Combined Cellulitis -Final
78
Group 2: Alison Hemy, Avril Hamilton, Gina Hummel, WaiSum Szeto, Saurabh Patel Date: June 17, 2011 Case 2 Cellulitis
Transcript of Combined Cellulitis -Final
Group 2: Alison Hemy, Avril Hamilton, Gina Hummel, WaiSum Szeto, Saurabh Patel
Date: June 17, 2011
Case 2 Cellulitis
Outline
Meet Christof Kottingheimer (CK)
What is cellulitis? Epidemiology Pathophysiology Risk Factors Microbiology Signs & Symptoms Complications Diagnosis
Drug therapy problems and therapeutic alternatives Mild to moderate (uncomplicated) cellulitis Methicillin resistant Staphylococcus aureus (MRSA) treatments Severe (progressive/complicated) cellulitis Care plan/ monitoring/patient education Summary

Meet Christoph Kottingheimer
• 75 years old• Visited emergency 5 days ago
– diagnosed with LEFT UPPER EXTREMITY (LUE) CELLULITIS
• Prescription for cephalexin 500mg po TID for 7 days, but lost it
• Today:– Increased swelling and pain in left forearm– Decreased range of motion and tenderness in right shoulder– New onset pain in right shoulder– Fever
invisibleparachute.com

Past Medical History
• Left-arm cellulitis, diagnosed 5 days ago
• Type 2 diabetes mellitus
– Recently diagnosed
• Atrial fibrillation
alanderickson.com
Surgical History
• 1980 - motor vehicle accident and acquired large bump on forehead
• 1982 – facial electrical burn requiring skin graft
• 2002- benign cyst removed from neck
Social History
Smokes 2 ppd x 20 years
Occasional alcohol
Denies illicit drug useanguishedrepose.wordpress.com

Medications
* No known drug allergies
Indication Medication Result to date
Cellulitis Cephalexin
500mg po TID
Patient did not take
T2DM Metformin
500mg po BID
Patient reports only taken “a
couple of doses”
Atrial Fibrillation Metoprolol
50mg BID
Heart rate controlled
leanpowerfulfitness.com

What is Cellulitis?• Type of skin and soft-tissue infection
– Acute
– Affects epidermis, dermis and subcutaneous layers
• Serious infection because possible spread through: – Lymphatic tissue
– Blood stream
• Commonly gram positive bacteria
Cellulitis. PubMed Health. National Library of Medicine. 2009. Accessed June 15, 2011.
en.wikipedia.org
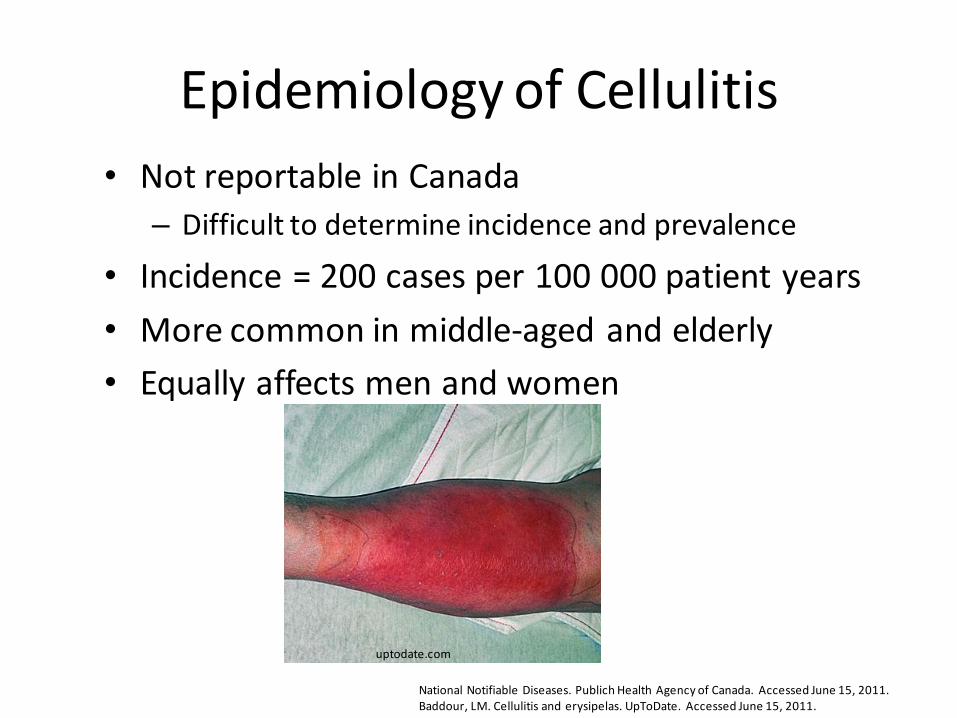
Epidemiology of Cellulitis
• Not reportable in Canada
– Difficult to determine incidence and prevalence
• Incidence = 200 cases per 100 000 patient years
• More common in middle-aged and elderly
• Equally affects men and women
National Notifiable Diseases. Publich Health Agency of Canada. Accessed June 15, 2011. Baddour, LM. Cellulitis and erysipelas. UpToDate. Accessed June 15, 2011.
uptodate.com
Pathophysiology of Cellulitis
• Break to skin
– Burn, trauma, ulcers, injections
• Organisms from skin can enter dermis and multiply
• Note:
– Although visible break in skin is common, can occur with microscopic breaks from dry and irritated skin
Cellulitis. PubMed Health. National Library of Medicine. 2009. Accessed June 15, 2011.
Baddour, LM. Cellulitis and erysipelas. UpToDate. Accessed June 15, 2011.
Risk Factors
• Co-morbidities
– Diabetes (*** our patient ***)
– Immunodeficiency
– Cancer
– Peripheral artery disease
• IV or SC drug use
Baddour, LM. Cellulitis and erysipelas. UpToDate. Accessed June 15, 2011.
invisibleparachute.com
Microbiology
• 80% of cases are gram positive: – β-hemolytic streptococci (ex. Streptococcus pyogenes)
– Staphlococcus aureus.
• Less common:– Streptococcus pneumoniae
– Haemophilus influenzae
– Gram-negative bacilli (pseudomonas, proteus, enterobacter)
– Anaerobes
• Mixed aerobic-anaerbic flora also occurs in diabetes
Baddour, LM. Cellulitis and erysipelas. UpToDate. Accessed June 15, 2011.Pendland SL, Fish DN, Danziger LH. Skin and soft tissue infections: In: DiPiro JT, Talbert RL, Yee GC, et al., eds. Pharmacotherapy: A Pathophysiologic Approach, 6th ed. New York, McGraw-Hill, 2005:1977–1995
biomarker.korea.ac.kr equidblog.com
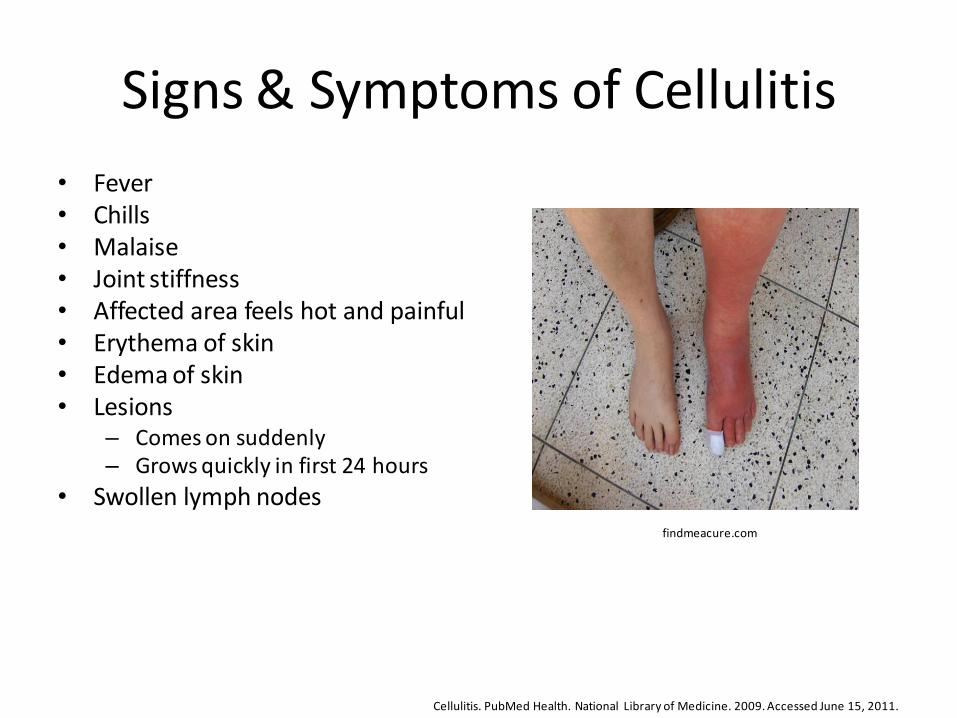
Signs & Symptoms of Cellulitis
• Fever• Chills• Malaise• Joint stiffness• Affected area feels hot and painful• Erythema of skin• Edema of skin• Lesions
– Comes on suddenly– Grows quickly in first 24 hours
• Swollen lymph nodes
Cellulitis. PubMed Health. National Library of Medicine. 2009. Accessed June 15, 2011.
findmeacure.com
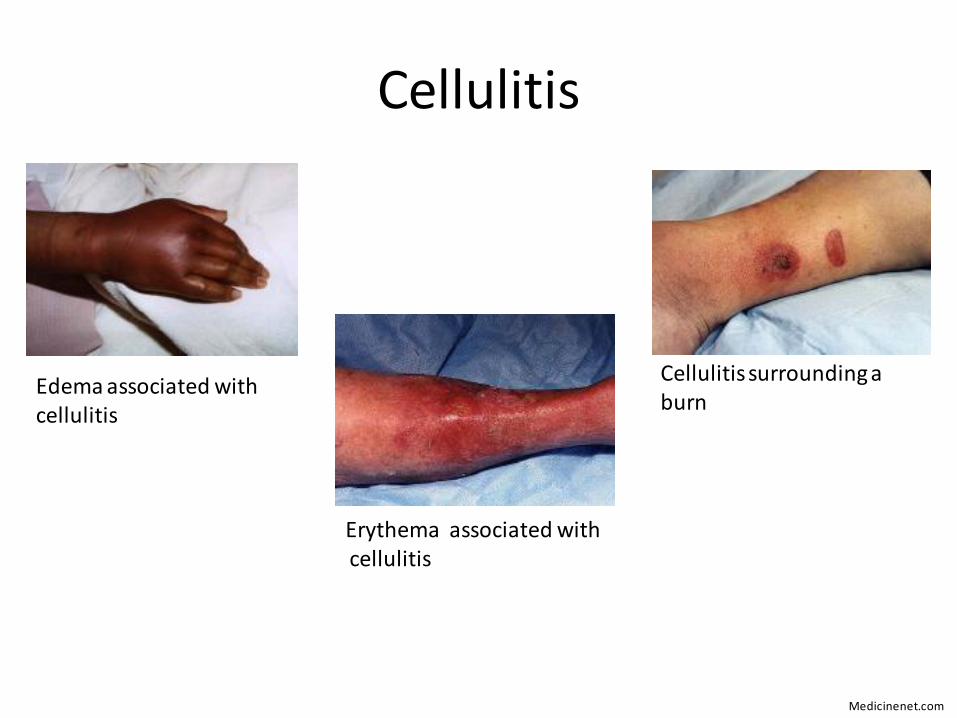
Cellulitis
Cellulitis surrounding a burn
Edema associated with cellulitis
Erythema associated withcellulitis
Medicinenet.com

Cellulitis Complications
• Osteomyelitis (bone infection)
• Lymphangitis (inflammation of lymph vessels)
• Meningitis
• Sepsis, shock
• Gangrene (tissue death)
Cellulitis. PubMed Health. National Library of Medicine. 2009. Accessed June 15, 2011.
wikinfo.org

Diagnosis of Cellulitis
• Must be distinguished from other infections – Herpes zoster
– Necrotizing fasciitis
– Erysipelas
– Impetigo
• Diagnosis often based on clinical manifestations
• Blood cultures, needle aspirations or biopsies not useful for mild infection– Positive 5-40% of the time
– Should be performed with serious disease (systemic toxicity, extensive skin involvement, comorbidities (lymphedema, malignancy, neutropenia, diabetes))
Back to CK• Vitals:
– BP 129/74
– HR 96
– RR 16
– T 38.3°C
– BMI 35
• CV:
– Irregularly irregular heart beat
• CrCl= 77 mL/mins
joetri-tthardt.blogspot.com
invisibleparachute.com

Back to CK
Kratz A, Ferraro M, Sluss, P, Lewandrowski KB. Laboratory Reference Values. N Engl J Med. 2004. 1548 -1564. .
Measurement Value Normal
WBC 26.3 x 10^3/mm3 3.2-9.8 x 10^3/mm3
Neutrophils 81% 40-70%
Bands 10% 0-10%
Lymphocytes 7% 22-44%
Monocytes 2% 4-11%
Blood Glucose 14 mmol/L 4-7 mmol/L (FBG)
5-10 mmol/L (PPG)
Na 134 mEg/L 136-145 mmol/L
K 3.6 mEq/L 3.5-5 mmol/L
CL 87 mEq/L 98-106 mmol/L
CO2 21 mEq/L 21-30 mEq/L
Urea 23 mg/dL 10-20 mg/dL
SCr 118 μmol/L <133 μmol/L
Hgb 155 g/L 138-182 g/L
Hct 44% 41-53%
Platelets 329 x 10^3/mm3 150-350 x 10^3/mm3
Brief Summary of Patient CK
• 75 year old male
• Presented to the emergency department 5 days ago– Diagnosed with left upper extremity cellulitis
– Given a prescription for cephalexin 500mg po TID for 7 days
• Medical Conditions – Type 2 diabetes mellitus
– Atrial Fibrillation
Brief Summary of Patient CK
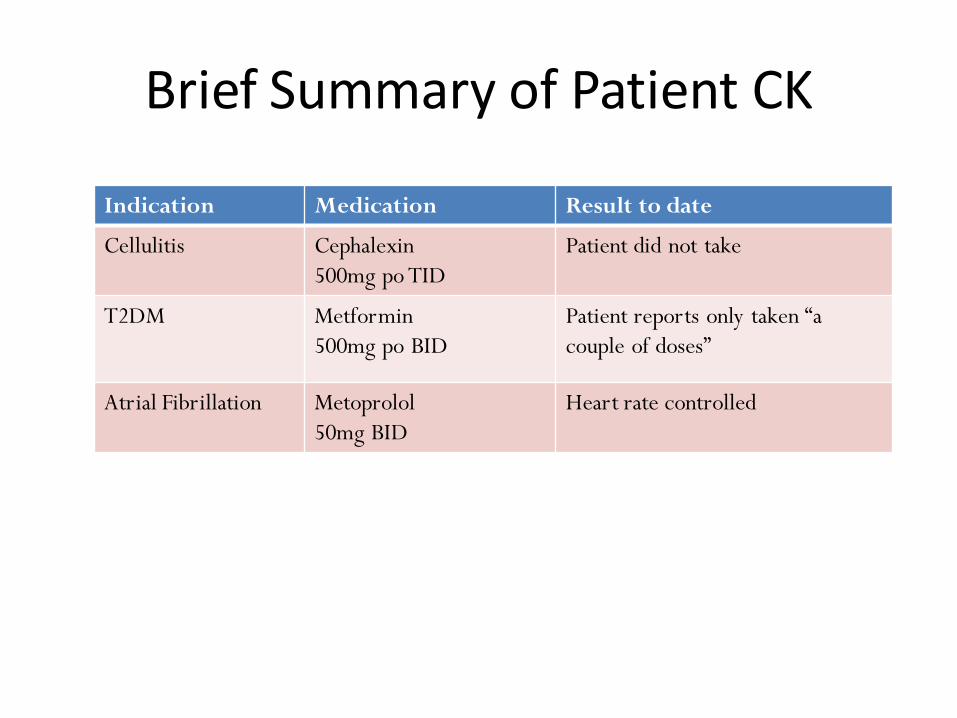
Indication Medication Result to date
Cellulitis Cephalexin
500mg po TID
Patient did not take
T2DM Metformin
500mg po BID
Patient reports only taken “a
couple of doses”
Atrial Fibrillation Metoprolol
50mg BID
Heart rate controlled

CK’s Drug Related Problems (DRPs)
• Mr. CK has progressive left arm cellulitis and requires a drug therapy.
• Mr. CKs T2DM is uncontrolled secondary to nonadherence, and requires education about the consequences of diabetes.
• Mr. CK is at risk of stroke due to atrial fibrillation and requires anticoagulant therapy.

• Mr. CK’s metoprolol may not be efficacious as his heart rate is 96bpm and irregularly irregular.
• Mr. CK smokes two packs of cigarettes per day and would benefit from smoking cessation education.
• Mr. CK is at risk of a cardiovascular event, and may require and ACEI and statin (lipid panel unknown).
• Mr. CK’s is at an increased risk of cardiovascular events due to BMI of 35, and requires lifestyle education.
Additional DRPs

Subjective and Objective Data Consistent with Cellulitis
Subjective: pain in left forearm, left upper extremity tenderness/pain in right shoulder, especially when gripping or
flexing
Objective: swelling (pitting edema), warm, red left forearm decreased range of motion in right shoulder fever tachycardia increased WBCs High neutrophils count, high bands, low lymphs, low monos negative for left upper extremity (LUE) DVT

Most Common Causative Organisms of Cellulitis
• Most often: S. pyogenes or S. aureus.
• Less common organisms include Strep. Pneumoniae, Haemophilus influenzae, Gram-negative bacilli and anaerobes
• Mixed aerobic-anaerbic flora also occurs in diabetes1.
1. Pendland SL, Fish DN, Danziger LH. Skin and soft tissue infections: In: DiPiro JT, Talbert RL, Yee GC, et al.,
eds. Pharmacotherapy: A Pathophysiologic Approach, 6th ed. New York, McGraw-Hill, 2005:1977–1995
CREST. Guidelines on the Management of Cellulitis in Adults. 2005

Goals of Therapy
• Cellulitis
– rapid eradication of infection
– relief of pain and tenderness in left forearm, left upper extremity, right shoulder, and return of range of motion
– resolution of fever
– prevention of further complications
– prevent recurrence

Goals of Therapy
• T2DM
– FBS 4-7mmol/L, PPBS 7-10mmol/L, HbA1c ~ 8 %
– Prevent complications
• microvascular: neuropathy, retinopathy, nephropathy, foot ulcers/wounds,
• macrovascular: CV disease
– Improve lifestyle factors (smoking, BMI)

Goals of Therapy
• Atrial Fibrillation
– control atrial fibrillation
• < 100 bpm
– decrease risk of tachycardia induced cardiomyopathy
– prevent stroke
Non-drug Therapies
• Local care of cellulitis: elevation and immobilization of the area involved to decrease swelling.
– Drainage of edema and inflammatory substances
• Ensure proper wound care and dressing changes
– Skin should be hydrated
• Avoid dryness, cracking but also maceration
• Management of underlying conditions
– Blood glucose control is important
Lowy FD, Sexton DJ, Baron EL. Up-to-date: Cellulitis and erysipelas. UpToDate INC, 2010. (Accessed June 12, 2011 at: www.uptodate.com)

Antimicrobial Options for the Treatment of Cellulitis
Staphylococci or unknown Gram positive: Mild:
Cloxacillin (250-500mg PO Q6h)
Moderate - Severe administration of semisyntheitic penicillin (nafcillin or oxacillin 1-2g IV q 4-6hrs)
administration of 1st gen cephalosporin (cefazolin)
clindamycin
both have activity against strep and staph
usual duration of therapy 5-10d
Streptococci: mild:
oral penicillin VK 0.5g q 6 hrs OR
IM procaine penicillin G 600 000U q 8-12hrs
severe: Penicillin G 1 – 2 million U IV q 4-6hrs OR
IV ceftriaxone 50-100mg/kg as single dose
if allergic to penicillin: oral or parenteral clindamycin OR
1st gen cephalosporin w/ caution (cefazolin 1-2g IV q 6-8hrs)
Pendland SL, Fish DN, Danziger LH. Skin and soft tissue infections: In: DiPiro JT, Talbert RL, Yee GC, et al., eds. Pharmacot herapy: A Pathophysiologic
Approach, 6th ed. New York, McGraw-Hill, 2005:1977–1995
Kish TD, Chang MH, Fung HB. Treatment of skin and soft tissue infections in the Elderly: A review. Am J Geriatr Pharmacother. 2010 Dec;8(6):485-513.
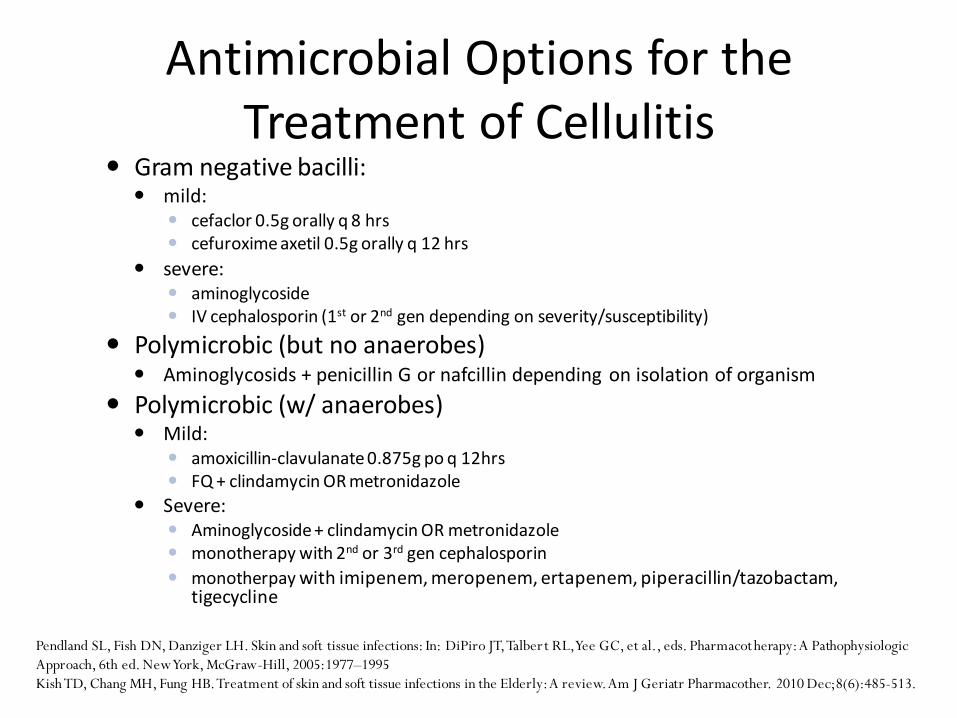
Antimicrobial Options for the Treatment of Cellulitis
Gram negative bacilli: mild:
cefaclor 0.5g orally q 8 hrs cefuroxime axetil 0.5g orally q 12 hrs
severe: aminoglycoside IV cephalosporin (1st or 2nd gen depending on severity/susceptibility)
Polymicrobic (but no anaerobes) Aminoglycosids + penicillin G or nafcillin depending on isolation of organism
Polymicrobic (w/ anaerobes) Mild:
amoxicillin-clavulanate 0.875g po q 12hrs FQ + clindamycin OR metronidazole
Severe: Aminoglycoside + clindamycin OR metronidazole monotherapy with 2nd or 3rd gen cephalosporin
monotherpay with imipenem, meropenem, ertapenem, piperacillin/tazobactam, tigecycline
Pendland SL, Fish DN, Danziger LH. Skin and soft tissue infections: In: DiPiro JT, Talbert RL, Yee GC, et al., eds. Pharmacot herapy: A Pathophysiologic
Approach, 6th ed. New York, McGraw-Hill, 2005:1977–1995
Kish TD, Chang MH, Fung HB. Treatment of skin and soft tissue infections in the Elderly: A review. Am J Geriatr Pharmacother. 2010 Dec;8(6):485-513.

Antibiotics vs. MicrobesMicrobes Recommended Alternatives
S. aureus (MSSA) Cephalexin, CloxacillinParentral cephalosporins,Vancomycin, Clindamycin
Streptococci sp.
β-hemolytic streptococci (Group A, & B common) & S. pyogenes
Penicillin G or V (some add Gentamycin for serious Group B infection & some add clindamycin for serious invasive Group A)
All β lactams, erythromycin, clarithromycin, azithromycin(however, macrolideresistance increasing)
CA-MRSA
Mild to moderateTMP-SMX or Doxycycline or Minocycline
Clindamycin, third or fourth generation Fluoroquinilones
Severe Vancomycin Linezolid or daptomycin
HA-MRSA VancomycinTMP-SMX (some strains resistant), linezolid, daptomycin
Empiric antibiotic therapy for management of cellulitis should include activity against beta-hemolytic streptococci and S. aureus.
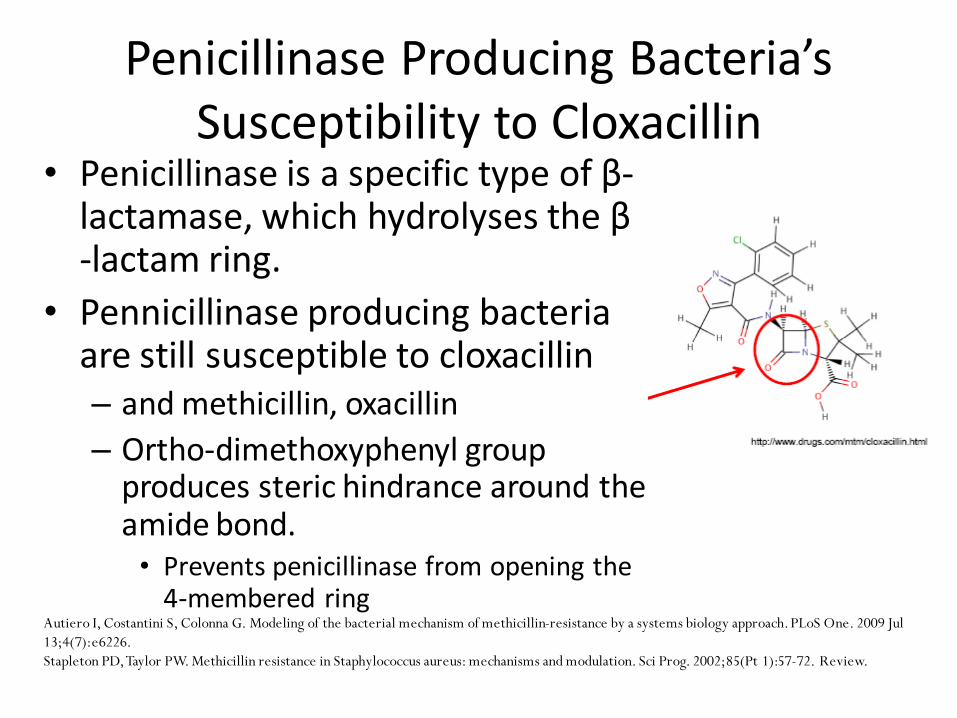
Penicillinase Producing Bacteria’s Susceptibility to Cloxacillin
• Penicillinase is a specific type of β-lactamase, which hydrolyses the β -lactam ring.
• Pennicillinase producing bacteria are still susceptible to cloxacillin– and methicillin, oxacillin
– Ortho-dimethoxyphenyl group produces steric hindrance around the amide bond. • Prevents penicillinase from opening the
4-membered ringAutiero I, Costantini S, Colonna G. Modeling of the bacterial mechanism of methicillin-resistance by a systems biology approach.PLoS One. 2009 Jul
13;4(7):e6226.
Stapleton PD, Taylor PW. Methicillin resistance in Staphylococcus aureus: mechanisms and modulation. Sci Prog. 2002;85(Pt 1):57-72. Review.
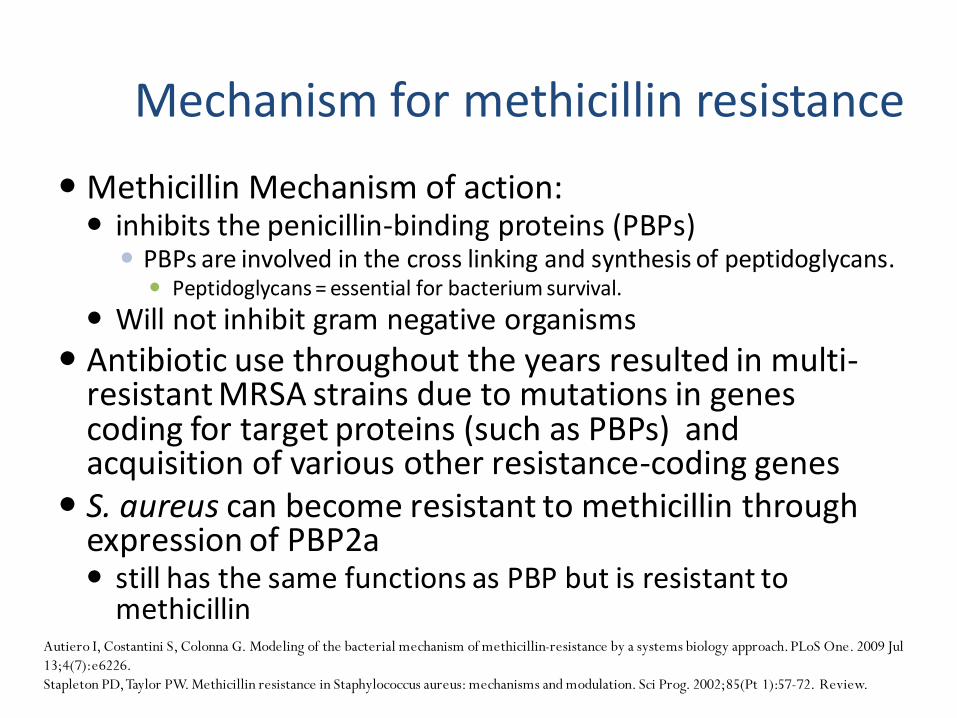
Methicillin Mechanism of action: inhibits the penicillin-binding proteins (PBPs) PBPs are involved in the cross linking and synthesis of peptidoglycans. Peptidoglycans = essential for bacterium survival.
Will not inhibit gram negative organisms
Antibiotic use throughout the years resulted in multi-resistant MRSA strains due to mutations in genes coding for target proteins (such as PBPs) and acquisition of various other resistance-coding genes
S. aureus can become resistant to methicillin through expression of PBP2a still has the same functions as PBP but is resistant to
methicillinAutiero I, Costantini S, Colonna G. Modeling of the bacterial mechanism of methicillin-resistance by a systems biology approach.PLoS One. 2009 Jul
13;4(7):e6226.
Stapleton PD, Taylor PW. Methicillin resistance in Staphylococcus aureus: mechanisms and modulation. Sci Prog. 2002;85(Pt 1):57-72. Review.
Mechanism for methicillin resistance
Back to Patient: ER Visit 1
First diagnosis: Left upper extremity (forearm) cellulitis
- Initiated on Cephalexin 500mg TID for 7 days
- Appropriate option?

Evidence- No definitive evidence in terms of which antibiotic is the best for
mild-to-moderate cellulitis- Decision really depend on culture results, host factors, common
organisms in the local area, resistance patterns, severity, and cost & convenience
- Our recommendations are based on following resources:- Infectious Diseases Society of America guideline(IDSA) – Diagnosis and
Management of Skin and Soft-tissue infections1
- Sanford Antimicrobial guideline2
- Evidence-based Infectious disease book3
- Essential Evidence Plus – Cellulitis4
- Up-To-Date – Cellulitis5
1. Stevens DL, Bisno AL, Chambers HF, Everett ED, Dellinger P, Goldstein EJ, Gorbach SL, Hirschmann JV, Kaplan EL, Montoya JG, Wade JC. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis 2005 Nov 15;41(10):1373-406
2. Gilbert DN., Moellergin RC, Eliopoulos GM. Sandford Guideline to Antimicrobial Therapy. 40th Edition. Virginia, Sandford: Antimicrobial Therapy Inc. 2010: 1-219
3. Loeb M, Smaill Fiona, Smieja M. Cellulitis and Erysipelas. IN: Evidence-based infectious diseases. 2nd edition. NJ: John Wiley & Sons, Inc., 2009: 11-154. Carek PJ, Steyer TE. Essential Evidence Plus: Cellulitis. John Wiley & Sons, Inc., 2011. (Accessed June 12, 2011 at: www.essentialevidenceplus.com/content/eee/724)5. Lowy FD, Sexton DJ, Baron EL. Up-to-date: Cellulitis and erysipelas. UpToDate INC, 2010. (Accessed June 12, 2011 at: www.uptodate.com)

Antibiotics vs. MicrobesMicrobes Recommended Alternatives
S. aureus (MSSA) Cephalexin, CloxacillinParentral cephalosporins,Vancomycin, Clindamycin
Streptococci sp.
β-hemolytic streptococci (Group A, & B common) & S. pyogenes
Penicillin G or V (some add Gentamycin for serious Group B infection & some add clindamycin for serious invasive Group A)
All β lactams, erythromycin, clarithromycin, azithromycin(however, macrolideresistance increasing)
CA-MRSA
Mild to moderateTMP-SMX or Doxycycline or Minocycline
Clindamycin, third or fourth generation Fluoroquinilones
Severe Vancomycin Linezolid or daptomycin
HA-MRSA VancomycinTMP-SMX (some strains resistant), linezolid, daptomycin
Empiric antibiotic therapy for management of cellulitis should include activity against beta-hemolytic streptococci and S. aureus.
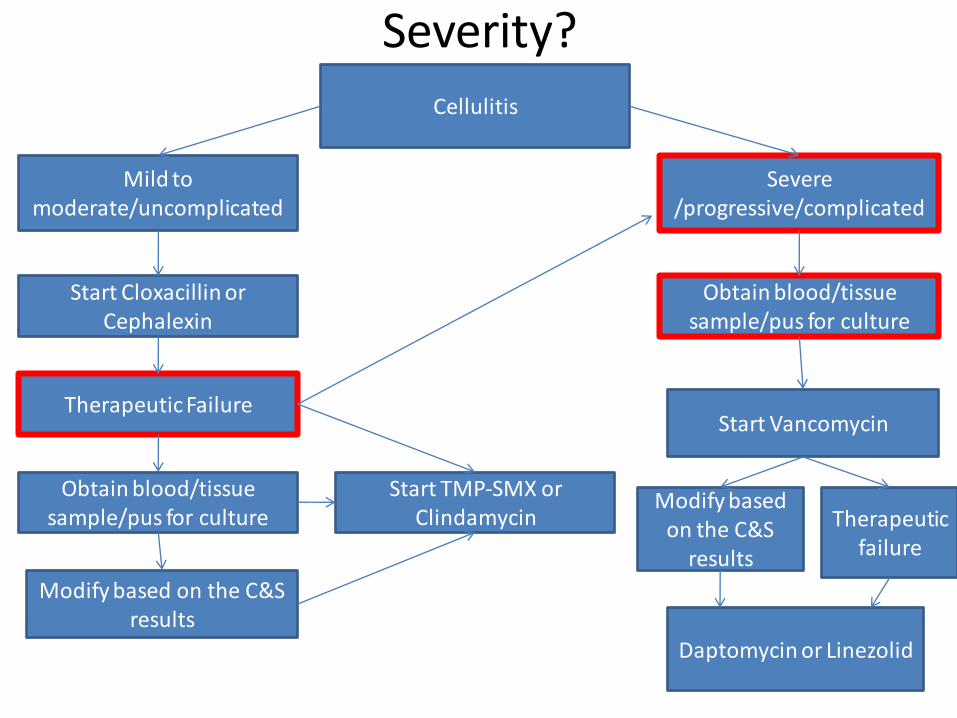
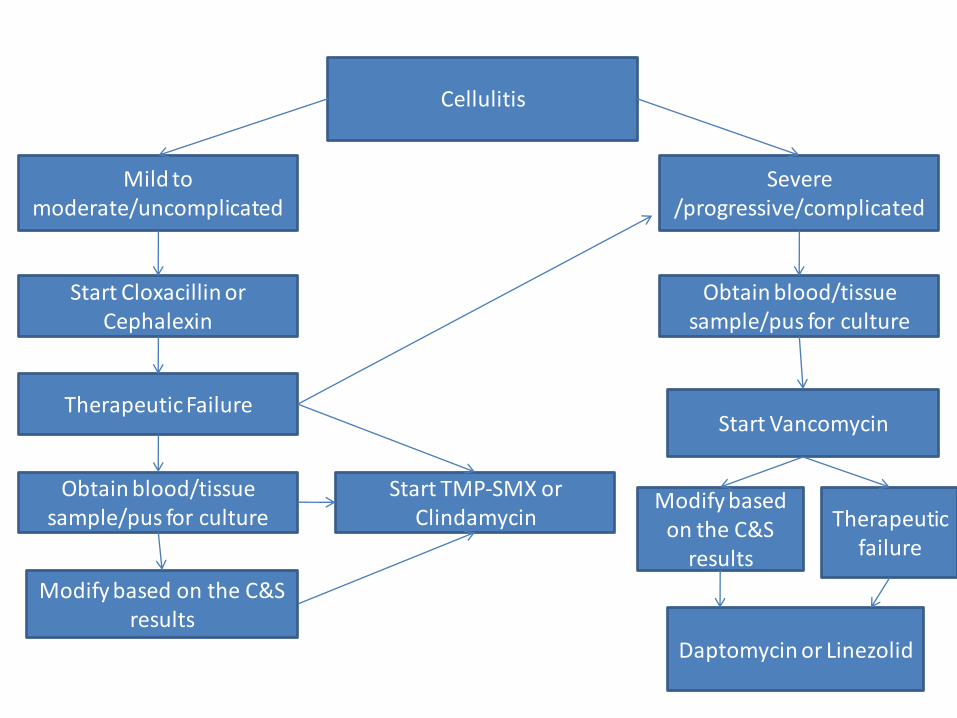
Cellulitis Therapeutic Treatment Algorithm

Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
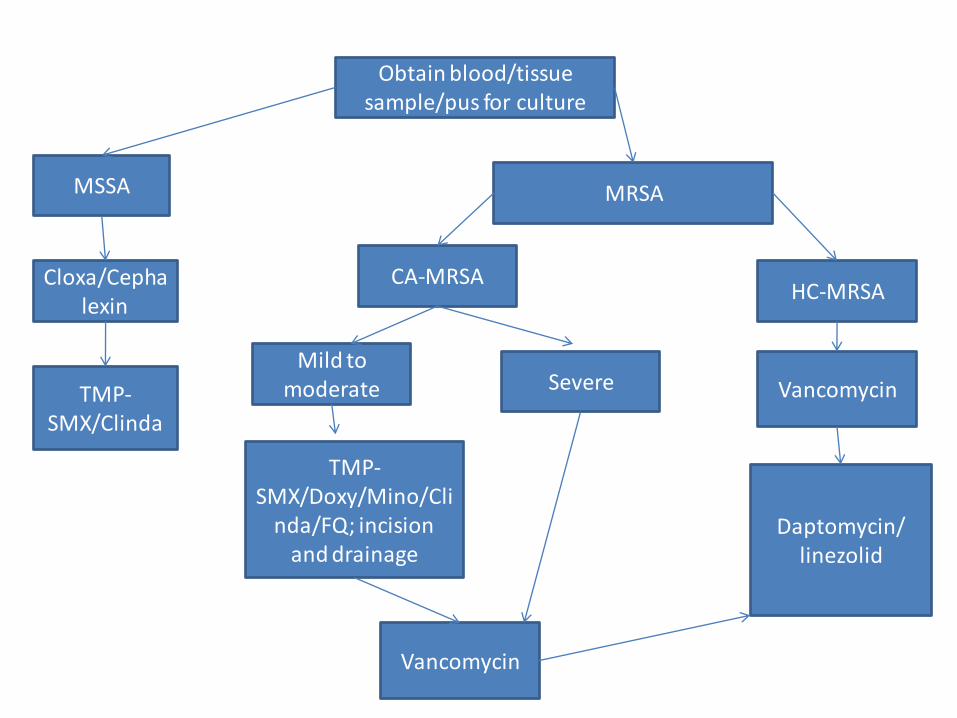
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid
Obtain blood/tissue sample/pus for culture
MRSAMSSA
Cloxa/Cephalexin
Mild to moderate
HC-MRSA
TMP-SMX/Clinda
Vancomycin
CA-MRSA
TMP-SMX/Doxy/Mino/Cli
nda/FQ; incision and drainage
Vancomycin
Daptomycin/linezolid
Severe

Answer
• Yes, cephalexin was appropriate
– Will see this clearer in the next few slides!
Back to patient: ER Visit 2
- His car was stolen and hence he did not take the medication
- He now has increase pain and swelling in the left arm, and also has new onset pain in his right shoulder and fever
- Severe?

Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid

Therapeutic alternatives
• Most commonly recommended
– Cephalexin
– Cloxacillin
– Clindamycin
– Trimethoprim-Sulfamethoxazole
– Fluoroquinolones
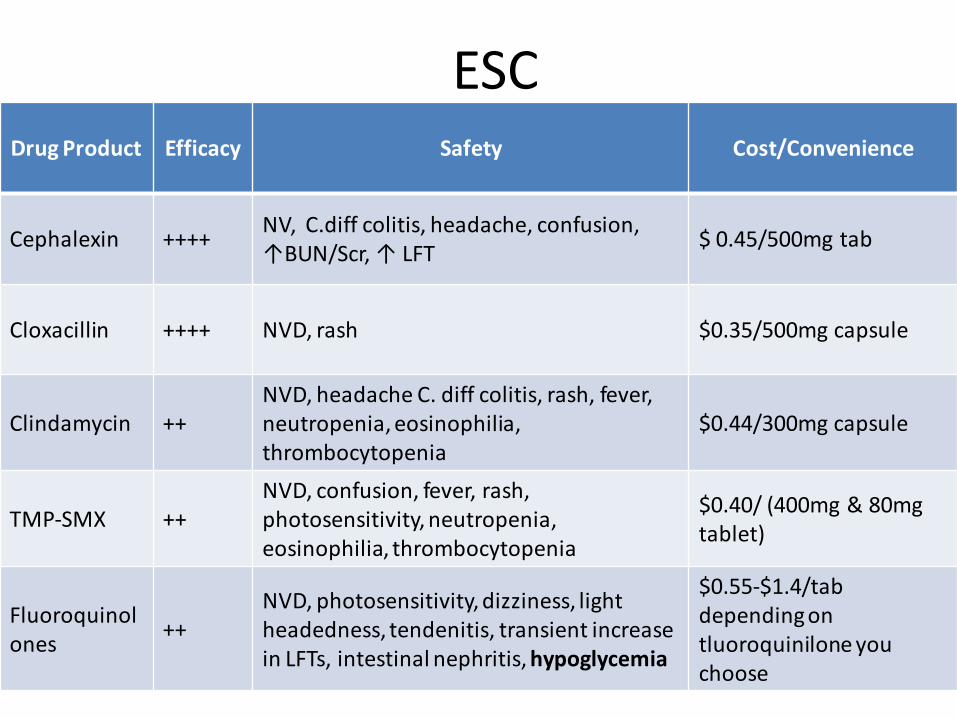
ESCDrug Product Efficacy Safety Cost/Convenience
Cephalexin ++++NV, C.diff colitis, headache, confusion, ↑BUN/Scr, ↑ LFT
$ 0.45/500mg tab
Cloxacillin ++++ NVD, rash $0.35/500mg capsule
Clindamycin ++NVD, headache C. diff colitis, rash, fever, neutropenia, eosinophilia, thrombocytopenia
$0.44/300mg capsule
TMP-SMX ++NVD, confusion, fever, rash, photosensitivity, neutropenia, eosinophilia, thrombocytopenia
$0.40/ (400mg & 80mg tablet)
Fluoroquinolones
++NVD, photosensitivity, dizziness, light headedness, tendenitis, transient increase in LFTs, intestinal nephritis, hypoglycemia
$0.55-$1.4/tab depending on tluoroquinilone you choose
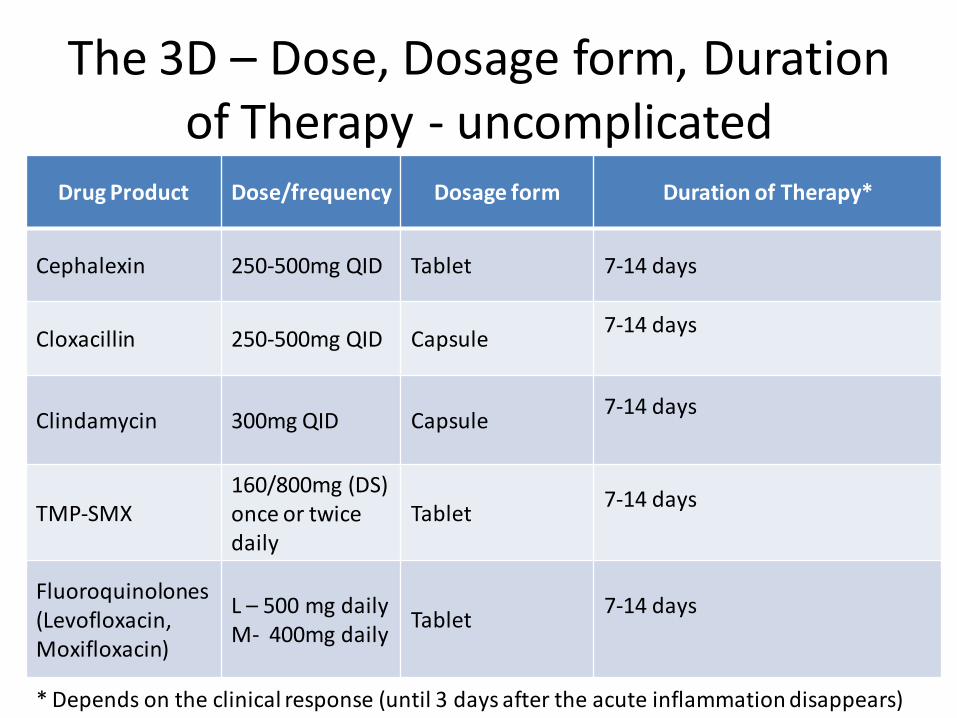
The 3D – Dose, Dosage form, Duration of Therapy - uncomplicated
Drug Product Dose/frequency Dosage form Duration of Therapy*
Cephalexin 250-500mg QID Tablet 7-14 days
Cloxacillin 250-500mg QID Capsule7-14 days
Clindamycin 300mg QID Capsule7-14 days
TMP-SMX160/800mg (DS) once or twice daily
Tablet7-14 days
Fluoroquinolones (Levofloxacin, Moxifloxacin)
L – 500 mg dailyM- 400mg daily
Tablet7-14 days
* Depends on the clinical response (until 3 days after the acute inflammation disappears)

Care Plan
Drug Product Dosage instructions Note changes
Cephalexin (Keflex) 500 mg four times a day for 7 days
Initiate
Indication: Cellulitis
Non-pharmacological:
•Patient education

Monitoring PlanEffectivenessParameter Change Timeframe
Clinical symptoms:Redness, edema, tenderness, warmth, pain, range of motion in affected area
Improved 24-48 hours
Temperature (38.3° C) Reduced to 37.5 ° C 24-48 hours
Pulse (96 bpm) Return (decrease) to normal (60-80 bpm)
24-48 hours
WBC count (26.3 x 10 3/mm3 ) 3.54 to 9.06 x 10 3/mm3 Improve in 3-4 daysNormal in 1 week
Bands (10%) 0-5% Improve in 3-4 daysNormal in 1 week
Neutrophils (81%) 40-70% Improve in 3-4 daysNormal in 1 week
Prevent complications (sepsis) None Continuously
Lowy FD, Sexton DJ, Baron EL. Cellulitis and erysipelas. Uptodate 2010. Retrieved June 15th, 2011.
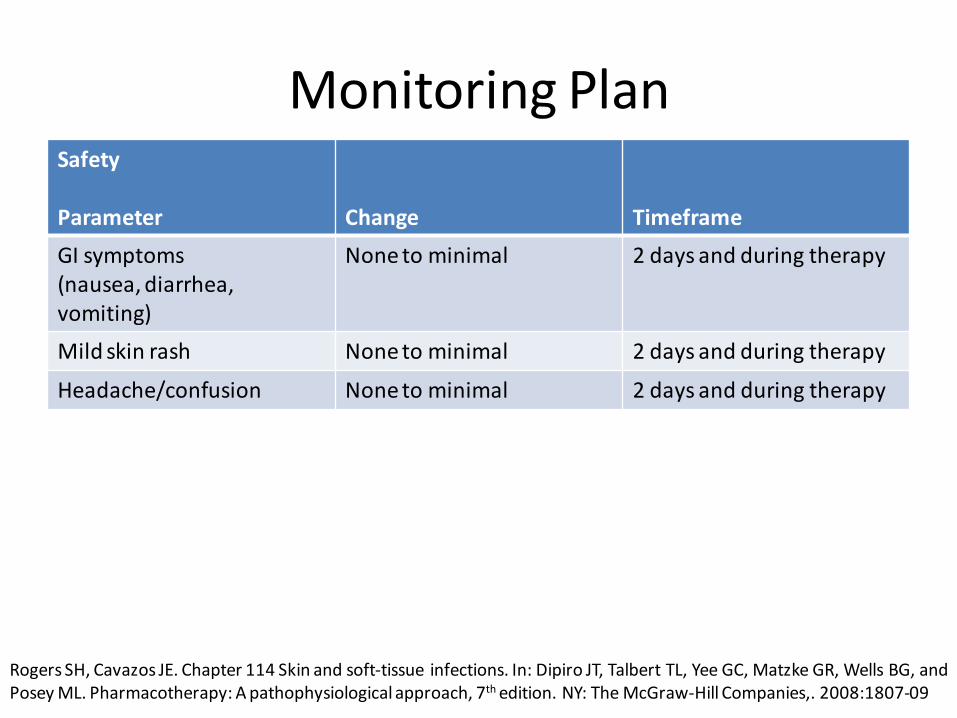
Monitoring PlanSafety
Parameter Change Timeframe
GI symptoms(nausea, diarrhea, vomiting)
None to minimal 2 days and during therapy
Mild skin rash None to minimal 2 days and during therapy
Headache/confusion None to minimal 2 days and during therapy
Rogers SH, Cavazos JE. Chapter 114 Skin and soft-tissue infections. In: Dipiro JT, Talbert TL, Yee GC, Matzke GR, Wells BG, and Posey ML. Pharmacotherapy: A pathophysiological approach, 7th edition. NY: The McGraw-Hill Companies,. 2008:1807-09
Therapeutic Failure
What is an alternative treatment if cephalexinfails?

Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid
Therapeutic Failure

Back to patient: ER visit 3
• CK took cephalexin as prescribed• Comes back to ER with following:
– Cellulitis progressing from left arm to right– Left arm cellulitis with pain, redness, tenderness,
increased edema– Right shoulder pain, tenderness, with new-onset right
axilla pain, and swelling; and left lower extremity pain radiating from the lower back
– Physical examination revealed: increase pitting edema of left arm, a right scapular fluid collection, a swollen right axilla, and adjacent lymphandopathy
ER visit 3
• MRI done to rule out compartment syndrome
• Two blood cultures drawn
• Orthopedics consulted for potential incision and drainage of the left arm cellulitis
• Admitted for complicated/progressive cellulitis and possible MRSA
• Started on Cefazolin 1g IV x one dose given in ED
Questions
• Severity?
• Appropriate drug of choice?
Background Information on MRSA
MRSA
• MRSA emerged in the 1960s– Health care associated MRSA ( HA-MRSA) 1
• Recently, MRSA infections without health care setting exposures is termed community-acquired MRSA (CA-MRSA) 1
• CA-MRSA associated with primarily skin and soft-tissue infections 1
– Sometimes associated with sepsis and necrotizing pneumonia 1
1) Rybak MJ, LaPlant KL. Community-associated methicillin-resistant Staypylococcusaureus: a review. Pharmacotherapy 2005;25:74-85
MRSA
• Defined as an oxicillin minimum inhibitory concentration
(MIC) 4mcg/mL 1
• If microorganism is resistant to oxicillin or methicillin,
they are also resistant to beta-lactam agents such as
dicloxacillin and cefazolin 1
• CA-MRSA tend to be less resistant than HA-MRSA and
has different types of gene complexes known as
staphylococcocal cassette chromosome mec (SCCmec) 2
1) Lowy FD, Sexton DJ, Baron EL. Treatment of skin and soft tissue infections due to methicillin-resistant Staphylococcus aureus in adults. Uptodate 2010. Retrieved June 15th, 2011.2) Rybak MJ, LaPlant KL. Community-associated methicillin-resistant Staphylococcus aureus: a review. Pharmacotherapy 2005;25:74-85

CA-MRSA vs. HA-MRSA
• The Centers for Disease Control and Prevention (CDC) has established a criteria to distinguish CA-MRSA and HA-MRSA 1
• CA-MRSA: 1
– Outpatient setting OR culture showing MRSA within 48 hours after admission to hospital
– In the following year before infection• No hospitalizations; admission to nursing home, skilled
nursing facility or hospice
• No indwelling catheters or medical devices that pass through the skin
1) Rybak MJ, LaPlant KL. Community-associated methicillin-resistant Staypylococcusaureus: a review. Pharmacotherapy 2005;25:74-85
Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid
Severity?
Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid
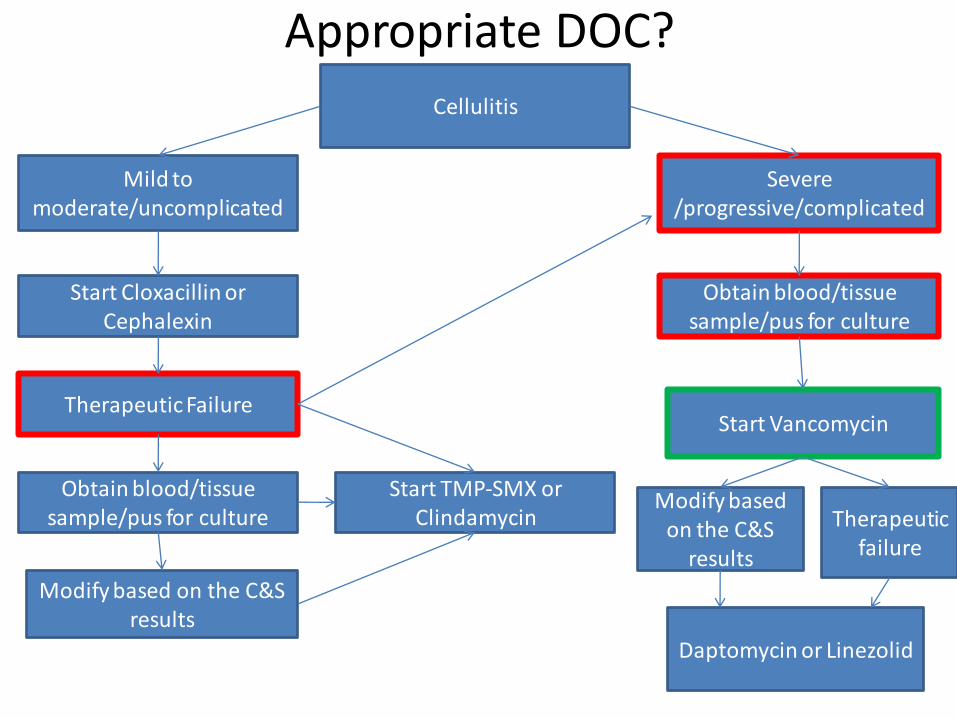
Appropriate DOC?

Obtain blood/tissue sample/pus for culture
MRSAMSSA
Cloxa/Cephalexin
Mild to moderate
HC-MRSA
TMP-SMX/Clinda
Vancomycin
CA-MRSA
TMP-SMX/Doxy/Mino/Cli
nda/FQ; incision and drainage
Vancomycin
Daptomycin/linezolid
Severe
Answers
• Very severe
• Cefazolin is an inappropriate drug of choice

Therapeutic Alternatives
- Vancomycin
- Linezolid
- Daptomycin

Vancomycin vs. LinezolidRCT: Non-blinded, open label, multi-centre
Goal: To compare effectiveness of linezolid vs. vancomycin in complicated skin and tissue infections
Patients: Infections caused by MRSA and severe enough to be hospitalized
Treatment: vancomycin 1g q 12 hour vs. linezolid 600mg twice daily for 7 days
Results: Clinical success rate in Vancomycin (88%) and linezolid (92%), not significant; adverse events similar in both group
Limitations: unblinded, conclusion favoring linezolid based on post-hoc group analysis, some patients were started on linezolid oral versus IV based on physician’s choice,
Bottom-line: Linezolid does not provide any significant advantages in terms of effectiveness over vancomycin. The unblinded nature of this study, post hoc subgroup analyses, and failure to describe criteria for initiating oral versus intravenous therapy are serious limitations. Any trends toward an advantage for linezolid should be interpreted very cautiously.
Weigelt J, Itani K, Stevens D, et al, for the Linezolid CSSTI Study Group. Linezolid versus vancomycin in treatment of complicated skin and softtissue infections. Antimicrob Agents Chemother 2005; 49:2260-66.
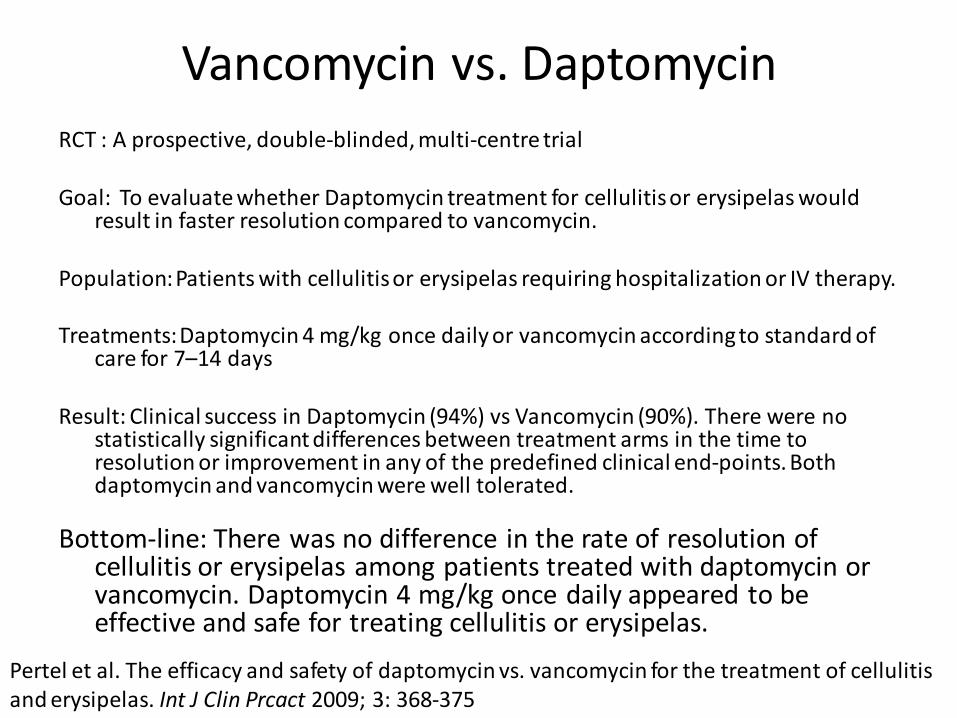
Vancomycin vs. Daptomycin
RCT : A prospective, double-blinded, multi-centre trial
Goal: To evaluate whether Daptomycin treatment for cellulitis or erysipelas would result in faster resolution compared to vancomycin.
Population: Patients with cellulitis or erysipelas requiring hospitalization or IV therapy.
Treatments:Daptomycin 4 mg/kg once daily or vancomycin according to standard of care for 7–14 days
Result: Clinical success in Daptomycin (94%) vs Vancomycin (90%). There were no statistically significant differences between treatment arms in the time to resolution or improvement in any of the predefined clinical end-points. Both daptomycin and vancomycin were well tolerated.
Bottom-line: There was no difference in the rate of resolution of cellulitis or erysipelas among patients treated with daptomycin or vancomycin. Daptomycin 4 mg/kg once daily appeared to be effective and safe for treating cellulitis or erysipelas.
Pertel et al. The efficacy and safety of daptomycin vs. vancomycin for the treatment of cellulitis and erysipelas. Int J Clin Prcact 2009; 3: 368-375
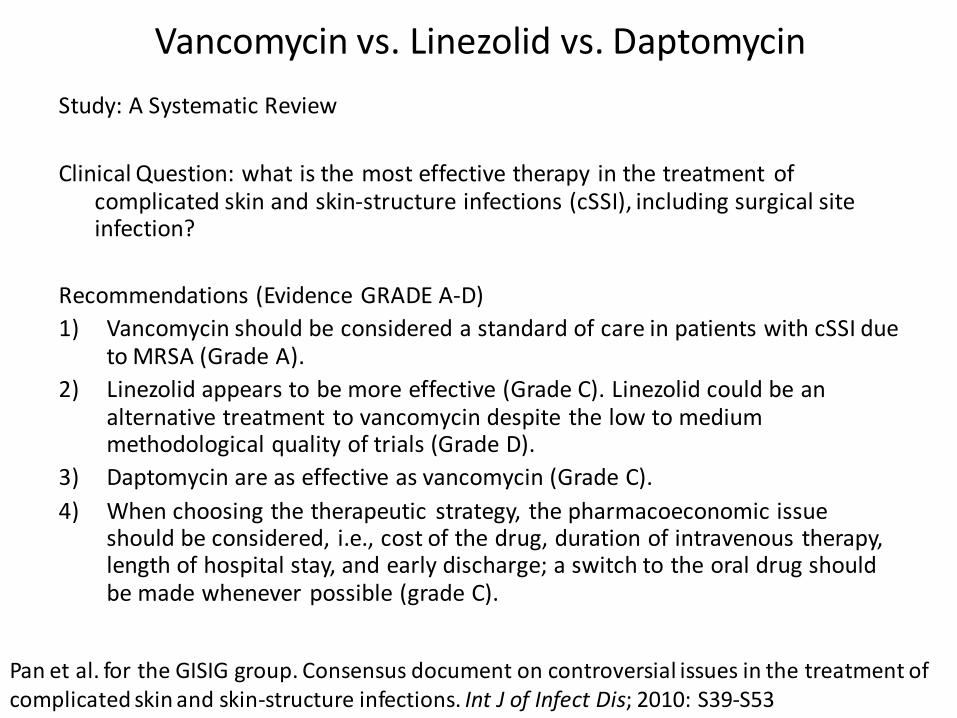
Vancomycin vs. Linezolid vs. Daptomycin
Study: A Systematic Review
Clinical Question: what is the most effective therapy in the treatment of complicated skin and skin-structure infections (cSSI), including surgical site infection?
Recommendations (Evidence GRADE A-D)
1) Vancomycin should be considered a standard of care in patients with cSSI due to MRSA (Grade A).
2) Linezolid appears to be more effective (Grade C). Linezolid could be an alternative treatment to vancomycin despite the low to medium methodological quality of trials (Grade D).
3) Daptomycin are as effective as vancomycin (Grade C).
4) When choosing the therapeutic strategy, the pharmacoeconomic issue should be considered, i.e., cost of the drug, duration of intravenous therapy, length of hospital stay, and early discharge; a switch to the oral drug should be made whenever possible (grade C).
Pan et al. for the GISIG group. Consensus document on controversial issues in the treatment of complicated skin and skin-structure infections. Int J of Infect Dis; 2010: S39-S53

ESC
Drug Product Efficacy Safety Cost/Convenience
Vancomycin +++++Nausea, vomiting, nephrotoxicity(rare), neutropenia, C. Diff., “red man syndrome”, Ototoxicity
$$$ IV
Linezolid ++++Nausea, vomiting, diarrhea, vision disturbances, headache, body aches, fever, rash
$$$$IVPO
Daptomycin ++++Vomiting, diarrhea, edema, numbness, tingling, headache, pneumonia, pain in throat, renal failure
$$$$IV
Note: Local antibiotic resistance patterns and culture susceptibility results are absolutely critical in tailoring the treatment. This table is a tool in selecting therapy when local resistance data and culture susceptibility are not available.

Care Plan
Drug Product Dosage instructions Note changes
Cefazolin 1g IV daily Discontinue
Vancomycin 1g every 12 hour, infused over two hours for 10 days
Initiate

Monitoring PlanEffectivenessParameter Change Timeframe
Clinical symptoms
Left arm -pain, redness, tenderness, increased swelling
Improvement in pain; decrease swelling
24-48 hours
Right shoulder pain, tenderness, right axillapain, and swelling; and swollen lymph nodes
Improvement in pain; decrease swelling
24-48 hours
Pain radiating to lower extremities
Decrease in severity of pain and radiation of pain subsides to the lower extremities
24-48 hours
Pain, redness, tenderness, swelling
Complete resolution 10-14 days
Shoulder motions Improve and normal Improve within 48 hours and normal within a week
BP/HR/temperature Improvement or stabilization 24-48 hours and on going
WBC/Neutrophils Improvement andnormalization
Improvement 24-48 hours; normalization – 10 to 14 days
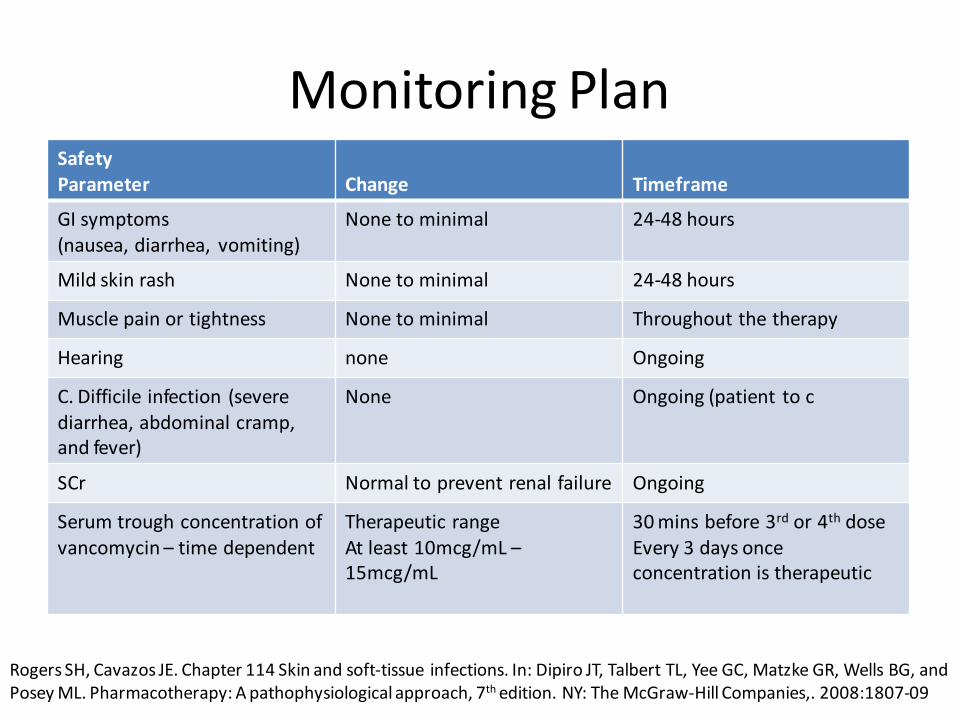
Monitoring PlanSafetyParameter Change Timeframe
GI symptoms(nausea, diarrhea, vomiting)
None to minimal 24-48 hours
Mild skin rash None to minimal 24-48 hours
Muscle pain or tightness None to minimal Throughout the therapy
Hearing none Ongoing
C. Difficile infection (severe diarrhea, abdominal cramp, and fever)
None Ongoing (patient to c
SCr Normal to prevent renal failure Ongoing
Serum trough concentration of vancomycin – time dependent
Therapeutic rangeAt least 10mcg/mL –15mcg/mL
30 mins before 3rd or 4th doseEvery 3 days once concentration is therapeutic
Rogers SH, Cavazos JE. Chapter 114 Skin and soft-tissue infections. In: Dipiro JT, Talbert TL, Yee GC, Matzke GR, Wells BG, and Posey ML. Pharmacotherapy: A pathophysiological approach, 7th edition. NY: The McGraw-Hill Companies,. 2008:1807-09
Therapeutic Failure
What to do if vancomycin does not work (improvement within 48 hour of effectiveness parameters) or the patient experiences serious side effects?

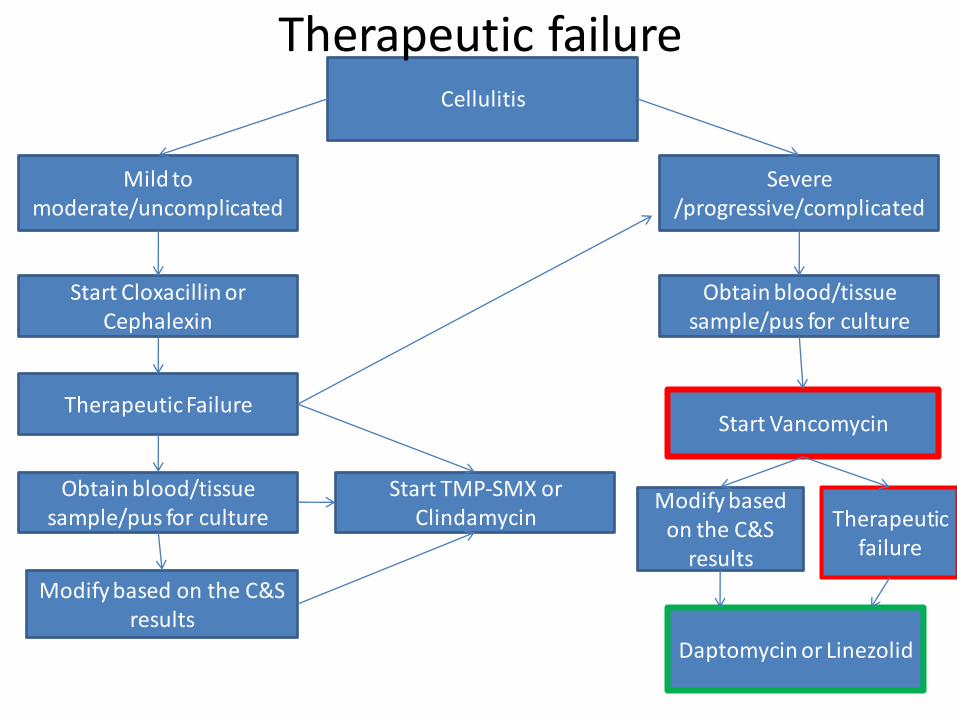
Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid
Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid
Therapeutic failure
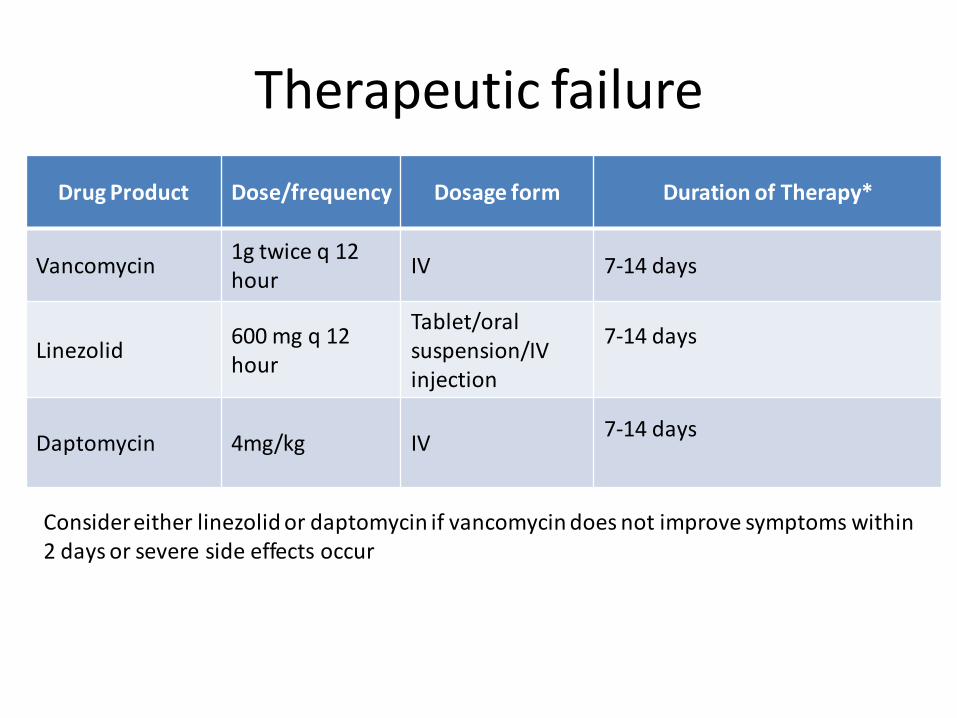
Therapeutic failure
Drug Product Dose/frequency Dosage form Duration of Therapy*
Vancomycin1g twice q 12 hour
IV 7-14 days
Linezolid600 mg q 12 hour
Tablet/oral suspension/IVinjection
7-14 days
Daptomycin 4mg/kg IV7-14 days
Consider either linezolid or daptomycin if vancomycin does not improve symptoms within 2 days or severe side effects occur

Follow-up regarding other DTPs
• Follow up with his family physician regarding additional therapy for CV prevention secondary to diabetes and stroke prevention secondary to his atrial fibrillation
• CVD risk reduction strategy – statin and ACE inhibitor therapy
• Assess patient’s desire for smoking cessation
Patient Education
• Elevation of affected area
– Improves draining of edema and inflammatory substances
• Keep affected area clean and dry
– Avoid antibacterial creams and ointments
• Keep skin hydrated to prevent cracks
• Patience
– Takes time to heal
Lowy FD, Sexton DJ, Baron EL. Cellulitis and erysipelas. Uptodate 2010. Retrieved June 15th, 2011.

Patient Education
• Adherence to antibiotics in the future
– Explain importance of full duration of treatment
• Effectiveness and resistance
– Explain side effects
• Adherence to his other medications ( i.e. Meformin,
consequence of diabetes, diet restrictions etc)
• Prevention
– Proper skin wound care
– Proper nutrition
Lowy FD, Sexton DJ, Baron EL. Cellulitis and erysipelas. Uptodate 2010. Retrieved June 15th, 2011.

Summary
• Cellulitis is a type of skin and soft tissue infection, affecting epidermis, dermis, and subcutaneous layers
• CK diagnosed with LUE cellulitis, but lost prescription for cephalexin,– returned 5 days later with progressing cellulitis
• given cephalexin
• CK took cephalexin as prescribed, but came back to ER again with progressing cellulitis (severe)– admitted for complicated/progressive cellulitis and possible MRSA
• given vancomycin
• CK also had multiple other drug therapy problems needing to be addressed at a later date– education regarding his conditions and medications– CV disease prevention
Cellulitis
Severe /progressive/complicated
Mild to moderate/uncomplicated
Obtain blood/tissue sample/pus for culture
Start Vancomycin
Modify based on the C&S
results
Therapeutic failure
Obtain blood/tissue sample/pus for culture
Start Cloxacillin or Cephalexin
Therapeutic Failure
Start TMP-SMX or Clindamycin
Modify based on the C&S results
Daptomycin or Linezolid

QUESTIONS?