Clinical Manifestations of Unconjugated Hyperbilirubinemia in Term and Late Preterm Infants
18
1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 1/18 Official reprint from UpToDate www.uptodate.com ©2016 UpToDate Authors Ronald J Wong, BA Vinod K Bhutani, MD, FAAP Section Editor Steven A Abrams, MD Deputy Editor Melanie S Kim, MD Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Nov 2015. | This topic last updated: Dec 14, 2015. INTRODUCTION — Almost all newborn infants develop a total serum or plasma bilirubin (TB) value greater than 1 mg/dL (17.1 micromol/L), which is the upper limit of normal for adults. As TB increases, it causes neonatal jaundice, the yellowish discoloration of the skin and/or conjunctiva caused by bilirubin deposition in half of all newborn infants. Neonates with severe hyperbilirubinemia (defined as a TB >25 mg/dL [428 micromol/L]) are at risk for bilirubininduced neurologic dysfunction (BIND), which occurs when bilirubin crosses the bloodbrain barrier and binds to brain tissue. The clinical manifestations of neonatal unconjugated hyperbilirubinemia including risk factors for severe hyperbilirubinemia in term and late preterm infants are reviewed here. The pathogenesis, etiology, evaluation, prevention and treatment of this disorder are discussed separately. (See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn" and "Evaluation of unconjugated hyperbilirubinemia in term and late preterm infants" and "Treatment of unconjugated hyperbilirubinemia in term and late preterm infants" .) DEFINITIONS OVERVIEW — The administration of Rh(D) immunoglobulin to Rhnegative mothers in the late 1960s dramatically decreased the incidence of neonatal Rh isoimmune hemolytic disease. Thus, the risk of kernicterus was reduced from its peak in the 1950s through the 1970s. Nevertheless, isolated cases of kernicterus, a preventable condition, continue to be reported [2,3 ]. (See 'Epidemiology' below.) Since the association between hyperbilirubinemia and kernicterus was first identified in infants with erythroblastosis fetalis more than 50 years ago [46 ], there has been a debate on what degree and duration of hyperbilirubinemia causes bilirubininduced neurologic dysfunction (BIND). Additional factors such as the rate of rise of total serum or plasma bilirubin (TB), the proportion of unbound (or "free") bilirubin, and the permeability of the bloodbrain barrier affect the potential for neurotoxicity. (See 'Neurologic manifestations' below.) Limited data based upon case reports suggest that kernicterus is unlikely to occur in healthy term infants with TB ≥20 mg/dL (342 micromol/L) [2,7 ]. This is illustrated in a report of 61 cases of readmitted patients (before seven days of age) that were voluntarily reported to the Pilot Kernicterus Registry [2 ]. The median TB on readmission was 39 mg/dL (667 micromol/L), range 21.5 to 50 mg/dL (368 to 855 micromol/L) [2 ]. A review of the literature in 2002 of 123 cases reported similar results; more than 90 percent of infants had TB >25 mg/dL (428 micromol/L). Based upon these data, the management of unconjugated hyperbilirubinemia in term and late preterm infants is ® ® Neonatal hyperbilirubinemia in infants ≥35 weeks gestational age (GA) is defined as total serum or plasma bilirubin (TB) >95 percentile on the hourspecific Bhutani nomogram ( figure 1 )[1 ]. ● th Severe neonatal hyperbilirubinemia is defined as a TB >25 mg/dL (428 micromol/L). It is associated with an increased risk for bilirubininduced neurologic dysfunction (BIND), which occurs when bilirubin crosses the bloodbrain barrier and binds to brain tissue. (See 'Neurologic manifestations' below.) ● Acute bilirubin encephalopathy (ABE) is used to describe the acute manifestations of BIND. (See 'Acute bilirubin encephalopathy' below.) ● Kernicterus is used to describe the chronic and permanent sequelae of BIND. (See 'Kernicterus' below.) ●
-
Upload
cristina-fernandez-valencia -
Category
Documents
-
view
219 -
download
1
description
v
Transcript of Clinical Manifestations of Unconjugated Hyperbilirubinemia in Term and Late Preterm Infants

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 1/18
Official reprint from UpToDate www.uptodate.com ©2016 UpToDate
AuthorsRonald J Wong, BAVinod K Bhutani, MD, FAAP
Section EditorSteven A Abrams, MD
Deputy EditorMelanie S Kim, MD
Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Nov 2015. | This topic last updated: Dec 14, 2015.
INTRODUCTION — Almost all newborn infants develop a total serum or plasma bilirubin (TB) value greater than 1mg/dL (17.1 micromol/L), which is the upper limit of normal for adults. As TB increases, it causes neonataljaundice, the yellowish discoloration of the skin and/or conjunctiva caused by bilirubin deposition in half of allnewborn infants. Neonates with severe hyperbilirubinemia (defined as a TB >25 mg/dL [428 micromol/L]) are atrisk for bilirubininduced neurologic dysfunction (BIND), which occurs when bilirubin crosses the bloodbrain barrierand binds to brain tissue.
The clinical manifestations of neonatal unconjugated hyperbilirubinemia including risk factors for severehyperbilirubinemia in term and late preterm infants are reviewed here. The pathogenesis, etiology, evaluation,prevention and treatment of this disorder are discussed separately. (See "Pathogenesis and etiology ofunconjugated hyperbilirubinemia in the newborn" and "Evaluation of unconjugated hyperbilirubinemia in term andlate preterm infants" and "Treatment of unconjugated hyperbilirubinemia in term and late preterm infants".)
DEFINITIONS
OVERVIEW — The administration of Rh(D) immunoglobulin to Rhnegative mothers in the late 1960s dramaticallydecreased the incidence of neonatal Rh isoimmune hemolytic disease. Thus, the risk of kernicterus was reducedfrom its peak in the 1950s through the 1970s. Nevertheless, isolated cases of kernicterus, a preventable condition,continue to be reported [2,3]. (See 'Epidemiology' below.)
Since the association between hyperbilirubinemia and kernicterus was first identified in infants witherythroblastosis fetalis more than 50 years ago [46], there has been a debate on what degree and duration ofhyperbilirubinemia causes bilirubininduced neurologic dysfunction (BIND). Additional factors such as the rate ofrise of total serum or plasma bilirubin (TB), the proportion of unbound (or "free") bilirubin, and the permeability ofthe bloodbrain barrier affect the potential for neurotoxicity. (See 'Neurologic manifestations' below.)
Limited data based upon case reports suggest that kernicterus is unlikely to occur in healthy term infants with TB≥20 mg/dL (342 micromol/L) [2,7]. This is illustrated in a report of 61 cases of readmitted patients (before sevendays of age) that were voluntarily reported to the Pilot Kernicterus Registry [2]. The median TB on readmissionwas 39 mg/dL (667 micromol/L), range 21.5 to 50 mg/dL (368 to 855 micromol/L) [2]. A review of the literature in2002 of 123 cases reported similar results; more than 90 percent of infants had TB >25 mg/dL (428 micromol/L).
Based upon these data, the management of unconjugated hyperbilirubinemia in term and late preterm infants is
®®
Neonatal hyperbilirubinemia in infants ≥35 weeks gestational age (GA) is defined as total serum or plasmabilirubin (TB) >95 percentile on the hourspecific Bhutani nomogram (figure 1) [1].
th
Severe neonatal hyperbilirubinemia is defined as a TB >25 mg/dL (428 micromol/L). It is associated with anincreased risk for bilirubininduced neurologic dysfunction (BIND), which occurs when bilirubin crosses thebloodbrain barrier and binds to brain tissue. (See 'Neurologic manifestations' below.)
Acute bilirubin encephalopathy (ABE) is used to describe the acute manifestations of BIND. (See 'Acutebilirubin encephalopathy' below.)
Kernicterus is used to describe the chronic and permanent sequelae of BIND. (See 'Kernicterus' below.)

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 2/18
focused on two key elements:
(See "Evaluation of unconjugated hyperbilirubinemia in term and late preterm infants" and "Treatment ofunconjugated hyperbilirubinemia in term and late preterm infants".)
EPIDEMIOLOGY
Total serum/plasma bilirubin (TB) — In the neonate, TB values vary substantially among institutions because ofdifferences in racial composition, hemolytic conditions, or breastfeeding practices. (See "Evaluation ofunconjugated hyperbilirubinemia in term and late preterm infants", section on 'Epidemiology' and "Pathogenesisand etiology of unconjugated hyperbilirubinemia in the newborn", section on 'Neonatal jaundice'.)
These factors may contribute to the observed global variations in the incidence of hyperbilirubinemia (TB >20mg/dL [342 micromol/L]).
Prevention of hyperbilirubinemia, defined as TB >95 percentile for hoursofage on the Bhutani nomogram[8], by identifying atrisk infants and beginning preventative therapeutic interventions (eg, phototherapy) asneeded [3]
th
Reduction of TB in infants with severe hyperbilirubinemia
In studies of term or late preterm infants from a large Northern California health maintenance organization(HMO), the following incidences of severe hyperbilirubinemia at different TB values were reported from birthdata collected between 1995 and 1998 [9,10]:
TB >20 mg/dL (342 micromol/L): 2 percent [10]•
TB >25 mg/dL (428 micromol/L): 0.14 percent [10]•
TB >30 mg/dL (513 micromol/L): 0.01 percent [9]•
The risk of TB >20 mg/dL (342 micromol/L) was lower in infants born to mothers who selfreported as AfricanAmerican than in those who were Caucasian (0.9 versus 1.5 percent, relative risk [RR] 0.62, 95% CI 0.560.69) [11]. However, the risk of severe hyperbilirubinemia, defined as TB >30 mg/dL (513 micromol/L), washigher in AfricanAmerican infants (0.13 versus 0.03 percent, RR 4.2, 95% CI 1.3313.2).
In a later cohort of infants from the same HMO born between 1995 and 2011 (n = 525,409), 47 infants wereidentified with severe hyperbilirubinemia resulting in an incidence of 8.6 per 100,000 births [12]. The etiologywas not identified in 33 patients, and 10 of 25 patients tested for glucose6phosphate dehydrogenase(G6PD) activity were found to be deficient. Four patients had acute bilirubin encephalopathy (ABE). Thisincluded three infants with G6PD deficiency with TB levels >40 mg/dL (684 micromol/L), in whom cerebralpalsy (CP) and sensorineural hearing loss (SNHL) developed in two patients, and SNHL only in one patient.(See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn", section on 'Increasedproduction'.)
In a Danish populationbased study from 2000 to 2007, the incidence of "extreme" hyperbilirubinemia (definedas a TB ≥26.3 mg/dL or 450 micromol/L) was 0.045 percent of infants born at gestational age (GA) ≥35weeks [13]. Of the 224 identified infants with extreme hyperbilirubinemia, three had advanced bilirubinencephalopathy and a peak TB level greater than 35 mg/dL (599 micromol/L), which was due to hemolysiseither from ABO incompatibility or G6PD deficiency. All three patients developed kernicterus. Two otherinfants had moderate bilirubin encephalopathy and their neurologic condition normalized over four to fivedays. One of the patients with moderate disease had ABO incompatibility.
In a populationbased study from Nova Scotia, the incidence of severe hyperbilirubinemia (defined as a TB≥19 mg/dL or 325 micromol/L) was 0.6 percent of live births (348 of 61,238) at term or late preterm [14].Severe hyperbilirubinemia was associated with breastfeeding, older maternal age (>35 years of age),nulliparous, nonsmoking mother, GA <37 weeks, male gender, and respiratory distress syndrome.

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 3/18
The higher reported incidence in the United States compared with Western Europe and Nova Scotia may reflectthe greater number of infants born of mothers who are East Asian or African American.
Kernicterus — Kernicterus is the chronic and permanent neurologic sequelae of bilirubininduced neurologicdysfunction (BIND). Although there had been concerns that the incidence of kernicterus was rising, the risk ofkernicterus appears to be stable based on population studies.
This was illustrated by a study that used diagnosis codes from data collected by the California Department ofDevelopmental Services to identify patients with kernicterus born between 1988 and 1997, and death certificatedata from the National Center for Health Statistics to examine kernicterus mortality trends [16]. The followingfindings were noted:
Determining the incidence of kernicterus is confounded by absence of populationbased data, reports of selectpatients who are admitted at varying stages of ABE, and variable timeliness to intervention. Similar incidences ofkernicterus per 100,000 live births have been reported in the United States (0.44) as were reported in populationbased studies in Germany (0.63) and Denmark (0.40), but a higher rate was seen in Canada [1618]. In a reportthat used prospective data from the Canadian Paediatric Surveillance Program (CPSP) from 2007 to 2008, 20cases of kernicterus (eg, chronic bilirubin encephalopathy) were identified resulting in an incidence of 2.3 casesper 100,000 live births [18]. Causes of neonatal hyperbilirubinemia included alloimmune hemolytic disease due toABO incompatibility or other red blood cell antibodies (n = 7), G6PD deficiency (n = 5), and sepsis (n = 2). Fifteenpatients had an abnormal brain magnetic resonance imaging (MRI) study during the neonatal period. Of the 14patients with followup data, six patients had signs of neurologic impairment and/or developmental delay, fiveinfants had choreoathetoid CP, and three were reported as healthy.
It appears that the incidences of kernicterus and hyperbilirubinemia are decreasing.
RISK FACTORS — In the 2004 American Academy of Pediatrics (AAP) Practice Guideline, the following majorrisk factors for severe hyperbilirubinemia (table 1) and bilirubininduced neurologic dysfunction (BIND) wereidentified [1]:
In a prospective populationbased study in the United Kingdom and Ireland between 2003 and 2005, theincidence of "severe" hyperbilirubinemia (defined as a TB >30 mg/dL or 513 micromol/L) was 7 per 100,000live births [15]. The mean GA of the 108 identified infants was 38.2 weeks. Eighty percent of the patientswere breastfed, twothirds were male, and about half were from a minority ethnic background. Fourteeninfants developed ABE, including three infants who died.
Twentyfive cases with a strict diagnosis of kernicterus were identified over the 10year period resulting in anoverall incidence of 0.44 per 100,000 live births averaged per year when reported for the entire study period.The incidence of kernicterus was higher in boys than in girls (0.71 versus 0.30 per 100,000 live births peryear).
The death rate due to kernicterus was 0.28 deaths per one million live births, which remained stablethroughout the study period from 1979 to 2006.
In one study using select reporting of nationally representative hospital discharge data in the US, thehospitalization rate for newborns who were coded to have kernicterus by clinicians declined from 5.1 per100,000 term neonates (patients ≤30 days of age) in 1988 to 1.5 per 100,000 neonates in 1994 [19]. In thisreport, a case of kernicterus, when reported, was defined by a diagnosis code and evidence of treatment withphototherapy or exchange transfusion, and data from late preterm infants were not included. Asian infantshad a higher rate of hospitalization than other ethnic groups, as did preterm compared with term infants.
A report from a multihospital healthcare system in the United States showed a declining rate of infants withextreme hyperbilirubinemia, defined as TB between 25 and 29.9 mg/dL (428 and 513 micromol/L) from 2002to 2010 [20] (figure 2). No patient in this cohort developed kernicterus.

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 4/18
Minor risk factors included [1] (table 1):
The ability of the AAP major risk factors to predict hyperbilirubinemia was illustrated in a retrospective nestedcasecontrol study of a large cohort of 285,295 newborn infants born with a BW ≥2000 g at a GA ≥34 weeksbetween 1995 and 2004 [27]. In this study, 62 infants (0.4 percent) were identified with a TB ≥25 mg/dL (428micromol/L) from a cohort of 17,986 infants (6.3 percent) with a TB between 17 and 22.9 mg/dL (291 to 392micromol/L) at age ≥48 hours of life. Four randomly selected control cases within the identified cohort group werematched to the patients with TB ≥25 mg/dL (428 micromol/L). Lower GA, bruising, a family history of neonatalhyperbilirubinemia, a rapid rise of TB ≥6 mg/dL (103 micromol/L) per day, and exclusive breastfeeding wereassociated with a TB ≥25 mg/dL (428 micromol/L). In the nested control sample, inpatient phototherapy withineight hours of a qualifying TB was associated with a decreased risk for a TB ≥25 mg/dL (428 micromol/L).
A populationbased study using data from the Swedish Medical Birth Right Register of term infants (≥37 weeksGA) born from 1999 to 2012 identified the following as risk factors for severe hyperbilirubinemia: GA between 37and 38 weeks, failed or successful vacuum extraction, macrosomic infants, obese mother, and being small forgestational age (SGA) [28]. In this cohort, planned cesarean delivery was associated with a reduced risk ofhyperbilirubinemia. In this study, severe hyperbilirubinemia was defined as 20 mg/dL (342 micromol/L) before 2008and 20.6 mg/dL (352 micromol/L) from 2008 and after.
Predischarge total serum or plasma bilirubin (TB) or transcutaneous bilirubin (TcB) in a highrisk zone definedas >95 percentile for age (figure 1). The risk for severe hyperbilirubinemia and the threshold for interventionbased upon the hourspecific TB value may be determined using the newborn hyperbilirubinemia assessmentcalculator (calculator 1). (See "Evaluation of unconjugated hyperbilirubinemia in term and late preterminfants", section on 'Total serum or plasma bilirubin (TB)' and "Evaluation of unconjugated hyperbilirubinemiain term and late preterm infants", section on 'Transcutaneous bilirubin'.)
th
Jaundice within the first 24 hours of life [21].
Hemolytic disease due to isoimmunemediated hemolysis from blood group incompatibility or inherited redcell enzymatic deficiencies or membrane defects (eg, glucose6phosphate dehydrogenase [G6PD]deficiency). In addition, evidence of hemolysis is a major risk factor for severe hyperbilirubinemia (eg,elevated endtidal carbon monoxide [CO], corrected for inhaled CO or endtidal carbon monoxideconcentration [ETCOc] levels). (See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in thenewborn", section on 'Increased production' and "Evaluation of unconjugated hyperbilirubinemia in term andlate preterm infants", section on 'Endtidal carbon monoxide concentration'.)
Gestational age (GA) 35 to 36 weeks [22,23]. (See "Late preterm infants".)
Sibling who previously received phototherapy [23,24].
Cephalohematoma or significant bruising from birth trauma [22].
Exclusive breastfeeding, particularly if nursing is not going well and weight loss is excessive (>12 percent ofbirth weight [BW]) [22,23].
East Asian race. (See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn",section on 'Ethnic variation in conjugation ability'.)
TB in a high intermediate range (>75 and ≤95 percentile for ageinhours) th th
Jaundice observed before discharge [23]Macrosomic infant of a diabetic mother [25,26]PolycythemiaMale gender [22]Maternal age ≥25 years [23]
1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 5/18
Although inherited deficiencies in hepatic conjugating capacity (eg, CriglerNajjar or Gilbert syndromes) were notincluded in the AAP guideline or assessed in the Swedish study as risk factors, genetic predisposition may play amajor role in severe hyperbilirubinemia, especially in Gilbert syndrome, which affects 9 percent of the generalpopulation [29,30]. This may in part explain why family history is a predictive risk factor for hyperbilirubinemia. Theunderlying decrease in bilirubin clearance of infants with Gilbert syndrome in combination with other factor(s) thatincreases TB can result in severe hyperbilirubinemia [31]. As an example, breastfed infants with Gilbert syndromehave a three to fourfold increased risk for TB >20 mg/dL (342 micromol/L) compared with breastfed infants withoutGilbert syndrome [32]. (See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn",section on 'Gilbert syndrome'.)
An alternative simpler approach of using the infant's discharge TB level and GA has been reported to accuratelyassess an infant's risk of developing significant hyperbilirubinemia [33].
Factors associated with decreased risk of severe hyperbilirubinemia include [1] (table 1):
These risk factors are used to assess the likelihood of developing clinically significant hyperbilirubinemia. The riskassessment and the age of the infant at the time of discharge from the hospital are used to determine the timing ofappropriate followup (table 2). (See "Evaluation of unconjugated hyperbilirubinemia in term and late preterminfants", section on 'Risk assessment' and "Evaluation of unconjugated hyperbilirubinemia in term and late preterminfants", section on 'Followup'.)
Readmission — Risk for readmission for hyperbilirubinemia for term infants based on a large populationbasedAustralian study included [36]:
CLINICAL MANIFESTATIONS — The clinical manifestations of hyperbilirubinemia are due to bilirubin depositionin the skin (jaundice) and/or the brain (bilirubininduced neurologic dysfunction [BIND]).
Jaundice — Jaundice is the yellow color produced by the deposition of bilirubin in the skin and subcutaneoustissues. Although an important, and timehonored clinical sign, the presence of jaundice is not a reliable method toassess total serum or plasma bilirubin (TB) concentration or identify infants at risk for rapidly rising bilirubin,especially in those with dark skin [2,37,38]. The examination for jaundice should be performed with adequateambient light or under daylight fluorescent light. Pressing on the skin with a finger reduces local skin perfusion andfacilitates detection of jaundice (picture 1).
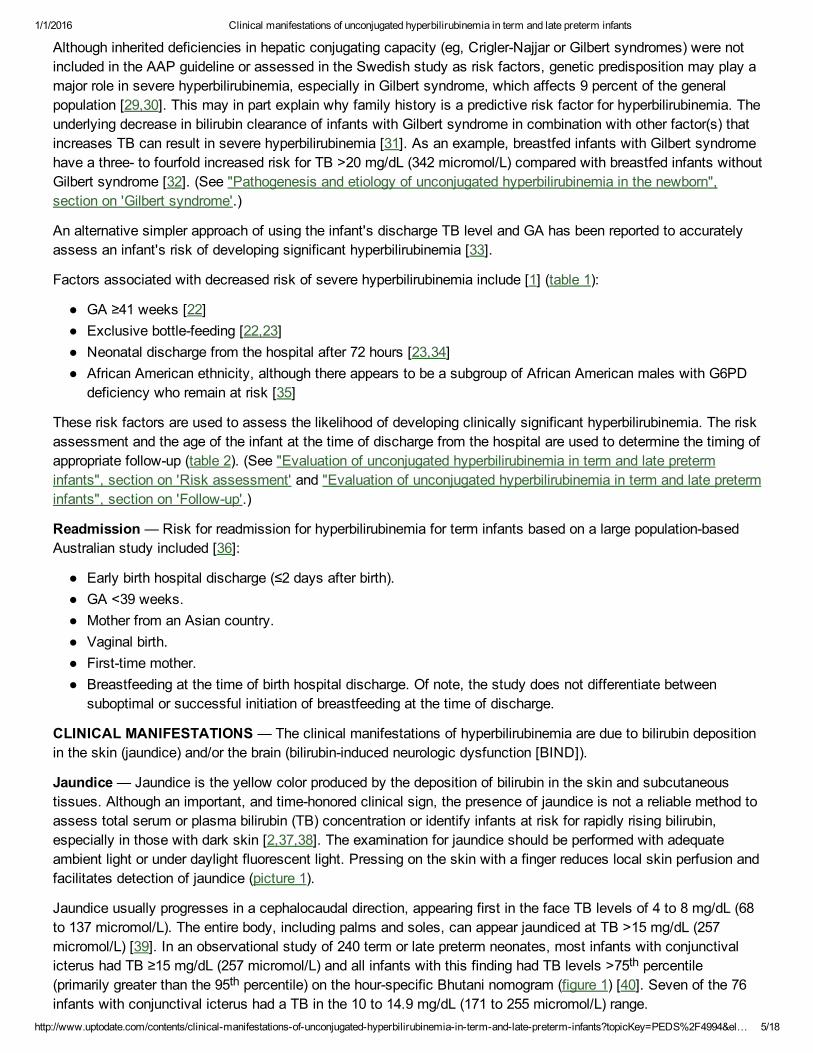
Jaundice usually progresses in a cephalocaudal direction, appearing first in the face TB levels of 4 to 8 mg/dL (68to 137 micromol/L). The entire body, including palms and soles, can appear jaundiced at TB >15 mg/dL (257micromol/L) [39]. In an observational study of 240 term or late preterm neonates, most infants with conjunctivalicterus had TB ≥15 mg/dL (257 micromol/L) and all infants with this finding had TB levels >75 percentile(primarily greater than the 95 percentile) on the hourspecific Bhutani nomogram (figure 1) [40]. Seven of the 76infants with conjunctival icterus had a TB in the 10 to 14.9 mg/dL (171 to 255 micromol/L) range.
GA ≥41 weeks [22]Exclusive bottlefeeding [22,23]Neonatal discharge from the hospital after 72 hours [23,34]African American ethnicity, although there appears to be a subgroup of African American males with G6PDdeficiency who remain at risk [35]
Early birth hospital discharge (≤2 days after birth).GA <39 weeks.Mother from an Asian country.Vaginal birth.Firsttime mother.Breastfeeding at the time of birth hospital discharge. Of note, the study does not differentiate betweensuboptimal or successful initiation of breastfeeding at the time of discharge.
thth

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 6/18
These results suggest that TB or transcutaneous bilirubin (TcB) levels should always be measured in an infantwith jaundice below the umbilicus or with conjunctival icterus. If there is uncertainty regarding the presence orextent of jaundice, a TB or TcB measurement should be performed. (See "Evaluation of unconjugatedhyperbilirubinemia in term and late preterm infants".)
Other findings on physical examination may suggest an increased risk for hyperbilirubinemia. These include pallor,enclosed hemorrhage (eg, cephalohematoma), bruising, and hepatosplenomegaly.
Neurologic manifestations — Bilirubin is a potential neurotoxin [4149]. Term and late preterm infants are at riskfor BIND when TB concentrations ≥25 mg/dL (428 micromol/L). In general, at this threshold, unconjugated bilirubin,which is not bound to albumin (also referred to as "free" or unbound bilirubin), can enter the brain and cause celldeath by apoptosis (programmed cell death) and/or necrosis [4749]. In vitro, animal cell culture studies suggestedthat lower levels of unconjugated bilirubin induce apoptosis and higher levels induce necrotic cell death [47]. Whichmechanism predominates in infants with severe unconjugated hyperbilirubinemia who develop BIND remainsuncertain [1]. BIND is a spectrum of subtle neurologic findings and sequelae [50], which can manifest as disordersin vision [51], hearing [52], gait [53], and speech, cognition, and language [54].
Acute bilirubin encephalopathy (ABE) may be reversible or result in permanent irreversible neurologic dysfunction(kernicterus). The brain regions most often affected include the basal ganglia and the brainstem nuclei foroculomotor and auditory function, accounting for the clinical features seen in infants with BIND [55].
Acute bilirubin encephalopathy — ABE typically progresses through three phases [55]:
In a report based on prospective data from the voluntary Canadian Paediatric Surveillance Program (CPSP), 32 of258 infants (12.4 percent) with severe hyperbilirubinemia (defined as a TB >24.8 mg/dL [424 micromol/L]) werediagnosed with ABE [56]. Twenty other infants had nonspecific neurologic findings that were not severe enough toconfidently make the diagnosis of ABE. Infants with ABE had higher peak TB levels than those without ABE (29.7versus 27.3 mg/dL [508 versus 467 micromol/L]). Infants with ABE who presented in the first 48 hours of life hadlower TB levels than those who presented after 48 hours. This study was unable to determine whether there was arelationship between ABE and the etiology of hyperbilirubinemia, as an underlying cause was determined in only41 percent of patients with ABE and 35 percent of patients without any neurologic abnormality.
In an observational study, 249 Egyptian neonates were selfreferred to a public hospital neonatal intensive careunit (NICU) following unknown duration of hyperbilirubinemia after delivery at outlying facilities over a 12monthperiod (January to December 2008). Characteristics of this atrisk infant cohort included: gestational age (GA) >34weeks, birth weight (BW) >2 kg, postnatal age <14 days, and admission TB ≥25 mg/dL (428 micromol/L). Ofthese, 44 (18 percent) were diagnosed with moderate or severe ABE, 55 (22 percent) with mild ABE, and theremaining infants were asymptomatic [57]. Although the median TB was lower in patients with no ABE symptoms(28.3 mg/dL [484 micromol/L]) and rose progressively for those with mild/moderate and severe ABE (32 to 33 and36.5 mg/dL, [547 to 564 and 624 micromol/L]), the range of TB values was similar in all three groups. Of the 26
In the early phase, the clinical signs may be subtle. The infant is sleepy but arousable, and when arousedhas mild to moderate hypotonia and a highpitched cry.
If there is no intervention, the intermediate phase evolves with progression and persistence ofhyperbilirubinemia. The infant can be febrile, lethargic with a poor suck, or irritable and jittery with a strongsuck. The cry can be shrill and the infant is difficult to console. Mild to moderate hypertonia develops,beginning with backward arching of the neck (retrocollis) and trunk (opisthotonos) with stimulation. Anemergent exchange transfusion at this stage might prevent permanent BIND.
The advanced phase is characterized by apnea, inability to feed, fever, seizures, and a semicomatose statethat progresses to coma. Hypertonicity presents as persistent retrocollis and opisthotonos with bicycling ortwitching of the hands and feet. The cry is inconsolable, or may be weak or absent. Death is due torespiratory failure or intractable seizures.

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 7/18
infants who died with evidence of ABE, 19 had a TB level ≥30 mg/dL (513 micromol/L). The seven infants whodied with lower TB had evidence of severe hemolysis and included six with Rh incompatibility. In this selectcohort of patients, multiple regression analyses demonstrated that sepsis, Rh incompatibility, and incremental TBincreases of 5 mg/dL (86 micromol/L) increased the risk of ABE.
Brainstem auditoryevoked responses (BAER) can be used to detect neurologic effects of hyperbilirubinemia [5860]. In one study, increased TB correlated with prolonged brainstem conduction time [59]. These abnormalitiesresolve as TB values decline. Changes in BAER also have been associated with elevated unbound bilirubin levels[61]. An abnormal BAER and normal otoacoustic emission (OAE) tests suggest that severe hyperbilirubinemiaresults in an auditory neuropathy.
Infants who are at increased risk for ABE include those who were born <37 weeks GA, were breastfed, havehemolytic disease, and are discharged home before 48 hours. Close surveillance of these atrisk infants withtimely intervention can prevent ABE. (See 'Risk factors' above and "Treatment of unconjugated hyperbilirubinemiain term and late preterm infants".)
Kernicterus — Kernicterus (the chronic and permanent sequelae of BIND) develops during the first year afterbirth [55]. Cognitive function usually is relatively spared. The major features of kernicterus include:
Most infants who develop kernicterus have manifested some or all of the findings associated with ABE [2].However, there are reported cases of infants who developed kernicterus with high TB, but without or with only afew signs of ABE [63,64].
In the previously mentioned report of 61 patients from the Pilot Kernicterus Registry who had been readmitted forhyperbilirubinemia, the following diagnoses were the major contributing causes of hyperbilirubinemia that resultedin kernicterus [2]:
All but one of the infants were breastfed. Sixteen infants had lost >10 percent of their BW at the time of hospitalreadmission. (See "Pathogenesis and etiology of unconjugated hyperbilirubinemia in the newborn".)
Choreoathetoid cerebral palsy (CP) (chorea, ballismus, tremor, and dystonia). (See "Hyperkinetic movementdisorders in children".)
Sensorineural hearing loss (SNHL) commonly manifesting as auditory neuropathy (abnormal BAER withnormal otoacoustic emissions). In a retrospective cohort study from a large multicenter health care system,SNHL based on chart review was found to be more frequently observed in patients who had TB ≥10 mg/dL(171 micromol/L) above the American Academy of Pediatrics (AAP) recommendation for exchangetransfusion threshold (ETT) compared with controls with TB below the ETT [62]. In this study, all of theextremely hyperbilirubinemic infants were treated with phototherapy in a timely and effective mannerconsistent with the routine clinical practice of the birth hospitals in this healthcare system. (See "Hearingimpairment in children: Etiology", section on 'Hyperbilirubinemia' and "Treatment of unconjugatedhyperbilirubinemia in term and late preterm infants", section on 'Management approach' and "Treatment ofunconjugated hyperbilirubinemia in term and late preterm infants", section on 'Exchange transfusion'.)
Gaze abnormalities, especially limitation of upward gaze.
Dental enamel dysplasia.
No etiology identified – 20 patientsGlucose6phosphate dehydrogenase (G6PD) deficiency – 20 patientsHemolysis – 9 patientsBruising from birth trauma – 6 patientsInfection – 4 patientsCriglerNajjar Syndrome or galactosemia – 3 patients

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 8/18
Neurologic dysfunction and moderate hyperbilirubinemia — It remains uncertain whether moderatehyperbilirubinemia may be associated with an increased risk of longterm neurologic dysfunction, as demonstratedby the following studies:
However, until there is convincing evidence that demonstrates moderate hyperbilirubinemia is associated withsignificant poor outcomes, recommendations regarding management should not be modified. (See "Treatment ofunconjugated hyperbilirubinemia in term and late preterm infants".)
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics" and"Beyond the Basics." The Basics patient education pieces are written in plain language, at the 5 to 6 gradereading level, and they answer the four or five key questions a patient might have about a given condition. Thesearticles are best for patients who want a general overview and who prefer short, easytoread materials. Beyondthe Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are writtenat the 10 to 12 grade reading level and are best for patients who want indepth information and are comfortablewith some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or email thesetopics to your patients. (You can also locate patient education articles on a variety of subjects by searching on"patient info" and the keyword(s) of interest.)
In the already mentioned populationbased study of 61,238 infants born between 1994 and 2000 from NovaScotia, there were no differences in the composite outcome of CP, developmental delay, hearing and visionlosses, autism, and attention deficit hyperactivity disorder (ADHD) between infants withouthyperbilirubinemia (n = 52,240) and the 3431 infants with mild hyperbilirubinemia, defined as TB of 13.5 to 19mg/dL (231 to 325 micromol/L), (adjusted relative risk [RR] 1.1, 95% CI 1.012.0) or the 348 infants withsevere hyperbilirubinemia, defined as TB >19 mg/dL (>325 micromol/L), (adjusted RR 1.1, 95% CI 0.81.4).When the groups were analyzed for each outcome measure, only developmental delay was increased inthose with moderate hyperbilirubinemia (adjusted RR 1.6, 95% CI 1.32.0) and ADHD in those with severehyperbilirubinemia (adjusted RR 1.9, 95% CI 1.13.3) compared with infants without hyperbilirubinemia.Although not statistically significant, there appeared to be a trend of increased likelihood of autism in infantswith hyperbilirubinemia compared with those without hyperbilirubinemia (adjusted RR 1.6, 95% CI 1.02.5).
Another prospective cohort study failed to find an increase in neurologic findings in 132 of 140 infants withTB levels ≥25 mg/dL (428 micromol/L) compared (blindly) with 372 matched controls who were either notjaundiced or had TB <22.8 mg/dL (390 micromol/L) at two to five years of age [65]. Infants withhyperbilirubinemia, who were treated with either phototherapy (136 cases) or exchange transfusions had alower incidence of questionable or abnormal findings on neurological examination than control infants (17versus 29 percent) [65]. In a subset analysis, nine patients with hyperbilirubinemia and a positive directantiglobulin test (DAT or Coombs test) had lower scores on cognitive testing than other patients withhyperbilirubinemia with a negative DAT.
In a casecontrol study, neonatal hyperbilirubinemia was not a risk factor for autism spectrum disorder for TBlevels of 15 to 19.9 mg/dL (257 to 340 micromol/L, odds ratio [OR] 0.7, 95% CI 0.51.2); 20 to 24.9 mg/dL(342 to 426 micromol/L, OR 0.7, 95% CI 0.31.6); or ≥25 mg/dL (428 micromol/L, OR 1.1, 95% CI 0.111.2)[66].
In contrast, a populationbased study of 733,826 infants born alive in Denmark between 1994 and 2004reported that neonatal jaundice was associated with an increased risk of psychological developmentdisorders including infantile autism [67]. In this study, the exposure to jaundice and the diagnoses ofpsychological disorders were determined based on diagnostic coding from data retrieved from the DanishNational Hospital Register.
th th
th th
Basics topics (see "Patient information: Jaundice in babies (The Basics)")

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&el… 9/18
SUMMARY
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia inthe newborn infant 35 or more weeks of gestation. Pediatrics 2004; 114:297.
Beyond the Basics topics (see "Patient information: Jaundice in newborn infants (Beyond the Basics)")
Total serum/plasma bilirubin (TB) levels >1 mg/dL (17.1 micromol/L) occur in almost all newborn infants andpresent as jaundice. Infants with severe hyperbilirubinemia (TB >25 mg/dL [428 micromol/L]) are at risk forbilirubininduced neurologic dysfunction (BIND), presenting acutely as acute bilirubin encephalopathy (ABE),and if inadequately treated, longterm neurologic sequelae (kernicterus).
In the neonate, TB values vary because of differences in racial composition, breastfeeding practices, theprevalence of hemolytic conditions, and methodology of TB measurements. In California, reported incidencesof hyperbilirubinemia for TB values >30 mg/dL (513 micromol/L), >25 mg/dL (428 micromol/L), and >20 mg/dL(342 micromol/L) were 0.01, 0.14, and 2 percent, respectively. (See 'Epidemiology' above and "Evaluation ofunconjugated hyperbilirubinemia in term and late preterm infants", section on 'Methods to measure bilirubin'.)
Infants remain at risk for severe hyperbilirubinemia and its sequelae of kernicterus, chronic BIND, because ofincreased prevalence of breastfeeding and early discharge of infants from the hospital with failure to set uptimely followup and initiate successful breastfeeding. (See 'Epidemiology' above.)
The following major risk factors identify infants at risk for severe hyperbilirubinemia and BIND (table 1) (see'Risk factors' above):
Predischarge TB or transcutaneous bilirubin (TcB) >95 percentile for age (figure 1)• th
Jaundice within the first 24 hours of life•
Hemolytic disease•
Gestational age (GA) <37 weeks•
Sibling who previously received phototherapy•
Cephalohematoma or significant bruising [22]•
Exclusive breastfeeding, particularly if feeding is not going well•
East Asian race•
Clinical manifestations are due to bilirubin deposition in the skin (jaundice) and the brain.
Jaundice is the yellow color produced by the deposition of bilirubin in the skin and subcutaneous tissues.Although an important and timehonored clinical sign, the presence of jaundice is not a reliable method forassessing the actual TB concentration or for identifying infants at risk for a rapidly rising bilirubin, especiallyin those with dark skin. If jaundice extends below the level of the umbilicus or if there is uncertainty regardingthe presence or extent of jaundice, a TB or TcB measurement should be performed. (See 'Jaundice' aboveand "Evaluation of unconjugated hyperbilirubinemia in term and late preterm infants".)
BIND can occur in otherwise healthy term infants when TB concentrations exceed 25 mg/dL (428micromol/L) and is manifested as ABE that can be reversible or result in kernicterus, a chronic permanentcondition. (See 'Neurologic manifestations' above.)

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 10/18
2. Johnson LH, Bhutani VK, Brown AK. Systembased approach to management of neonatal jaundice andprevention of kernicterus. J Pediatr 2002; 140:396.
3. Maisels MJ. What's in a name? Physiologic and pathologic jaundice: the conundrum of defining normalbilirubin levels in the newborn. Pediatrics 2006; 118:805.
4. MOLLISON PL, CUTBUSH M. A method of measuring the severity of a series of cases of hemolyticdisease of the newborn. Blood 1951; 6:777.
5. HSIA DY, ALLEN FH Jr, GELLIS SS, DIAMOND LK. Erythroblastosis fetalis. VIII. Studies of serumbilirubin in relation to Kernicterus. N Engl J Med 1952; 247:668.
6. HSIA DY, GELLIS SS. Studies on erythroblastosis due to ABO incompatibility. Pediatrics 1954; 13:503.7. Maisels MJ, Newman TB. Kernicterus in otherwise healthy, breastfed term newborns. Pediatrics 1995;
96:730.8. Bhutani VK, Johnson L, Sivieri EM. Predictive ability of a predischarge hourspecific serum bilirubin for
subsequent significant hyperbilirubinemia in healthy term and nearterm newborns. Pediatrics 1999; 103:6.9. Newman TB, Liljestrand P, Escobar GJ. Infants with bilirubin levels of 30 mg/dL or more in a large managed
care organization. Pediatrics 2003; 111:1303.10. Newman TB, Liljestrand P, Escobar GJ. Combining clinical risk factors with serum bilirubin levels to predict
hyperbilirubinemia in newborns. Arch Pediatr Adolesc Med 2005; 159:113.11. Wickremasinghe AC, Kuzniewicz MW, Newman TB. Black race is not protective against hazardous bilirubin
levels. J Pediatr 2013; 162:1068.12. Kuzniewicz MW, Wickremasinghe AC, Wu YW, et al. Incidence, etiology, and outcomes of hazardous
hyperbilirubinemia in newborns. Pediatrics 2014; 134:504.13. Ebbesen F, Bjerre JV, Vandborg PK. Relation between serum bilirubin levels ≥450 μmol/L and bilirubin
encephalopathy; a Danish populationbased study. Acta Paediatr 2012; 101:384.14. Jangaard KA, Fell DB, Dodds L, Allen AC. Outcomes in a population of healthy term and nearterm infants
with serum bilirubin levels of >or=325 micromol/L (>or=19 mg/dL) who were born in Nova Scotia, Canada,between 1994 and 2000. Pediatrics 2008; 122:119.
15. Manning D, Todd P, Maxwell M, Jane Platt M. Prospective surveillance study of severe hyperbilirubinaemiain the newborn in the UK and Ireland. Arch Dis Child Fetal Neonatal Ed 2007; 92:F342.
16. Brooks JC, FisherOwens SA, Wu YW, et al. Evidence suggests there was not a "resurgence" ofkernicterus in the 1990s. Pediatrics 2011; 127:672.
17. Bjerre JV, Petersen JR, Ebbesen F. Surveillance of extreme hyperbilirubinaemia in Denmark. A method toidentify the newborn infants. Acta Paediatr 2008; 97:1030.
18. Sgro M, Campbell DM, Kandasamy S, Shah V. Incidence of chronic bilirubin encephalopathy in Canada,20072008. Pediatrics 2012; 130:e886.
19. Burke BL, Robbins JM, Bird TM, et al. Trends in hospitalizations for neonatal jaundice and kernicterus in theUnited States, 19882005. Pediatrics 2009; 123:524.
20. Christensen RD, Lambert DK, Henry E, et al. Unexplained extreme hyperbilirubinemia among neonates in amultihospital healthcare system. Blood Cells Mol Dis 2013; 50:105.
21. Newman TB, Liljestrand P, Escobar GJ. Jaundice noted in the first 24 hours after birth in a managed careorganization. Arch Pediatr Adolesc Med 2002; 156:1244.
22. Newman TB, Xiong B, Gonzales VM, Escobar GJ. Prediction and prevention of extreme neonatalhyperbilirubinemia in a mature health maintenance organization. Arch Pediatr Adolesc Med 2000; 154:1140.
23. Maisels MJ, Kring E. Length of stay, jaundice, and hospital readmission. Pediatrics 1998; 101:995.24. Gale R, Seidman DS, Dollberg S, Stevenson DK. Epidemiology of neonatal jaundice in the Jerusalem
population. J Pediatr Gastroenterol Nutr 1990; 10:82.25. Berk MA, Mimouni F, Miodovnik M, et al. Macrosomia in infants of insulindependent diabetic mothers.
Pediatrics 1989; 83:1029.26. Peevy KJ, Landaw SA, Gross SJ. Hyperbilirubinemia in infants of diabetic mothers. Pediatrics 1980; 66:417.27. Kuzniewicz MW, Escobar GJ, Wi S, et al. Risk factors for severe hyperbilirubinemia among infants with
borderline bilirubin levels: a nested casecontrol study. J Pediatr 2008; 153:234.

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 11/18
28. Norman M, Åberg K, Holmsten K, et al. Predicting Nonhemolytic Neonatal Hyperbilirubinemia. Pediatrics2015; 136:1087.
29. Watchko JF. Vigintiphobia revisited. Pediatrics 2005; 115:1747.30. Kadakol A, Sappal BS, Ghosh SS, et al. Interaction of coding region mutations and the Gilberttype promoter
abnormality of the UGT1A1 gene causes moderate degrees of unconjugated hyperbilirubinaemia and maylead to neonatal kernicterus. J Med Genet 2001; 38:244.
31. Watchko JF. Genetics and the risk of neonatal hyperbilirubinemia: commentary on the article by Huang et al.on page 682. Pediatr Res 2004; 56:677.
32. Huang MJ, Kua KE, Teng HC, et al. Risk factors for severe hyperbilirubinemia in neonates. Pediatr Res2004; 56:682.
33. Keren R, Luan X, Friedman S, et al. A comparison of alternative riskassessment strategies for predictingsignificant neonatal hyperbilirubinemia in term and nearterm infants. Pediatrics 2008; 121:e170.
34. Soskolne EI, Schumacher R, Fyock C, et al. The effect of early discharge and other factors on readmissionrates of newborns. Arch Pediatr Adolesc Med 1996; 150:373.
35. Kaplan M, Herschel M, Hammerman C, et al. Neonatal hyperbilirubinemia in African American males: theimportance of glucose6phosphate dehydrogenase deficiency. J Pediatr 2006; 149:83.
36. Lain SJ, Roberts CL, Bowen JR, Nassar N. Early discharge of infants and risk of readmission for jaundice.Pediatrics 2015; 135:314.
37. Moyer VA, Ahn C, Sneed S. Accuracy of clinical judgment in neonatal jaundice. Arch Pediatr Adolesc Med2000; 154:391.
38. Tayaba R, Gribetz D, Gribetz I, Holzman IR. Noninvasive estimation of serum bilirubin. Pediatrics 1998;102:E28.
39. Knudsen A, Ebbesen F. Cephalocaudal progression of jaundice in newborns admitted to neonatal intensivecare units. Biol Neonate 1997; 71:357.
40. Azzuqa A, Watchko JF. Bilirubin Concentrations in Jaundiced Neonates with Conjunctival Icterus. J Pediatr2015; 167:840.
41. Chuniaud L, Dessante M, Chantoux F, et al. Cytotoxicity of bilirubin for human fibroblasts and rat astrocytesin culture. Effect of the ratio of bilirubin to serum albumin. Clin Chim Acta 1996; 256:103.
42. Amato MM, Kilguss NV, Gelardi NL, Cashore WJ. Doseeffect relationship of bilirubin on striatalsynaptosomes in rats. Biol Neonate 1994; 66:288.
43. Hoffman DJ, Zanelli SA, Kubin J, et al. The in vivo effect of bilirubin on the NmethylDaspartatereceptor/ion channel complex in the brains of newborn piglets. Pediatr Res 1996; 40:804.
44. Bratlid D. How bilirubin gets into the brain. Clin Perinatol 1990; 17:449.45. Dainat J, de Balbian Verster F, Zand R, Sellinger OZ. Agedependent changes in the specificity of tRNA
methyltransferases in the cerebellum of the icteric and nonicteric Gunn rat. Neurochem Res 1979; 4:557.46. Roger C, Koziel V, Vert P, Nehlig A. Regional cerebral metabolic consequences of bilirubin in rat depend
upon postgestational age at the time of hyperbilirubinemia. Brain Res Dev Brain Res 1995; 87:194.47. Hankø E, Hansen TW, Almaas R, et al. Bilirubin induces apoptosis and necrosis in human NT2N neurons.
Pediatr Res 2005; 57:179.48. Grojean S, Koziel V, Vert P, Daval JL. Bilirubin induces apoptosis via activation of NMDA receptors in
developing rat brain neurons. Exp Neurol 2000; 166:334.49. Rodrigues CM, Solá S, Brites D. Bilirubin induces apoptosis via the mitochondrial pathway in developing rat
brain neurons. Hepatology 2002; 35:1186.50. Bhutani VK, Wong R. Bilirubininduced neurologic dysfunction (BIND). Semin Fetal Neonatal Med 2015;
20:1.51. Good WV, Hou C. Visuocortical bilirubininduced neurological dysfunction. Semin Fetal Neonatal Med 2015;
20:37.52. Olds C, Oghalai JS. Audiologic impairment associated with bilirubininduced neurologic damage. Semin
Fetal Neonatal Med 2015; 20:42.53. Rose J, Vassar R. Movement disorders due to bilirubin toxicity. Semin Fetal Neonatal Med 2015; 20:20.

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 12/18
54. Wusthoff CJ, Loe IM. Impact of bilirubininduced neurologic dysfunction on neurodevelopmental outcomes.Semin Fetal Neonatal Med 2015; 20:52.
55. Volpe JJ. Neurology of the Newborn, 4th ed, WB Saunders, Philadelphia 2001.56. Sgro M, Campbell D, Barozzino T, Shah V. Acute neurological findings in a national cohort of neonates with
severe neonatal hyperbilirubinemia. J Perinatol 2011; 31:392.57. Gamaleldin R, Iskander I, Seoud I, et al. Risk factors for neurotoxicity in newborns with severe neonatal
hyperbilirubinemia. Pediatrics 2011; 128:e925.58. Vohr BR, Karp D, O'Dea C, et al. Behavioral changes correlated with brainstem auditory evoked responses
in term infants with moderate hyperbilirubinemia. J Pediatr 1990; 117:288.59. Gupta AK, Mann SB. Is auditory brainstem response a bilirubin neurotoxicity marker? Am J Otolaryngol
1998; 19:232.60. Agrawal VK, Shukla R, Misra PK, et al. Brainstem auditory evoked response in newborns with
hyperbilirubinemia. Indian Pediatr 1998; 35:513.61. Ahlfors CE, Parker AE. Unbound bilirubin concentration is associated with abnormal automated auditory
brainstem response for jaundiced newborns. Pediatrics 2008; 121:976.62. Wickremasinghe AC, Risley RJ, Kuzniewicz MW, et al. Risk of Sensorineural Hearing Loss and Bilirubin
Exchange Transfusion Thresholds. Pediatrics 2015; 136:505.63. VAN PRAAGH R. Diagnosis of kernicterus in the neonatal period. Pediatrics 1961; 28:870.64. JONES MH, SANDS R, HYMAN CB, et al. Longitudinal study of the incidence of central nervous system
damage following erythroblastosis fetalis. Pediatrics 1954; 14:346.65. Newman TB, Liljestrand P, Jeremy RJ, et al. Outcomes among newborns with total serum bilirubin levels of
25 mg per deciliter or more. N Engl J Med 2006; 354:1889.66. Croen LA, Yoshida CK, Odouli R, Newman TB. Neonatal hyperbilirubinemia and risk of autism spectrum
disorders. Pediatrics 2005; 115:e135.67. Maimburg RD, Bech BH, Vaeth M, et al. Neonatal jaundice, autism, and other disorders of psychological
development. Pediatrics 2010; 126:872.
Topic 4994 Version 34.0
1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 13/18
GRAPHICS
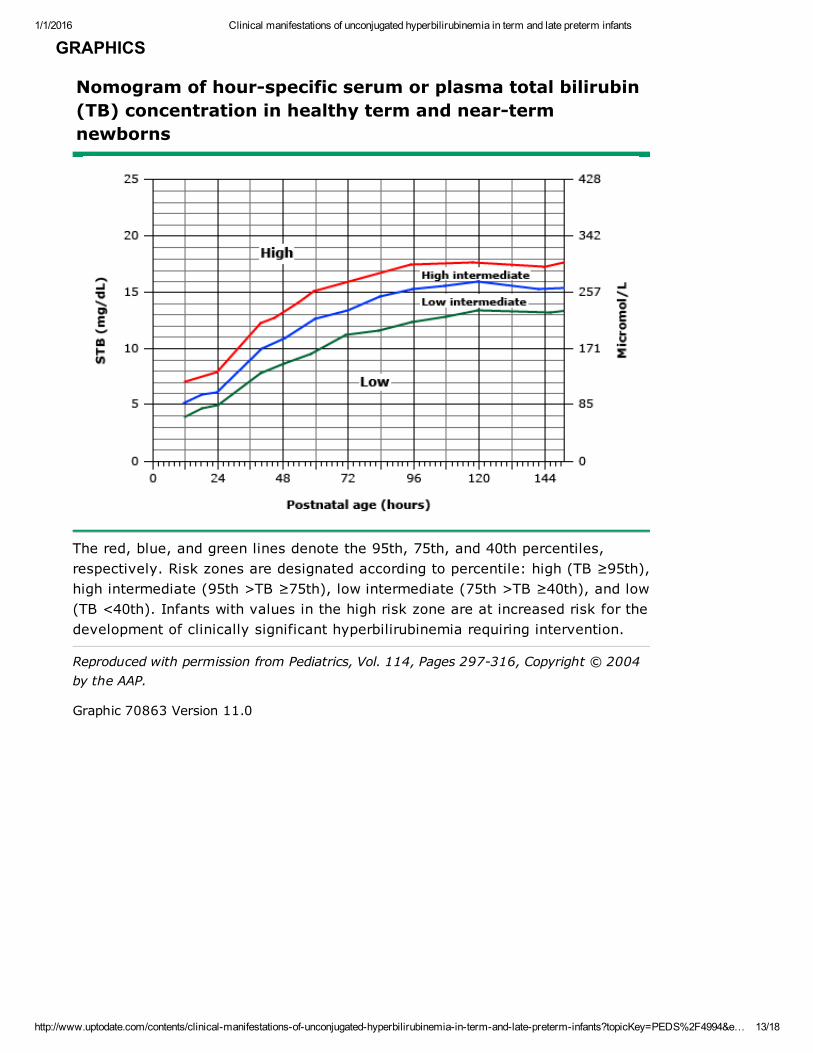
Nomogram of hourspecific serum or plasma total bilirubin(TB) concentration in healthy term and neartermnewborns
The red, blue, and green lines denote the 95th, 75th, and 40th percentiles,respectively. Risk zones are designated according to percentile: high (TB ≥95th),high intermediate (95th >TB ≥75th), low intermediate (75th >TB ≥40th), and low(TB <40th). Infants with values in the high risk zone are at increased risk for thedevelopment of clinically significant hyperbilirubinemia requiring intervention.
Reproduced with permission from Pediatrics, Vol. 114, Pages 297316, Copyright © 2004by the AAP.
Graphic 70863 Version 11.0

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 14/18
Changes in the incidence of extreme hyperbilirubinemia in the United States
Comparison of the incidence of extreme hyperbilirubinemia (total serum bilirubin >25 mg/dL) for 302,399infants born at one of the Intermountain Healthcare (IMHC) facilities from 2001 to 2010, historical data fromthe sevenyear Collaborative Perinatal Project of 41,324 singleton white and black births with birth weights>2.5 kg initiated in 1959 (prior to availability of phototherapy and most [85 percent] infants with total bilirubin>20 mg/dL were treated with an exchange transfusion), and from Northern California population (Newman etal) managed soon after the implementation of 1994 American Academy of Pediatrics (AAP) Guidelines.
From: Brites D, Bhutani VK. Pathways involving bilirubin and other braininjuring agents. In: Clinics in DevelopmentMedicine: Cerebral palsy: Science and clinical practice, Dan B, Mayston M, Paneht N, Rosenbloom L (Eds), Mac Keith Press,London 2014. Copyright © 2014 Mac Keith Press. Reproduced with permission of John Wiley & Sons Inc. This image hasbeen provided by or is owned by Wiley. Further permission is needed before it can be downloaded to PowerPoint, printed,shared or emailed. Please contact Wiley's permissions department either via email: [email protected] or use theRightsLink service by clicking on the 'Request Permission' link accompanying this article on Wiley Online Library(http://onlinelibrary.wiley.com).
Graphic 101082 Version 1.0

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 15/18
Risk factors for development of severe hyperbilirubinemia in infantsof 35 or more weeks gestation (in approximate order of importance)
Major risk factors
Predischarge TB or TcB level in the highrisk zone
Jaundice observed in the first 24 hours
Blood group incompatibility with positive direct antiglobulin test, other known hemolytic disease(eg, G6PD deficiency), elevated ETCOc
Gestational age 35 to 36 weeks
Previous sibling received phototherapy
Cephalohematoma or significant bruising
Exclusive breastfeeding, particularly if nursing is not going well and weight loss is excessive
East Asian race*
Minor risk factors
Predischarge TB or TcB level in the high intermediaterisk zone
Gestational age 37 to 38 weeks
Jaundice observed before discharge
Previous sibling with jaundice
Macrosomic infant of a diabetic mother
Maternal age ≥25 years
Male gender
Decreased risk (these factors are associated with decreased risk ofsignificant jaundice, listed in order of decreasing importance)
TB or TcB level in the lowrisk zone
Gestational age ≥41 weeks
Exclusive bottle feeding
Black race*
Discharge from hospital after 72 hours
TB: total serum or plasma bilirubin; TcB: transcutaneous bilirubin; G6PD: glucose6phosphatedehydrogenase; ETCOc: endtidal carbon monoxide concentration.* Race as defined by mother's description.
Reproduced with permission from Pediatrics, Vol. 114, Pages 297316, Copyright © 2004 by the AAP.
Graphic 64584 Version 15.0

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 16/18
Recommended timing of followup visits for term and near terminfants (>35 weeks gestation)
Age infant discharged Timing of followup visit*
Less than 24 hours of age 72 hours
Between 24 and 47.9 hours of age 96 hours
Between 48 and 72 hours of age 120 hours
* Earlier followup visits and perhaps more frequent visits are required for infants who have risk factorsfor hyperbilirubinemia. If appropriate followup cannot be ensured, especially in infants with an increasedrisk for severe hyperbilirubinemia, then discharge should be delayed until appropriate followup can beensured or the period of greatest risk has passed (72 to 96 hours).
Graphic 65147 Version 2.0
1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 17/18
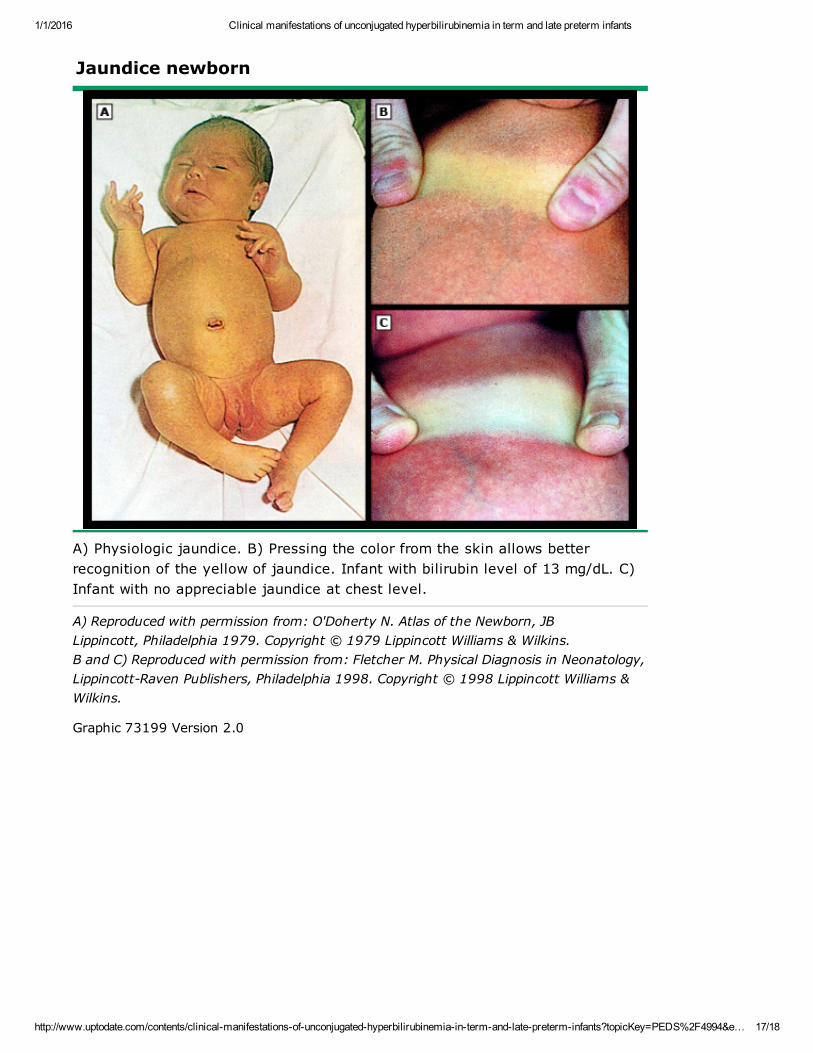
Jaundice newborn
A) Physiologic jaundice. B) Pressing the color from the skin allows betterrecognition of the yellow of jaundice. Infant with bilirubin level of 13 mg/dL. C)Infant with no appreciable jaundice at chest level.
A) Reproduced with permission from: O'Doherty N. Atlas of the Newborn, JBLippincott, Philadelphia 1979. Copyright © 1979 Lippincott Williams & Wilkins.B and C) Reproduced with permission from: Fletcher M. Physical Diagnosis in Neonatology,LippincottRaven Publishers, Philadelphia 1998. Copyright © 1998 Lippincott Williams &Wilkins.
Graphic 73199 Version 2.0

1/1/2016 Clinical manifestations of unconjugated hyperbilirubinemia in term and late preterm infants
http://www.uptodate.com/contents/clinicalmanifestationsofunconjugatedhyperbilirubinemiaintermandlatepreterminfants?topicKey=PEDS%2F4994&e… 18/18
Disclosures: Ronald J Wong, BA Nothing to disclose. Vinod K Bhutani, MD, FAAP Nothing to disclose. Steven A Abrams, MDGrant/Research/Clinical Trial Support: MeadJohnson, Nutrition [Pediatric Nutrition (Infant formulas)]. Consultant/Advisory Boards:MilkPrep [dairy products (fluid milk)]. Melanie S Kim, MD Nothing to disclose.Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through amultilevel review process, and through requirements for references to be provided to support the content. Appropriately referencedcontent is required of all authors and must conform to UpToDate standards of evidence.Conflict of interest policy
Disclosures