Engage 2013 - National Co-ordinating Centre for Public Engagement
Upload
the-kings-fundCategory
view
303download
0description

How can we co-ordinate care from the information perspective
Experience from Carmarthenshire Chronic Conditions Demonstrator, Wales
Leo LewisSenior Fellow
International Foundation for Integrated Care

Health and social care has tended to create a series of simple,
disconnected, linear systems each designed to maximise one goal…

…and yet we have the knowledge, technology and imperative to formulate a sustainable way of delivering services rather than pursuing approaches that
simply mitigate negative impacts.

Building the CCM Model
Predictive Risk Tool
Telehealth and Telecare
Generic CCM support worker
Generic Care Pathway
Core MDT CCM Teams
Locality GP
Clusters
Care Co-ordinator
CCM Model – population based c50,000

Ecosystems are complex, interconnected and interdependent and designed towards an optimised
overall system

From information to understanding

CCM model and framework: role of care co-ordination
• Identify, plan and co-ordinate services to meet needs at each of the model’s four levels
• Liaise with patients, carers and service providers from private, voluntary, statutory and independent agencies
• Monitor patient progress and service delivery across primary, secondary, community and social care
• Co-ordinate primary care collaborative networks and networked services
• Advise on the commissioning of chronic conditions services

Confusion!
Views on the Care Co-ordinator role:• The person who took the lead in ensuring the Unified Assessment process was implemented for service users – either health or social services• Case Manager• Care Management• Community Chronic Disease Management Specialist Nurse

Clarification
Analysis of Skills for Health competencies for care co-ordination, care management and case management:
• 154 competencies delineated into three functional areas:– Strategic co-ordination and planning at a population level– Clinical/social care co-ordination focused on delivery of
services to individuals– Data and information competencies to support other
roles

Care Co-ordinator became
Care Services Planning Co-ordinator

Based on mid year estimates 2008 population growth & 2008/09 QoF as a % of the total registered population 2009
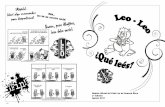
Planning: chronic condition prevalence
Projected Over 75 years QoF Events by disease 2009 to 2014 & 2019Towy Taf Locality
622
408
2823
254
1110 13
69
281
252 52
1 742
39
339
65
628 689
503
49369
5
456
3155
284
1241 15
30
314
282 58
2 829
44
379
73
702 770
562
55181
2
533
3687
332
1450
1788
367
329
680 96
9
51
443
85
820 900
657
643
0
500
1000
1500
2000
2500
3000
3500
4000
AF
Asth
ma BP
Canc
er CHD
CKD
COPD
Dem
entia
Depr
essio
n(d
iagno
sis) DM
Epile
psy HF M
H
Obe
sity
Stro
ke/T
IA
Thyr
oid
Popu
lation
>75
/ 10
QoF Disease area
Num
bers
of p
atie
nts 2009Evts>75
2014 Evts>75
2019 Evts>75

Planning and co-ordination: service utilisation
Emergency medical admissionsEMAs by Chronic Disease; Carmarthenshire Residents
0
100
200
300
400
500
600
700
800
900
COPD HF Diabetes All Type 1 Type 2 Other Diabetes
Condition
Nu
mb
er Calendar Year 2004
Calendar Year 2005
FY 06/07
FY 07/08

Planning – population and individual: predictive risk tool

Locality workforce profile

Individual care co-ordination: care plan

Planning and care delivery: health and social care directory of services

Information to support others: multi-disciplinary team meetings

Planning and delivery: chronic conditions generic care pathway

Chronic conditions – average length of stay:
measuring achievement
10
9
8
7
6
Month
Da
ys
_X=6.817
UCL=7.446
LCL=6.188
1
6
551
Rolling 12 Months' Average Length of StayCOPD Emergency Admissions
I Chart of Carmarthenshire by Month
5.75
5.50
5.25
5.00
4.75
4.50
Month
Da
ys
_X=4.813
UCL=4.971
LCL=4.656
Rolling 12 Months' Average Length of StayCHD Emergency Admissions
I Chart of Carmarthenshire by Month
Source: HSW Web Indicators SaFF 10
(Target 5.7 days) (Target 5.7 days)

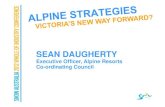
From information to understanding:our integrated community services care model

Care Services Directory Menu
Carmarthenshire Community Services Care ModelIdentify Cases Initiate Care Process Care Delivery and ReviewCare Assessment and Planning
Information Point for Citizen, Carer, and Professional
Single Point of Access
24/7Response
Unplanned Referral
Initial Referral
Generate Intervention
Requests
Diagnostic Intervention
Assess
Planned Community Services Intervention
Urgent Community Services Intervention
Review and Assess
Case Finding
Self Referral
Allocate Key Worker
Enter Referral
Unplanned Community Services Intervention
Unplanned Intervention – (not CS)
Re-
allo
cate
Prism and PARR++
GP Registers
Case Lists
Activity Reports
Assessment & Prioritise
Update H&SC
Records
Update H&SC
Records
Update H&SC
Records
Escalate to Community MDT Team Escalate
Main CCM Delivery Providers include:Social Care, District Nursing, Canllaw, DRT, CDM, General Practices, Out of Hours, Ambulance Trust, Voluntary Sector, Independent Sector, ART , TC/TH
Integrated Health and Social Care Register
Discharge
CommunityMDT Team
Update H&SC
Records
Produce Care Plan
Planned Intervention – (Not CS)
Normal
Unplanned
Info ResourceNormal PathUnexpected Path

Integrated, comprehensive solution that addresses multiple challenges simultaneously and coherently.

Rhayader Home Support Service

You never change things by fighting the existing reality. To change something, build a new
model that makes the existing model obsolete.
Michael Pawlyn 2013