Cardiovascular Patho 1 Ogena

of 87
-
Upload
quolette-constante -
Category
Documents
-
view
220 -
download
0
Transcript of Cardiovascular Patho 1 Ogena
-
8/14/2019 Cardiovascular Patho 1 Ogena
1/87
Cardiovascula
r System
-
8/14/2019 Cardiovascular Patho 1 Ogena
2/87
Pathophysiologic
Concepts
-
8/14/2019 Cardiovascular Patho 1 Ogena
3/87
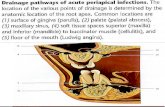
Thrombus
A thrombus
a blood clot that can develop
anywhere in the vascular system causing the narrowing of a vessel.
blood flow can be occluded
(reduced or totally blocked)
-
8/14/2019 Cardiovascular Patho 1 Ogena
4/87
Thrombus develop from any injury to the vessel wall
endothelial cell injury draws platelets and other
mediators of inflammation to the area.
substances stimulate clotting and activation of the
coagulation cascade.
formation can occur when blood flow through a vessel
is sluggish,
when blood flow is irregular or erratic
during periods of irregular heartbeat or cardiac arrest
-
8/14/2019 Cardiovascular Patho 1 Ogena
5/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
6/87
Thrombus
-
8/14/2019 Cardiovascular Patho 1 Ogena
7/87
Embolus
Embolus
a substance that travels in the
bloodstream from a primary site to a
secondary site becomes trapped in the vessels at the
secondary site
causes blood flow obstruction.
Most emboli are blood clots
(thromboemboli)
usually deep leg veins
-
8/14/2019 Cardiovascular Patho 1 Ogena
8/87
Other sources of emboli fat
released during the break of a long bone
produced in response to any physical trauma, and
amniotic fluid
which may enter maternal circulation during the
intense pressure gradients generated by labor
contractions.
Air and displaced tumor cells also may act as emboli to
obstruct flow.
Embolus
-
8/14/2019 Cardiovascular Patho 1 Ogena
9/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
10/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
11/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
12/87
Aneurysm Aneurysm
is a dilation of the arterial wall caused by a
congenital or developed weakness in the wall.
Weakness in the wall may develop as a result of an
infection, from trauma, or, more commonly, from
lesions produced by atherosclerosis.
Aneurysms may burst with increased pressure,
leading to massive internal hemorrhage.
-
8/14/2019 Cardiovascular Patho 1 Ogena
13/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
14/87
Alterations in Capillary Forces
of Filtration or Reabsorption
Occasionally, forces favoring filtration
from the capillary into the interstitial
fluid are greater than forces favoring
reabsorption of fluid into the capillaryfrom the interstitial space.
The result is net filtration.
Net filtration across the capillary
results in interstitial edema.
-
8/14/2019 Cardiovascular Patho 1 Ogena
15/87
Alterations in Capillary Forces of
Filtration or Reabsorption
The opposite occurs when forces favoring
reabsorption of fluid from the interstitial
space into the capillary are greater than
those favoring filtration. This results in net reabsorption, which
leads to increased plasma volume, stroke
volume, and cardiac output.
Blood pressure may be increasedsignificantly.
-
8/14/2019 Cardiovascular Patho 1 Ogena
16/87
Causes of Increased Capillary
Filtration
Causes of increased capillary filtration include
increased capillary pressure
caused by high blood pressure
increased capillary leakage
caused by injury or inflammation. increase in protein concentration in the
interstitial fluid
caused by increased capillary breakdown
decreased lymph flow to the area would
also cause net filtration, leading to edemaand swelling of the interstitial space.
-
8/14/2019 Cardiovascular Patho 1 Ogena
17/87
Causes of Increased
Capillary Filtration
Causes of increased capillary filtration
include
decreased production or increased
loss of plasma proteins
reduce the reabsorption of fluid
back into the capillary.
can occur with liver disease orloss of protein in the urine.
-
8/14/2019 Cardiovascular Patho 1 Ogena
18/87
Causes of Increased
Capillary Reabsorption Causes of increased
reabsorption of fluid from theinterstitial space include
decreased blood pressure inthe capillary due to a decrease in
systemic pressure or
constriction of the arterioleor precapillary sphincter.
-
8/14/2019 Cardiovascular Patho 1 Ogena
19/87
Increased plasma colloid osmotic pressurealso draws fluid back into the capillary.
Plasma colloid osmotic pressure increaseswith dehydration, leading to a return of fluid
from the interstitium to the plasma, whichhelps return plasma volume toward normal.
Finally, increased interstitial fluid pressureincreases reabsorption by opposing furtheraccumulation of fluid.
-
8/14/2019 Cardiovascular Patho 1 Ogena
20/87
Stenosis
Stenosis
a narrowing of any vessel or opening.
stenosis of the heart valves may
occur.
congenital defect or an inflammatory
process (e.g., after rheumatic fever).
-
8/14/2019 Cardiovascular Patho 1 Ogena
21/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
22/87
Results of Cardiac Valve
Stenosis
chamber upstream of the stenosispumping more forcefully to expel itsblood through the narrowed orifice.
After years of this extra work,cardiac muscle can hypertrophy(increase in size).
If the chamber cannot pump
forcefully enough to overcome thestenosis, blood flow out of thechamber will be reduced.
-
8/14/2019 Cardiovascular Patho 1 Ogena
23/87
Results of Cardiac Valve
Stenosis
chamber increases its oxygenconsumption and energy demands.
The coronary arteries supplying themuscle may be unable to supply adequate
oxygen to meet this demand. blood may accumulate in the chamber
and stretch its muscle fibers.
If this is significant or prolonged, a
decrease in muscle contractility can result.
-
8/14/2019 Cardiovascular Patho 1 Ogena
24/87
Examples of Cardiac Valve Stenosis
Any cardiac valve
Mitral stenosis
narrowing of the valve between the left atriumand left ventricle.
Aortic stenosis
narrowing of the valve between the leftventricle and the aorta.
Tricuspid stenosis
narrowing of the valve between the rightatrium and the right ventricle.
Pulmonary stenosis narrowing of the valve between the right
ventricle and the pulmonary artery.
-
8/14/2019 Cardiovascular Patho 1 Ogena
25/87
Valve Incompetence
An incompetent valve is one that
does not close completely, allowing
blood to move in both directionsthrough that valve when the heart
contracts (valve regurgitation).
Any of the cardiac valves may be
incompetent.
Each chamber may hypertrophy.
-
8/14/2019 Cardiovascular Patho 1 Ogena
26/87
Cardiac Shunts
a shunt is a connection between thepulmonary vascular system and thesystemic vascular system.
During fetal life, shunts between the right
and left sides of the heart and between theaorta and pulmonary artery are normal.
The direction blood flows through a shuntis determined by resistance to flow in eachdirection.
-
8/14/2019 Cardiovascular Patho 1 Ogena
27/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
28/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
29/87
Right-to-Left Shunt
the flow of blood from the right side of theheart to the left, or from the pulmonary arteryto the systemic circulation.
After birth, right heart and pulmonary artery
blood is poorly oxygenated. Therefore, a right-to-left shunt delivers poorly oxygenated bloodto the systemic circulation.
called a cyanotic shunt because delivery of
poorly oxygenated blood to the systemiccirculation causes cyanosis (bluish tinge tothe skin).
-
8/14/2019 Cardiovascular Patho 1 Ogena
30/87
Left-to-Right Shunt
the flow of blood from the left side ofthe heart to the right side, or from theaorta to the pulmonary circulation.
Left heart blood is well oxygenated. Blood going to the lungs from the leftside of the heart recirculates to theleft atrium and left ventricle.
Because the blood is well-oxygenated, this shunt is acyanotic.
-
8/14/2019 Cardiovascular Patho 1 Ogena
31/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
32/87
Two Types of Cardiac Defects
Congenital
Anatomic>abnormal function
Acquired
Disease process
Infection
Autoimmune response
Environmental factors
Familial tendencies
-
8/14/2019 Cardiovascular Patho 1 Ogena
33/87
Causes of CHD
Chromosomal/genetic = 10%-12% Maternal or environmental = 1%-2%
Maternal drug use Fetal alcohol syndrome50% have CHD
Maternal illness Rubella in 1st 7 wks of pregnancy50%
risk of defects including PDA andpulmonary branch stenosis
CMV, toxoplasmosis, other viral
illnesses>> cardiac defects IDMs = 10% risk of CHD (VSD,
cardiomyopathy, TGA most common) Multifactorial = 85%
-
8/14/2019 Cardiovascular Patho 1 Ogena
34/87
CHD
Incidence: 5-8 per 1000 live births About 2-3 of these are symptomatic in first year
of life Major cause of death in first year of life (after
prematurity)
Most common anomaly is VSD 28% of kids with CHD have another recognized
anomaly (trisomy 21, 13, 18, +++ )
-
8/14/2019 Cardiovascular Patho 1 Ogena
35/87
Older Classifications of CHD
Acyanotic
May become cyanotic
Cyanotic May be pink
May develop CHF
-
8/14/2019 Cardiovascular Patho 1 Ogena
36/87
Newer Classification ofCHD
Hemodynamic characteristics
Increased pulmonary blood
flow
Decreased pulmonary blood
flow
Obstruction of blood flow out
of the heart
Mixed blood flow
-
8/14/2019 Cardiovascular Patho 1 Ogena
37/87
Increased Pulmonary
Blood Flow Defects
Abnormal connection between
two sides of heart
Either the septum or the great
vessels
Increased blood volume on
right side of heart
Increased pulmonary blood flow
Decreased systemic blood flow
-
8/14/2019 Cardiovascular Patho 1 Ogena
38/87
Increased Pulmonary
Blood Flow Defects
Atrial septal defect
Ventricular septal defect
Patent ductus arteriosus
-
8/14/2019 Cardiovascular Patho 1 Ogena
39/87
ATRIAL SEPTAL DEFECT (ASD)
Abnormal opening between the atria
an abnormal opening between the left and
right atria.
foramen ovale fails to close after birth, or
when another opening between the left
and right atria is present due to improper
closure of the wall between the two atria
during gestation.
-
8/14/2019 Cardiovascular Patho 1 Ogena
40/87
PATHOPHYSIOLOGY
Blood flows from left to the
right
Increase flow of oxygenated
blood nto the right side of the
heart
-
8/14/2019 Cardiovascular Patho 1 Ogena
41/87
ASD
-
8/14/2019 Cardiovascular Patho 1 Ogena
42/87
CLINICAL MANIFESTATIONS
Asymptomatic
May develop congestive heart
failure Murmur
Atrial dysrhythmias
-
8/14/2019 Cardiovascular Patho 1 Ogena
43/87
VENTRICULAR SEPTAL
DEFECT (VSD)
Abnormal opening between
right and left ventricle
the most common cardiac
congenital defect
May close spontaneously : 1st
year of life
-
8/14/2019 Cardiovascular Patho 1 Ogena
44/87
VSD
-
8/14/2019 Cardiovascular Patho 1 Ogena
45/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
46/87
PATHOPHYSIOLOGY
Blood flow from higher pressure
left ventricle to low pressure
right ventricle
Increased blood volume is
pumped into the lungs
Right ventricular hypertrophy
-
8/14/2019 Cardiovascular Patho 1 Ogena
47/87
CLINICAL MANIFESTATIONS
Murmur
Congestive heart failure iscommon
C S
-
8/14/2019 Cardiovascular Patho 1 Ogena
48/87
PATENT DUCTUSARTERIOSUS
Failure of the fetal ductus
arteriosus (artery connecting
aorta and pulmonary artery) to
close within the first weeks oflife
-
8/14/2019 Cardiovascular Patho 1 Ogena
49/87
PATHOPHYSIOLOGY
Blood flow from high pressure
aorta to lower pressure pulmonary
artery Increased workload on the left side
of the heart
Hypertrophy
-
8/14/2019 Cardiovascular Patho 1 Ogena
50/87
PDA
-
8/14/2019 Cardiovascular Patho 1 Ogena
51/87
CLINICAL
MANIFESTATIOn
AymptomaticSigns of congestive heart
failure
Machinery-like murmur
Widened pulse pressure
-
8/14/2019 Cardiovascular Patho 1 Ogena
52/87
Obstructive Defects
Coarctation of the aorta
Aortic stenosis
Pulmonic stenosis
-
8/14/2019 Cardiovascular Patho 1 Ogena
53/87
COARCTATION OF THE AORTA
(COA)
Localized narrowing near the
insertion of the ductus
arteriosus,
increased pressure proximal to
the defect
-
8/14/2019 Cardiovascular Patho 1 Ogena
54/87
COA
-
8/14/2019 Cardiovascular Patho 1 Ogena
55/87
CLINICAL MANIFESTATION
High BP and bounding pulses inarms
Weak or absent femoral pulses
Cool lower extremities Low BP in the lower extremities Dizziness Headache
FaintingEpistaxis
-
8/14/2019 Cardiovascular Patho 1 Ogena
56/87
Aortic Stenosis
-
8/14/2019 Cardiovascular Patho 1 Ogena
57/87
-
8/14/2019 Cardiovascular Patho 1 Ogena
58/87
Aortic Stenosis
a narrowing in the opening of the valve betweenthe left ventricle and the aorta.
follows rheumatic fever or is a congenitalmalformation.
ventricle must pump more forcefully to expel
blood through the narrow orifice. This causes ventricular hypertrophy and
eventually reduces compliance. As blood backsup in the ventricle, atrial pressure increases and
blood backs up into the pulmonary system andthe right side of the heart.
-
8/14/2019 Cardiovascular Patho 1 Ogena
59/87
Clinical Manifestations
Clinical manifestations may be absent or severe,depending on the level of stenosis.
Pulmonary congestion, with signs of dyspnea andpulmonary hypertension, may occur if blood backs upinto the pulmonary vascular system.
Dizziness and fatigue may occur due to decreasedcardiac output and decreased stroke volume. Heartrate may be elevated via sympathetic stimulation.
-
8/14/2019 Cardiovascular Patho 1 Ogena
60/87
Diagnostic Tools
A systolic heart murmur may
be heard as blood rushes
through the narrow orifice.
Echocardiography may be
used to diagnose abnormal
valve structure and motion.
-
8/14/2019 Cardiovascular Patho 1 Ogena
61/87
Complications
Left ventricular hypertrophy may
develop, leading to congestive
heart failure. Treatment
Treatment for congestive heart
failure may be required.
-
8/14/2019 Cardiovascular Patho 1 Ogena
62/87
Pulmonic Stenosis
-
8/14/2019 Cardiovascular Patho 1 Ogena
63/87
Pulmonic Stenosis
a narrowing of the opening between theright ventricle and the pulmonary valve.
most commonly occurs due to a congenitaldefect.
With a narrow orifice, the right ventriclemust pump more forcefully to expel blood.This can lead to right ventricularhypertrophy, backing up into the right
atrium and causing dilation of the venacava and blood accumulation in thesystemic veins.
-
8/14/2019 Cardiovascular Patho 1 Ogena
64/87
Blood flow into the lungs andleft side of the heart will bereduced if the stenosis is
severe, leading to a decreasein blood pressure. Right heartfailure may develop.
Clinical
-
8/14/2019 Cardiovascular Patho 1 Ogena
65/87
ClinicalManifestations
may be absent or severe depending
on the level of stenosis.
Decreased pulmonary flow causes
poor oxygenation of the blood andfeelings of weakness and fatigue.
Venous distention and swelling of the
ankles and feet are common.
-
8/14/2019 Cardiovascular Patho 1 Ogena
66/87
Diagnostic Tools
Echocardiography may be used to diagnose
abnormal valve structure and motion. Complications
Right heart hypertrophy and subsequent rightheart failure may occur.
Treatment
Treatment for heart failure may be required. Valve replacement or surgical correction of
the stenosis may be attempted.
Decreased Pulmonary
-
8/14/2019 Cardiovascular Patho 1 Ogena
67/87
Decreased PulmonaryBlood Flow Defects
Tetralogy of Fallot
Tricuspid atresia
-
8/14/2019 Cardiovascular Patho 1 Ogena
68/87
Tetralogy of Fallot
The classic form includes
four defects
Ventricular septal defectPulmonic stenosis
Overriding of the aorta
Right ventricular
hypertrophy
-
8/14/2019 Cardiovascular Patho 1 Ogena
69/87
Tetralogy of Fallot
-
8/14/2019 Cardiovascular Patho 1 Ogena
70/87
Tetralogy of Fallot
CLINICAL MANIFESTATIONS
Infants
Cyanotic at birth
Episodes of cyanosis
and hypoxia called Blue
or tet spells
Crying or after feeding
-
8/14/2019 Cardiovascular Patho 1 Ogena
71/87
Tricuspid Atresia
Tricuspid Atresia
-
8/14/2019 Cardiovascular Patho 1 Ogena
72/87
Tricuspid Atresia
The deformity consists of a
complete lack of formation of the
tricuspid valve with absence of
direct connection between theright atrium and right ventricle.
prevalence of 0.3-3.7% in
patients with congenital heartdisease
Clinical
-
8/14/2019 Cardiovascular Patho 1 Ogena
73/87
ClinicalManifestation
detected in infancy because ofpresenting cyanosis, congestiveheart failure, and growth
retardation. history of poor skin colorationinability to complete a feedingsession, frequent pauses during
feeding, and/or frank anorexia.
-
8/14/2019 Cardiovascular Patho 1 Ogena
74/87
Clinical Manifestation
As a result, the infantdemonstrates poor growthpatterns.
Respiratory difficulties areoften reported as nasalflaring or muscle retractions
-
8/14/2019 Cardiovascular Patho 1 Ogena
75/87
Mixed Defects
Transposition of great
vessels
Total anomalous pulmonaryvenous connection
Hypoplastic heart syndrome
RightLeft
Transposition of
-
8/14/2019 Cardiovascular Patho 1 Ogena
76/87
Transposition ofGreat Vessels
The pumonary artery
arised from the left
ventricle and the aortaexits from the right
ventricle
-
8/14/2019 Cardiovascular Patho 1 Ogena
77/87
Transposition of Great Vessels
-
8/14/2019 Cardiovascular Patho 1 Ogena
78/87
CLINICAL MANIFESTATION
Depend on the type and size of
associated defects
Minimal communication Severely cyanotic and depressed at
birth
Large septal defects Less cyanotic but may have
symptoms of CHF
Totally Anomalous Pulmonary
-
8/14/2019 Cardiovascular Patho 1 Ogena
79/87
Totally Anomalous Pulmonary
Venous Connection
Rare Defect.
Pulmonary veins fail to join L atrium.
Clinical manifestations: Usually
cyanotic early on. Condition rapidly
deteriorates as pulmonaryblood flow
increases and causes CHF.
Totally Anomalous Pulmonary
-
8/14/2019 Cardiovascular Patho 1 Ogena
80/87
Totally Anomalous Pulmonary
Venous Connection
-
8/14/2019 Cardiovascular Patho 1 Ogena
81/87
Hypoplastic Left Heart
L side of heart is underdeveloped.
L ventricle is small and aortic atresia.
Most blood flows across patent foramen
ovale to R atrium..to R ventricle and out thepulmonary artery.
Descending aorta receives blood from the
PDA to supply the systemic circulation. PDAclosure >>rapid deterioration and CHF.
Hypoplastic Left
-
8/14/2019 Cardiovascular Patho 1 Ogena
82/87
Hypoplastic LeftHeart
-
8/14/2019 Cardiovascular Patho 1 Ogena
83/87
Clinical Manifestations
As the ductus arteriosus begins to closenormally over the first 24-48 hours of life
Symptoms of cyanosis, tachypnea,respiratory distress, pallor, lethargy,
metabolic acidosis, and oliguria develop. Without intervention to reopen the ductus
arteriosus, death rapidly ensues.
-
8/14/2019 Cardiovascular Patho 1 Ogena
84/87
Clinical Manifestations
With a right-to-left shunt,cyanosis, fatigue, and
weakness occur. Knee-to-chest
or squatting behavior may beobserved. Clubbing of the digits
may develop.
-
8/14/2019 Cardiovascular Patho 1 Ogena
85/87
Clinical Manifestations
With a left-to-right shunt,pulmonary congestion and
dyspnea may occur. Left heart
failure may develop.
Treatment
-
8/14/2019 Cardiovascular Patho 1 Ogena
86/87
Some defects may be small, require no treatment, or close
spontaneously. Surgical correction of the defect is often required.
Treatment for congestive heart failure may be necessary.
Prostaglandin E is administered to maintain patency of the
ductus arteriosus in preductal coarctation.
Administration of the prostaglandin inhibitor indomethacin will
initiate closure of the ductus in patent ductuctus arteriosus.
-
8/14/2019 Cardiovascular Patho 1 Ogena
87/87