Cardiac causes of cardiac arrest workshop guidance Jun 2016 · 2018-12-01 · Cardiac causes of...
7
Page 1 of 7 Australian Resuscitation Council www.resus.org.au ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1 Cardiac causes of cardiac arrest workshop – ALS2 Recert Course Learning outcomes By the end of this workshop candidates should be able to: F describe the different types of ACS F explain how to recognise and assess an ACS F list the relevant immediate treatment for each type of ACS F discuss how to recognise and respond to other cardiac conditions that may cause cardiac arrest Instructor Information The scenario has been written to give consistency in teaching and is a CASTeach. The session will ensure that candidates are exposed to common cardiac causes of cardiac arrest. The patient will require ongoing treatment and the candidates should be able to assess the risks to the patient and identify the required treatment pathway and priority. Slides have been produced for this session but are not essential if a scenario based approach covers the same material. The subsequent slides will reveal the key problems and suggested interventions. At the end of each scenario, discuss further actions/treatment. Candidates will have had experience of the ABCDE approach/High Quality Defibrillation and CPR in the relevant skill stations earlier in the course and through reading the manual. Therefore a demonstration is not required at the beginning of this session. These scenarios should be led as a combination of: Short discussion to set scene on Cardiac Causes including ACS and other causes CASTeach Simulation Case-based discussion using visual aids following It is recommended that the scenario is delivered to identify risk assessment and include the specific treatments for ACS in Circulation, (aspirin/oxygen if appropriate/pain relief) in the ABCDE pre-arrest and the post arrest care include discussion on reperfusion strategies and their considerations. When starting the scenario, the background information for the candidates should be delivered in an ISBAR (Identify, Situation, Background, Assessment, Recommendation) or RSVP (Reasons, Story, Vital signs, Plan) format, according to local practice. The same format should also be used for a handover at the end of a scenario. At least one Australian Resuscitation Council ALS2 Instructor, and one other member of faculty who is either a full instructor or a recertifying Instructor, must supervise the workshop. See the CASTeach guide for the scenario facilitation. Expand the scenario with discussion on Cardiac Causes and specific considerations similar to a special circumstances workshop: perform assessments of the patient using the ABCDE approach (as per ABCDE workshop) e.g.: o assess responsiveness o Airway: check patency o Breathing: check respiratory rate, expansion, effort, percussion, breath sounds, SpO 2 o Circulation: check pulse, blood pressure, capillary refill, urine output and ACS Specific care o Disability: assess conscious level (AVPU, GCS), and pupils, measure blood glucose o Exposure: temperature, assess the whole patient, look for evidence of haemorrhage, rashes etc. Instructor information – points for discussion/further demonstration Initial treatment using ABCDE approach leading to definitive intervention Use of oxygen in ACS Early administration of aspirin/antiplatelet Reperfusion strategies available Summary Recognise different presentations of ACS application of the CASTeach/ABCDE approach to a simulated situation and considerations in C for ACS start appropriate immediate treatment – arrange PPCI when appropriate be aware of other cardiac causes of arrest requiring different management
Transcript of Cardiac causes of cardiac arrest workshop guidance Jun 2016 · 2018-12-01 · Cardiac causes of...

Page 1 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
Cardiac causes of cardiac arrest workshop – ALS2 Recert Course
Learning outcomes By the end of this workshop candidates should be able to:
describe the different types of ACS explain how to recognise and assess an ACS list the relevant immediate treatment for each type of ACS discuss how to recognise and respond to other cardiac conditions that may cause cardiac arrest
Instructor Information The scenario has been written to give consistency in teaching and is a CASTeach. The session will ensure that candidates are exposed to common cardiac causes of cardiac arrest. The patient will require ongoing treatment and the candidates should be able to assess the risks to the patient and identify the required treatment pathway and priority. Slides have been produced for this session but are not essential if a scenario based approach covers the same material. The subsequent slides will reveal the key problems and suggested interventions. At the end of each scenario, discuss further actions/treatment. Candidates will have had experience of the ABCDE approach/High Quality Defibrillation and CPR in the relevant skill stations earlier in the course and through reading the manual. Therefore a demonstration is not required at the beginning of this session. These scenarios should be led as a combination of: Short discussion to set scene on Cardiac Causes including ACS and other causes CASTeach Simulation Case-based discussion using visual aids following
It is recommended that the scenario is delivered to identify risk assessment and include the specific treatments for ACS in Circulation, (aspirin/oxygen if appropriate/pain relief) in the ABCDE pre-arrest and the post arrest care include discussion on reperfusion strategies and their considerations. When starting the scenario, the background information for the candidates should be delivered in an ISBAR (Identify, Situation, Background, Assessment, Recommendation) or RSVP (Reasons, Story, Vital signs, Plan) format, according to local practice. The same format should also be used for a handover at the end of a scenario. At least one Australian Resuscitation Council ALS2 Instructor, and one other member of faculty who is either a full instructor or a recertifying Instructor, must supervise the workshop. See the CASTeach guide for the scenario facilitation. Expand the scenario with discussion on Cardiac Causes and specific considerations similar to a special circumstances workshop: perform assessments of the patient using the ABCDE approach (as per ABCDE workshop) e.g.:
o assess responsiveness o Airway: check patency o Breathing: check respiratory rate, expansion, effort, percussion, breath sounds, SpO2 o Circulation: check pulse, blood pressure, capillary refill, urine output and ACS Specific care o Disability: assess conscious level (AVPU, GCS), and pupils, measure blood glucose o Exposure: temperature, assess the whole patient, look for evidence of haemorrhage, rashes etc.
Instructor information – points for discussion/further demonstration Initial treatment using ABCDE approach leading to definitive intervention Use of oxygen in ACS Early administration of aspirin/antiplatelet Reperfusion strategies available Summary Recognise different presentations of ACS application of the CASTeach/ABCDE approach to a simulated situation and considerations in C for ACS start appropriate immediate treatment – arrange PPCI when appropriate be aware of other cardiac causes of arrest requiring different management
Page 2 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
Instructor Information Clinical syndromes caused by the same disease process:
unstable angina non-ST-elevation myocardial infarction ST-elevation myocardial infarction
Discuss common signs and symptoms associated with ACS above Consideration for diabetic presentations that may be atypical Discuss risk assessment related to ALS Risk assessment (lower to higher risks associated with)
1. History 2. History + ECG Changes 3. History + ECG Changes + Enzyme rise (e.g. Troponin)
Immediate treatment of ACS – Use ABCDE approach
Administer aspirin 300mg orally (crushed/chew) o to all patients, unless known sensitivity as soon as possible
Glycerol trinitrate sublingual when possible (systolic blood pressure considered) o Use patients own if available o If first time ever using GTN use a tablet. In event profound hypotension the remainder of any
tablet may be expelled by patient. Fentanyl/Morphine for pain relief if needed
o Not proven to decrease mortality and caution with heart failure, (humane reasons for administration). Anti-emetics frequently not required – consider if nauseated.
Oxygen o if hypoxic (SpO2 < 94%)
§ or unable to record/measure SpO2 o if any signs of shock o aim to achieve SpO2 with oxygen between 94-98% when measurement possible
Instructor Information
UNSTABLE ANGINA AND NSTEMI
anti-thrombotic
aspirin (loading then regular dose)
clopidogrel or ticagrelor (or prasugrel) - (loading then regular dose)
LMW heparin or fondaparinux
If very high risk: glycoprotein IIb/IIIa inhibitor
pain relief
nitrate
fentanyl/morphine
oxygen if hypoxaemic
myocardial protection
beta blocker
planned coronary angiography (+/- PCI)

Page 3 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
Instructor Information: For discussion/consideration: Other cardiac causes of cardiac arrest
in any cardiac arrest look for evidence of the cause not all cardiac arrests are due to ACS other causes may be ‘structural’ or ‘electrical’ some are inherited, some acquired, some congenital
Examples of other cardiac causes
Condition Nature Causation
Severe aortic stenosis Structural Mostly acquired Sometimes congenital
Hypertrophic cardiomyopathy Structural Inherited
High-grade AV block Electrical Mostly acquired Occasionally congenital
Long QT syndrome Electrical Inherited, but… there are other causes of a long QT interval
Anomalous coronary anatomy Structural Congenital
Preventing other cardiac causes
be alert for warning symptoms (e.g. unexplained syncope) arrange urgent specialist assessment and treatment (including genetic family) with inherited conditions, don’t forget the family

Page 4 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
CASTeach A 1: ACS - Unstable Angina or NSTEMI initially
Clinical setting and history (may be adapted to candidate background) I: You receive a call from a nurse S: asking you to review urgently a 55-year-old woman with a 3-hour history of central chest pain B: Jasvinder self-presented and is normally well. A: She looks unwell, clammy and anxious. High flow oxygen commenced. R: Please assess her immediately. Clinical course initially – A: clear, patient talking, B: RR 20 min-1, SpO2 100% on high flow oxygen, Her SpO2 indicates
that her oxygen concentration should be reduced C: P 100 min-1 (sinus tachycardia), SBP 110/65 mmHg: CRT <2 s (earlier 12 lead ECG/Troponin (negative result) available), D: verbal response, pupils equal and reactive, patient appears anxious, glucose 7.0 mmol L-1 E: clammy, pale, nil else noted
agonal gasping/no signs of circulation initial rhythm is VF after 3rd shock rhythm should change to sinus tachycardia (timing of each loop may be shortened/not in
real time to complete the scenario) patient breathing and pulse present (EtCO2 change noted when available).
Interventions Cardiac arrest management VF Checks patient –confirms cardiac arrest – starts CPR (30:2) Calls resuscitation team/requests defibrillator Defibrillator arrives if not already present Applies defibrillator adhesive pads VF Checks monitor/confirms rhythm
1st shock Airway/ventilation/oxygen IV/IO access 2 min CPR
VF Checks monitor/confirms rhythm 2nd shock 2 min CPR Adrenaline 1 mg IV/IO
VF Checks monitor/confirms rhythm 3rd shock 2 min CPR Amiodarone 300 mg IV/IO
STach Checks monitor/confirms rhythm Checks patient (signs of life/pulse) ABCDE assessment/Post-arrest investigations A: clear/patent (SGA tolerated if present), B: RR 10 min-1, Clear on auscultation, SpO2 95%, C: P 100 min-1
(sinus tachycardia), SBP 85/65 mmHg: CRT <2 s, Bloods/blood gas, 12 lead ECG (see below), D: Unconscious, glucose 6.8 mmol L-1 E: No change – Plan for disposal and care Handover and transfer ICU/catheter lab and CCU Plan: Urgent cardiology review/revascularisation (method depends on setting used), waiting repeat
troponin - consider oral anti-platelets and possible candidate for TTM
Discussion points: High quality CPR
Minimise pre-shock pause between stopping compressions and giving shock
Post-shock CPR without checking monitor
Uninterrupted chest compressions and end-tidal CO2 monitoring after advanced airway insertion
Post-resuscitation care including the ABCDE approach
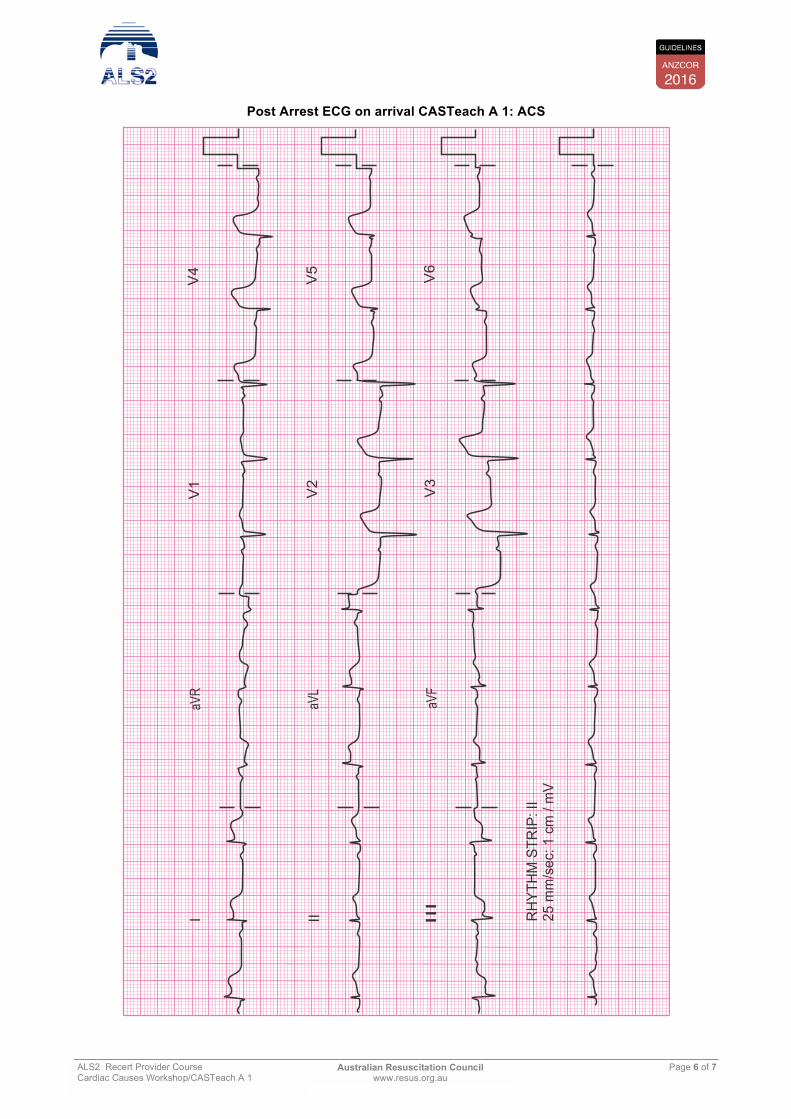
Need for immediate re-vascularisation post-ROSC ECG showed new ST elevation

Page 5 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
Initial ECG on arrival CASTeach A 1: ACS
Page 6 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
Post Arrest ECG on arrival CASTeach A 1: ACS
I II III
aVR
aVL
aVF
RH
YTH
M S
TRIP
: II
25 m
m/s
ec: 1
cm
/ m
V
V1
V4
V2
V5
V3
V6

Page 7 of 7 Australian Resuscitation Council www.resus.org.au
ALS2 Recert Provider Course Cardiac Causes Workshop/CASTeach A 1
early reperfusion with thrombolysis effective
contraindications and considerations for thrombolysis choice of agent for indigenous and pacific islander population
Primary PCI – needs to be timely including activation of STEMI team PPCI can be performed during CPR – consideration for mechanical compression device