other VascularCoronary and Other Vascular
DiseaseDisease
Established coronary disease.Established coronary disease.
Atherosclerotic vascular disease: Atherosclerotic vascular disease:
PeripheralPeripheral arterialarterial disease,disease, Atherosclerotic aortic disease, and Atherosclerotic aortic disease, and
Carotid artery disease.Carotid artery disease.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 30/72
30M Chadi Alraies
SMOKINGSMOKING
Goal: Complete cessation. No exposure toGoal: Complete cessation. No exposure toenvironmental tobacco smoke.environmental tobacco smoke.
Ask about tobacco use status at every visit. Ask about tobacco use status at every visit.
Advise every tobacco user to quit. Advise every tobacco user to quit. Assess the tobacco user·s willingness to quit. Assess the tobacco user·s willingness to quit. Assist by counseling and developing a plan for quitting. Assist by counseling and developing a plan for quitting. Arrange follow Arrange follow--up, referral to special programs, orup, referral to special programs, or
pharmacotherapy (including nicotine replacement andpharmacotherapy (including nicotine replacement andbupropion).bupropion).
Urge avoidance of exposure to environmental tobaccoUrge avoidance of exposure to environmental tobaccosmoke at work and home.smoke at work and home.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 31/72
31M Chadi Alraies
A A 5555--yearyear--old man is evaluated for cough, scant clearold man is evaluated for cough, scant clear--toto--yellow yellow sputum, and malaise of sputum, and malaise of 33 days' duration. He has not had fever,days' duration. He has not had fever,chills, wheezing, or pleuritic chest pain, or recent contact withchills, wheezing, or pleuritic chest pain, or recent contact with
anyone who has been ill. He has aanyone who has been ill. He has a 4040--pack pack--year smoking history year smoking history and has had similar symptoms three times in the pastand has had similar symptoms three times in the past 66 months,months,feeling well in the intervals between episodes.feeling well in the intervals between episodes.
On physical examination, temperature isOn physical examination, temperature is 3737..22 °°C ( C (9999..00 °°F), andF), andpulse rate, respiration rate, and blood pressure are normal. Thepulse rate, respiration rate, and blood pressure are normal. The
cardiopulmonary examination is normal, including clear lungs oncardiopulmonary examination is normal, including clear lungs onauscultation with no signs of consolidation.auscultation with no signs of consolidation.
W hich of the following is the most appropriate initial smoking W hich of the following is the most appropriate initial smoking--cessation management step during this visit?cessation management step during this visit?
A Recommend nicotine gum A Recommend nicotine gum B Provide a clear, personalized message to the patientB Provide a clear, personalized message to the patient
C Refer the patient to a behavioralC Refer the patient to a behavioral--modification programmodification program
D Prescribe bupropionD Prescribe bupropion
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 32/72
32M Chadi Alraies
BLOOD PRESSURE CON TROLBLOOD PRESSURE CON TROL
Goal:Goal: For patients withFor patients with blood pressureblood pressure140140//9090 mm Hg (ormm Hg (or 130130//8080 mm Hg formm Hg forindividuals with chronic kidney disease orindividuals with chronic kidney disease or
diabetes.diabetes. Initiate or maintain lifestyle modificationInitiate or maintain lifestyle modification³ ³
weight control; increased physical activity; weight control; increased physical activity;alcohol moderation; sodium reduction; andalcohol moderation; sodium reduction; andemphasis on increased consumption of freshemphasis on increased consumption of freshfruits, vegetables, and low fruits, vegetables, and low--fat dairy products.fat dairy products.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 33/72
33M Chadi Alraies
BLOOD PRESSURE CON TROLBLOOD PRESSURE CON TROL
Add blood pressure medication, Add blood pressure medication,
Treating initially with ß Treating initially with ß--blockers and/or ACEblockers and/or ACE
inhibitors.inhibitors. Addition of other drugs such as thiazides as Addition of other drugs such as thiazides as
needed to achieve goal blood pressureneeded to achieve goal blood pressure..
Use JNCUse JNC 77
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 34/72
34M Chadi Alraies
A 55 A 55--yearyear--old man is evaluated for epigastric discomfort that hasold man is evaluated for epigastric discomfort that hasbeen increasing in frequency despite the use of antacids. Thebeen increasing in frequency despite the use of antacids. Thediscomfort occurs with exercise, but at times he is able todiscomfort occurs with exercise, but at times he is able toexercise without provocation of his symptoms. He has no otherexercise without provocation of his symptoms. He has no other
medical conditions and takes only an 81medical conditions and takes only an 81--mg aspirin daily andmg aspirin daily andoccasional chondroitin sulfate for joint aches.occasional chondroitin sulfate for joint aches.
Physical examination, including vital signs and cardiacPhysical examination, including vital signs and cardiacexamination, is normal. Electrocardiogram shows normal sinusexamination, is normal. Electrocardiogram shows normal sinusrhythm with normal waveforms. Lipid tests show totalrhythm with normal waveforms. Lipid tests show total
cholesterol of 199 mg/dL (5.15 mmol/L), LDL cholesterol of cholesterol of 199 mg/dL (5.15 mmol/L), LDL cholesterol of 131 mg/dL (3.39 mmol/L), and HDL cholesterol of 35 mg/dL131 mg/dL (3.39 mmol/L), and HDL cholesterol of 35 mg/dL(0.91 mmol/L).(0.91 mmol/L).
W hat is the most appropriate next step in the evaluation of this W hat is the most appropriate next step in the evaluation of thispatient?patient? A Measurement of C A Measurement of C--reactive proteinreactive protein
B Measurement of coronary calcium by electronB Measurement of coronary calcium by electron--beam C T beam C T
C Measurement of serum homocysteineC Measurement of serum homocysteine
D Exercise electrocardiographic stress testD Exercise electrocardiographic stress test
E Exercise echocardiogramE Exercise echocardiogram

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 35/72
M Chadi Alraies 35
LIPIDLIPID
MANAGEMEN TMANAGEMEN T
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 36/72
M Chadi Alraies 36
LDLLDL
´The lower the betterµ´The lower the betterµ
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 37/72
M Chadi Alraies 37
HDLHDL
´The higher the betterµ´The higher the betterµ

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 38/72
38M Chadi Alraies
LIPID MANAGEMEN TLIPID MANAGEMEN T
1.1. Start dietary therapy.Start dietary therapy.2.2. Reduce intake of saturated fats (to <Reduce intake of saturated fats (to <77% of total% of total
calories),calories),3.3.
Cholesterol (to <Cholesterol (to <200200 mg/d).mg/d).4.4. LDLLDL--C <C <100100 mg/dLmg/dL5.5. nonnon--HDLHDL--C should be <C should be <130130 mg/dLmg/dL6.6. Adding plant stanol/sterols ( Adding plant stanol/sterols (22 g/d) and viscous fiberg/d) and viscous fiber
(>(>1010 g/d) will further lower LDLg/d) will further lower LDL--C.C.7.7. Encourage increased consumption of omegaEncourage increased consumption of omega--33 fatty fatty
acids in the form of fish or in capsule form ( acids in the form of fish or in capsule form (11 g/d)g/d)for risk reduction.for risk reduction.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 39/72
39M Chadi Alraies
LIPID MANAGEMEN TLIPID MANAGEMEN T
Assess fasting lipid profile in all patients, and Assess fasting lipid profile in all patients, and
within within 2424 hours of hospitalization for those withhours of hospitalization for those withan acute cardiovascular or coronary eventan acute cardiovascular or coronary event..
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 40/72
40M Chadi Alraies
LIPID MANAGEMEN TLIPID MANAGEMEN T
For hospitalized patients, initiate lipidFor hospitalized patients, initiate lipid--lowering medication aslowering medication asrecommended below before discharge according to the following recommended below before discharge according to the following schedule:schedule: LDLLDL--C should be <C should be <100100 mg/dL and«mg/dL and«
Further reduction of LDLFurther reduction of LDL--C to <C to <7070 mg/dL is reasonable.mg/dL is reasonable. If baseline LDLIf baseline LDL--C isC is 100100 mg/dL, initiate LDLmg/dL, initiate LDL--lowering drug therapy.lowering drug therapy.
If onIf on--treatment LDLtreatment LDL--C isC is 100100 mg/dL, intensify LDLmg/dL, intensify LDL--lowering drug lowering drug therapy (may require LDLtherapy (may require LDL--lowering drug combination.lowering drug combination.
If baseline LDLIf baseline LDL--C isC is 7070 toto 100100 mg/dL, it is reasonable to treat to LDLmg/dL, it is reasonable to treat to LDL--CC
<<7070 mg/dL.mg/dL. If triglycerides areIf triglycerides are 200200 toto 499499 mg/dL, nonmg/dL, non--HDLHDL--C should be <C should be <130130
mg/dL. And«mg/dL. And«
Further reduction of nonFurther reduction of non--HDLHDL--C to <C to <100100 mg/dL is reasonable.mg/dL is reasonable.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 41/72
41M Chadi Alraies
LIPID MANAGEMEN TLIPID MANAGEMEN T
Therapeutic options to Therapeutic options to reduce nonreduce non--HDL:HDL:
More intense LDLMore intense LDL--CC² ²lowering therapy lowering therapy
Niacin orNiacin or
Fibrate therapy Fibrate therapy
If triglycerides areIf triglycerides are 500500 mg/dL, therapeuticmg/dL, therapeutic
options to prevent pancreatitis are fibrate oroptions to prevent pancreatitis are fibrate or
niacin before LDLniacin before LDL--lowering therapy.lowering therapy.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 42/72
42M Chadi Alraies
(HMG(HMG--Co A) reductase inhibitors (statins)Co A) reductase inhibitors (statins)
Aggressive LDL lowering is associated with Aggressive LDL lowering is associated withgreater benefits.greater benefits. The Heart Protection Study (HPS), simvastatin The Heart Protection Study (HPS), simvastatin 4040
mg a day reduces vascular events by more thanmg a day reduces vascular events by more than 2020%.%. The PROVE The PROVE--I T trial showed that vascular eventsI T trial showed that vascular events
were reduced with more aggressive lipid lowering were reduced with more aggressive lipid lowering (atorvastatin(atorvastatin 8080 mg/d compared to pravastatinmg/d compared to pravastatin 4040
mg/d following an acute coronary syndrome),mg/d following an acute coronary syndrome),providing more evidence of "lower is better" providing more evidence of "lower is better"
The TN T ( Treating to New Targets) The TN T ( Treating to New Targets)
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 43/72
43M Chadi Alraies
(HMG(HMG--Co A) reductase inhibitors (statins)Co A) reductase inhibitors (statins)
Although true regression of plaque is Although true regression of plaque is
uncommon even with intensive lipid therapy (asuncommon even with intensive lipid therapy (asin the REVERSAL and AS TEROID trials),in the REVERSAL and AS TEROID trials),
progression can be prevented at least in theprogression can be prevented at least in theshort run in many patients.short run in many patients.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 44/72
44M Chadi Alraies
HDLHDL Has been shown to be Cardioprotective in theHas been shown to be Cardioprotective in the
Framingham Heart Study, and in retrospectiveFramingham Heart Study, and in retrospectiveanalyses of intervention trials such as the Coronary analyses of intervention trials such as the Coronary Primary Prevention Trial and the Multiple Risk Primary Prevention Trial and the Multiple Risk
Factor Intervention T
rialFactor Intervention T
rial55--77
The data were consistent with a The data were consistent with a 22%% toto 33%%decrease in CHD risk for each decrease in CHD risk for each 1 1 mg/dL mg/dL increase in HDLincrease in HDL,, after adjustment to control forafter adjustment to control forother risk factors.other risk factors.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 45/72
45M Chadi Alraies
Treatment of low HDL Treatment of low HDL
Niacin in high dosages ( Niacin in high dosages (22² ²33 g/d or more)g/d or more)
Gemfibrozil ( Gemfibrozil (600600 mg twice daily)mg twice daily)
A 32A 32 yearyear old woman is brought to the hospital with chest pain at rest after aold woman is brought to the hospital with chest pain at rest after a
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 46/72
46M Chadi Alraies
A 32 A 32--yearyear--old woman is brought to the hospital with chest pain at rest after aold woman is brought to the hospital with chest pain at rest after aparty. She has had similar pain previously, primarily in the morning and rarely party. She has had similar pain previously, primarily in the morning and rarely with exertion. The pain usually subsides spontaneously and occasionally is with exertion. The pain usually subsides spontaneously and occasionally isassociated with diaphoresis but rarely dyspnea. She almost lost consciousnessassociated with diaphoresis but rarely dyspnea. She almost lost consciousnessat work during the most recent episode. She smokes a half pack of cigarettes aat work during the most recent episode. She smokes a half pack of cigarettes a
week and has occasionally inhaled cocaine. She is otherwise healthy and takes week and has occasionally inhaled cocaine. She is otherwise healthy and takesno medications. She has no family history of coronary artery disease.no medications. She has no family history of coronary artery disease. Her blood pressure is 128/70 mm Hg and pulse rate is 72/min. There is noHer blood pressure is 128/70 mm Hg and pulse rate is 72/min. There is no
neck vein distention or carotid bruits. The lungs are clear and cardiacneck vein distention or carotid bruits. The lungs are clear and cardiacexamination reveals a normal S1 and S2 and a faint midexamination reveals a normal S1 and S2 and a faint mid--systolic click but nosystolic click but nomurmur. Examination of the abdomen and extremities is normal.murmur. Examination of the abdomen and extremities is normal.Electrocardiogram shows a 1Electrocardiogram shows a 1--mV inferior S TmV inferior S T--segment elevation; a subsequentsegment elevation; a subsequent
electrocardiogram is normal. Serum troponin concentration is 1.5 times theelectrocardiogram is normal. Serum troponin concentration is 1.5 times theupper limit of normal. Therapy with heparin, aspirin, metoprolol, andupper limit of normal. Therapy with heparin, aspirin, metoprolol, andnitroglycerin is begun. The next morning, coronary angiography showsnitroglycerin is begun. The next morning, coronary angiography showsnormal angiographic appearance of the arteries and normal left ventricularnormal angiographic appearance of the arteries and normal left ventricular wall motion. The patient is prescribed a daily aspirin and encouraged to stop wall motion. The patient is prescribed a daily aspirin and encouraged to stopusing cocaine.using cocaine.
W hat additional medical therapy should be prescribed at discharge? W hat additional medical therapy should be prescribed at discharge? A Angiotensin A Angiotensin--converting enzyme inhibitorconverting enzyme inhibitor B B --blockerblocker
C CalciumC Calcium--channel blockerchannel blocker D ClopidogrelD Clopidogrel
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 47/72
47M Chadi Alraies
AC TIVI TY AC TIVI TY
EncourageEncourage 3030 toto 6060 minutes of moderateminutes of moderate--
intensity aerobic activity, such as brisk walking intensity aerobic activity, such as brisk walking all days of the week ( all days of the week (55 days is acceptable).days is acceptable).
Supplemented by an increase in daily lifestyleSupplemented by an increase in daily lifestyleactivities (eg, walking breaks at work, gardening,activities (eg, walking breaks at work, gardening,
household work).household work).
Encourage resistance training Encourage resistance training 22 days per week.days per week.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 48/72
48M Chadi Alraies
W EIGH T MANAGEMEN T W EIGH T MANAGEMEN T
Assess body mass index and/or waist Assess body mass index and/or waist
circumference on each visit and consistently.circumference on each visit and consistently.
Encourage weight maintenance/reductionEncourage weight maintenance/reductionthrough an appropriate balance of physicalthrough an appropriate balance of physicalactivity, caloric intake.activity, caloric intake.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 49/72

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 50/72
50M Chadi Alraies
DIABE TES MANAGEMEN TDIABE TES MANAGEMEN T
Goal:Goal: HbAHbA11c <c <77%%
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 51/72
51M Chadi Alraies
AN TIPLA TELE T AGEN TS/ AN TIPLA TELE T AGEN TS/ AN TICOAGULAN TS AN TICOAGULAN TS
Start aspirinStart aspirin 7575 toto 162162 mg/d unlessmg/d unless
contraindicated.contraindicated.
For patients undergoing CABG, aspirin shouldFor patients undergoing CABG, aspirin shouldbe started withinbe started within 4848 hours after surgery.hours after surgery.
Doses higher thanDoses higher than 162162 mg/d can be continuedmg/d can be continued
for up tofor up to 11 year.year.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 52/72
52M Chadi Alraies
AN TIPLA TELE T AGEN TS/ AN TIPLA TELE T AGEN TS/ AN TICOAGULAN TS AN TICOAGULAN TS
Start and continue clopidogrelStart and continue clopidogrel 7575 mg/d inmg/d in
combination with aspirin for up tocombination with aspirin for up to 1212 months inmonths inpatients after:patients after:
ACS, PCI with stent placement ACS, PCI with stent placement
Patients who have undergone percutaneousPatients who have undergone percutaneouscoronary intervention with stent placementcoronary intervention with stent placement
should initially receive highershould initially receive higher--dose aspirin atdose aspirin at 325325mg/d formg/d for 11 month for bare metal.month for bare metal.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 53/72
53M Chadi Alraies
AN TIPLA TELE T AGEN TS/ AN TIPLA TELE T AGEN TS/ AN TICOAGULAN TS AN TICOAGULAN TS
Manage warfarin to international normalizedManage warfarin to international normalized
ratio=ratio=22..00 toto 33..00 for paroxysmal or chronic atrialfor paroxysmal or chronic atrialfibrillation or flutterfibrillation or flutter
Use of warfarin in conjunction with aspirinUse of warfarin in conjunction with aspirinand/or clopidogrel is associated with increasedand/or clopidogrel is associated with increased
risk of bleeding and should be monitoredrisk of bleeding and should be monitored
closely.closely.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 54/72
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 55/72
M Chadi Alraies 55
RENINRENIN--ANGIO TENSIN ANGIO TENSIN-- ALDOS TERONE S Y S TEM ALDOS TERONE S Y S TEM
BLOCKERSBLOCKERS

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 56/72
56M Chadi Alraies
ACE inhibitors ACE inhibitors
Start and continue indefinitely in all patientsStart and continue indefinitely in all patients
with« with«
LV EFLV EF 4040%.%.
H TN,H TN,
DMDM
Chronic kidney disease.Chronic kidney disease.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 57/72
57M Chadi Alraies
Angiotensin receptor blockers Angiotensin receptor blockers
Intolerance of ACE inhibitorsIntolerance of ACE inhibitors
Heart failureHeart failure
Myocardial infarction with left ventricularMyocardial infarction with left ventricularejection fractionejection fraction 4040%.%.
Consider use in combination with ACEConsider use in combination with ACE
inhibitors in systolicinhibitors in systolic--dysfunction heart failure.dysfunction heart failure.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 58/72
58M Chadi Alraies
A A 5555--yearyear--old man with coronary artery disease is evaluatedold man with coronary artery disease is evaluated 22 weeks after having had a myocardial infarction. On discharge, weeks after having had a myocardial infarction. On discharge,his medications included aspirin, sustainedhis medications included aspirin, sustained--release metoprolol,release metoprolol,
isosorbide mononitrate, lisinopril, and atorvastatin.isosorbide mononitrate, lisinopril, and atorvastatin.Echocardiogram at that time showed inferior and posterior wallEchocardiogram at that time showed inferior and posterior wallakinesis and a left ventricular ejection fraction of akinesis and a left ventricular ejection fraction of 4040%. On%. Onexamination, his heart rate isexamination, his heart rate is 6060/min and his blood pressure is/min and his blood pressure is130130//7070 mm Hg. Jugular venous pressure is normal and themm Hg. Jugular venous pressure is normal and thechest is clear. Cardiac rhythm is regular, with normal Schest is clear. Cardiac rhythm is regular, with normal S11 and Sand S22
and no murmurs or extra heart sounds. Laboratory results fromand no murmurs or extra heart sounds. Laboratory results fromyesterday are potassiumyesterday are potassium 55..77 meq/L ( meq/L (55..77 mmol/L), creatininemmol/L), creatinine 11..00mg/dL ( mg/dL (8888..4242 mol/L), and LDL cholesterolmol/L), and LDL cholesterol 6565 mg/dL ( mg/dL (11..6868mmol/L). Lisinopril therapy is stopped.mmol/L). Lisinopril therapy is stopped.
W ich of the following medications should be started in this W ich of the following medications should be started in thispatient?patient?
1.1. Valsartan Valsartan
2.2. SpironolactoneSpironolactone
3.3. Amlodipine Amlodipine
4.4. EplerenoneEplerenone
5.5. HydralazineHydralazine
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 59/72
59M Chadi Alraies
Aldosterone blockade Aldosterone blockade
Use in postUse in post² ²myocardial infarction patients,myocardial infarction patients,
without« without«
Significant renal dysfunction orSignificant renal dysfunction or
HyperkalemiaHyperkalemia
Already receiving therapeutic doses of an ACEI and Already receiving therapeutic doses of an ACEI andBB.BB.
Left ventricular ejection fractionLeft ventricular ejection fraction 4040%% Diabetes or heart failure.Diabetes or heart failure.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 60/72
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 61/72
61M Chadi Alraies
INFLUENZA VACCINA TIONINFLUENZA VACCINA TION
Patients with cardiovascular disease should havePatients with cardiovascular disease should have
an influenza vaccination.an influenza vaccination.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 62/72
62M Chadi Alraies
A ntioxidant A ntioxidant
( (HOPE) trial found that vitamin E may even beHOPE) trial found that vitamin E may even be
harmful by increasing the likelihood of heartharmful by increasing the likelihood of heartfailure and other trials have suggested thatfailure and other trials have suggested that
vitamin E may hinder the effectiveness of statin vitamin E may hinder the effectiveness of statintherapy.therapy.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 63/72
63M Chadi Alraies
Elevated plasma homocysteine levelsElevated plasma homocysteine levels
Associated with an increased risk of vascular Associated with an increased risk of vascular
events.events.
Reduced with dietary supplements of Reduced with dietary supplements of folic acidfolic acid
( (11 mg/d)mg/d) in combination within combination with vitamin B vitamin B66 andand vitamin B vitamin B1212..
RC T showed they are of little or no value inRC T showed they are of little or no value in
preventing vascular events.preventing vascular events.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 64/72
64M Chadi Alraies
Hormone replacement therapy HR THormone replacement therapy HR T
In HERS trial, neither combined estrogenIn HERS trial, neither combined estrogen² ²
progesterone nor estrogen alone therapy isprogesterone nor estrogen alone therapy isprotective (in fact both cause harm).protective (in fact both cause harm).

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 65/72
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 66/72
66M Chadi Alraies
A A 3535--yearyear--old man is evaluated during a routine examination. Heold man is evaluated during a routine examination. Hedoes not smoke and has no family history of early coronary does not smoke and has no family history of early coronary artery disease.artery disease.
On examination, BMI isOn examination, BMI is 3535..22, and waist circumference is, and waist circumference is 114114 cmcm( (4545 in). Blood pressure isin). Blood pressure is 142142//8888 mm Hg. The remainder of themm Hg. The remainder of thephysical examination is normal. Laboratory studies indicatephysical examination is normal. Laboratory studies indicateborderline hyperglycemia (fasting plasma glucose,borderline hyperglycemia (fasting plasma glucose, 121121 mg/dLmg/dL[ [66..77 mmol/L]). Serum total cholesterol level ismmol/L]). Serum total cholesterol level is 246246 mg/dL ( mg/dL (66..3636
mmol/L), highmmol/L), high--density lipoprotein level isdensity lipoprotein level is 3131 mg/dL ( mg/dL (00..88mmol/L), and low mmol/L), and low--density lipoprotein level isdensity lipoprotein level is 158158 mg/dL ( mg/dL (44..0505mmol/L).mmol/L).
W hich of the following recommendations is most appropriate W hich of the following recommendations is most appropriatefor this patient?for this patient?
A Electron A Electron--beam C T beam C T B Exercise treadmill testB Exercise treadmill test
C HydrochlorothiazideC Hydrochlorothiazide
D Intensive lifestyle modificationD Intensive lifestyle modification
E Intake of red wineE Intake of red wine

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 67/72
67M Chadi Alraies
Pathophysiology of Chronic Ischemia &Pathophysiology of Chronic Ischemia & Acute Coronary Syndromes Acute Coronary Syndromes
Chronic ischemia, including stable angina, isChronic ischemia, including stable angina, isclassically caused by supply and demandclassically caused by supply and demand
mismatch.mismatch.
Precipitants include exercise, eating, coldPrecipitants include exercise, eating, cold
weather, and emotional stress. weather, and emotional stress.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 68/72
68M Chadi Alraies
Pathophysiology of Chronic Ischemia &Pathophysiology of Chronic Ischemia & Acute Coronary Syndromes Acute Coronary Syndromes
ACS of ACS of unstable anginaunstable angina andand MI cMI caused by:aused by:
Plaque disruptionPlaque disruption
Platelet and thrombinPlatelet and thrombin--mediated coronary mediated coronary thrombosisthrombosis
Coronary spasmCoronary spasm
Microvascular dysfunction.Microvascular dysfunction.
These episodes occur in the early morning or These episodes occur in the early morning orshortly after arising.shortly after arising.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 69/72
69M Chadi Alraies
Pathophysiology of Chronic Ischemia &Pathophysiology of Chronic Ischemia & Acute Coronary Syndromes Acute Coronary Syndromes
Antithrombotic therapy is directed toward Antithrombotic therapy is directed toward
inhibition of platelet activity (aspirin,inhibition of platelet activity (aspirin,
clopidogrel, IIb/IIIa receptor antagonists),clopidogrel, IIb/IIIa receptor antagonists),inhibition of coagulation (unfractionated or low inhibition of coagulation (unfractionated or low--
molecularmolecular--weight heparin), and fibrinolysis for weight heparin), and fibrinolysis forS TS T--segment elevation myocardial infarction.segment elevation myocardial infarction.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 70/72
70M Chadi Alraies
T ypes & Pathoph ysiology of T ypes & Pathoph ysiology of
myocardialmyocardial ischemiaischemia presentation presentation
Symptomatic, causing Symptomatic, causing angina pectoris.angina pectoris.
Completely silent.Completely silent. In patients with diagnosed CAD silent ischemicIn patients with diagnosed CAD silent ischemic
episodes have the same prognostic import asepisodes have the same prognostic import as
symptomatic ones.symptomatic ones.
8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 71/72
71M Chadi Alraies
Myocardial Hibernation & Stunning Myocardial Hibernation & Stunning
Areas of myocardium that are persistently Areas of myocardium that are persistently underperfused.underperfused.
Still viableStill viable
May develop sustained contractile dysfunction.May develop sustained contractile dysfunction.
May lead to LV failure.May lead to LV failure.
Reversible following coronary revascularization.Reversible following coronary revascularization.
Identified by Identified by Radionuclide testing,Radionuclide testing, (PE T ), MRI,(PE T ), MRI,
Inotropic stimulation with dobutamine.Inotropic stimulation with dobutamine.

8/8/2019 926277 Coronary Heart Disease
http://slidepdf.com/reader/full/926277-coronary-heart-disease 72/72
Myocardial Hibernation & Stunning Myocardial Hibernation & Stunning
A related phenomenon, termed "myocardial A related phenomenon, termed "myocardial
stunning," is the occurrence of persistentstunning," is the occurrence of persistentcontractile dysfunction following prolonged orcontractile dysfunction following prolonged or
repetitive episodes of myocardial ischemia.repetitive episodes of myocardial ischemia.