Appendix Biliary Conduit Choledochal Cysts · Appendix as a Biliary Conduit for Choledochal Cysts...
4
Appendix as a Biliary Conduit for Choledochal Cysts in Children Abstract Biliary conduits are constructed in operations for choledochal rysts. A wide variety of options are available for biliary tract re- construction. We present our experience of treating six children with choledochal cysts by using the appendix as a biliary con- duit. After mobilizing the appendix on its vascular pedicle, non- refluxing, tunneled anastomosis was made with the 2nd part of the duodenum and the appendix. The operative procedure was simple and less time-consuming. Postoperative evaluation was done with the help of HIDA scan and ultrasound examination. Postoperative cholangitis was conspicuously absent in the two years of follow-up. One child has been lost to follow-up. From our preliminary experience, the operation seems simple and sat- isfuing. Though the long-term efficacy still remains to be proven, the appendix should prove durable as a functional conduit. Keywords Choledochal cyst. appendix R6sum6 Des n6o-conduits biliaires sont r6alis6s pour traiter les kystes du chol6doque. Une large vari6t6 de possibilit6s sont disponibles pour la reconstruction de l'arbre biliaire. Nous pr6sentons notre exp6rience du traitement de six enfants avec des kystes du cho- l6doque en utilisant I'appendice comme n6o-canal biliaire. AprEs avoir mobilis6 I'appendice sur son p6dicule vasculaire, une anas- tomose tunn6lisr6e non refluente 6tait r6alisee entre la deuxidme partie du duod6num et I'appendice. Le proc6d6 op6ratoire est A. A. Shah A. V. Shah simple et peu consommateur de temps. L'6valuation post-op6ra toire 6tait faite avec l'aide d'une scintigraphie i HIDA et un 6chographie. Une cholangite post-op6ratoire n'6tait jamais ob serv6e dans les deux ans de suivi. Un enfant a 6t6 perdu de vut De iette exp6rience prdliminaire, cette op6ration parait simple t satisfaisante. Quoiqu'une efficacit6 i plus long terme reste prouver, I'appendice pourrait €tre un n6o-canal biliaire valable. Mots-cl6s Kyste du chol6doque' appendice Resumen En las operaciones por quiste del col6doco es necesario recor struir la via biliar para lo que hay varias opciones disponible Presentamos nuestra experiencia en el uso del ap6ndice com conducto biliar en 6 niflos con quiste del col6doco. Tras moviliz; el ap6ndice con su pediculo vascular se realiz6 una anastomos tunelizada entre la segunda porci6n del duodeno y el ap6ndic, El procedimiento operatorio fue fdcil y breve. La evaluaci6n post operatoria se hizo con ayuda de HIDA y estudio ecogr6fico. N hubo colangitis postoperatoria en los 2 af,os de seguimientr Hemos perdido de vista uno de los niflos. De esta experienci preliminar deducimos que esta operaci6n parece Simple y satil factoria aunque la eficacia a largo plazo no ha sido arin probad El ap6ndice parece ser un conducto biliar funcional. Palabras clave Quiste del col6doco. ap6ndice Affiliation Department of Pediatric Surgery K. M. School of Postgraduate Medicine and Research, N. H. L. Municipal Medical College, V. S. Hospital, Ahmedabad, India Correspondence Dr. Anirudh V. Shah. "Anicare", 13, shantisadan society. Nr. Parimal Garden, Nr. Doctor House. Ellisbridge, Ahmedabad, 380006 . lndia . E-mail: [email protected], [email protected] Received: January 8, 2004 .Accepted after Revision: March 14, 2004 Bibliography EurJ Pediatr Surg 2005; 15: 728-731. @ Georg Thieme Verlag KG Stuttgart ' New York' DOI 10.105s/s-2004-827220 . rssN 0939-7248
Transcript of Appendix Biliary Conduit Choledochal Cysts · Appendix as a Biliary Conduit for Choledochal Cysts...

Appendix as a Biliary Conduit forCholedochal Cysts in Children
Abstract
Biliary conduits are constructed in operations for choledochal
rysts. A wide variety of options are available for biliary tract re-
construction. We present our experience of treating six childrenwith choledochal cysts by using the appendix as a biliary con-
duit. After mobilizing the appendix on its vascular pedicle, non-
refluxing, tunneled anastomosis was made with the 2nd part ofthe duodenum and the appendix. The operative procedure was
simple and less time-consuming. Postoperative evaluation was
done with the help of HIDA scan and ultrasound examination.
Postoperative cholangitis was conspicuously absent in the twoyears of follow-up. One child has been lost to follow-up. From
our preliminary experience, the operation seems simple and sat-
isfuing. Though the long-term efficacy still remains to be proven,
the appendix should prove durable as a functional conduit.
KeywordsCholedochal cyst. appendix
R6sum6
Des n6o-conduits biliaires sont r6alis6s pour traiter les kystes du
chol6doque. Une large vari6t6 de possibilit6s sont disponiblespour la reconstruction de l'arbre biliaire. Nous pr6sentons notre
exp6rience du traitement de six enfants avec des kystes du cho-
l6doque en utilisant I'appendice comme n6o-canal biliaire. AprEs
avoir mobilis6 I'appendice sur son p6dicule vasculaire, une anas-
tomose tunn6lisr6e non refluente 6tait r6alisee entre la deuxidmepartie du duod6num et I'appendice. Le proc6d6 op6ratoire est
A. A. Shah
A. V. Shah
simple et peu consommateur de temps. L'6valuation post-op6ra
toire 6tait faite avec l'aide d'une scintigraphie i HIDA et un
6chographie. Une cholangite post-op6ratoire n'6tait jamais ob
serv6e dans les deux ans de suivi. Un enfant a 6t6 perdu de vut
De iette exp6rience prdliminaire, cette op6ration parait simple tsatisfaisante. Quoiqu'une efficacit6 i plus long terme reste
prouver, I'appendice pourrait €tre un n6o-canal biliaire valable.
Mots-cl6sKyste du chol6doque' appendice
Resumen
En las operaciones por quiste del col6doco es necesario recor
struir la via biliar para lo que hay varias opciones disponible
Presentamos nuestra experiencia en el uso del ap6ndice com
conducto biliar en 6 niflos con quiste del col6doco. Tras moviliz;
el ap6ndice con su pediculo vascular se realiz6 una anastomos
tunelizada entre la segunda porci6n del duodeno y el ap6ndic,
El procedimiento operatorio fue fdcil y breve. La evaluaci6n post
operatoria se hizo con ayuda de HIDA y estudio ecogr6fico. N
hubo colangitis postoperatoria en los 2 af,os de seguimientr
Hemos perdido de vista uno de los niflos. De esta experienci
preliminar deducimos que esta operaci6n parece Simple y satil
factoria aunque la eficacia a largo plazo no ha sido arin probad
El ap6ndice parece ser un conducto biliar funcional.
Palabras clave
Quiste del col6doco. ap6ndice
AffiliationDepartment of Pediatric Surgery K. M. School of Postgraduate Medicine and Research, N. H. L. MunicipalMedical College, V. S. Hospital, Ahmedabad, India
CorrespondenceDr. Anirudh V. Shah. "Anicare", 13, shantisadan society. Nr. Parimal Garden, Nr. Doctor House.
Ellisbridge, Ahmedabad, 380006 . lndia . E-mail: [email protected], [email protected]
Received: January 8, 2004 .Accepted after Revision: March 14, 2004
BibliographyEurJ Pediatr Surg 2005; 15: 728-731. @ Georg Thieme Verlag KG Stuttgart ' New York'DOI 10.105s/s-2004-827220 .
rssN 0939-7248

Zusammenfassung
Bei der Operation von Choledochuszysten muss eine biliiire Ab_leitung mit Zwischenschaltung anderer Organe durchgeftihrtwerden. Zur Rekonstruktion der Gallenwege werden vielfiiltigeTechniken angegeben. In der vorliegenden Arbeit werden 6 I(in-der mit einer Choledochuszyste vorgestellt, bei denen die Ap-pendix zur Gallenableitung verwandt wurde. Nach Mobilisie-rung der Appendix mit ihrer vaskuldren Versorgung wurde einnicht refluxiver Tunnel mit dem zweiten Teil des Duodenumsangelegt und die Appendix mit dem Choledochus verbunden.Das operative Verfahren war einfach und wenig zeitaufwdndig.Postoperativ wurden mithilfe des HIDA-Scans und des Ultra-
schalls die I(inder nachuntersucht. Bei allen war, zumindest zweiJahre nach dem Eingriff, keine postoperative Cholangitis zu be-obachten. Ein I(ind konnte nicht weiter nachuntersucht werden.Schlussfolgerungen: Von unseren begrenzten Erfahrungen herkann die Operation mit Interposition einer Appendix zwischenCholedochus und unterem Duodenum bei Vorliegen einer Chole-dochuszyste empfohlen werden. Allerdings muss noch geprtiftwerden, ob die Appendix selbst als ein brauchbares, funktionel-les und vor allem dauerhaftes Ersatzrohr geeignet ist.
SchliisselwiirterCholedochuszyste . Appendix . Galleableitung
Introduction
The use of intestinal segments to reconstruct the biliary systemafter surgery for biliary atresia or choledochal cyst is not new.I(asai et al. [9] first described hepaticoportoenterostomy, whichinvolved the use of a Roux-en-y jejunal loop. Later, many modifi-cations were made to the technique by l(asai and others [4,5,10,11,171, but a major problem ofthese techniques has been as-cending cholangitis. Ascending cholangitis has been noted in upto 50-90% of cases with a high incidence of morbidity [12]. Theauthors describe here their experience with the use ofthe appen-dix as a biliary conduit for biliary reconstruction following exci-sion of choledochal cysts in six children. The operation is easierand it achieves an anatomic reconstruction that is close to nor-mal.
Materials and Methods
Six patients between 4 and g months of age with choledochalcysts type I were studied from March 2000 to September 2001.Three patients presented with conjugated hyperbilirubinemia,while one presented with a perforated choledochal cyst withbiliary peritonitis. Two were diagnosed incidentally on abdomi-nal ultrasound.
In addition to clinical examination, hematological tests for a fullblood count, renal lunction tests, liver function tests, and a coag-ulation profile were carried out. An ultrasound examination wasdone in all cases for the evaluation of the extra- and intrahepaticducts. Magnetic resonance cholangiopancreatography was donepreoperatively in all cases to rule out biliopancreatic ductanomalies.
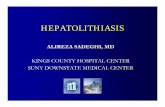
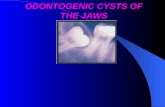
The abdomen was opened through a supraumbilical right trans-verse incision. The right colon and hepatic flexure was mobilizedto bring the cecum under the liver. The appendix was then de-tached, preserving the vascular pedicle. The stump was ligatedand buried, using purse string sutures. The tip of the appendixwas cut open so as to form a tube from the appendix. This wasirrigated with a solution of providone iodine and saline. Thececal end of the appendix was anastomosed with the commonhepatic duct with interrupted 5-0 dexon or vicryl sutures. Thedistal end of the appendix was anastomosed to the duodenum
with interrupted 5 - 0 dexon or vicryl sutures after forming a tun-nel between the mucosa and the muscularis. The seromuscularlayers were closed over it using interrupted 5-0 dexon sutures(Figs.1 and 2). Adrainwas placed in the sub-hepatic space. post-operatively it has been our practice to give prophylactic antibiot-ics for a period of six weeks. We used a combination of trimetho-prim and sulphamethoxazole (cotrimoxazole 1.2mg/kg once dai-ly in all our patients. Hematological and biochemical investiga-tions were repeated two weeks after surgery and subsequentlyat six weeks during the first follow-up. An ultrasound was doneat 3 months and supplemented with a Tc HIDA scan in threepatients. Repeat ultrasound scans were done on a yearly basisfor the first two years. Hematological and biochemical investi-gations were repeated every 6 months for the first two years.Follow-up was done every 6 months up to a period of two years,following which the children will be reviewed on a yearly basis(Table 1 ).
Results
All children did well in the postoperative period. There was noevidence of cirrhosis in any ol the patients. One child was lost tofollow-up after two weeks. All hematological and biochemicalinvestigations were normal at the two-week check-up. Jaundicehad resolved in all three children who had initially presentedwith hyperbilirubinemia. A Tc HIDA scan was done in three pa-tients operated for choledochal cyst excision with interpositionof the appendix three months after surgery which showed a nor-mal length and caliber of the duct with free flow of the contrastinto the duodenum and no evidence of reflux. Follow-up HIDAscans could not be carried out in all patients because ofeconomicrestraints, but the lack of clinical evidence of cholangitis or jaun-dice eliminated the possibility of reflux or strictures and ensureda free flow ofbile. Repeat ultrasound scans done on a yearly basisshowed no dilatation of the intrahepatic biliary tree or changesofportal vasculature.
We had no febrile episodes to suggest cholangitis in the twoyears of follow-up of our patients. Currently all five patients infollow-up are free ofjaundice.
Shah AA, Shah AV. Appendix as a Biliary ... Eur I pediatr Surg 2005; t5: 128 - 131

Fig.2 Picture show'ing the appendix (A)
placed between thecommon bile ductand the 2nd part ofthe duodenum (D).
Fig.1 Picture showing the mobilized appendlx preservlng tne vascu-
lar pedicle (A).
Discussion
An ideal biliary conduit is one that should allow a free flow of bile
from the liver to the duodenum, without allowing reflux of any
intestinal contents back into the biliary tree. Though the jejunal
loop is well known and effective, it has its own drawbacks'
Cholangitis is one of the main problems that the surgeons have to
face in these patients. As many as 50 % of patients who have been
operated for Biliary Atresia, and about 46% ofpatients operated
for biliary reconstruction after resection of choledochal cysts
have episodes of cholangitis. This high incidence has prompted
various modifications ofthejejunal grafts to prevent reflux' e'g'
using interposition grafts, intussuscepted ileocolic interposition
grafi 1t,+,t01, jejunal nipple valve [3,10,15], mucosal flap valve
irOl, ana sphincter of Oddi valve [13], but in spite of all these
modifications the incidence of cholangitis remains significant'
Jejunal loop has its own disadvantages, i.e' the use of a wide loop
thatmaynecessitatetailoring,stricturesatthesiteofanastomo-sis, and loss ofa longjejunal loop out ofthe intestinal circuit'
The use of the appendix, on the other hand, is well suited as a
biliary conduit. The procurement of the appendix is simple and
direct. The conical base and the tapering tip are well suited for
biliary replacement. The small caliber, well-vascularized tube
can be anastomosed to the duodenum using a nonrefluxing tun-
nel. The bile is directed into the duodenum, which is a physir
logical area for the intestinal and biliary contents to be mixed'
We used prophylactic antibiotics for up to six weeks after su
gery. O'Neill [14] suggests that the chances of postoperative chc
ingitis diminish six weeks after surgery' Decreased incidence
poitoperative cholangitis as suggested by Gupta et al' [8] wh(
itre appenaix was used as a biliary conduit was possibly due
the role played by the presence of lymphoid follicles in the w;
of the appendix.
Grosfeld et al. [7] first reported the use of an appendiceal gri
for biliary reconstruction in mongrel dogs' Greenholz et al' I
performed an ancillary appendiceal conduit to provide bilia
irainage of an independent bile duct' Crombleholme et al' ha
used this technique successfully in patients with biliary atrel
and choledochal cyst [21. The appendix has also been used ar
ureteral conduit and long-term patency and function has be
documented for as long as 11 years postoperatively [18]' Our i
tial experiences with the use of the appendix as a bilioente
mobilized appendix preserving the vascu-
Table 1 Patient details
Patientno. Ageinmonths
rl: :::r:l i:r,l,'l',:]:tl:6rl..ii.::t l'r:l::
25:.13.''a:'].;.:i:i:'t;r..]rei::].
44
Prcsentation LFf ot 6 weekspost op.
Follow-up
HIDA - Normal
Lost to follow-uP
r:tiijiritri.ti:]ii,i.trt tti,li9riiri':i $6 7112 Male lncidental
USG - Normal
Shah AA, Shah AV. Appendix as a Biliary "' Eurl Pediatr Surg 2005: 15: 128-131

ii
conduit in children with choledochal cyst seem to be promisingand long-term follow-up of these children would be interesting.
References
1 Chiba T. Bile duct reconstruction with an ileocaecal intestinal graft toprevent postoperative ascending cholangitis. Jpn J Soc Pediatr Surg1974: 1,0: 611 - 618
2 Crombleholme TM, Harrison MR, Langer JC et al. Biliary appendico-duodenostomy: A nonrefluxing conduit for biliary reconstruction.
J Pediatr Surg 1989; 24: 665 - 6673 Donahoe PI(, Hendren WH. Roux-en-Y on line intussusception to void
ascending cholangitis in biliary atreisa. Arch Surg 1983; 118: 1091 -1094
a Endo M, I(atsumata K, Yokoyama J et al. Extended dissection of theportahepatis and creation of an intussuscepted ileo-colic conduit forbiliary atresia.J Pediatr Surg 1983; 18: 784-793
s Freund H, BerlotzkyY, SchillerM. The ileocaecal segment: An anti-re-flux conduit for hepatic portoenterostomy. J Pediatr Surg 1979; 14:
169 -17'-16 Greenholz SK, LillyJR, Shikes RH et al. Biliary atresia in the newborn.
J Pediatr Surg 1986; 21:1147 -11.48
7 GrosfeldJL, Weinberger M, Clatworthy HW. Vascularized appendicealtransplants in biliary and urinary tract replacement. J Pediatr Surg1971,: 6: 630 - 638
8 Gupta DI(, Rohatgi M. Use of appendix in biliary atresia. Indian J Pe-diarr 1989; 56:479-482
e Kasai M, Kimura S, Asakura Y et al. Surgical treatment of biliary atre-sia. J Pediatr Surg 1968; 3: 665 - 675
10 Kaufman BH, Luck SR, Raffensperger JG. The evolution of a valvedhepato-duodenal-intestinal conduit. J Pediatr Surg 1981; 16:.279-283
11 Lilly JR, Altman RP. Hepatic portoenterostomy (the I(asai operation)for biliary atresia. Surgery 1975;78:76-BG
l'z Lilly JR, I(arrer FM. Contemporary surgery for biliary atresia. PediatrClin NorthAm 1985; 32: 1233-1246
13 Lilly JR, Stenllin G. Catheter decompression of hepatic portocholecys-tostomy. J Pediatr Surg 1982: '17:904 - 950
1a o'Neill JA. Choledochal cyst. Curr Probl Surg 1992; 29: 361. - 41015 Reynolds M, Luck SR, Raffensperger JG. The valved conduit prevents
ascending cholangitis: A follow-up.J Pediatr Surg 1985; 20:696-70216 Shin WI(T, ZhangJZ. Antirefluxing Roux-en-Y biliary drainage for hep-
atic portoenterostomy: Animal experiments and clinical experience.
J Pediatr Surg 1985; 20: 689-69217 Suruga I(, I(omo S, Miyano T et al. Treatment of biliary atresia: Micro-
surgery for hepatic porto-enterostomy. Surgery 1976; B0: 558-56218 Weinberg RW. Appendix ureteroplasty. BrJ Urol 1976:48:234
Shah AA, Shah AV. Appendix as a Biliary ... Eur I Pediatr Surg 2005; 15: 128 - 131