
CO ordinating R eferrals E ffectively CORE
21
COORDINATING REFERRALS EFFECTIVELY CORE Carol VanDeusen Lukas, EdD Boston University Safety Net ACTION Partnership Funded by AHRQ ACTION under contract HHSA2902006000012 TO6 September 27, 2010
-
Upload
maisie-mcknight -
Category
Documents
-
view
22 -
download
0
description
CO ordinating R eferrals E ffectively CORE. Carol VanDeusen Lukas, EdD Boston University Safety Net ACTION Partnership Funded by AHRQ ACTION under contract HHSA2902006000012 TO6 September 27, 2010. CORE team. BUSPH/BMC central team: Carol VanDeusen Lukas, EdD , BUSPH, PI - PowerPoint PPT Presentation
Transcript of CO ordinating R eferrals E ffectively CORE
COORDINATING REFERRALS EFFECTIVELY CORE
Carol VanDeusen Lukas, EdD
Boston University Safety Net ACTION Partnership
Funded by AHRQ ACTION under contract HHSA2902006000012 TO6
September 27, 2010
2
CORE teamBUSPH/BMC central team:
Carol VanDeusen Lukas, EdD, BUSPH, PIMari-Lynn Drainoni, PhD, BUSPH, co-PICharles Williams, MD, BMC Family Medicine, clinical redesign leadAndrea Niederhauser, MPH, BUSPH, project manager
Clinical redesign team members:Christine Odell, MD, BMC Ambulatory Care CenterJoseph Peppe, MD, South Boston Community Health CenterStephen Tringale, MD, Codman Square Health CenterRonald Iverson, MD, BMC Department of Obstetrics and
GynecologyFrancis Farraye, MD, BMC Department of Gastroenterology
AHRQ task order officersClaire Weschler, MSEd, CHESMary Barton, MD, MPP
3
Project aim: To improve referral processes between Primary & Specialty care
AHRQ-sponsored ACTION task orderUsing SUTTP principlesFive clinical sites
Two specialty clinics: Obstetrics and Gynecology (OB/GYN) Gastroenterology (GI)
Three family medicine primary care sites: Codman Square Health Center South Boston Community Health Center BMC Family Medicine Ambulatory Care Clinic (ACC)

4
Clinical redesign process
Regular meetings with clinical redesign team to conduct the work of redesign MDs + with periodic participation of senior referral staff
Meetings early in process with providers & with referral staff in each site for input
Periodic meetings to brief health center clinical leaders + HealthNet + BMC clinical leaders/administrators
5
Why redesign?Current referral system fragmented; varies among &
between primary care sites & specialties
Patients often unclear about reason for referral, how to make appointment, what to do after seeing specialist
Specialists do not consistently receive clear reason for the referral or adequate information on tests already done
Primary care physicians do not receive information about outcome of referral visit
Referral staff cope with multiple discordant processes & lost information

6
Intended benefits
For patients – clearer instructions & improved timeliness
For primary care providers & specialists – consistent, complete information from the other & clear outline of follow-up care plans
For referral staff – a standard method of processing referrals & clear outline of handling no-show appointments
For all parties – feedback on how the system is working for ongoing process improvement
7
Redesigned system: primary care standard elements
Patient contact number
PCP name
PCP pager
Appointment needed by date
Diagnosis
Reason for referral/ question
Labs included
Patient handout printed
8
Redesigned system: specialist standard elements
Referral receipt & provider acknowledged
Diagnosis provided, question answered
Follow-up plans indicated for:PatientSpecialistPCP
Note signed by specialist within 2 weeks & available in electronic records in PCP office
9
Redesigned system: building it into practice
CORE standard elements embedded in:Referral form from PCP to specialistLetter from PCP to patient Consult report from specialist to PCP
Service agreement among participating practices
CORE user toolsCORE summary sheetReferral guidelines Desk guide
10
Developing the implementation process
Work to fit with existing structures & systems
Clinical redesign team members – the clinicians in the participating sites – Help design the implementation processPlay key roles in carrying it out
Clinical redesign team lead has ongoing relationships with sites and with organizational leaders
11
Implementation process with users
Introduce new system at regular provider meetingsClinical redesign team members are local
implementation leadsWritten materials to support presentations
Review with administrative & referral staff
Make adjustments based on feedback Initial meetings and follow-up conversationsClinical redesign lead makes technical changes
Provide feedback after two-month trial implementation
12
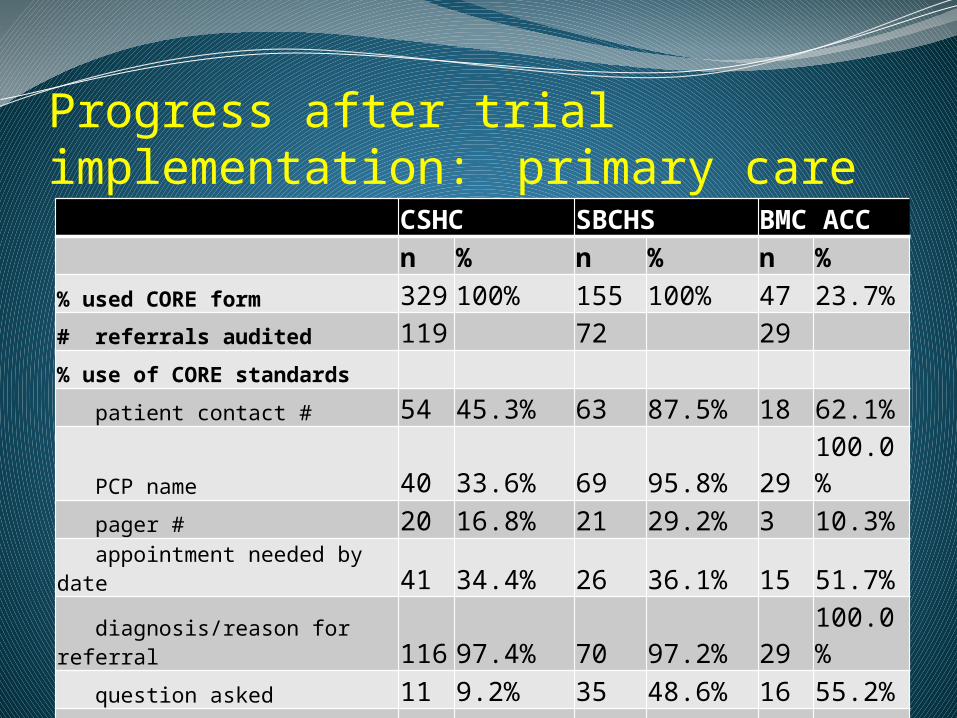
Progress after trial implementation: primary care CSHC SBCHS BMC ACC
n % n % n %
% used CORE form 329 100% 155 100% 47 23.7%# referrals audited 119 72 29
% use of CORE standards
patient contact # 54 45.3% 63 87.5% 18 62.1%
PCP name 40 33.6% 69 95.8% 29 100.0%
pager # 20 16.8% 21 29.2% 3 10.3%
appointment needed by date 41 34.4% 26 36.1% 15 51.7%
diagnosis/reason for referral 116 97.4% 70 97.2% 29 100.0%
question asked 11 9.2% 35 48.6% 16 55.2%
labs included 8 6.7% 0 0.0% NA NA patient handout printed 7 5.8% 3 4.2% 0 0.0%

13
Progress after trial implementation: specialty care OB/GYN GI
n % n %# reports audited 15 10 % CORE table completed 2 13% 3 30%% use of CORE standards
referral receipt acknowledged 8 53% 8 80% referring provider acknowledged 7 47% 10 100% diagnosis provided 14 93% 10 100% question answered 1 25% 4 100% care plan stated 15 100% 10 100% patient follow-up plan indicated 7 47% 7 70% PCP follow-up plan indicated 1 7% 3 30% specialist follow-up plan indicated 5 33% 5 50% note signed by specialist within 2 weeks 14 93% 10 100% note available in logician at health center 2 13% 0 0%
14
Implementation challenges: ….a work in progress
Influence of electronic medical records Overlapping development & implementation of e-
ReferralsWorking in larger hospital system
Difficult organizational environment
Provider resistance
15
Overlapping development & implementation with e-Referrals
Some success in building CORE changes into e-Referrals system
But, CORE implementation challenged by:Confusion at front-line between CORE & e-ReferralsE-Referrals roll out problems delay CORESome desired CORE changes could not be
accommodatedMonitoring reports generated by e-Referrals limited

16
Working in a larger hospital system
ACC clinic records part of larger hospital system
Limits to possible EMR changes in ACC because all providers across hospital use same system
CORE cannot simply replace forms CORE not default, have to select from menu
CORE referral form difficult because of limited text box capacity
17
Difficult organizational environment
New BMC CEO
Massachusetts health reform changes state financing at great loss to BMC
Several reductions in force in course of project
Restructuring in BMC ACC
High stress levels from hiring freeze, diminished service capacity, leadership changes

18
Provider resistance
In addition to previous challenges …
Providers hard to get together
Hard to convince of mutual benefits of new system
Chose path of least resistanceOn PCP side, patient letter not automatic

19
Role of project team in implementation
Central project team:Facilitated process , audited data, provided toolsMet regularly with clinical redesign leads to
troubleshootAfter two months, full team met to address
ambiguities, clarify some elements, remove others
Clinical redesign leader provided TA, modified systems directly working closely with sites
Clinical redesign leads provided feedback to their colleagues supported by audit data, crib sheet of why each element important & talking points
20
Continuing steps
Feedback to providers and referral staff
Feedback from providers and referral staff
Brief clinical and administrative leaders
Develop system for ongoing monitoring

21
On reflection…
Clinical redesign team membership
Life goes on in the organizations
Iteration, adaptation and continued discovery


















