Chapter 20: The Heart Primary sources for figures and content: Marieb, E. N. Human Anatomy &...
120
Chapter 20: The Heart Primary sources for figures and content: Marieb, E. N. Human Anatomy & Physiology. 6 th ed. San Francisco: Pearson Benjamin Cummings, 2004. Martini, F. H. Fundamentals of Anatomy & Physiology. 6 th ed. San Francisco: Pearson Benjamin Cummings, 2004.
-
Upload
maryann-lyons -
Category
Documents
-
view
221 -
download
1
Transcript of Chapter 20: The Heart Primary sources for figures and content: Marieb, E. N. Human Anatomy &...

Chapter 20:
The Heart
Primary sources for figures and content:
Marieb, E. N. Human Anatomy & Physiology. 6th ed. San Francisco: Pearson Benjamin Cummings, 2004.
Martini, F. H. Fundamentals of Anatomy & Physiology. 6th ed. San Francisco: Pearson Benjamin Cummings, 2004.

The cardiovascular system and heart.

Figure 20–1
The Cardiovascular System
The Cardiovascular System
• Pulmonary circuit:– Carries blood to and from gas
exchange surfaces of lungs– Right ventricle lungs left atrium
• Systemic circuit:– Carries blood to and from the body– Left ventricle body right atrium

3 Types of Blood Vessels
• Arteries:– carry blood away from heart
• Veins:– carry blood to heart
• Capillaries (exchange vessels):– networks between arteries and veins– Exchange materials between blood and tissues– Dissolved gases, nutrients, wastes

The heart and its general features.

Anatomy of the Heart
• Located directly behind sternum
Figure 20–2a

The Heart• Location:
– Left of midline, between 2nd rib and 5th intercostal space– posterior to sternum, in pericardial cavity in
mediastinum• Heart is fist sized, < 1 lb• Beats 100,000 times/day moving 8,000 Liters blood/day• Surrounded by pericardium:
– serous and fibrous layers• Serous membranes: visceral and parietal
– secrete pericardial fluid, reduce friction

The Heart
1. Pericarditis– Inflammation of pericardium, usually
due to infection– Causes friction
2. Cardiac tamponade– Buildup of fluid in pericardial space– Restricts heart movement
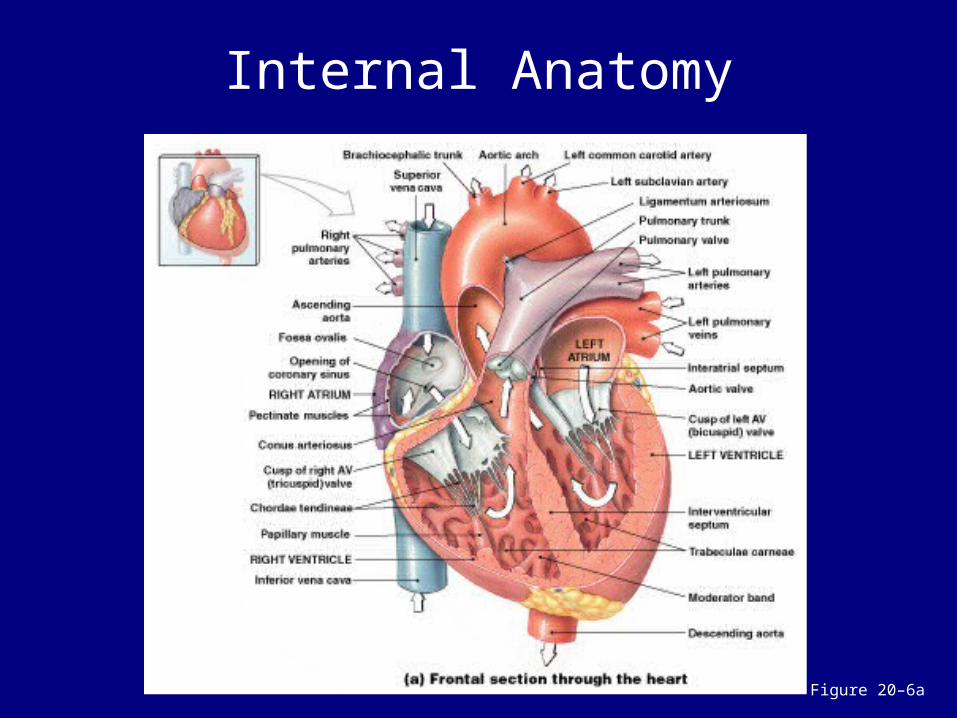
Internal Anatomy
Figure 20–6a

4 Chambers of the Heart
• 2 for each circuit:– left and right: 2 ventricles and 2 atria
2 Atria– Superior, thin walls– Smooth posterior walls internally– Pectinate muscles (ridges) anteriorly– has expandable flap called an auricle lateral
and superior – Left and right separated by interatrial septum

2 Ventricles– Inferior, thick walls, lined with
trabeculae carneae (muscular ridges)– Left and right separated by
interventricular septum– Left ventricle 3x thicker, 5x more
friction while pumping, same volume as right• WHY?
– Left is round, right is crescent
4 Chambers of the Heart

Left and Right Ventricles
• Have significant structural differences
Figure 20–7

The Left Ventricle
• Systemic circulation:– blood leaves left ventricle through
aortic valve into ascending aorta– ascending aorta aortic arch

4 Chambers of the Heart
• Right atrium:– collects blood from systemic circuit
• Right ventricle:– pumps blood to pulmonary circuit
• Left atrium:– collects blood from pulmonary circuit
• Left ventricle:– pumps blood to systemic circuit

Relation to Thoracic Cavity
Figure 20–2b

Figure 20–2c
The Heart:External Divisions
• Great veins and arteries at the base• Pointed tip is apex

2 Layers of Pericardium
1. Parietal pericardium:– outer layer
2. Visceral pericardium:– inner layer of pericardium

Superficial Anatomy of the Heart
Figure 20–3

Sulci
• Coronary sulcus:– divides atria and ventricles
• Anterior and posterior interventricular sulci:– separate left and right ventricles– contain blood vessels of cardiac
muscle

The layers of the heart wall.

The Heart Wall
Figure 20–4

3 Layers of the Heart Wall
1. Epicardium (thin): outer layer– Visceral pericardium: serous membrane
•Loose CT attached to myocardium 2. Myocardium (thick): middle layer
– Cardiac muscle tissue with CT, vessels, and nerves
3. Endocardium (thin): inner layer– Simple squamous epithelium lining with basal
lamina– Continuous with endothelium blood vessesl

Cardiac Muscle Cells
Figure 20–5

Cardiac Muscle Tissue
• Muscle cells = cardiocytes• Uses actin and myosin sliding filaments to contract• Rich in mitochondria, resists fatigue but dependent
on aerobic respiration• Cells connected by intercalated discs• Contraction is all or none• Longer contractile phase than skeletal muscle• Fibrous skeleton of the heart (tough CT) acts as the
tendon

Cardiac Muscle Cells
• Intercalated discs:– interconnect cardiac muscle cells– secured by desmosomes – linked by gap junctions– convey force of contraction – propagate action potentials
The path of blood flow through the heart, and
the major blood vessels, chambers, and heart
valves.

Internal Anatomy
Figure 20–6a

The Vena Cava
• Delivers systemic circulation to right atrium
• Superior vena cava:– receives blood from head, neck,
upper limbs, and chest• Inferior vena cava:
– receives blood from trunk, and viscera, lower limbs

The Heart Valves
• One-way valves prevent backflow during contraction
Figure 20–8

Atrioventricular (AV) Valves
• Connect atria to ventricles • Permit blood flow in 1 direction:
– atria to ventricles
• Flaps = cusps• Pressure closes valve cusps during
ventricular contraction1.Tricuspid valve: right side, 3 cusps2.Bicuspid/Mitral valve: left side, 2 cusps

• Cusps attached to chordae tendineae from papillary muscles on ventricle wall
• Contraction of papillary muscles prevent cusps opening backward during ventricle contraction– Prevent back flow
• Cusps hang loose when ventricles not contraction, allow ventricles to fill with blood
Cusps
Semilunar Valves
• Between ventricles and arteries• 3 cusps• No chordae tendineae or muscles• Forced open by blood from
ventricular contraction• Snap closed to prevent backflow

Heart Disorders
1. Valvular heart disease- Valve function deteriorates to extent that heart
cannot maintain adequate circulation- Rheumatic fever: childhood reaction to
streptococcal infection, chronic carditis, VHD in adult
2. Heart murmur- Leaky valve - Mitral valve prolapse: murmur of left AV valve,
cusps don’t close properly, blood regurgitates back into left atrium

3. Congestive heart failure– Decreased pumping efficiency
• Diseased valves, damaged muscle
– Blood backs up fluid leaks from vessels and collects in lungs and tissues
Heart Disorders

Blood Flow Through the Heart

The Pulmonary Circuit
• Pulmonary trunk divides into left and right pulmonary arteries
• Blood flows from right ventricle to pulmonary trunk through pulmonary semilunar valve

Return from Pulmonary Circuit
• Blood from the lungs gathers into left and right pulmonary veins
• Pulmonary veins deliver to left atrium
• Blood from left atrium passes to left ventricle through left atrioventricular (AV) valve (bicuspid valve or mitral valve)
Damage to the semilunar valve on the right side of the heart would affect blood flow
to which vessel?
A. aortaB. superior vena cavaC. pulmonary arteryD. coronary artery

What prevents the AV valves from opening back into the
atria?
A. papillary musclesB. valve cuspsC. moderator bandD. chordae tendineae

Why is the left ventricle more muscular than the right
ventricle?
A. Because it must pump a larger volume.
B. Because it must generate more force.
C. Because it must open a tighter atrioventricular valve.
D. Both A and B are correct.

Fetal Heart: Adapted to bypass lungs

Foramen Ovale
• Before birth, is an opening through interatrial septum in the right atrium
• Connects the 2 atria• ~25% of blood bypasses directly the left
atrium• Closes at birth leaving scar called fossa
ovalis

Ductus arteriosus
• Connects pulmonary trunk to aorta• ~90% of blood bypasses lungs• Closes at birth leaving the ligamentum
arteriosum
Failure of either to close = poor oxygenation of blood, cyanosis, “blue baby syndrome”

KEY CONCEPT• The heart has 4 chambers:
– 2 for pulmonary circuit:• right atrium and right ventricle
– 2 for systemic circuit:•left atrium and left ventricle
• Left ventricle has a greater workload– more massive than right ventricle, but the two chambers pump
equal amounts of blood
• AV valves prevent backflow from ventricles into atria• Semilunar valves prevent backflow from aortic and
pulmonary trunks into ventricles

Blood supply to the heart.

Blood Supply to the Heart• Coronary circulation
Figure 20–9

Coronary Circulation
• Coronary arteries and cardiac veins• Supplies blood to muscle tissue of heart• Heart = <1% body mass, requires 5% of blood• Too thick for diffusion• Coronary arteries
– originate at base of ascending aorta– branch to capillary beds for diffusion
• Blood returns via cardiac veins – Cardiac veins empty into right atrium

Right Coronary Artery
• Supplies blood to:– right atrium– portions of both ventricles– cells of sinoatrial (SA) and
atrioventricular nodes – marginal arteries
• surface of right ventricle

Left Coronary Artery
• Supplies blood to:– left ventricle– left atrium– interventricular septum

Coronary artery disease
• Partial or complete block of coronary circulation, results in coronary ischemia
• Can lead to myocardial infraction (heart attack)– Heart tissue denied oxygen dies
• Common symptom– Angina pectoralis:
• plan in the chest, especially during activity, as a result of ischemia

Coronary bypass surgery
• Use healthy veins (from legs) to create anatomoses around blockages
• Most people have 4 major coronary arteries “quadruple bypass”

Figure 20–11
The Cardiac Cycle

The Heartbeat• A single contraction of the heart• 1% myocardial cells autorhythmic
– Depolarize without neural or endocrine stimulation
• Depolarization transmitted to other myocardial cells through cardiac conduction system1.Sinoatrial (SA) node2.Atrioventricular (AV) node3.Conducting cells

Structures of the Conducting System
1. SA node:– Right atrium wall near superior vena
cava
2. AV node: – Inferior portion of interatrial septum
above tricuspid valve

3. Conducting cells: – controls and coordinates heartbeat– In the atrium:
• Interconnect SA and AV nodes
– Connect nodes and myocardium– Distribute stimulus through myocardium
• Run down interventricular septum and around apex
– In the ventricles: AV bundle, bundle branches and Purkinji fibers
Structures of the Conducting System
The Cardiac Cycle
• Begins with action potential at SA node– gradually depolarizes toward threshold– transmitted through conducting system– produces action potentials in cardiac muscle
cells (contractile cells)
• SA node Also called pacemaker potential• SA node depolarizes first, establishing
heart rate

Figure 20–12
• Cells of nodes cannot maintain resting membrane potential, drift to depolarization:– SA node: 80-100 action potentials/min
•“natural pacemaker”– AV node: 40-60 action potentials/min
• Resting rate (sinus rhythm) – ~75 bpm set by SA node + parasympathetic stimulation

Figure 20–12
The Conducting System
The components and functions of the
conducting system of the heart.

Figure 20–13
Impulse Conduction through the Heart

The Sinoatrial (SA) Node
• In posterior wall of right atrium• Contains pacemaker cells• Connected to AV node by
internodal pathways• Begins atrial activation (Step 1)

The Atrioventricular (AV) Node
• In floor of right atrium• Receives impulse from SA node
(Step 2)• Delays impulse (Step 3)• Atrial contraction begins

The AV Bundle
• In the septum• Carries impulse to left and right
bundle branches:– which conduct to Purkinje fibers (Step
4)
• And to the moderator band:– which conducts to papillary muscles

4. The Purkinje Fibers
• Distribute impulse through ventricles (Step 5)
• Atrial contraction is completed• Ventricular contraction begins
Total time = ~370 ms

Abnormal Pacemaker Function
• Normal average heart rate = ~70-80 bpm– Max = ~230 bpm, but inefficient above 180
1. Bradycardia: <60 bpm– abnormally slow heart rate
2. Tachycardia: >100 bpm– abnormally fast heart rate

If the cells of the SA node failed to function, how would the heart rate be affected?
A. It would be faster.B. It would be slower.C. It would be irregular.D. It would not change.

In a person with bradycardia, is cardiac output likely to be
greater than or less than normal?
A. greater than normalB. less than normal

Why is it important for impulses from the atria to be delayed at
the AV node before they pass into the ventricles?
A. to prevent backflow of atrial blood
B. to allow complete ventricular contraction
C. to allow complete atrial emptying
D. to create more forceful ventricular contraction
The electrical events that are associated with a
normal electrocardiogram (EKG).

The Electrocardiogram
Figure 20–14b

Electrocardiogram (ECG or EKG)
• A recording of electrical events in the heart
• Obtained by electrodes at specific body locations
• Abnormal patterns diagnose damage

Features of an ECG
• P wave: atria depolarize– Depolarization wave from SA node through
atria ~80ms• QRS complex: ventricles depolarize– Atrial repolarization and ventricle
depolarization ~80ms
• T wave:– Ventricle repolarization ~160ms

Time Intervals & Diagnosis of Heart Problems
• P–R interval:– from start of atrial depolarization, to start of
QRS complex– P-R longer than 200 ms = damage to AV
node or conducting cells•Total heart block =
– Cause = damage AV node, – Effect = no impulses transmitted
through, atria and ventricles beat independently (atria fast, ventricles slow)

• Q–T interval:– from ventricular depolarization, to
ventricular repolarization– Longer than 380 ms = coronary
ischemia or myocardial damage
Time Intervals & Diagnosis of Heart Problems

EKG used to diagnose heart problems
1. Cardiac Arrhythmias– Abnormal patterns of cardiac electrical
activity
2. Fibrillation– Rapid, irregular, out of phase
contractions due to activity in areas other than SA node
– Defibrillation to stop all activity so SA node can resume control

KEY CONCEPT
• Heart rate is normally established by cells of SA node
• Rate can be modified by autonomic activity, hormones, and other factors
• From the SA node, stimulus is conducted to AV node, AV bundle, bundle branches, and Purkinje fibers before reaching ventricular muscle cells
• Electrical events associated with the heartbeat can be monitored in an electrocardiogram (ECG)

The events that take place during an action
potential in cardiac muscle.

Contractile Cells
• Purkinje fibers distribute the stimulus to the contractile cells, which make up most of the muscle cells in the heart

Action Potentials in Skeletal and Cardiac Muscle
Figure 20–15

The events that take place
during the cardiac cycle, including atrial and
ventricular systole and diastole.

The Cardiac Cycle
• The period between the start of 1 heartbeat and the beginning of the next
• Alternation contraction and relaxation

2 Phases of the Cardiac Cycle
• Within any 1 chamber:– systole (contraction)
• Contraction• High pressure • Blood gets pushed to next chamber
– diastole (relaxation)• Relaxation• Low pressure• Chamber fills with blood

Blood Flow
• Blood flows from high to low pressure:– controlled by timing of contractions– directed by one-way valves

Phases of the Cardiac Cycle
Figure 20–16

4 Phases of the Cardiac Cycle
1. Atrial systole2. Atrial diastole3. Ventricular systole 4. Ventricular diastole

Cardiac Cycle and Heart Rate
• At 75 beats per minute:– cardiac cycle lasts about 800 msecs
• When heart rate increases:– all phases of cardiac cycle shorten,
particularly diastole

Cardiac Cycle: Pressure and Volume
Figure 20–17

8 Steps in the Cardiac Cycle
1. Atrial systole begins: – atrial contraction begins– right and left AV valves are open
2. Atria eject blood into ventricles:– filling ventricles
3. Atrial systole ends: – AV valves close– ventricles contain maximum volume

8 Steps in the Cardiac Cycle
4. Ventricular systole: 1st phase– ventricular contraction– pressure in ventricles rises– AV valves shut
5. Ventricular systole (ejection): 2nd phase – Pressure in ventricle rises and exceeds
pressure in the arteries– semilunar valves open– blood flows into pulmonary and aortic trunks

8 Steps in the Cardiac Cycle
6. Ventricular pressure falls:– semilunar valves close
7. Ventricular diastole: – At start ventricular pressure is
higher than atrial pressure and all heart valves are closed
– Then ventricles relax

8 Steps in the Cardiac Cycle 8. Ventricular diastole: Atrial pressure is higher
than ventricular pressure– AV valves open– Blood fills the relaxed atria
• Atria contraction only adds ~30% more to ventricles (can live with bad atria)
– cardiac cycle ends
Incr. heart rate decr. cycle time, decr. diastole time decr. time to fill

Heart sounds relate to specific events
in the cardiac cycle.

Heart Sounds
Figure 20–18b

Heart Sounds
• S1: “lubb”– produced by AV valves closing at start of
ventricular systole
• S2: “dubb”– produced by semilunar valves closing at
start of ventricular diastole
• S3, S4:– soft sounds– blood flow into ventricles and atrial
contraction

Cardiac output and the factors that
influence it.
Cardiodynamics
• The movement and force generated by cardiac contractions
• CO = cardiac output– Amount of blood pumped by each
ventricle in one minute, depends on heart rate and stroke volume
– CO = HR x SV

Important Cardiodynamics Terms
• End-diastolic volume (EDV) ~ 120 ml– Volume of blood in ventricle before contraction
• End-systolic volume (ESV) ~ 50 ml– Volume of blood in ventricle following a beat– Typically 50 ml
• Stroke volume (SV): ~ 70 ml– Amount of blood pumped by ventricle
SV = EDV — ESVUsually SV is constant, you need to change HR to
increase CO as needed.

Stroke Volume• Volume (ml) of blood ejected per
beat
Figure 20–19

Cardiac Output
• Cardiac output (CO) ml/min = • Heart rate (HR) beats/min • Stroke volume (SV) ml/beat

Heart rate effectors.
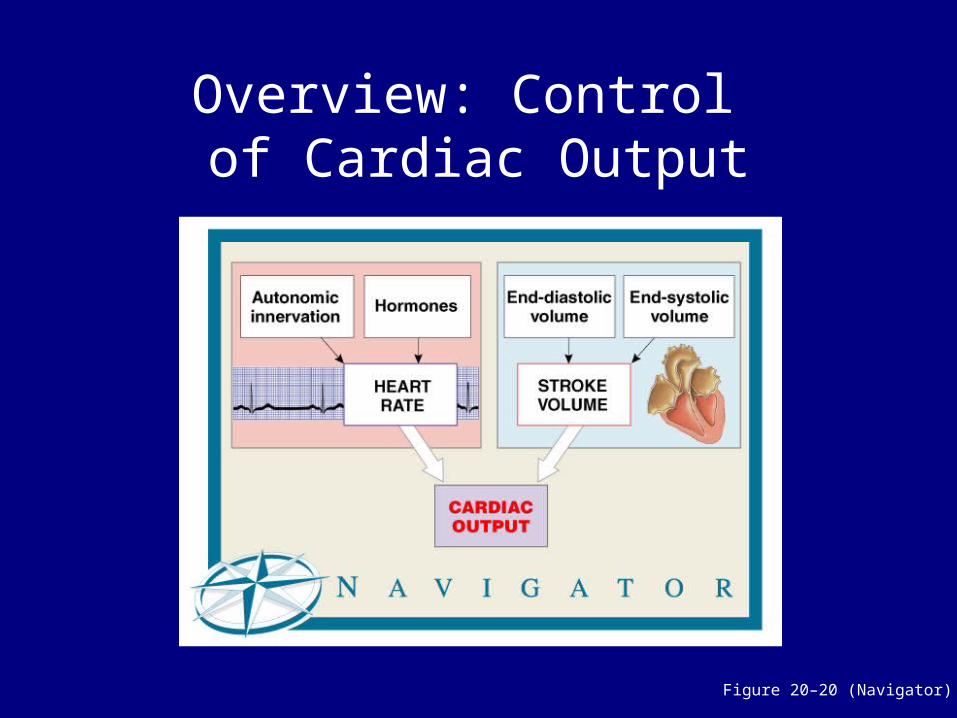
Overview: Control of Cardiac Output
Figure 20–20 (Navigator)
HR affected by:1. Autonomic nervous input
– Parasympathetic stimulation•slows the heart
– Sympathetic stimulation•speeds the heart
2. Hormones3. Venous return
– More blood return = incr. HR– Stretch receptors in right atrium
•trigger incr. heart rate through incr. sympathetic activity4. Other factors: ions, drugs

Cardiac Output
• At 160-180 bpm CO is at max:– Incr. HR decr. time to fill ventricles– If ventricle is not full decr. SV and CO
• Conditioning can incr. SV and decr. HR• Fit athletes can
– incr. max CO by 700%– decr. resting HR by 50% with same CO
due to incr. SV

Variables that influence stroke volume and heart
rate effectors.

Heart Rate Effectors
1. Autonomic Innervations– SA node, AV node and atrial myocardium
innervated by both sympathetic (NE) and parasympathetic (Ach) nerve fibers equally
– Sympathetic dominated in ventricles– Cardiac centers in medulla oblongata monitor
blood pressure and gasses to adjust HR•A) Cardioacceleratory center – sympathetic•B) Cardioinhibitory center - parasympathetic
Heart Rate Effectors
1. Autonomic Innervations– Parasympathetic tone reduce rate of SA node
•72-80 bpm females•64-72 bpm males•40 bpm athletes
2. Hormones– Epinephrine, Norepinephrine, thyroxine all
increase HR by acting at SA node– Beta blockers: treats hypertension
•Blocks B-receptors for E/NE thus preventing sympathetic stimulation

Other Heart Rate Effectors
• Caffeine– Rapid depolarization of SA node, incr. HR
• Nicotine– Stimulates sympathetic neurons, incr. HR
• Hyperkalemia– High K+, inhibits repolarization– Beats week, heart can stop

Other Heart Rate Effectors
• Hypercalcemia– High Ca+ – Muscle cells excitable, incr. HR– Can cause prolonged contraction heart seizes
• Hypocalcemia– Low Ca+– Contractions weak heart can stop
• Temperature– Affects metabolic rate of cardiocytes– High temp incr. HR– Low temp decr. HR

What effect does drinking large amounts of caffeinated
drinks have on the heart?
A. increased heart rateB. decreased heart rateC. erratic heart rateD. bradycardia

If the cardioinhibitory center of the medulla oblongata were damaged,
which part of the autonomic nervous system would be affected,
and how would the heart be influenced?
A. parasympathetic; increased heart rate
B. parasympathetic; decreased heart rate
C. sympathetic; increased heart rate
D. sympathetic; decreased heart rate
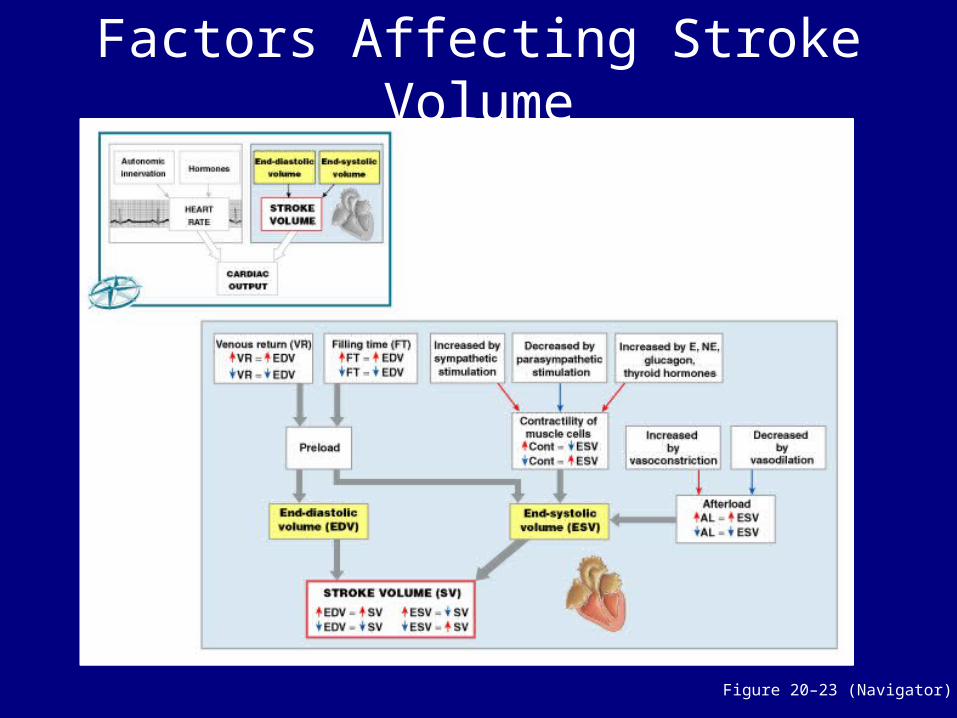
Factors Affecting Stroke Volume
Figure 20–23 (Navigator)

Factors Affecting Heart Rate and Stroke Volume
Figure 20–24

KEY CONCEPT
• Cardiac output:– the amount of blood pumped by the
left ventricle each minute– adjusted by the ANS in response to:
• circulating hormones• changes in blood volume • alterations in venous return

What effect would stimulating the
acetylcholine receptors of the heart have on cardiac
output?A. It would increase cardiac
output.B. It would decrease cardiac
output.C. It would cause erratic
cardiac output.D. It would have no effect.

What effect would an increase in venous return
have on the stroke volume?
A. It would increase stroke volume.
B. It would decrease stroke volume.
C. It would cause erratic stroke volume.
D. It would have no effect.

Joe’s end-systolic volume is 40 ml, and his end-diastolic
volume is 125 ml. What is Joe’s stroke volume?
A. 165 mlB. 155 mlC. 85 mlD. 100 ml
SUMMARY• Organization of cardiovascular system:
– pulmonary and systemic circuits• 3 types of blood vessels:
– arteries, veins, and capillaries• 4 chambers of the heart:
– left and right atria– left and right ventricles
• Pericardium, mediastinum, and pericardial sac• Coronary sulcus and superficial anatomy of the heart• Structures and cells of the heart wall
SUMMARY
• Internal anatomy and structures of the heart:– septa, muscles, and blood vessels
• Valves of the heart and direction of blood flow• Connective tissues of the heart• Coronary blood supply• Contractile cells and the conducting system:
– pacemaker calls, nodes, bundles, and Purkinje fibers

SUMMARY
• Electrocardiogram and its wave forms• Refractory period of cardiac cells• Cardiac cycle:
– atrial and ventricular– systole and diastole
• Cardiodynamics:– stroke volume and cardiac output
• Control of cardiac output