


Clinical Trial Designs for RCTs focussing on the …...run-in phase, but substantially reduced...
29
Clinical Trial Designs for RCTs focussing on the Treatment of Agitation in people with Alzheimer’s disease Professor Clive Ballard Dr Byron Creese University of Exeter, UK
Transcript of Clinical Trial Designs for RCTs focussing on the …...run-in phase, but substantially reduced...
Clinical Trial Designs for RCTs focussing on the Treatment of
Agitation in people with Alzheimer’s disease
Professor Clive BallardDr Byron Creese
University of Exeter, UK

Penryn
ESI
Guardian guide for 2018: Top 5 UK medical school
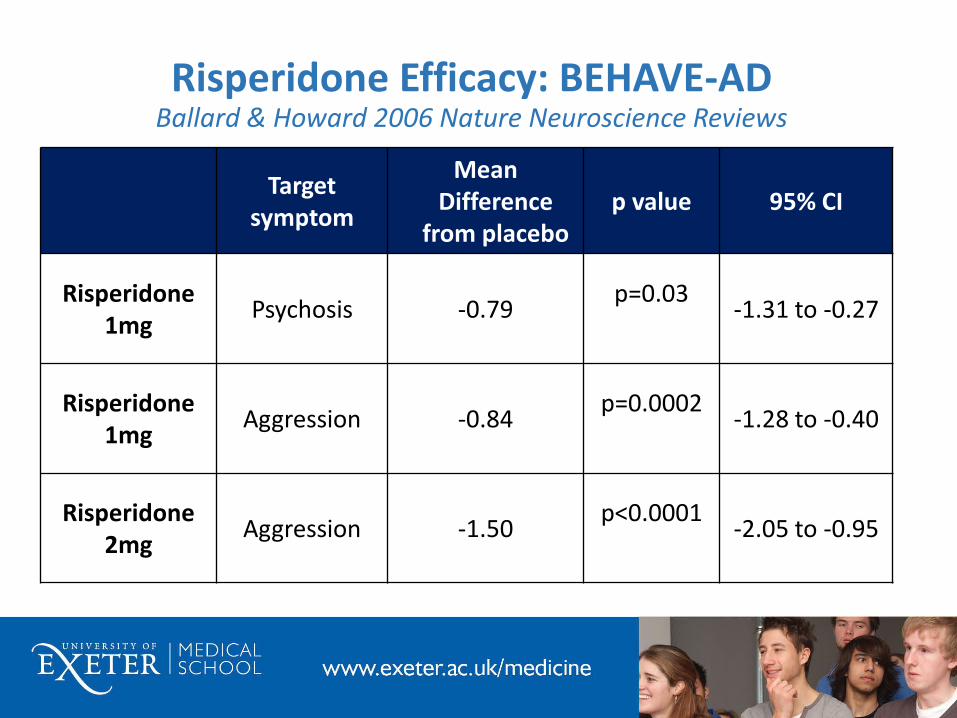
Risperidone Efficacy: BEHAVE-ADBallard & Howard 2006 Nature Neuroscience Reviews
Targetsymptom
Mean Difference
from placebop value 95% CI
Risperidone1mg
Psychosis -0.79p=0.03
-1.31 to -0.27
Risperidone1mg
Aggression -0.84p=0.0002
-1.28 to -0.40
Risperidone2mg
Aggression -1.50p<0.0001
-2.05 to -0.95

STAR TRIAL: Zhong et al 2007
Quetpiapine200mg (N=114)
Quetiapine 100mg (N=120)
Placebo (N=92)
Evaluation
PANSS-EC -5.7 (0.9) -4.9 (0.8) -3.9 (0.9) NS
NPI (total) -9.7 (2.2) -8.9 (2.1) -8.2 (2.4) NS
NPI (agitation)
-1.1 (0.5) -0.9 (0.5) -1.2 (0.5) NS
NPI (psychosis)
-2.5 (0.9) -1.8 (0.8) -2.5 (0.9) NS
CGIC 3.0 (0.2) 3.2 (0.2) 3.6 (0.2) NS

Major Adverse Outcomes with antipsychotics over 6-12 weeks
(FDA, Schneider et al 2005,Ballard et al 2009)
• Parkinsonism
• Sedation
• Gait disturbance
• Increased respiratory infections
• Oedema
• Accelerated cognitive decline (2-4 fold)
• Stroke (>3 fold)
• Other thrombo-embolic events (up to 80%)
• Mortality (1.5-1.7 fold)

Possible Interpretations
• Therapies Not good enough• Small effect sizes
• Targets unclear
• Very heterogenous study populations
• Challenges with trial design• Heterogenous trial populations
• Low entry thresholds
• Short duration
• No non pharmacological interventions –doesn’t follow best practice
• How rigorously have underlying medical causes and pain been excluded
• High placebo response
• Difficult to interpret major adverse events without a meta-analysis

Longer duration

Change from Baseline to 6 months DART AD Ballard et al PLOS Medicine 2008

DART AD: Differential Survival Ballard et al Lancet Neurology 2009
0%
10%
20%
30%
40%
50%
60%
70%
80%
Number of months
Differences in the survival rates in the DART-AD trial
Survival rate on placebo
Survival rate on a antipsychotic
Survival rate on placebo 71% 59% 53%
Survival rate on a antipsychotic 46% 30% 26%
24 36 42
The dementia antipsychotic withdrawal trial (DART-AD): long-term follow-up of a randomised placebo-controlled trial. www.thelancet.com/neurology.09 Jan 2009
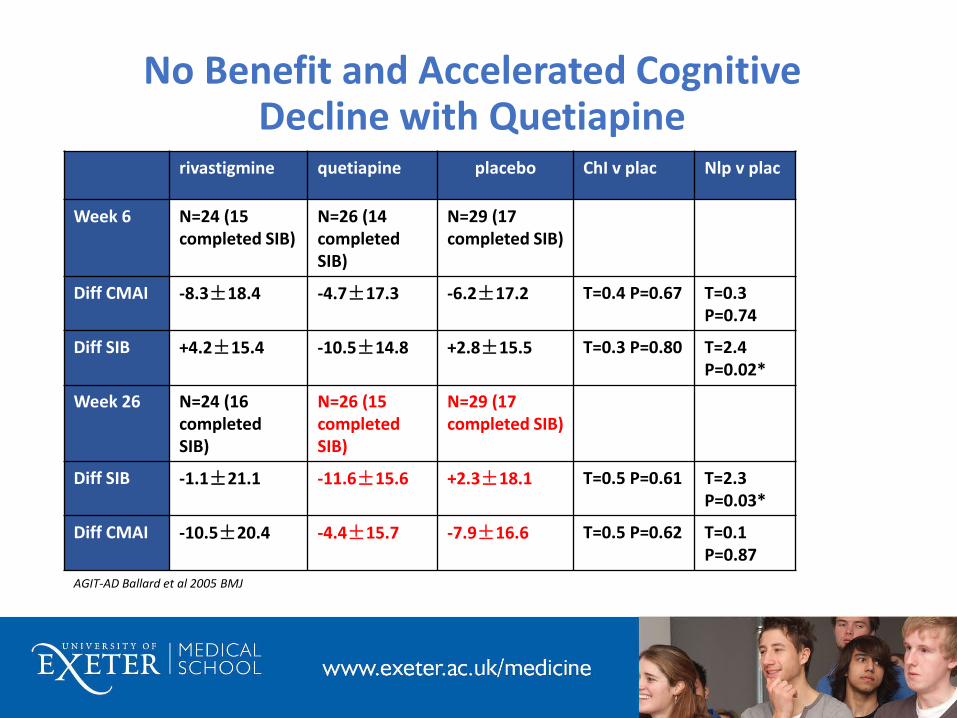
No Benefit and Accelerated Cognitive Decline with Quetiapine
rivastigmine quetiapine placebo ChI v plac Nlp v plac
Week 6 N=24 (15 completed SIB)
N=26 (14 completed SIB)
N=29 (17 completed SIB)
Diff CMAI -8.3±18.4 -4.7±17.3 -6.2±17.2 T=0.4 P=0.67 T=0.3 P=0.74
Diff SIB +4.2±15.4 -10.5±14.8 +2.8±15.5 T=0.3 P=0.80 T=2.4 P=0.02*
Week 26 N=24 (16 completed SIB)
N=26 (15 completed SIB)
N=29 (17 completed SIB)
Diff SIB -1.1±21.1 -11.6±15.6 +2.3±18.1 T=0.5 P=0.61 T=2.3 P=0.03*
Diff CMAI -10.5±20.4 -4.4±15.7 -7.9±16.6 T=0.5 P=0.62 T=0.1 P=0.87
AGIT-AD Ballard et al 2005 BMJ
Novel Statistical Approaches

Dextromethorphan/Quinidine (DM/Q) JAMA 2015
• 220 patient randomized to Dextromethorphan/Quinidine (DM/Q) orplacebo in 10 week trial
• Complicated 3:4 randomization design with re-randomization of placebonon-responders after 5 weeks
• 88% completed trial
• Significant benefits in agitation/aggression and CGIC, with benefits evidentfrom week 1
• Falls and diarrhea were the main emergent adverse events (both <10%)

Non-Pharmacological Therapy

WHELD: Key Results Ballard et al Am J psychiatry 2016
• AR significantly reduced antipsychotic use by 50% (OR 0.17, 95% CI 0.05to 0.60, p=0.006).
• AR and SI significantly reduced mortality (OR=0.36, 95% CI 0.23 to 0.57,p<0.001)
• Benefits in mortality were achieved without a worsening ofneuropsychiatric symptoms in people receiving AR and SI (-0.44, CI -4.39 to 3.52, p=0.82)
• EX significantly improved depression (-4.74, CI 0.76 to 8.72) andneuropsychiatric symptoms (-4.01, 95% CI -7.91 to -0.10, p=0.045).
• SI significantly improved quality of life (6.04, 95% CI 0.24 to 11.84,p=0.042)
• Combination of both SI and AR (p<0.04) and EX and AR (P<0.02) alsosignificantly improved apathy

Brief Psychosocial Therapy (BPST©) in clinical trials
• Previous clinical trials of psychosis and behavioural symptoms in Alzheimer’s Disease have experienced problems with high placebo response
• It is important to make sure a new drug is being tested in people who genuinely need it
• BPST© is designed to mirror best practice guidelines and reduce the placebo response by identifying people who improve with a non-drug approach
• Only people who do not improve following BPST© progress to pharmacological treatment
• In 3 previous trials of psychosis or agitation, has excluded 25% of people in run-in phase, but substantially reduced placebo response -with significant benefits compared to placebo in 2 of the trials (Howard et al 2007, Ballard et al 2009, Cummings et al 2014, Ballard et al 2017)
• Currently being used in 3 further ongoing clinical trials
How is the BPST© delivered?
• Two - four week intervention to enable enjoyable activities between a person with dementia and their caregiver for 10-15 minute a day
• Therapist works with a caregiver (care assistant or family member) over four sessions: • Training (Day 1): in person (30-45 minutes)• Follow-up (regular x 2*): by telephone (15 minutes)• Baseline (Day 14-28): in person (15 minutes)
• Caregiver delivers the BPST© to the patient • Daily: 10-30 min• Completion of a simple diary• Follow-up calls support and reinforce the caregiver
*Schedules for each person with depend on screening period:Four weeks = weekly follow-upTwo weeks = Follow up every 4 days

Discontinuation Design

Clear Criteria

Cummings et al 2017: IPA criteria for agitation
• Patients must meet criteria for cognitive impairment and exhibit behaviours such as excessive activity and verbal or physical aggression severe enough to produce disability in social, or interpersonal functions, or activities of daily living. These symptoms should not be attributable to other psychiatric or medical disorders, suboptimal environment, or drug effects. Future validation studies are needed to confirm or revise the definition. This definition will facilitate clinical trials and other types of clinical and translational research. New IPA Criteria for Agitation in Cognitive Impairment. Available from: https://www.researchgate.net/publication/308775448_New_IPA_Criteria_for_Agitation_in_Cognitive_Impairment [

Modified CGIC

CitAD: JAMA 2014
• OBJECTIVE: To evaluate the efficacy of citalopram for agitation in patients with Alzheimer disease.
• DESIGN, SETTING, AND PARTICIPANTS: CitAD was a randomized, placebo-controlled, double-blind, parallel group trial with 186 patients with probable AD and clinically significant agitation
• INTERVENTIONS: Patients were randomized to receive a psychosocial intervention plus either citalopram (n = 94) or placebo (n = 92) for 9 weeks. Dosage began at 10 mg per day with planned titration to 30 mg per day over 3 weeks based on response and tolerability.

CitAD: Results
MAIN OUTCOMES AND MEASURES:
• The NBRS-A estimated treatment difference (citalopram minus placebo)was -0.93 (95% CI, -1.80 to -0.06), P = .04.
• CGIC showed 40% of citalopram participants having moderate or markedimprovement from baseline compared with 26% of placebo recipients,with estimated treatment effect (odds ratio [OR] of being at or betterthan a given CGIC category) of 2.13 (95% CI, 1.23-3.69), P = .01 (Cohen’sd standardized effect size 0.36).
• Participants who received citalopram showed significant improvementon the CMAI, total NPI, and caregiver distress scores but not on the NPIagitation subscale,
• Worsening of cognition (-1.05 points; 95% CI, -1.97 to -0.13; P = .03) andQT interval prolongation (18.1 ms; 95% CI, 6.1-30.1; P = .01) were seen inthe citalopram group.
Central Rating

-020 Study: Pimavanserin Demonstrated Highly Significant Antipsychotic Efficacy (Lancet Feb 2014)
26
**
*
SAPS-PD (primary endpoint)(ITT, N=185; change from baseline)
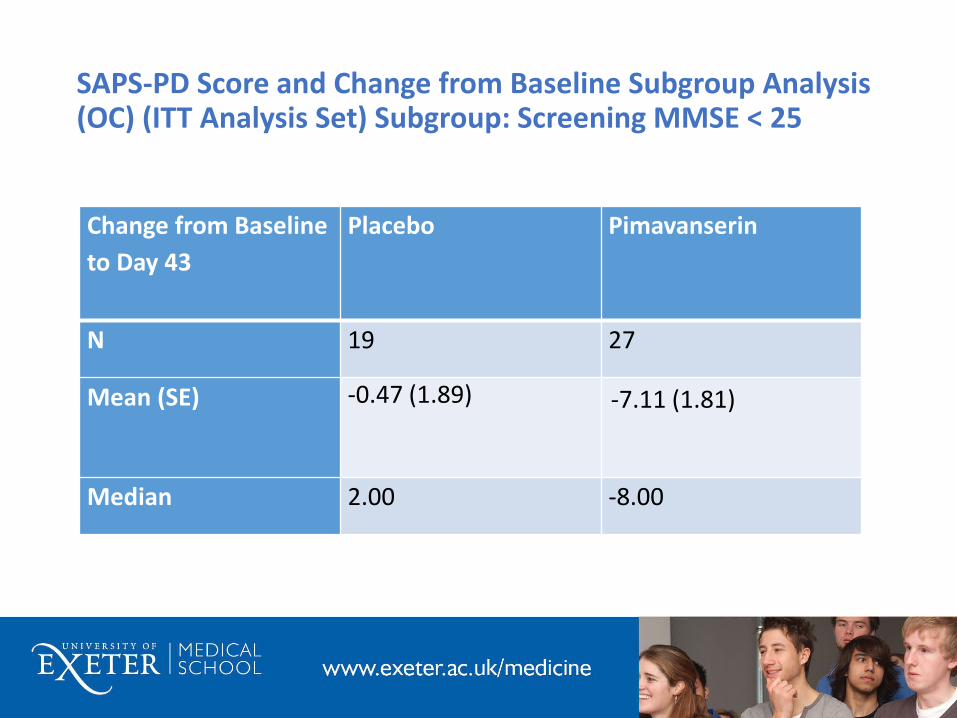
SAPS-PD Score and Change from Baseline Subgroup Analysis (OC) (ITT Analysis Set) Subgroup: Screening MMSE < 25
Change from Baseline
to Day 43
Placebo Pimavanserin
N 19 27
Mean (SE) -0.47 (1.89) -7.11 (1.81)
Median 2.00 -8.00

Improved trial design
• Clearer definition of agitation (and sub-syndromes)
• Non-pharmacological interventions to reduce placebo response
• Central rating of primary outcome to reduce impact of inter-rater variability
• New CGIC for neuropsychiatric symptoms
• Novel statistical approaches
• Discontinuation element to establish continued benefit
• Higher threshold for study entry
• Longer duration of trial (particularly for adverse events)
• Better targets (syndrome definition, molecular targets)


















