Chronic liver disease
36
Chronic Liver Disease BY PROF/ GOUDA ELLABBAN
-
Upload
scu-hospital -
Category
Health & Medicine
-
view
151 -
download
3
Transcript of Chronic liver disease

Chronic Liver Disease
BY PROF/ GOUDA ELLABBAN

Burden
Markedly decreased life expectancy 12th leading cause of death in US 25,000 deaths annually 373,00 hospital discharges High morbidity and mortality due to
complications

Cirrhosis
Alcoholic liver disease
Chronic hepatitis B
Chronic hepatitis C
Primary biliary cirrhosis
Primary sclerosing cholangitis
Autoimmune hepatitis
Hereditary hemochromatosis
Wilson’s disease
Alpha1-antitrypsin deficiency
Hepatic Fibrosis

Hepatic fibrosis
Fibrosis is a wound healing response in which damaged regions are encapsulated by an extracellular matrix or scar
Develops in almost all patients with chronic liver injury
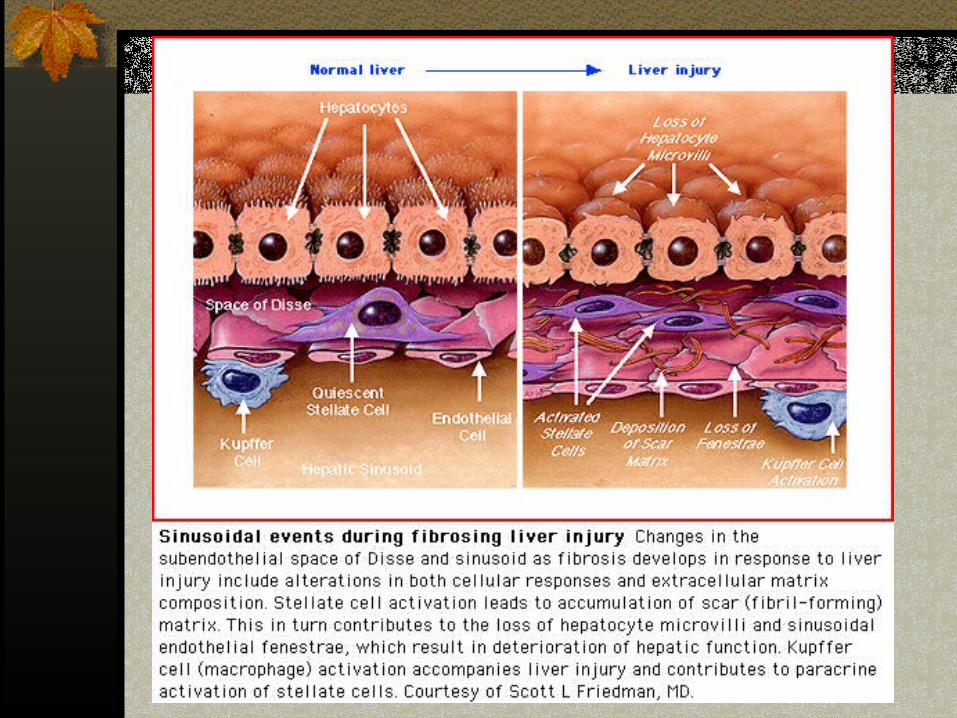

Cirrhosis
Late stage of progressive hepatic fibrosis Characterized distortion of hepatic
architecture and formation of regenerative nodules
Generally irreversible in advanced stages

Case
55 yo man with h/o heavy ETOH use presents with abdominal swelling and pain
What other questions would you ask the patient???
What are you looking for on your exam???
Case
Exam Temp 99.5, BP 98/66, scleral icterus Chest- crackles in bases, scattered
“spiders” Abd- distended, dilated abd wall veins,
diffusely tender Ext- 2+ edema B

Case
AST 150, ALT 73, alk phos 153, GGT 320, bili 4.3/3.1, TP 8.3, alb 2.2, PT INR 1.9
WBC 2.2, H/H 11/33. Plt 78K Na 130

LFT’s
LFT’s is a misleading term Do not reflect how well the liver is
functioning Abnormal values can be caused by non-
hepatic diseases

LFT’s
Enzyme tests- AST ALT, Alk P and GGT Synthetic function- Albumin and PT Hepatic transport ability- Bilirubin
Patterns
Disproportionate elevation of transaminases seen with hepatocellular processes
Diproportionate elevation of Alk P in cholestatic process
Serum Bili can be elevated in both processes so not helpful in differentiating
Patterns Low albumin suggests a chronic prcess Normal albumin suggest acute process Elevated PT is either Vit K deficiency
(due to juandice and malabs of Vit K) or significant hepatocellular dysfunction
Failure of parenteral Vit K to correct PT indicates the latter
Bilirubin
Catabolic product of heme metabolism Elevated from:
Overproduction Impaired uptake, conjugation or exceretion Backwards leakage from damaged
hepatocytes or bile ducts

Case
AST 150, ALT 73, alk phos 153, GGT 320, bili 4.3/3.1, TP 8.3, alb 2.2, PT INR 1.9
WBC 2.2, H/H 11/33. Plt 78K Na 130
What would you do first in the evaluation of this patient??

Paracentesis
What information do you get from peritoneal fluid analysis???
What studies do you want to perform on the ascites fluid???

Ascitic fluid
Cloudy fluid Albumin 0.5 TP 0.7 Cell count- 425 WBC, 90% PMN’s Gram stain- many PMN’s, no bacteria

How do you interpret the results from your tap??

Serum-to ascites albumin gradient (SAAG)
SAAG= (serum albumin)-(ascitic fluid albumin) What is our patient’s SAAG???
SAAG > 1.1 indicates portal HTN SAAG < 1.1 indicates pt does not have
portal HTN


Diagnosis of SBP
Definition- ascitic fluid infection w/o intraabdominal source of infection
Positive ascitic fluid culture and/or PMN>250 Calculate this patient’s ascitic PMN count
Consider secondary peritonitis if: TP >1.0 Glucose <50 LDH > upper limit for serum

How will you treat SBP??

Antibiotic choice
Need to cover gut flora as well as Strep and Staph
3rd generation cephalosporin such as cefotaxime 2g IV q8hrs
Treat for 5 days and reassess patient If has had good response, d/c antibiotics If still has fever or abd pain, re-tap
PMN <250, stop antibiotics PMN > pre-treatment level, look for surgical cause PMN >250 but < pre-treatment level, give 48 hrs antibiotocs
and repeat tap

SBP Prophylaxis
Indicated for patients with h/o SBP or variceal bleed
Proven to decrease mortality, to prevent bacterial infections, and to be cost effective

SBP Prophylaxis Regimens
If h/o SBP, Norfloxacin 400 mg qd or Bactrim DS qd
If recent variceal bleed, Norfloxacin 400 mg BID or Bactrim DS BID for 7 days

Why do patients with cirrhosis develop ascites??
Ascites formation in cirrhosis
1st step is development of portal HTN (>12 mm Hg)
Portal HTN leads to splanchnic vasodilation Collateral vein formation Local production of vasodilators (NO)
Vasodilation leads to systemic effects

How will you treat the ascites??
Treatment of ascites
Goal is to minimize edema and ascites w/o intravacular volume depletion
No evidence that treatment of ascites improves survival, but pt’s feel better
Treat underlying disorder- ETOH and autoimmune hepatitis
Avoid NSAID’s Limit Na to 2g/day
Treatment of ascites
Start with combo of spironolactone and furosemide (100 mg and 40mg) or spironolactone alone
Max rec’d doses: spironolactone 400mg/d and furosemide 160 mg/d
Rec’d wt loss is 300-500g/d w/o edema and 800-1000g/d w/edema

Treatment of large volume ascites
Treatment of choice is large volume paracentesis
Faster, more effective and fewer adverse effects vs. diuresis
Diuretics should be given as maintenance therapy to prevent recurrence

Complications of cirrhosis
Variceal hemorrhage Ascites Spontaneous bacterial peritonitis Hepatorenal syndrome Hepatic encephalopahty Hepatopulmonary syndrome Hepatocellular carcinoma