Oral Patho 3

of 21
-
Upload
yahya-al-omary -
Category
Documents
-
view
222 -
download
0
Transcript of Oral Patho 3
-
7/29/2019 Oral Patho 3
1/21
"
"
Lets start our lecture ,
Last time we defined leukoplakiaas a white patches that
cant be removed by scrubbing and it cant be diagnosed as
any clinical disease , it doesnt reflect a true
histopathological features and true picture . sometime the
appearance of leukoplakia -as homogenous or nonhomogenous- can tell us if leukoplakia is having a higher
tendency for epithelial dysplasia or not ( non is higher), but
we cant rely on this clinical appearance to determine if
theres high risk or low because some of homogenous
leaukoplakia ll have dysplasia .
Histopathological appearances of leaukoplakia are
epithelial dysplasia , keratosis alone , hyperplasia alone ,keratosis and hyperplasia together or karatosis hyperplasia
dysplasia , squamous cell carcinoma ( malignant change ) .
The factors that ll give us clinical pic of leaukoplakia are :
-keratosis,
-epithelial thickness,
-epithelial dysplasia,
-chronic inflammation
Now we mention keratosis and as we know it can be
parakeratosis (with nuclei ) or orthokeratosis ( without
-
7/29/2019 Oral Patho 3
2/21
neuclei). We can see an prominent layer here (the arrow )
and its called granular layer ( its more obvious in
orthokeratosis than parakeratosis ) .
Para ortho
The thickness of epithelium is variable , Some
leaukoplakia can give you increased epithelial thickness
( acanthosis ) , or atrophy espesialy if the leakoplakia is
speckled . because of atrophy the lesion is red .
( *remember from histology : as we know the epithelium
is avascular and its supplied by the vascular connective
tissue that lied under it , so when the epithelium is thinner
the blood vessels of connective tissue will be more
prominent so the red color ll appear .
-
7/29/2019 Oral Patho 3
3/21
Acanthosis atrophy
Epithelial dysplasia may show clear cut (abrupt) junctionbetween dysplastic epithelium and normal one , or may
show gradual transition between them. In dysplastic
epithelium we can see hyperchromatism like as in the pic .
Dysplastic side normal side
Features of dysplasia that indicate smoking :
1- chevron peaks(triangular curve) of keratin or epithelium
itself
-
7/29/2019 Oral Patho 3
4/21
2- increased melanin production in basal keratinocytes
( melanin incontinence ) , its over production of melanin
that ll escape to the underlying tissue then itll be engulfed
by macrophages , so most of the time we see melanin in theunderlying connective tissue inside the cytoplasm of
macrophages .
So these two features are highly suggestive of smoking as
etiological factor that associated with leaukoplakia .
Now epithelial dysplasia isnt present in most
leaukoplakias , it depend on geographic location , habits ,
risk factors . the percents of finding dysplasia is usually18% ( less than 20%) .
The dysplasia is an architecture change in the epithelium
that include cellular atypia and the over all morphology of
the epithelium . as we know the cellular atypia is the
change in the individual cell , but the dysplasia is the
change in whole epithelium . we can classify dysplasia
according to cellular atypia extension into mild , moderate
and severe :
-Mild dysplasia when atypia isnt extending beyond the
lower(basal) third of the epithelium
-
7/29/2019 Oral Patho 3
5/21
-moderate dysplasia when atypia involves the basal two
thirds
-severe one when atypia involves the superficial third
In the pic below we can say its severe because we can see
atypical cells ( large and have increased nuclear to
cytoplasmic ratio ) in the upper third .
We said that we cant predict the histopatholigical features
of leaukoplakia based on the clinical pic alone , however
theres indication by homogenous and non homogenous ,
non homogenous usually have dysplasia ( 50% according to
some studies ) more than homogenous(10%) .Speckled leaukoplakia have 100% of presence of
dysplasia .
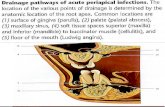
Now in the figure below :
-
7/29/2019 Oral Patho 3
6/21
First we can see the normal , then the homogenous we can
notice increase thickness of keratin in comparison to
normal , increase thickness of epithelium and theres some
lymphocytic infiltrate but the dysplasia isnt present .Now when we have thick fissured leaukoplakia it still
homogenous except some grooves and fissures and here we
can see some dysplastic ( mild in the lower third ) features .
but the surface of leakoplakia start to be nodular with more
fissuring then the dysplasia ll be more present and in
higher rate , so here its moderate severe and then there ll
be erythroplakia and now we can notice how the
epithelium start to be atrophic ( so the epithelium ll beatrophic when there is erythroplakia . if it is erythroplakia
and hyperplastic then itll be speckled leaukoplakia .
The dysplastic features ll reflect change in maturation ,
proliferation and differentiation of the epithelium . features
of dysplasia :
-
7/29/2019 Oral Patho 3
7/21
1. Increased and abnormal mitoses , now the normal
location of mitoses is in the basal layer , while in
dysplasia it ll be higher suprabasal , and in the basal
layer there ll be increase in number and this ll giveabnormal shape .
As we see in the pics its not the normal mitoses that
we know ( not two parallel lines of chromosomes in
the midline ), here we have X shape or star shape
appearance . here we may find normal mitoses but it
can be suprabasal .
2. Basal cell hyperplasia, its cuboidal and
hyperchromatic ( dark color) cells , here we can see
these cells more than in the basal third of normal
epithelium . so here we can see thick layer of basaloid
cells , so this is basal cell hyperplasia and reflect
abnormal proliferation . mitotic figures also reflectabnormal proliferation .
-
7/29/2019 Oral Patho 3
8/21
3. Drop-shaped rete ridges that the epithelium ll be
elongated and widened like a drop , its constricted
above and widened toward the basal layer, and this is
because of more and more proliferation in basal area .
4. Disturbed polarity of basal cells or loss of cellularorientation , you wont see the basal layer normally a
lined or side by side next to each other , it ll be poorly
oriented and extended suprabasaly to the superficial
-
7/29/2019 Oral Patho 3
9/21
layer , this may be by increasing of the proliferation in
the basal area .
5. Increase in nuclear/cytoplasmic ratio , in this casewell see nucleus as big and the cytoplasm is less than
normal cells . if we go up from the basal layer well
see big nucleus and less cytoplasm , so it can be seen
in the middle and superficial layers not just in the
basal .
6. Nuclear hyperchromatism, well see some nucleisdeeply blue because they take stain more than others
because they are hyperchromatised . now
hyperchromatic cells are restricted to the basal layer ,
but here we see it in the middle so its abnormal .
-
7/29/2019 Oral Patho 3
10/21
7. Prominent and enlarged nucleoli , as we can see its a
nucleus and inside it prominent nucleoli . this feature
in many tumors .
8. Irregular epithelial stratification or disturbedmaturation , in normal epithelium we havecuboidal basal layer ,above it flattened pickledcell layer ,and at the top will be more flattened
and thin. This stratification is lost in dysplasia,everything is looking the same all of them arecuboidal and hyper chromatic. Also maturationwill be disturbed, when epithelial cells becomemature it starts forming keratin .so we cant see
-
7/29/2019 Oral Patho 3
11/21
any granular layer because all layers like eachother . this is an architectural feature andthats mean I cant say its atypia because its
just in individual cell , but we can say itsdysplasia because it involves atypia andarchtictural features .
9.Nuclear and cellular pleomorphism , you can see
variation in shape and stain of the cells . the nucleus may
show slight change in size and shape like to be
polyhedral , round several shapes .
10.Abnormal keratinization , keratin as we know ll be in
the superficial and top layer (surface) , but sometime we
can see it even below the granular layer. So this is
abnormal maturation .
-
7/29/2019 Oral Patho 3
12/21
11.Loss or reduction of intercellular adhesion , it ll be
decreased so we can see a spaces between cells . so thistell us the dysplasia is coming soon .
Now ,
Sometime the epithelial dysplasia may be seen in a
reactive area like candidoses or inflammation , so the
dysplasia here ll be considered as reactive because when
we give an antifungal or vaccine it can be reversed .
In some studies theres a rate up to 14% that leaukoplakia
ll transform to carcinoma . this transition depend on the
location in the oral cavity , some have high risk like
ventral of the tongue, Floor Of the Mouth, lingual aspect
-
7/29/2019 Oral Patho 3
13/21
of lower alveolar mucosa. These sight show high
malignant transformation even there is any medical
treatment or vaccine . these lesions are called sublingual
keratosis , it have a high risk of transformation tosquamous cell carcinoma even though 25% will
transform .
If leaukoplasia has a hyperkeratosis alone there ll be no
risk to transform . while leaukoplakia that carry
dysplastic features ll has high risk .
The majority of dysplastic lesions remain unchanged
during observation period.
We cant leave our patient go home with leaukoplakia
without take a biopsy because of high percentage of
having transformation .
Sometimes we see white areas in the corner of the
smokers mouth and it cant be removed by scrubbing ,
but when we give them antifungal theyll be improved so
its a candida infection . in this infection there is 30% to
transform .
-Dysplastic leukoplakia have higher rate to progress than
non neoplastic (10-30%)
-More severe dysplasia higher risk
-Majority of dysplasia remain unchanged
May progress or improve
- No clear corelation between histology and clinical:
-
7/29/2019 Oral Patho 3
14/21
-Sublingual keratosis even with mild dysplasia is
high risk
There is a feature that ll indicate transformation itsthe DNA content . the normal DNA content is diploid ,
so if the leaukoplakia carry diploid there ll be low risk .
but if it carry tetraploid ( double of the normal ) it ll
have intermediate risk . and if it carry aneuploid
( abnormal amount of DNA even less than normal or
more) it ll have the highest risk to transform .
The risk assessment is based on:1. Size ( bigger have higher risk )
2. Site
3. Clinical appearance ( speckled vs homogenous vs
erythroplakia )
4. Degree of epithelial dysplasia.
**Note : the dr said the percentage is included , so youshould know it .
We said the causes of white lesions in the oral cavity
are :- traumatic causes ( mechanical , chemical and
thermal )
- hereditary causes ( sponge nevus )
- idiopathic causes ( leaukoplakia )
- and now terminological causes (Lichen Planus and
Lupus Erythematosus)
-
7/29/2019 Oral Patho 3
15/21
* Lichen Planus :
It may present in the skin and oral cavity . usually if the
patient has Lichen Planus in the skin , 50% there ll be
in the oral cavity . if the patient has it in the oral cavity,
10% there ll be in the skin .
Now Skin lesions:
-Violaceous, itchy papules, may have white streaks on
surface that we call it Wickhams striae. Usually appear
along the scratch
-Variable patterns for papules: discrete, linear, annular,bullous, or widespread rash
-Predilection to flexor surface of wrist.
10% with nail involvement in the form of vertical ridges.
-Lesions develop slowly and 85% resolve within 18months, sometimes with recurrence.
Now oral lesions : it ll show a white striations on the
buccal mucosa and mostly affect it , oral lesions show a
-
7/29/2019 Oral Patho 3
16/21
much more chronic course sometimes extending over
many years.
-may also affect tongue, gingiva , palate and lips.
-Bilateral (most of the time bilateral) and wide spectrumof presentations, alone or in combination.
**Non-erosive type:
- reticular or annular, papular, plaque-like.
- usually asymptomatic.
**Erosive/atrophic types:
- red glazed appearance with areas of superficialulceration which may take several weeks to heal.
- occasionally, ulcers are preceded by bullae (bullous
type).
- often associated with typical areas of non-erosive
lichen planus.
- pain and discomfort may be severe.
-
7/29/2019 Oral Patho 3
17/21
Why the atrophic type ll take the higher risk ?
Because the epithelium ll be thin and the barrier is
impaired ( we concern about epithelium as a barrier also ,so when the epithelium is atrophic the insult ll be more
effective and the barrier is less .
When the Lichen planus involve the gingiva often presents
as a desquamative gingivitis. But its not the marginal
gingiva ( the gingiva at the margin of the tooth and gingiva
that lies above it attached gingiva attach to the bone .** I
think we took about these two concepts briefly in a figure
in oral histo course ** .
What are the Histopathologic Features? :
- hyper keratosis para or ortho ( white areas)
-Epithelial atrophy especially in red areas (so epitheliumthickness and keratosis ll reflect the color ) or
acanthosis (sawtooth pattern of rete ridges).
-
7/29/2019 Oral Patho 3
18/21
- the most important well-defined band of subepithelial
mononuclear infiltrate immediately below the
epithelium , its component is lymphocyte mainly
CD8+ type that is cytotoxic T-cells. These cells llattack the epithelium and ll cause Liquefactive
degeneration of basal layer so we cant see the
basement membrane . may be the attack occure
because of high activity or infection ( we can say like
the antigen of epithelium like the virus antigen so itll
be attacked ). Sometime by this the fluid ll
accumulate and sometime bullae ll be there or not .
- we may see Civatte bodies , its hyaline shrunken
bodies representing apoptotic cells. And by this the
basal layer wont appear .
the causes of the Lichen planus :
not fully understood but it can be due to :-Widely accepted that cell-mediated immune responses
to an external antigen, or internal antigenic changes in
epithelial cells, are involved.
-
7/29/2019 Oral Patho 3
19/21
-Response resembles type IV hypersensitivity.
-Cytotoxic lymphocytes damage basal epithelium
-In most cases the precipitating factors are unknown andwhen the cause is removed it ll be better.
-May be hypersensitivity to drugs and dental materials
-Association with systemic conditions: Hepatitis C
-Graft versus host reaction that present when the patient
has transplant and the body reject it so this rejection ll
affect the skin and the oral cavity , so the body ll reject
the organ and also ll attack the oral mucosa and othersand its fatal sometimes .
-In some patients, lesions are triggered by
hypersensitivity to drugs or dental materials.
-In such cases the condition resolves upon withdrawal ofthe offending agent.
-Such lesions are referred to as lichenoid reactions to
distinguish them from idiopathic lichen planus.
**** Slide 56 so important and the dr just read it
We forgot to say females are affected more than males
with lichen planus.
The last disease for today :
-
7/29/2019 Oral Patho 3
20/21
Lupus erythmatosus
Two types :
1. Chronic discoid :more localized, rounded area on the
face ll show white and purple scaly likekeratosis.intra orally we may have areas that is white
but with some atrophic red parts and some striations
that are more prominent than systemic(sle) ( so by this
we can differentiate between them and by biopsy also ,
or even examining the patient for antinuclear antibody
may help). These areas wont go away by any topical
cream
Most common is a discoid area of erythema or ulcerationsurrounded by white keratotis border sometimes with
radiating striae
--butterfly appearance : more common in sle ( sys lopus
eryth) not in discoid because the most common in
discoid is round .
2. Systemic LE: disseminated.
A variety of autoantibodies are present in SLE,
e.g. antinuclear antibodies (ANA)
Females are affected more than males.
" )
)"
-
7/29/2019 Oral Patho 3
21/21
*** important note: after you read this script I advice you
to refer to the slides because the dr didnt mention all the
things in the slide , the record wasnt good enough to giveme support to cover all the lecs information and the drs
voice sometimes was too low . so I hope that the record ll
be better for you for the next lec script.
Forgive me if theres any mistake
Best wishes for all ^_^
Done by :
Yahya al Omary