BORDERNETwork Training on HIV and HCV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers,...
30
BORDERNETwork Training on HIV and HCV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers, M.A. www.bordernet.eu www.aidshilfe-potsdam.de
-
Upload
marsha-doyle -
Category
Documents
-
view
215 -
download
0
Transcript of BORDERNETwork Training on HIV and HCV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers,...

BORDERNETwork Training on
HIV and HCV Co-Infections Dr. med. Wolfgang Güthoff / Alexander Leffers, M.A.
www.bordernet.eu
www.aidshilfe-potsdam.de

This presentation arises from the BORDERNETwork project which has received funding from the European Union, in the framework of the Health Program, and co-funding of the Ministry of Environment, Health and Consumer Protection of the Federal State of Brandenburg. The sole responsibility of any use that may be made of the information lies with the authors (SPI, AIDS-Hilfe Potsdam e.V.)

Table of Contents
Epidemiology
Natural Course
Therapy
Treatment

Chronic Hepatitis C infection is one of the major co morbidities in people with HIV infection
Worldwide about 5 million of the 33 million HIV infected people are co-infected with HCV, but there are differences between several regions
High rate of co-infection in different countries depends on the common blood borne transmission pathway, especially to high occurrence of intravenous drug use
HIV/HCV Co-infections

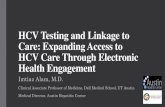
Rate of HIV / HCV Coinfection
Sulkowski Ann Intern Med 2003; Sherman Clin Infect Dis 2002; Rockstroh J; D 2005; Dore J Clin Virol
In Northern America, Europe and Asia together the rate of co-infections amounts about 30%!

Prevalence of hepatitis C in the HIV population (1960/5957 patients = 33%)
Regions:SouthCentralNorthEast
North: 359 = 23,2 %
East: 613 = 46,9 %
South: 695 = 41,4 %
Central: 293 = 19,6 %

Different Routes of HCV Transmission in HIV patients
Rates of vertical HCV transmission are low (3-6%), but in HIV infection it increases 5-fold
Rates of sexual HCV transmission are below 1%
Transmission with blood to blood contact (intravenous drug users) is very high and amounts about 80 to 90%

Hepatitis C is Common in HIV-infected IDUs
Rockstroh JID 2005; Sulkowski Ann Intern Med 2003; Danta J AIDS 2007; Fierer J Infect Dis 2008
HCV transmission in HIV positive IDUs amounts about 80%

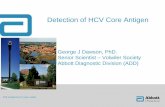
Hepatitis C co-infection in EuroSIDA
HCV genotype distribution and percentage of naturally cleared HCV infection within EuroSIDA
Results: Of 2263 HCVAb+ patients, 1677 (74%) were serum HCV RNA+ (95% CI:71–78%)
Northern Europe
0
20
40
60
1 2 3 4
Southern Europe
Central Europe
Eastern Europe
1 2 3 4 1 2 3 4 1 2 3 4
Distribution of HCV by genotype (1–4) in European regions
Genotype
Soriano et al. 11th EACS, Madrid 2007. PS8/1

Diagnostic in patients with HIV/HCV Coinfection
All HIV patients have to be screened for hepatitis C. If HCV antibody test is negative in progressive stage of HIV infection and if there is further suspicion of possible HCV infection, a measurement of HCVRNA with PCR should be done.
HCV genotype and viral concentration before starting therapy
Liver fibrosis staging (liver biopsy as the best method but not mandatory for considering treatment)
All necessary laboratory measurements for excluding possible contraindications of combination therapy with pegylated interferon and ribavirin

Natural Course of HIV / HCV Coinfection Influence of HCV on HIV-Infection
HCV infection does not have a relevant influence on the course of HIV infection
• There was no difference in the EuroSIDA cohort regarding CD4 cell
recovery after starting ART in mono-infected HIV patients in comparison to HCV co-infected patients (1)
• Hepatitis coinfection does not influence the virological and immunologic response to ART (2)
(1) Rockstroh 2009. / (2) Peters,L.:J Acquir Immune Defic Syndr. 2009, 15;457-63.

Natural Course of HIV / HCV CoinfectionInfluence of HIV on HCV-Infection
HIV infection influences all stages of hepatitis C in different ways:
1. HIV increases the rate of hepatitis c persistence, the spontaneous recovery of acute HCV infection is decreased
Correlates of Hepatitis C Virus Clearance from HIV Status
Factor No. (% Clearence)
HIV negative 420 (13,8)
HIV positive CD4 > 500
72 (8,3)
HIV positiveCD4 200 – 499
162 (8,6)
HIV positiveCD4 < 200
119 (5,0)
Thomas, D.L.; The Natural History of Hepatitis C Virus Infection; JAMA 2000; 284:450-456

Natural Course of HIV / HCV Coinfection Influence of HIV on HCV-Infection
2. There is a rapid progression of liver fibrosis in HIV / HCV co-infected patients in contrast to hepatitis C mono-infected
patients.
Probably this is due to the lack of CD4-T cell response against hepatitis C virus.
The Time of development to liver cirrhosis is shorter in co-infected patients than in mono-infected HCV patients.
Martin-Carbonero, L. et al.: Incidence and predictors of severe liver fibrosis in HIV infected patients with chronic hepatitis C.Clin Infect Dis 2004, 128-33

Natural Course of HIV / HCV CoinfectionInfluence of HIV on HCV-Infection
3. As a result of faster progression of liver fibrosis and faster
development of cirrhosis the incidence of hepatocellular
carcinoma is also higher in HIV/HCV co-infected patients
than in HCV mono-infected patients
Giordano, TP et al.: Cirrhosis and HCC in HIV infected veterans with and without the hepatitis C virus. Arch Intern Med 2004, 2349-54

Therapeutic Challenges in co-infected patients with hepatitis C and HIV
Treatment of chronic Hepatitis C: • Access to treatment, costs of therapy, • Duration of therapy depends on HCV genotype, baseline HCV
viral load and virological response and can take 72 weeks
In co-infected patients the sustained virological response is lower then in HCV mono-infected patients
Choice of ART together with concomitant HCV therapy regarding side effects and interactions
Challenges in treatment of HCV with the new oral agents Telaprevir and Boceprevir

Treatment of Hepatitis C in HIV infected People
1. Pegylated interferon alfa 2a
Standard dosage: 180 g sc once weekly independent of body weight
or
Pegylated interferon alfa 2b
Standard dosage: 1.5 g / kg body weight once weekly
combined with
2. Ribavirin
Standard dosage of ribavirin for HCV genotype 1 is 1000mg per day (<75kg body weight), or 1200mg per day (>75kg body weight

Treatment outcome in HIV/HCV: PegIFN and Ribavirin
Carrat et al. JAMA 2004, Laguno et al. AIDS 2004, Nunez et al. AIDS Res Hum Retroviruses 2007
Chung et al. NEJM 2004, Torriani et al. NEJM 2004, Alvarez et al. CROI 2005, Abstract 927
ACTG5071
289 205n with PEG-IFN-2a + RBV
Type PEG-IFN-
Patients with IVDA
Patients with cirrhosis
Genotype 1-4
normal ALT
mean CD4+
on HAART*
Therapy discont. (AE or L)
66
EOT (ITT)
SVR (ITT)
52
2a 2b2a 2b
62% 80%- 75%
15% 39% (F3-F4)11% 19%
67% 61%77% 63%
0 16%34% 0
520 477495 570
83% 83%85% 94%
25% 17%*12% 17%
49% 35%41% 52%
40% 27%27% 44%
APRICOT RIBAVIC Laguno
389
2a
90%
28% (F3-F4)
61%
0
546
74%
8%
67%
50%
PRESCO

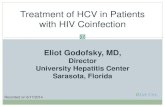
IL-28B Genotypes and SVR Rates
Recent studies demonstrate polymorphisms near interleukin 28 B (IL28B) gen
predict sustained virological response (SVR) to treatment with Peg-IFN + RBV in HCV-mono-infected patients harbouring genotype 1
Study assessing potential role of the IL-28B treatment induced clearance of rs12979860 polymorphism in acute and chronic hepatitis C in HIV-positive patients
0
25
50
75
100
C/C C/T T/T
IL28B genotype
P=0.008
%S
VR
HIV(-)/HCV(+)
P=0.039
IL28B genotype
HIV(+)/chronic hepatitis C
C/C C/T T/T
0
25
50a
75
100
%S
VR
P=n.s.
IL28B genotype
HIV(+)/acute hepatitis C
C/C C/T T/T
0
25
50
75
100
%S
VR
Natterman J, et al. . 17th CROI; San Francisco, CA; February 16-19, 2010. Abst. 164; JID 2011 in press; Source: Rockstroh 2011 Potsdam

Proposed optimal duration of HCV therapy inHCV/HIV coinfected patients
Rockstroh: HIV Medicine 2008; update EACS Conference in Cologne November 2009, update 2011 Belgrade EACS Conference
* In patients with baseline low viral load and minimal fibrosis
W 4 W 12 W 24 W 48 W 72
HCV-RNA negative
HCV-RNA positive
G 2/3
G 1/4
>2 log drop in HCV-RNA
<2log drop in HCV-RNA STOP
24 weeks‘ therapy*
48 weeks‘ therapy
72 weeks‘ therapy
HCV-RNA positive
HCV-RNA negative
STOP
G 1/4
G 2/3

HIV Medication with HCV Therapy
Didanosine (ddI) is contraindicated
Use of AZT and d4T should be avoided due to increased risk of
toxicity
Increasing side effects of combination Atazanavir – Ribavirine is
possible
Combination of Efavirenz and PEG-IFN – high risk of severe
depression

PIs in the treatment of HIV/HCV Co-infected Patients
New directly acting agents (DAAs)
Two groups of protease inhibitors (PI)
• linear and macrocylic PI
First two linear PI are approved in US and Europe:
• Telaprevir
• Boceprevir
Triple therapy (PEG-IFN, Ribavirine + PI) is an additional
challenge for clinicians

Telaprevir – Drug Interaction with ARVs
(6) Van Heeswijk R et al.: Pharmacokinetic interactions between ARV agents and the investigational HCV protease inhibitor TVR in healthy volunteers. 18th Conference on Retroviruses and Opportunistic Infections. February 27 – March 2, 2011,Boston, USA. Session 34, Abstract 119
TVR dose ARV TVR AUC TVR Cmin ARV AUC ARVCmin
TVR 750 mg TID ATV/r 0.80 (0.76-0.98) 0.85 (0.75-0.98) 1.17 (0.97-1.43) 1.85 (1.40-2.44)
DRV/r 0.65 (0.61-0.69) 0.68 (0.63-0.74) 0.60 (0.57-0.63) 0.58 (0.52-0.63)
FPV/r 0.68 (0.63-0.72) 0.70 (0.64-0.77) 0.53 (0.49-0.58) 0.44 (0.40-0.50)
LPV/r 0.46 (0.41-0.52) 0.48 (0.40-0.56) 1.06 (0.96-1.17) 1.14 (0.96-1.36)
TVR 1250 mg TID EFV
0.82 (0.73-0.92) 0.75 (0.66-0.86)0.82 (0.74-0.90) 0.90 (0.81-1.01)
TDF 1.10 (1.03-1.18) 1.17 (1.06-1.28)
TVR 1500 mg BID EFV
0.80 (0.73-0.88) 0.52 (0.42-0.64)0.85 (0.79-0.91) 0.89 (0.82-0.96)
TDF 1.10 (1.03-1.17) 1.06 (0.98-1.15)

Boceprevir – Drug Interactions with ARVs
Boceprevir and PIs:
Boceprevir reduced mean trough concentrations of boosted
Atazanavir, Lopinavir and Darunavir by 49%, 43% and 59%
Boosted Lopinavir and Darunavir decreased the exposure of
Boceprevir by 45% and 32%

Treatment of HIV/HCV Coinfection with PI containing therapy - Conclusions
New options for therapy also in setting of HIV/HCV co-infected
patients, especially for patients with detected liver fibrosis
Recommended backbone:
• Tenofovir with Emtricitabine or lamivudine,
or Abacavir/Lamivudine.
Use of boosted PIs together with Telaprevir and especially with
Boceprevir is problematic
Use of Raltegravir is possible
Excellent management of combination therapy is necessary for
success of treatment

Antiviral Therapy of Acute Hepatitis C in HIV Patients
Recommendations from the European AIDS TreatmentNetwork (NEAT) for acute hepatitis C in HIV
infected individuals
The European AIDS Treatment Network
Acute Hepatitis C Consensus Panel
AIDS 2011, 25: 399 - 409

Acute Hepatitis C in HIV Patients –Criteria for Case Definition
1. Positive anti HCV and positive HCVRNA and da documented
negative antiHCV in the last 12 month (grade A, Level II)
2. Positive HCVRNA and a documented negative HCVRNA and
negative antiHCV in the previous 12 month (grade A, Level II)
3. If there do not exist serological data for HCV in the past:
• Positive HCVRNA with acute rise of ALAT more than 10 times
the upper limits of normal (ULN) (B III)
• Positive HCVRNA with acute rise more than 5 times the ULN,
with documented normal ALAT within 12 month (B III)
In these cases acute Hepatitis A, B and E have to be excluded

Antiviral Therapy of Acute Hepatitis C in HIV PatientsStart treatment if HCVRNA is positive yet at week 12
*Evidence based on using a 615 IU/ml cutoff to define negative HCV-RNA; NEAT Consensus statement AIDS 2011Vogel M, et al., HIV 10; Glasgow; November 7-11, 2010; Abst. O313.
HCV-RNAnegative*
Stop therapyBIII
peg-IFN + RBV (AII)
< 2 log10
24 weeksAII
Drop HCV-RNA 2 log10
Week 4 Week 12
HCV-RNApositive*
48 weeksBIII

Summary 1
HCV/HIV co-infected patients show an accelerate progression to
cirrhosis and increased liver-related mortality
Every co-infected patient should be evaluated for combination
therapy with pegylated interferon + ribavirin
Duration of therapy depends on the HCV genotype, baseline HCV
concentration and treatment response
Higher CD4 cell counts are associated with higher treatment
response, so ART should not be withheld in coinfected patients
ART needs to be adapted to concomitant HCV therapy

Summary 2
The new protease inhibitors in HCV therapy induce better chances
of cure in HIV/HCV co-infected patients, but the use of Telaprevir
and Boceprevir together with ART causes additional challenges.
Further studies regarding drug interactions optimizing therapy are
necessary
Treatment of co-infections should be carried out only in special
treatment centres