
Con Iber Fairview Health Systems University of Minnesota Health The Future of Sleep Health.
26
Con Iber Fairview Health Systems University of Minnesota Health The Future of Sleep Health
-
Upload
kayli-welbourn -
Category
Documents
-
view
215 -
download
0
Transcript of Con Iber Fairview Health Systems University of Minnesota Health The Future of Sleep Health.

Con IberFairview Health Systems
University of Minnesota Health
The Future of Sleep Health
Objectives• To identify opportunities in transitioning from
sleep medicine to sleep health• To propose a snapshot of the future of the
field• To identify methods of transforming ourselves
into what the future requires of us
Caveat
There will be unanswered questions that we must all solve together
Harry: “OK……where’s the map?”

Harry, don’t check the map while your driving!!
Where should we go and how should we get there?
Let’s get a higher altitude view
• Health care cost/quality gaps • History of perverse incentives• Technical innovation• Public accountability
Pressures for Change

OECD Health data 2012
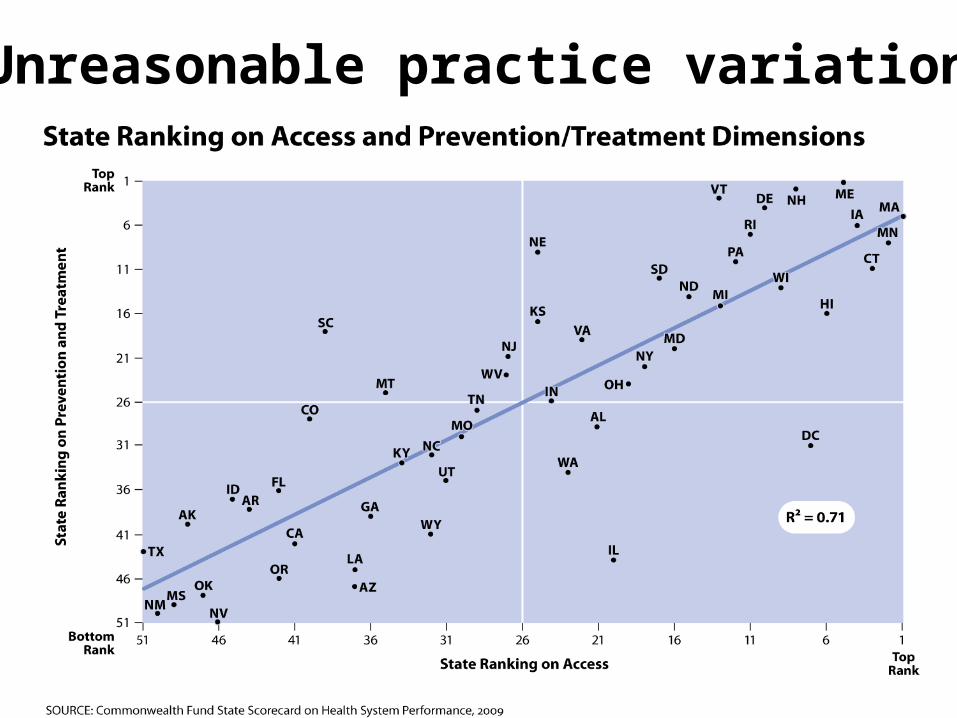
Unreasonable practice variation
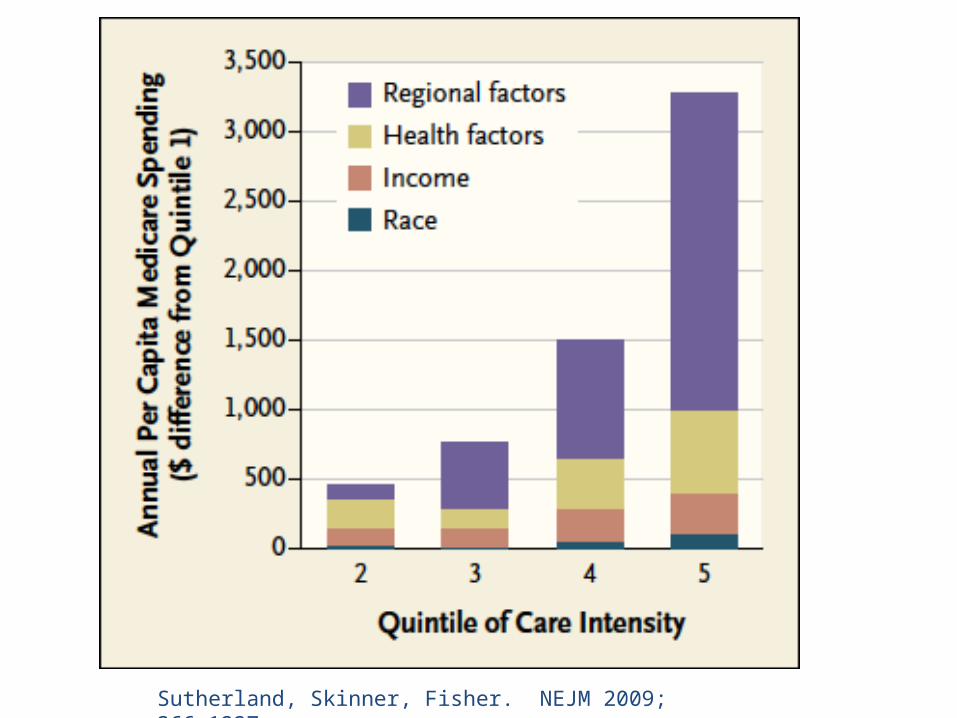
Sutherland, Skinner, Fisher. NEJM 2009; 366:1227
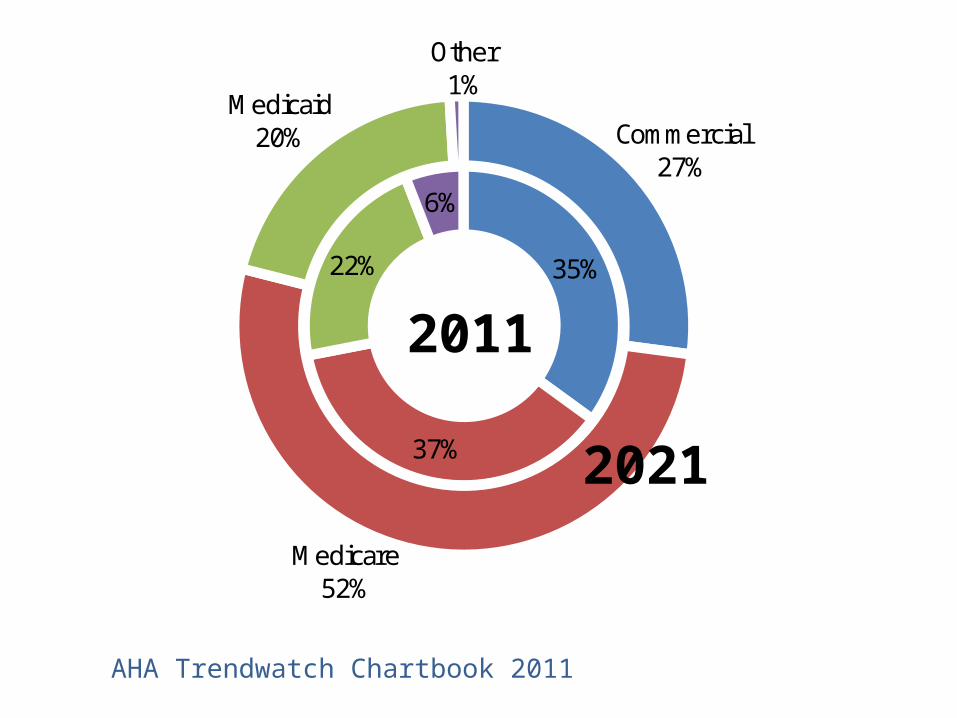
35%
37%
22%
6%
Commercial27%
Medicare52%
Medicaid20%
Other1%
AHA Trendwatch Chartbook 2011
2011
2021
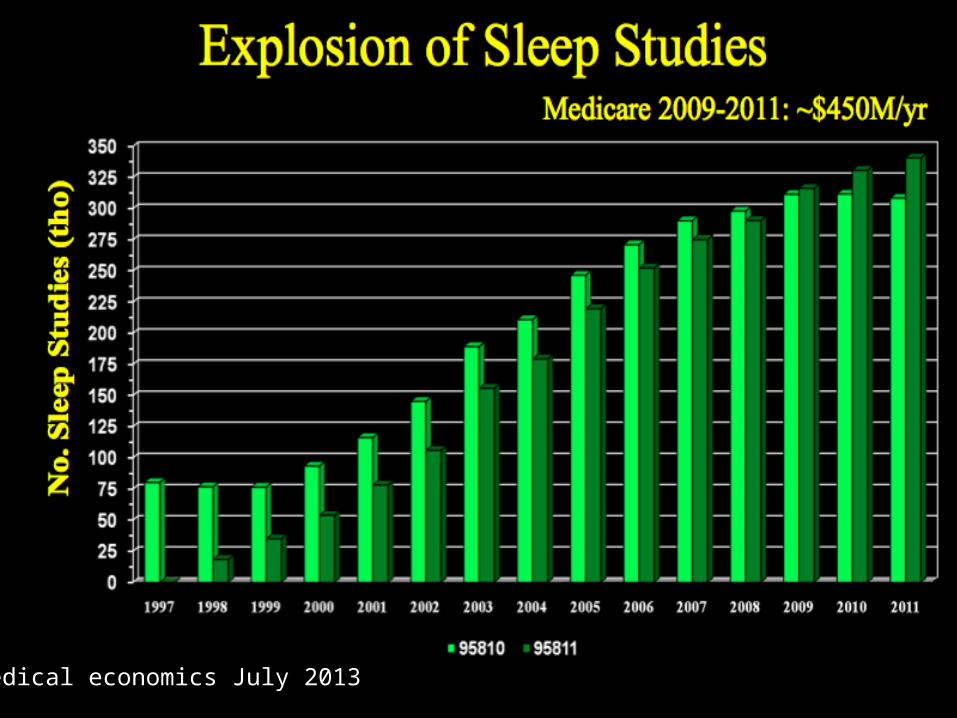
Medical economics July 2013
What are the opportunities for merging sleepmedicine into sleep health?
More adaptable to changing models• diagnosis at home• decreased reliance on complex testing• increased utilization of evolving therapies
More honest-• shift work/insufficient sleep• preventative methods are more powerful• better alignment with driving forces
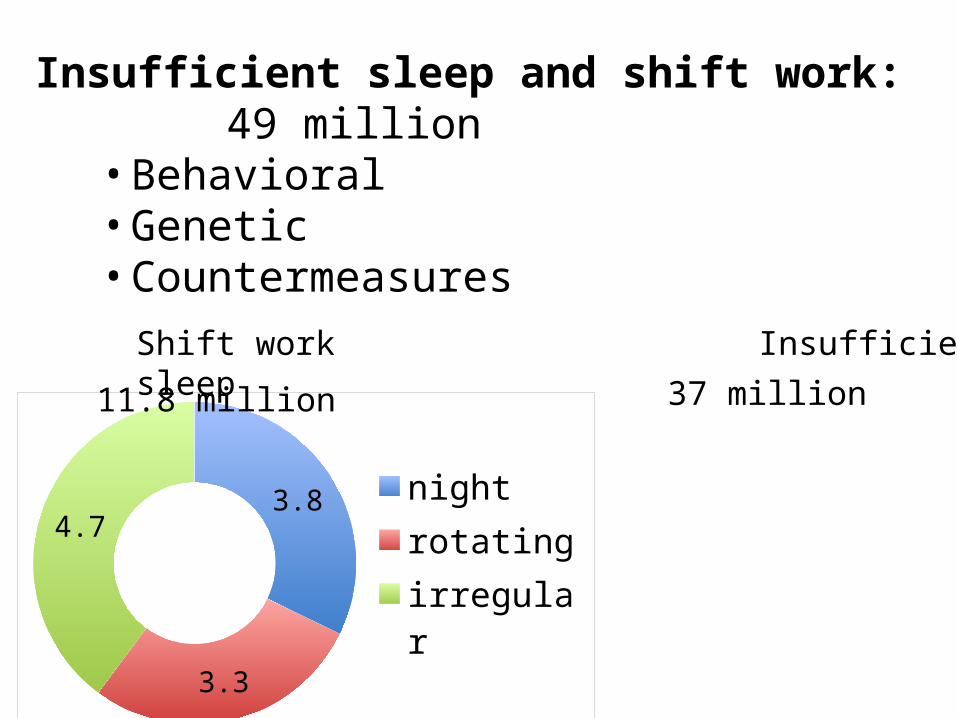
3.8
3.3
4.7 nightrotatingirregular
11.8 million
Insufficient sleep and shift work:49 million
• Behavioral• Genetic• Countermeasures
Shift workInsufficient sleep 37 million
What are the opportunities for transitioning from sleep
medicine into sleep health?
More diversified-• meets need for distributive model• population/employee based• flexibility of cross-training workforce
More integrated –• case finding->diagnosis->therapy• population management
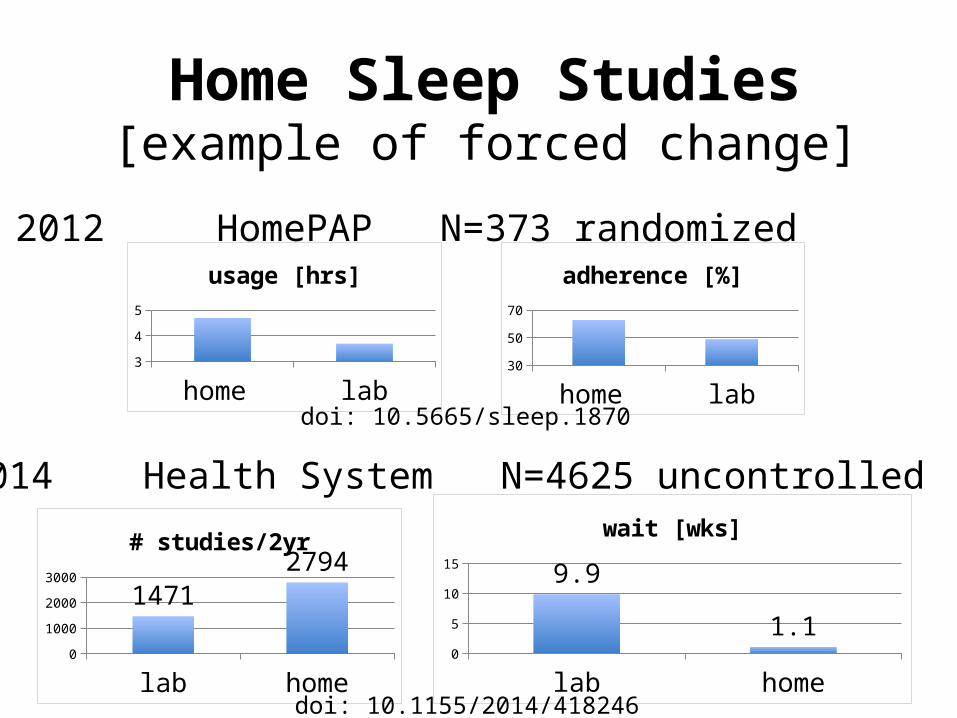
Home Sleep Studies[example of forced change]
2012 HomePAP N=373 randomized
home lab3
3.54
4.55
usage [hrs]
home lab3040506070
adherence [%]
lab home0
50010001500200025003000
1471
2794# studies/2yr
lab home02468
1012 9.9
1.1
wait [wks]
2014 Health System N=4625 uncontrolled
doi: 10.1155/2014/418246
doi: 10.5665/sleep.1870
Dental devices[example of change to be forced]
Gap-underutilization of devices in the US
Drivers-• user preference• guideline changes• payer preference
Snapshot of the future
Where do we want to go?
• Change that will improve sleep health• Quality and cost optimization
• Adaptable to predictable forces• User satisfaction
• Distribute care and maintain continuity• Incorporate population management• Develop and integrate collaborative networks• Negotiate change consensus• Leverage technology
Strategies-high altitude

• Reduce variation • Virtual care• Sleep therapy management• Cross discipline collaboration• Payer negotiation• Stratified resource use• Cross-training workforce
Tactics-zoom lens[adopt new lexicon]
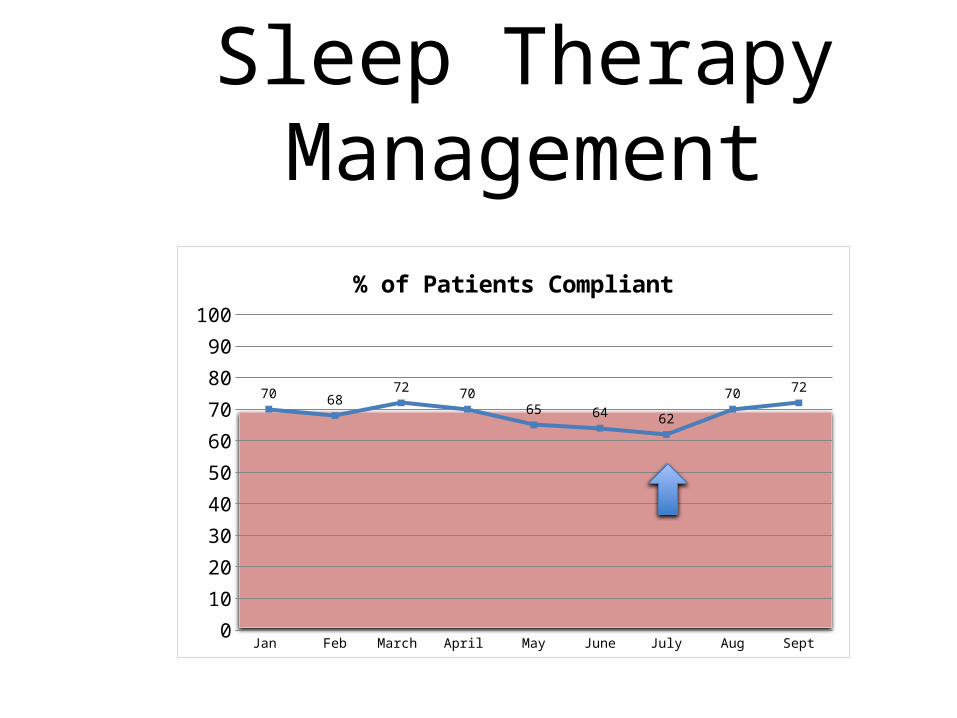
Jan Feb March April May June July Aug Sept0
10
20
30
40
50
60
70
80
90
100
70 6872 70
65 64 62
70 72
% of Patients Compliant
Sleep Therapy Management
Structural changes: reduce points of care and variation, expand comprehensive care, develop stem to stern pathways, partner, tune to outcomes
Behavioral changes: team concept, monitor progress to achievable/meaningful goals, anticipate and manage failure, expand scope of practices
Components of Change
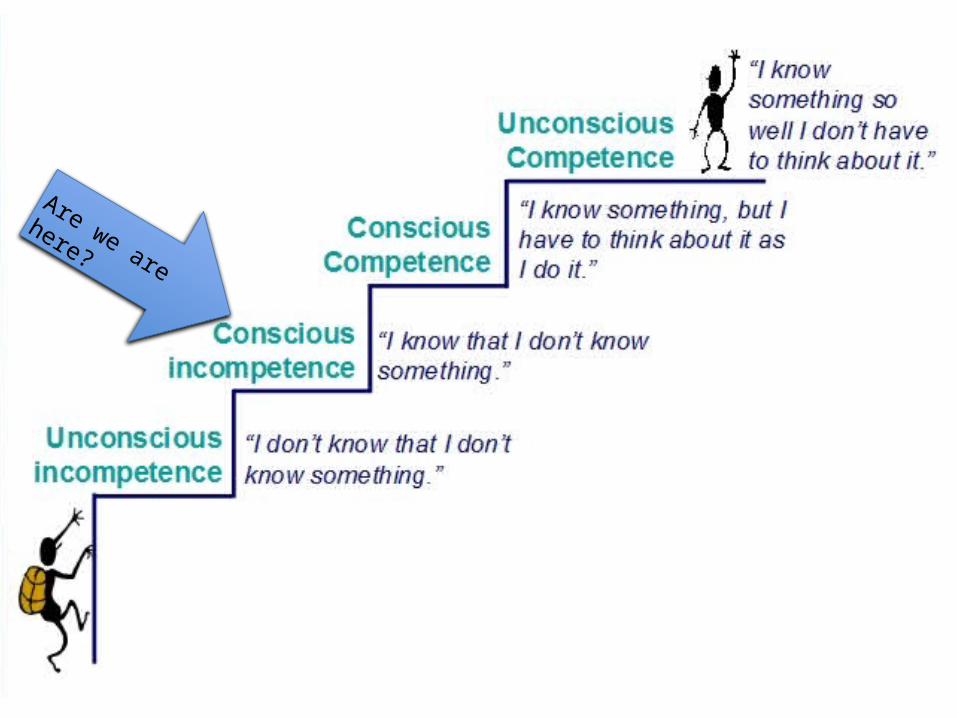
Are we are here?
• “Single visit”: initial diagnostic procedure for uncomplicated sleep apnea and insomnia moved to primary care with therapy determination made by sleep center and virtualization of >50% of point of care followup visits.
• Consolidation of laboratory studies to verify ambiguous home studies, serious comorbidities, parasomnias, suspected seizures.

• Increased scope of onsite clinic operations to include partners in dental, otolaryngology, pediatric, and occupational sleep medicine.
• Population management to incorporate long term management, innovation, outcome monitoring, payer negotiation.


















