
Recommendations for Evaluation of Prosthetic Valves With Echocardiography and Doppler Ultrasound

Br Heart J 1989;62:1-8
Colour flow Doppler mapping in the assessment ofprosthetic valve regurgitationJOHN CHAMBERS MARK MONAGHAN, GRAHAM JACKSON
From the Cardiac Department, King's College Hospital, London
SUMMARY Two hundred Carpentier-Edwards, Bjork-Shiley, and Starr-Edwards prostheses in173 patients were examined. Sixteen (16%) in the aortic and 24 (25%) in the mitral position wereassociated with clinical signs of regurgitation. A phased array system (Hewlett-Packard A77020A)with a 2-5 MHz duplex and 1-9 MHz continuous wave transducer was used. Colour flow mappingshowed trivial transvalvar regurgitation in 23 (53%) metal aortic prostheses, and only nine (20%)metal mitral prostheses. This difference was probably attributable to shielding ofthe left atrium bythe metal components. Colour mapping confirmed abnormal regurgitation in all aortic prostheseswith early diastolic murmurs, but regurgitation was also shown in 25 (29%) with no diastolicmurmur. Abnormal mitral regurgitation was found in 13 (54%) patients with a pansystolicmurmur, but also in six (8%) with no systolic murmur. Two patients, thought on clinical groundsto have mild mitral regurgitation, had unexpectedly large jets on colour flow mapping. About one
in three prostheses had paraprosthetic leaks, 65 (79%) ofwhich were small with a jet area less than20% of the area of the receiving chamber. The development ofnew paraprosthetic leaks led to thediagnosis of bacterial endocarditis in two patients. In eight patients regurgitation was firstdiagnosed with continuous wave Doppler, but was afterwards shown with colour mapping and in a
further 10 regurgitation could only be shown by continuous wave Doppler.Colour flow mapping was less sensitive than continuous wave Doppler in detecting regurgita-
tion, but seemed able to distinguish normal transvalvar from paraprosthetic regurgitation. Furtherstudies in the natural course of paraprosthetic leaks and a comparison of the transoesophageal andtransthoracic approaches in the assessment of mitral prostheses are needed.
It is important to be able to detect and localise the siteof regurgitation associated with prosthetic valves.The development of a new leak in a paraprostheticposition may suggest bacterial endocarditis or in atransvalvar position may be the first indication ofprimary failure in a bioprosthesis. It is also useful tobe able to guide the surgeon when repair of aparaprosthetic leak is required.
Continuous wave Doppler ultrasound is highlysensitive for the detection of regurgitation, but itcannot pinpoint the leak. Although localisation ispossible with conventional pulsed Doppler, it is timeconsuming and of limited accuracy.`13 Colour flowDoppler mapping gives a cross sectional version ofconventional pulsed Doppler. Velocity and direc-tional information are collected at multiple depths
Requests for reprints to Dr John Chambers, Cardiac Unit, Guy'sHospital, St Thomas Street, London SEI 9RT.
Accepted for publication 24 January 1989
down each scan line and are then superimposed on across sectional echocardiographic image in real time.Colour flow Doppler mapping is highly sensitive fordetecting regurgitation in native valves,45 but thereare no published studies of its application in theassessment of regurgitation associated with pros-thetic valves.The aim of this study was to establish the role and
likely benefits of colour flow Doppler mapping inassessing the incidence, severity, and localisation ofregurgitant jets in prosthetic valves.
Patients and methods
PATIENTSConsecutive patients with prosthetic valves referredeither for routine echocardiography or with sus-pected prosthetic regurgitation were studied from1 December 1986 to 30 March 1988. Patients withtricuspid valve prostheses or aortic and mitral pros-theses other than Carpentier-Edwards, Bjork-
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from
Chambers, Monaghan, Jackson
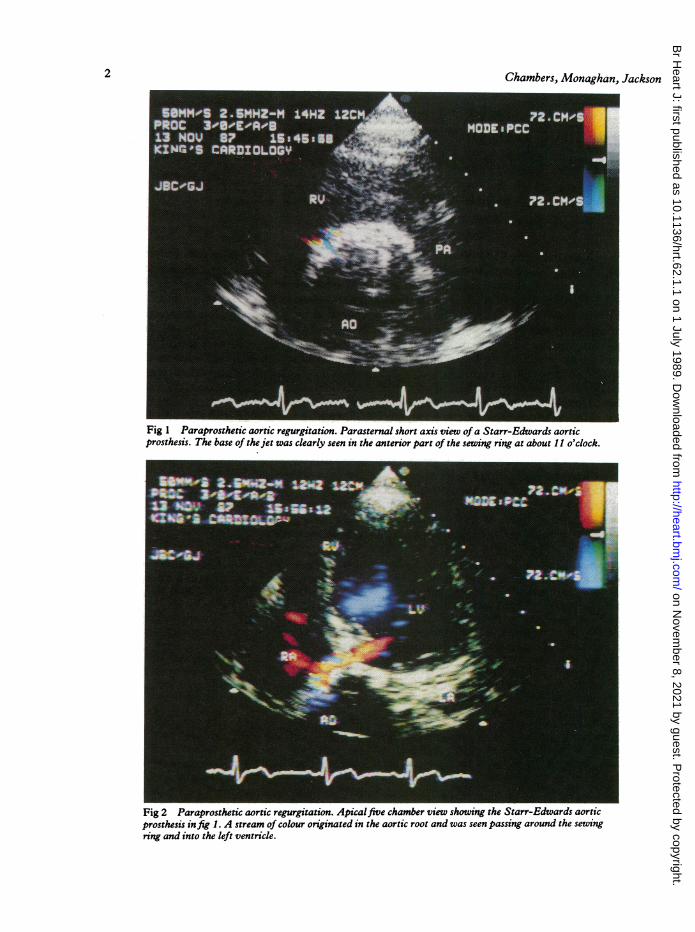
Fig 1 Paraprosthetic aortic regurgitation. Parasternal short axis view ofa Starr-Edwards aorticprosthesis. The base of the jet was clearly seen in the anterior part of the sewing ring at about 11 o'clock.
__~~~~~~~~~~
Fig 2 Paraprosthetic aortic regurgitation. Apicalfive chamber view showing the Starr-Edwards aorticprosthesis in fig 1. A stream of colour originated in the aortic root and was seen passing around the sewingring and into the left ventricle.
2
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from

Colourflow Doppler mapping in the assessment ofprosthetic valve regurgitation
Fig 3 Paraprosthetic aortic regurgitation. Apicalfour chamber view of a Starr-Edwards mitral valve.Flow accekration (red) was seen within the left ventricle at the edge of the sewing ring. There was a mitralregurgitant jet in the left atriwn, but no clear stream of colour around the prosthesis.
Shiley, or Starr-Edwards were excluded becausethere were too few of them. This left 200 prosthesesin 173 patients. There were 103 aortic prostheses inwhich 16 (16%) had the murmur of aortic regurgita-tion and 97 mitral prostheses of which 24 (25%) hadpansystolic murmurs.
APPARATUSWe used a phased array ultrasound system (Hewlett-Packard A77020A) with a 1 9 MHz continuous waveDoppler probe and a duplex 2 5 MHz transducer forimaging and colour flow Doppler mapping. Thecolour flow Doppler system was set to maximumpacket size and minimum reject with the gain justbelow the level at which ambiguous colour floodingoccurred. Both enhanced and variance thresholdmaps were used. Recordings were made on toprofessional quality three quarter inch U-matic tape.
STUDYA clinical examination was performed to look forevidence of prosthetic dysfunction or coexistenttricuspid regurgitation. Cross sectional imaging withcolour flow Doppler was then performed in allconventional approaches and in addition the trans-
ducer was tilted in an attempt to detect areas ofabnormal flow in more anterior and posterior posi-tions. The parasternal short axis view was found to beparticularly useful for localising aortic jets (fig 1). Acontinuous wave examination was then performedfrom the apical approach with multiple gain settingsand angulations. If a regurgitant jet was shown forthe first time on continuous wave Doppler a secondattempt was made to detect it by colour flow Dopplermapping.
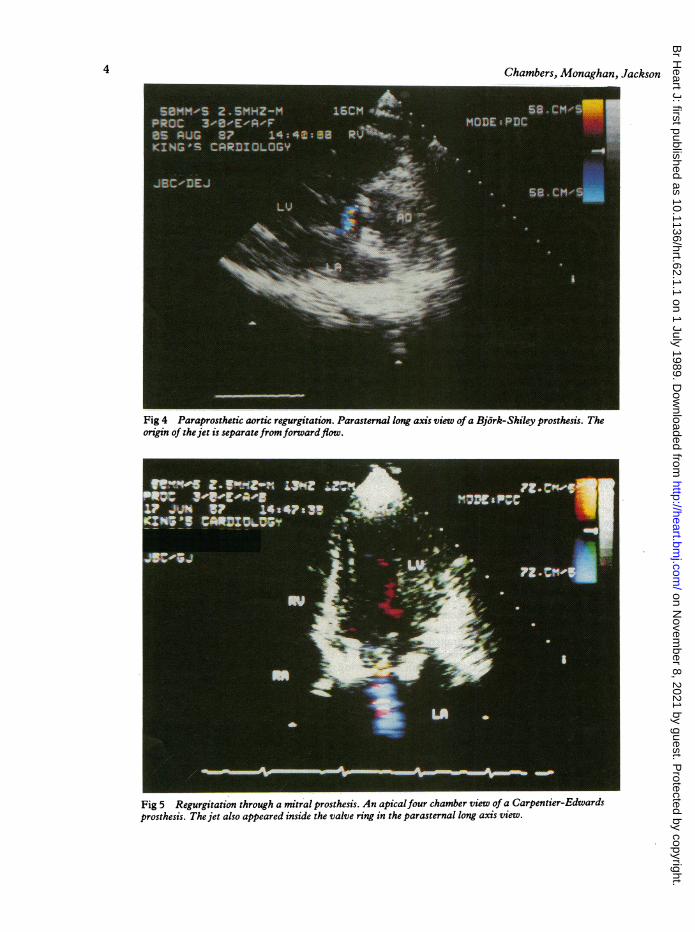
Regurgitation was considered to be paraprostheticif: (a) a stream of colour was visible around thesewing ring in mitral prostheses during systole and inaortic prostheses during diastole (fig 2); (b) the originofthe regurgitant jet was visible at a point outside thesewing ring although there was no visualisation offlow around the valve (fig 3); (c) the origin of theregurgitant jet was in the region of the sewing ringand although not clearly outside the ring, wasseparate from forward flow (fig 4).
Regurgitation was considered to be transvalvar if:(a) its origin was seen within the orifice (as defined bythe forward flow pattern) in at least two differentviews (fig 5); (b) in metal mitral prostheses systolicretrograde flow was seen originating at the edge ofthe
3
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from
Chambers, Monaghan, Jackson
Fig 4 Paraprosthetic aortic regurgitation. Parasternal long axis view of a Bjork-Shiley prosthesis. Theorigin of the jet is separatefromforwardflow.
Fig 5 Regurgitation through a mitral prosthesis. An apicalfour chamber view of a Carpentier-Edwardsprosthesis. The jet also appeared inside the valve ring in the parasternal long axis view.
4
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from

Colourflow Doppler mapping in the assessment ofprosthetic valve regurgitation
Fig 6 Parasternal long axis view of transvalvar regurgitation. A high velocity jet was recorded by
continuous wave. On colourflow Doppler mapping, there was high velocityflow (blue) between the disc andthe sewing ring continuous with a billowing low velocity jet seen within the left atrium in systole.
occluder (disk or ball) in the parasternal long axisview (fig 6); or (c) beyond the shielding of theoccluder in the absence of evidence of a parapros-thetic leak.The severity of paraprosthetic aortic regurgitation
was estimated from the arc occupied by the base ofthe jet around the sewing ring. The maximum area ofthe aortic or paraprosthetic mitral jet was alsoexpressed as a percentage of the receiving chamberarea6 when the approach that gave optimal imaging ofthe jet was used. A semiquantitative estimate of jetarea in transmitral regurgitation was not attemptedbecause of shielding by the metal components.
Five patients with severe prosthetic dysfunctionwere evaluated by cardiac catheterisation and con-trast injection-four proceeded to operation. Onefurther patient had an operation without previouscatheterisation and four cases had catheterisation forcoronary artery disease and the prosthesis was alsoevaluated at this time.
Results
INCIDENCE OF REGURGITATIONRegurgitation was detected in 97 (49%) prostheses
(table 1). Trivial transvalvar regurgitation was shownmore commonly in the Bjork-Shiley (63%) than theStarr-Edwards (27%) prostheses in the aortic posi-tion, but in similar frequencies in the mitral position.Paraprosthetic leaks occurred in 73% Starr-Edwardsaortic prostheses, in 6% Carpentier-Edwards mitralprostheses, and in 21-28% of Starr-Edwards mitral,Carpentier-Edwards aortic, Bjork-Shiley mitral, andBjork-Shiley aortic. Of the 12 Carpentier-Edwardsprostheses with transvalvar regurgitation, all but onehad been in position for longer than 48 months (mean77 (29) months). Of those with paraprosthetic re-gurgitation, eight (40%) had been in position for lessthan 12 months. It was impossible to localise the siteof regurgitation in one Carpentier-Edwards prosth-esis where the base of the jet was broad.
Aortic regurgitation was confirmed in all pros-theses with an early diastolic murmur, but mildparaprosthetic regurgitation was also found in afurther 25 (29%) of 87 patients with no murmur. Ofthe 24 cases with pansystolic murmurs, 13 (54%) hadmitral regurgitation and in the others only tricuspidregurgitation was found. One mitral prosthesis with ahigh pitched ejection systolic murmur had minorregurgitation originating at the base of one cusp.
5
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from

Table 1 Occurrence of regurgitation shown by ultrasound (percentages in parentheses)
Carpentier-Edwards Bj6rk-Shiley Starr-Edwards
AVR MVR AVR MVR AVR MVR(n = 60) (n = 53) (n = 32) (n = 29) (n = 11) (n = 15)
Total frequency 23 (38) 11 (21) 30 (94) 17 (59) 10 (91) 6 (40)PP on CFD 17 (28) 3 (6) 9 (28) 6 (21) 8 (73) 4 (27)Transvalvar on CFD 6 (10) 6 (11) 20 (63) 7 (24) 3 (27) 2 (13)PP and transvalvar 1 (2) 0 3 (9) 0 2 (18) 0Uncertain 1 0 0 0 0 0Multiple PP 1 1 1 0 0On CW not CFD 0 2 4 (13) 4 (14) 1 0Murmur 8 (13) 7 (13) 5 (16) 4 (14) 3 (27) 2 (13)
AVR, aortic valve replacement; CFD, colour flow Doppler; CW, continuous wave Doppler; MVR, mitral valve replacement; PP,paraprosthetic.
Two further mitral valves with new ejectionmurmurs had demonstrable flow acceleration in theleft ventricular outflow tract thought to be related tothe tip ofone ofthe stents. Ofthe 73 mitral prostheseswith no pansystolic murmur, six (8%) had para-prosthetic mitral regurgitation. Most cases of severeprosthetic dysfunction were suspected clinically, butin two severe paraprosthetic mitral regurgitation wasshown by colour flow Doppler despite only softpansystolic murmurs. In two patients the develop-ment of new paraprosthetic regurgitation led to thediagnosis of bacterial endocarditis. A further 11patients with unexplained breathlessness wereshown to have normal prosthetic function.
SEVERITY OF REGURGITATION (TABLE 2)Most of the regurgitant jets were small. The area ofthe jet in 65 (79%) was less than 20% ofthe receivingchamber area. Shielding by the prosthesis precludedreliable estimation of the severity of regurgitationthrough metal mitral prostheses. Paraprostheticmitral regurgitant areas were also likely to have beenunderestimated because ofpartial shielding ofthe jet.The base of the aortic jet involved approximately
Table 2 Severity of regurgitation
<100% 10-19% 20-40% >40%
Aortic CE:PP 4 11 2 0Through 1 3 1 1
Mitral CE:PP 2 1 0 0Through 4 0 1 1
Aortic BS:PP 2 2 3 2Through 13 7 0 0
Mitral BS:PP 2 2 2 0
Aortic SE:PP 2 4 1 1Through 2 1 0 0
Mitral SE:PP 1 1 2 0
900 ofthe ring in one prosthesis, approximately 450 ineight, and < 200 in the remaining 37. Table 3 showsthe distribution of the jets. The jets were multiple inorigin in three prostheses.
COLOUR FLOW DOPPLER COMPARED WITHCONVENTIONAL DOPPLERAll regurgitant jets shown by colour flow Dopplerwere also recorded by continuous wave or conven-tional pulsed Doppler. There were, however, 10patients in whom low intensity regurgitant jetsshown by continuous wave were not seen on colourflow Doppler. In eight further patients, regurgitationwas missed with the first colour flow Dopplerexamination but shown at a subsequent examination.There were 15 patients with regurgitant prostheses
who had been examined by conventional Dopplerultrasound alone and in whom it had not beenpossible confidently to localise the jet. We thoughtthat localisation was possible with colour flowDoppler in all of these patients.
COMPARISON WITH CATHETER OR FINDINGS AT
OPERATIONCardiac catheterisation was performed in fivepatients and confirmed the Doppler findings in all ofthem. There was mild regurgitation through aseverely stenotic prosthesis in two patients and
Table 3 Localisation ofparaprosthetic regurgitant jets
Type of valve Anterior Posterior RV side LV side
Aortic:CE 8 7 5 1BS 6 1 2 1SE 3 3 1 1
Mitral: Anterior Posterior Septal Free wallCE 1 1 1 0BS 4 0 1 2SE 1 0 1 2
CE, Carpentier-Edwards; BS, Bj6rk-Shiley; PP, paraprosthetic; CE, Carpentier-Edwards- BS, Bjork-Shiley; LV, left ventricle;SE, Starr-Edwards. RV, right ventricle; SE, Starr-Edwards.
6 Chambers, Monaghan, Jackson
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from

Colour flow Doppler mapping in the assessment ofprosthetic valve regurgitation
severe paraprosthetic regurgitation in three. Atoperation, however, one patient who was thought tohave a paraprosthetic leak was found to have a sinusbetween the base of the cusp and the stent, but nodehiscence of the sewing ring. The colour flowfindings were confirmed in the other four patients.Two patients thought to have considerable parapros-thetic regurgitation had severe intercurrent illnesswhich prevented further intervention. Catheterisa-tion was also performed for suspected coronaryartery disease in four patients with Carpentier-Edwards prostheses; it confirmed the absence ofregurgitation.
Discussion
This is the first study to use colour flow Dopplermapping to describe patterns of regurgitation in aconsecutive series of patients with prosthetic valves.The striking finding was the high frequency ofunsuspected paraprosthetic regurgitation in pros-theses of all three types in the aortic position and inBjork-Shiley and Starr-Edwards prostheses in themitral position.Most of the regurgitant jets were, however, small
and probably not haemodynamically important.Furthermore, most severely dysfunctioning pros-theses were diagnosed clinically. Was colour flowmapping, therefore, of clinical use? Two patientswith severe paraprosthetic regurgitation were firstdiagnosed with colour flow Doppler and in twofurther patients newly developed mild regurgitationled to the diagnosis of bacterial endocarditis. Local-isation of the site of regurgitation guided the surgeonin all three patients with paraprosthetic leaks whounderwent reoperation. In all 24 mitral prostheseswhere a new systolic murmur was heard after opera-tion, colour flow mapping was able to localise theorigin of the flow disturbance to the mitral ortricuspid valve or to the left ventricular outflow tract.It may be difficult clinically to exclude mitral pros-thetic regurgitation in a patient with coexistenttricuspid regurgitation. Colour flow mapping alsocontributed by excluding significant prostheticregurgitation in 11 patients in whom the cause offailure to improve after operation was not obviousclinically.
Paraprosthetic leaks may occur because the bedcreated by scraping away calcified tissue is neverperfectly circular so that the prosthesis cannot alwaysfit snugly. Regurgitation may be less common in theCarpentier-Edwards mitral prostheses because theannulus is covered in sponge and may allow a betterfit than the rings ofmetal prostheses. The state oftherecipient tissue, the type and technique of suturing,and the methods of myocardial preservation may all
contribute to the development of paraprostheticregurgitation and future studies should evaluatethese prospectively.Normally functioning Bjork-Shiley and Starr-
Edwards prostheses have trivial transvalvar leaksduring closure. In the aortic prostheses these jetswere always small, less than 20% of the receivingchamber area, and usually narrow. Twin jets weresometimes seen. Transvalvar regurgitation was seenless commonly in the mitral prostheses. In thisposition, access can be improved by the use of thetransoesophageal approach, which allows interroga-tion of the left atrium without the problem ofshielding. It is likely that shielding by mitral pros-theses was the reason why paraprosthetic regurgita-tion was seen more frequently with valves in theaortic rather than the mitral position. There is,however, no published study describing the resultsthat can be obtained with the transoesophagealapproach and how often clinically important infor-mation gained by this route is missed by the trans-thoracic approach. Most studies with conventionalDoppler reported lower incidences of regurgitationthan shown here, but they were studies of smallnumbers.278 A study of the functioning of Bjork-Shiley prostheses by colour flow Doppler failed tofind regurgitation in any of the 10 aortic prosthesesexamined.9 The fact that we detected regurgitation in63% of aortic prostheses probably reflects theincreased sensitivity of the apparatus that we used.There is uncertainty about whether any regurgita-
tion through Carpentier-Edwards prostheses can beregarded as normal. Conventional ultrasoundshowed regurgitation in 8-26% of aortic pros-theses810' and in 4-11% of mitral prostheses.'01' Wefound valvar regurgitation in 10% of the aortic and11% of the mitral valves. Only one regurgitantprosthesis had been in position for less than 48months; this suggests that transvalvar regurgitationis a sign of primary failure.
Systematic validation with angiography of thelocalisation of regurgitation by colour Doppler map-ping is not a practical proposition. Furthermore,angiography may be less accurate than Dopplerultrasound' and it is possible that colour flowDoppler mapping will soon be considered thereference standard for localisation. In one case in thisseries a leak at the base of the cusp was wronglydiagnosed as being paraprosthetic. This emphasisesthat colour flow Doppler mapping may not alwaysreliably distinguish between eccentric jets through aprosthesis and paraprosthetic leaks. When abnormalflow is clearly seen around the sewing ring it isunlikely that mistakes can be made.The area of the regurgitant jet shown by colour
flow Doppler is dependent on gain and instrument
7
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from

8 Chambers, Monaghan, Jacksonsettings"2"3 and may not always give an accurateassessment of the severity of regurgitation. Helmckeet al, however, have shown a good correlation be-tween the angiographically assessed severity andmitral regurgitant jet area expressed as a percentageofleft atrial area.'4 Most patients with mild regurgita-tion by angiographic criteria had regurgitant areas ofless than 20% and most with severe regurgitation hadareas over 40%.We conclude that colour flow Doppler mapping
detects most expected and abnormal regurgitant jets,most of which are small and probably not haemo-dynamically important. Occasionally, however, theyare more severe than had been suspected on clinicalgrounds. New paraprosthetic leaks suggest the pos-sibility of bacterial endocarditis. The technique isuseful for the localisation ofnew murmurs appearingafter mitral valve replacement and probably forexcluding important valve dysfunction. Furtherstudies of the natural course of paraprosthetic regur-gitation and comparative studies of the transoeso-phageal and transthoracic approaches in the assess-ment of prostheses should now be undertaken.
JC holds a British Heart Foundation Fellowship. MrKerry Packer donated the colour flow system.
References
1 Veyrat C, Wichitz S, Lessana A, Ameur A, Abitbol G,Kalmanson D. Valvar prosthetic dysfunction. Local-isation and evaluation of the dysfunction using theDoppler technique. Br Heart J 1985;54:273-84.
2 Sagar KB, Wann S, Paulsen WHJ, Romhilt DW.Doppler echocardiographic evaluation of Hancockand Bjork-Shiley prosthetic valves. JAm Coll Cardiol
1986;7:681-7.3 Chambers JB, Monaghan MJ, Jackson G, Jewitt DE.
Doppler echocardiographic appearance of cusp tearsin tissue valve prostheses. J Am Coll Cardiol 1987;10:462-6.
4 Switzer DF, Nanda NC. Doppler color flow mapping.Ultrasound Med Biol 1985;1 1:403-16.
5 Omoto R, Yokote Y, Takamoto S, et al. The develop-ment of real-time two-dimensional Doppler echocar-diography and its clinical significance in acquiredvalvular diseases. Jpn Heart J 1984;25:325-40.
6 Miyatake H, Izumi S, Okamoto M, et al. Semiquanti-tative grading of severity of mitral regurgitation byreal-time, two-dimensional Doppler flow imagingtechnique. J Am Coll Cardiol 1986;7:82-8.
7 Panidis IP, Ross J, Mintz GS. Normal and abnormalprosthetic valve function as assessed by Dopplerechocardiography. JAm Coll Cardiol 1986;8:317-26.
8 Ramirez ML, Wong M, Sadler N, Shah PM. Dopplerevaluation of bioprosthetic and mechanical aorticvalves: data from four models in 107 stableambulatory patients. Am Heart J 1988;115:418-25.
9 Dittrich H, Nicod P, Hoit B, Dalton N, Sahn D.Evaluation of Bjork-Shiley prosthetic valves by real-time two-dimensional Doppler echocardiographicflow mapping. Am Heart J 1988;115:133-8.
10 Cooper DM, Stewart WJ, Schiavone WA, et al. Evalua-tion of normal prosthetic valve function by Dopplerechocardiography. Am Heart J 1987;114:576-82.
11 Gibbs JL, Wharton GA, Williams GJ. Doppler echo-cardiographic characteristics of the Carpentier-Edwards xenograft. Eur Heart J 1986;7:353-6.
12 Sahn DJ, Chung KJ, Tamura T, et al. Factors affectingjet visualisation by color flow mapping Doppler echo:in vitro studies [Abstract]. Circulation 1986;74(supplII):271.
13 Otsuji Y, Tei C, Kisanuki A, Natsugoe K, Kawazoe Y.Color Doppler echocardiographic assessment of thechange in the mitral regurgitant volume. Am Heart J1987;114:349-54.
14 Helmcke F, Nanda NC, Hsuing MC, et al. ColorDoppler assessment of mitral regurgitation withorthogonal planes. Circulation 1987;75:175-83.
on Novem
ber 8, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.62.1.1 on 1 July 1989. D
ownloaded from


















