
Choledochal cyst
53
Choledochal Cyst (Greek chol- bile + docho- duct) Jibran Mohsin Resident, Surgical Unit I SIMS/Services Hospital, Lahore
-
Upload
jibran-mohsin -
Category
Health & Medicine
-
view
205 -
download
2
Transcript of Choledochal cyst

Choledochal Cyst(Greek chol- bile + docho- duct)
Jibran Mohsin
Resident, Surgical Unit I
SIMS/Services Hospital, Lahore

A 35 year old female resident of Lahore presented in medical emergency on 29 December 2014 with
presenting complaint of severe epigastric pain radiating directly to back for last 3 days, relieved on leaning forward and medication.

A 35 year old female resident of Lahore presented in medical emergency on 29 December 2014 with
presenting complaint of severe epigastric pain radiating directly to back for last 3 days, relieved on leaning forward and
medication.
Frequently diagnosed in infancy or childhood(Approximately 60%-67% cases < 10 years)
around 50 % cases have reached adulthood when diagnosed

A 35 year old female resident of Lahore presented in medical emergency on 29 December 2014 with
presenting complaint of severe epigastric pain radiating directly to back for last 3 days, relieved on leaning forward and medication.
M:F (1:3 to 1:8)
A 35 year old female resident of Lahore presented in medical emergency on 29 December 2014 with
presenting complaint of severe epigastric pain radiating directly to back for last 3 days, relieved on leaning forward and medication.
Much more prevalent in Asia than in Western countries(1: 100,000 – 1: 150,000)
Approximately 33-50% of reported cases come from Japan( as high as 1:1000)

A 35 year old female resident of Lahore presented in medical emergency on 29 December 2014 with
presenting complaint of severe epigastric pain radiating directly to back for last 3 days, relieved on leaning forward and medication, associated
with 4-5 episodes of greenish colored vomiting
AdultsPresent with one or more severe complications
(obstructive jaundice, pancreatitis and cholangitis)
Frequently, adults with choledochal cysts complain of vague epigastric or right upper quadrant pain and can develop jaundice or cholangitis.
Most common symptom in adults is abdominal pain.

• Abdominal examination revealed tenderness in epigastrium with no mass/viscera palpable and bowel sounds audible– Rest of examination was unremarkable
• Among Baselines– TLC 17.2 , total bilirubin 0.8
– Serum amylase 438 and lipase 1018

Classic Triad of abdominal pain, jaundice and RUQ mass seen in only 10-20 % cases
• Abdominal examination revealed tenderness in epigastrium with no mass/viscera palpable and bowel sounds audible– Rest of examination was unremarkable
• Among Baselines– TLC 17.2 , total bilirubin 0.8
– Serum amylase 438 and lipase 1018

• Abdominal examination revealed tenderness in epigastrium with no mass/viscera palpable and bowel sounds audible– Rest of examination was unremarkable
• Among Baselines– TLC 17.2 , total bilirubin 0.8
– Serum amylase 438 and lipase 1018
Cholangitis
• Abdominal examination revealed tenderness in epigastrium with no mass/viscera palpable and bowel sounds audible– Rest of examination was unremarkable
• Among Baselines– TLC 17.2 , total bilirubin 0.8
– Serum amylase 438 and lipase 1018
May Reveal Obstructive Jaundice

• Abdominal examination revealed tenderness in epigastrium with no mass/viscera palpable and bowel sounds audible– Rest of examination was unremarkable
• Among Baselines– TLC 17.2 , total bilirubin 0.8
– Serum amylase 438 and lipase 1018
Acute Pancreatitis
Patient was admitted on medical floor and was managed and worked up on lines of
ACUTE PANCREATITIS
&
Departmental USG abdomen was done

Patient was admitted on medical floor and was managed and worked up on lines of
ACUTE PANCREATITIS
&
Departmental USG abdomen was done
DIFFERENTIAL DIAGNOSIS of Choledochal Cyst
Bile Duct Tumors
Biliary Obstruction
Cholangiocarcinoma
Acute Pancreatitis

Patient was admitted on medical floor and was managed and worked up on lines of
ACUTE PANCREATITIS
&
Departmental USG abdomen was done
Associated Morbidity in Adults
• hepatic abscesses
• Secondary biliary cirrhosis
• portal hypertension
• recurrent pancreatitis
• cholelithiasis and CBD stone
• Cyst rupture Peritonitis
• Cholangiocarcinoma

Ultrasound Abdomen( 04-01-2015)
• Dilated CBD with 1.8 cm calibre
• Sludge ball without acoustic shadowing measuring 1.6 x 0.8 cm in distal part of CBD
• Intrahepatic Biliary channels not dilated
• Impression:– Choledochocele with possibility of sludge ball at distal end of CBD– ERCP advised

US shows a cyst mass near pancreatic head
US shows: 1- splenic vein; 2-portal vein and 3 - cystic mass;

US shows relationship of cystic mass(C) with gall bladder(GB) and portal vein(VP)
Portal vein and its relation with cystic mass

On the basis of dilated CBD finding on USG, for the workup of obstructive jaundice
CT scan was advised, followed by MRCP

CT-Abdomen and Pelvis with IV & oral Contrast (07-01-2015)
• Cystic dilation of 38.5 x 19.5 mm along with sludge and particulate matter
• Partially contracted Gallbladder with sludge
• Generalised decreased echogenicity of pancreas with coarse margins.
• Dilated CBD 10.7 mm at portahepatis and 3.8 mm at distal end

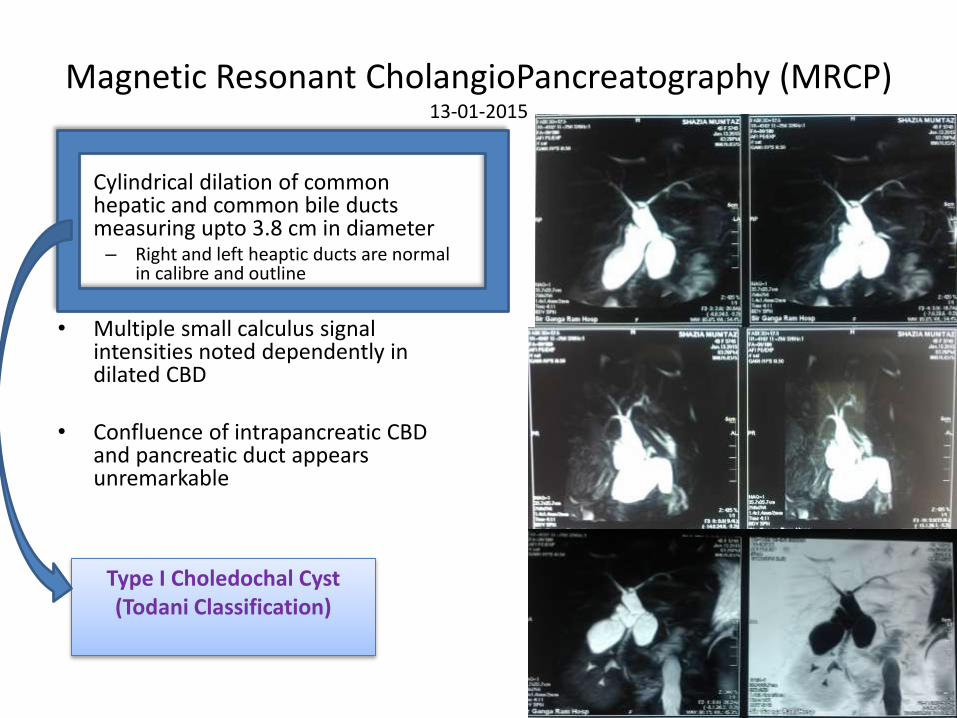
Magnetic Resonant CholangioPancreatography (MRCP)13-01-2015
• Cylindrical dilation of common hepatic and common bile ducts measuring upto 3.8 cm in diameter– Right and left heaptic ducts are normal
in calibre and outline
• Multiple small calculus signal intensities noted dependently in dilated CBD
• Confluence of intrapancreatic CBD and pancreatic duct appears unremarkable
Magnetic Resonant CholangioPancreatography (MRCP)13-01-2015
• Cylindrical dilation of common hepatic and common bile ducts measuring upto 3.8 cm in diameter– Right and left heaptic ducts are normal
in calibre and outline
• Multiple small calculus signal intensities noted dependently in dilated CBD
• Confluence of intrapancreatic CBD and pancreatic duct appears unremarkable
Type I Choledochal Cyst(Todani Classification)

Magnetic Resonant CholangioPancreatography (MRCP)13-01-2015
• Cylindrical dilation of common hepatic and common bile ducts measuring upto 3.8 cm in diameter– Right and left heaptic ducts are normal
in calibre and outline
• Multiple small calculus signal intensities noted dependently in dilated CBD
• Confluence of intrapancreatic CBD and pancreatic duct appears unremarkable
Choledocholithiasis

Magnetic Resonant CholangioPancreatography (MRCP)13-01-2015
• Cylindrical dilation of common hepatic and common bile ducts measuring upto 3.8 cm in diameter– Right and left heaptic ducts are normal
in calibre and outline
• Multiple small calculus signal intensities noted dependently in dilated CBD
• Confluence of intrapancreatic CBD and pancreatic duct appears unremarkable
Anomalous junction between the common bile duct and the pancreatic duct
>1 cm common channel (90-100 % cases)
allows pancreatic secretions to reflux into the common bile ductActivated pancreatic proenzymes damage and weak the bile duct wall (Long common channel/Babbit theory-1969)

Type Configuration Biliary Tract Incidence Treatment
Extrahepatic Intra-hepatic
I A Saccular Most or all >50 % to 75 %
Excision of involved portion of extrahepatictract + Roux-en-Y Hepato-jejunostomy
B Limited
C Fusiform Most or all
II IsolatedDiverticulumOf CBD
5 % Excision with closure of defect over T-tube or same as above
III IntraduodenalPart ofCBD
5 % < 3 cm =endoscopic sphincterotomy> 3cm = excision via transduodenalapproachCHOLEDOCHOCELE
TODANI(1977) CLASSIFICATION

Type Configuration Biliary Tract Incidence Treatment
Extrahepatic Intra-hepatic
IV A
Mu
ltip
le
Dila
tio
ns
30 % ExtrahepaticExcision of involved portion + Roux-en-Y Hepato-jejunostomy
IntrahepaticResection of segment or lobeOr transplantation
B
V 1 %
VI Isolated Cyst of Cystic Duct
ExtremelyRare
Cystic Ductligation near CBD
CAROLI DISEASE (1958)
NOT part of Todani Classification
TODANI(1977) CLASSIFICATION
Jacques CaroliFrench gastroenterologist, 1902-1979

• Call to Surgical Unit on Call was sent on 16-01-2015 and patient shifted to Surgical floor for further management.
• Time for ERCP ( 09-02-2015) taken for choledocholithiasis and managed conservatively and sent on leave
• ERCP team deferred ERCP as patient was asymptomatic with normal LFTs and no obstruction and referred back to surgery

After optimizing the patient for general anesthesia, patient was operated on 16-02-2015

After optimizing the patient for general anesthesia, patient was operated on 16-02-2015
surgery is the only currently available definitive therapy

OPERATIVE FINDINGS
– Type I septate Choledochal Cyst
– Choledocholithiasis
– Saponification of omentum

OPERATIVE FINDINGS
– Type I septate Choledochal Cyst
– Choledocholithiasis
– Saponification of omentum
Main Disease

OPERATIVE FINDINGS
– Type I septate Choledochal Cyst
– Choledocholithiasis
– Saponification of omentum
Associated Morbidity

OPERATIVE FINDINGS
– Type I septate Choledochal Cyst
– Choledocholithiasis
– Saponification of omentum
Visual confirmation of initial diagnosis of Acute Pancreatitis(complication/associated morbidity of Choledochal Cyst)

PROCEDURE
Excision of choledochal Cyst +
Roux-en-Y hepatojejunostomy +
Cholecystectomy

PROCEDURE
Excision of choledochal Cyst +
Roux-en-Y hepatojejunostomy +
Cholecystectomy
PRINCIPLE OF SURGERY
Treatment of choice for choledochal cysts is complete excision of the cyst +
with construction of a biliary-enteric anastomosis to restore continuity with the GI tract

PROCEDURE
Excision of choledochal Cyst +
Roux-en-Y hepatojejunostomy +
Cholecystectomy
MUST in all cases of choledochal Cyst

• Kocher incision made
• Mobilisation of Transverse Colon from hepatic Flexure
• Retrograde dissection of GB from liver bed

• Kocher incision made
• Mobilisation of Transverse Colon from hepatic Flexure
• Retrograde dissection of GB from liver bed
Retrograde Dissected GB
Cystic Duct
CholedochalCyst
CBD

• Choledochal Cyst dissected away from portal vein and hepatic artery ( Lilly Technique)
• Cyst wall opened till common hepatic duct junction

• Choledochal Cyst dissected away from portal vein and hepatic artery ( Lilly Technique?)
• Cyst wall opened till common hepatic duct junction

• Choledochal Cyst dissected away from portal vein and hepatic artery ( Lilly Technique?)
• Cyst wall opened till common hepatic duct junction
Occasionally, Cyst adheres densely to the portal vein secondary to long-standing inflammatory reaction
complete, full-thickness excision of the cyst may not be possible
serosal surface of the duct is left adhering to the portal vein, while the mucosa of the cyst wall is obliterated by curettage or cautery
Theoretically, this removes the risk of malignant transformation in that segment of the duct
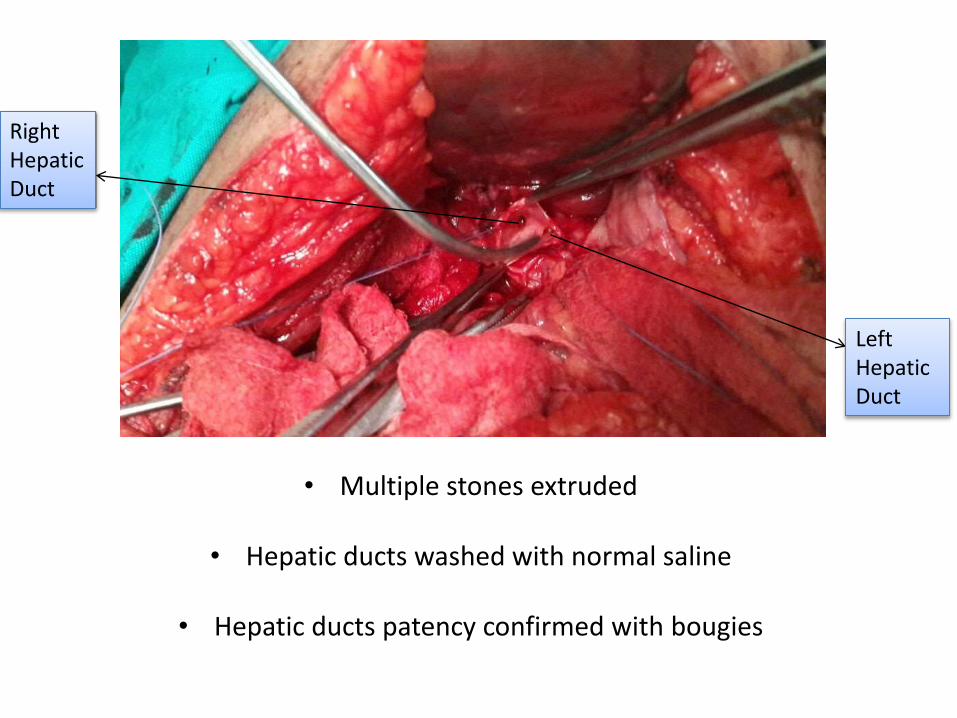
• Multiple stones extruded
• Hepatic ducts washed with normal saline
• Hepatic ducts patency confirmed with bougies
• Multiple stones extruded
• Hepatic ducts washed with normal saline
• Hepatic ducts patency confirmed with bougies
Left HepaticDuct
Right HepaticDuct

• Roux-en-Y (french: rōō'ěn-wī')
Hepatojejunostomy done(retrocolic isoperistaltic functional side-to-side)
Cesar RouxSwiss Surgeon (1857-1934),
(Performed 1st successful excision ofpheochromocytoma in 1926)
(End-to-side)
(End-to-side ORSide-to-side)

• Cholecystectomy done en bloc
• Subhepatic Drain placed
• Specimen sent for histopathology

• Cholecystectomy done en bloc
• Subhepatic Drain placed
• Specimen sent for histopathology
Cyst Wall• Chronic inflammation, Sparse mucin glands and metaplasia• Either glandular with normal cuboidal epithelium with cavities in
mucosa or fibrotic type with fibrous cyst wall
most feared histologic abnormality is the presence of cholangiocarcinoma

Post Operative Recovery
• Patient kept NPO for 72 hours
• Early mobilization
• Chest Physiotherapy and Incentive Spirometry
• IV fluids, antibiotics(Zinacef, then Tinem), PPI and analgesics
• Drain removed on 5th POD (21-02-2015)
– 24 hours after removal of drain (6th POD) patient start complaining of RHC pain along with swinging fever(max. 1030F)
– Drain site wound bandage slightly soaked with bile stained fluid– USG guided Drain was replaced through previous drain wound with 600 ml of
greenish fluid aspirated BUT minimal fluid drained till then

Right Pleural Effusion
Pre operative 8th Post Operative Day(24-02-2015)

Right Subphrenic and subhepatic Collection
CT-scan done on11th Post Operative Day
(27-02-2015)

Reinserted Drain removed on 14th POD (02-03-2015)

Further Plan
USG-guided Aspiration
Versus
Re-exploration

Follow Up
Lifelong follow-up because of the increased risk of cholangiocarcinoma,
even after complete excision of the cyst
(even at site of anastomosis)

Follow Up
Lifelong follow-up because of the increased risk of cholangiocarcinoma,
even after complete excision of the cyst
(even at site of anastomosis)
Cholangiocarcinoma: most feared complication(9 -28% cases; increases with age; more common with type I and V )



















