Bifurcation tutnours: Is endoscopic...
4
ENDOBILIAR Y PROSTHESES Bifurcation tutnours: Is endoscopic drainage sufficient? H I LAR TUMOURS INCLUDE CARCl- no mas of th e hepat ic du ct (Klats kin' s tumour) (1), gallbladd er carcinoma and meta stases located in the confluence. A tumour is type l wh en stri ct ure is l imit ed to the common hepatic duct, type II when both left and right hepatic ducts are involved, a nd type Ill when one or more sectorial ducts are in volved (Figure l ). The an atomi ca l variations of the bile ducts around the confluence have been described byCouinaud (2) (Figure 2) . T hey are important fo r prec ise diag- nosis of the sectors or segments in - vo lv ed, but also for manageme nt . These variations are more difficult to recog- nize when the ducts are enlarged above the confluence. Bifurca tion tumours are ex treme ly difficult to manage surgica lly. Extensive resection to cure th e disease is ce rtainly the best treatment when possible (3), as is liver transplantation, which can only be proposed fo r carefu ll y sel ec ted young patie nts with invasive carcinoma of the bifur ca ti on wi th o ut ex r ra h ep atic sprea<l . MICHEL C REMER, JACQUES D EVI ERE Figure 1) T ypes of hilar s trictures (bismuth) Palliati ve surgery, which is the usual ou tcome of laparotomy ( 4) and which is not easy nor completely successful, has a mortal ity rate bet ween lO a n<l 15%. Moreover, when the pati ent sur- vives after ope ra tion, the mea n survival rime is ve ry short : betwee n six and 16 months (5,6). Fina ll y, only a small minority of Hopital Eras me - Universire Libre de Brux elles, Brussels, B elgium Con·es p ondence and re prin ts: Dr M Cremer, Hof ii tal Erasme - Universi te Libre de B ruxe l les , Brussels , Bel gium patie nts having a tumour of t he con- fluen ce are ca n<lid ates fo r surge ry be- ca use of assoc iated diseases oft en related to agein g, hut also to extension of th e tumo ur and the presence of lymph nodes. Th e pe rc utaneous- transhepatic ap- proach to bifurcat ion tumours carri es a high rate of severe co mpli cations, cg, peritonea l bile leakage, hemobil ia anJ cholangitis, and fa il ure to <lrain these leaves the patie nt even worse (7 ,8). A lth ough endoscopic sce nt ing has 576 CAN J GASTROENTEROL VOL 4 NO 9 D ECEMBER 1 990
Transcript of Bifurcation tutnours: Is endoscopic...

ENDOBILIAR Y PROSTHESES
Bifurcation tutnours: Is endoscopic drainage
sufficient?
H ILAR TUMOURS INCLUDE CARCl
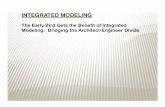
no mas o f the hepat ic du c t (Klatskin's tumour) (1), gallbladder carcinoma and metastases located in the confluence. A tumour is type l when stricture is limited to the commo n hepatic duct, type II when both left and right hepatic ducts are involved, and type Ill when one or more sectorial ducts are involved (Figure l ).
T he anatomical variations of the bile ducts around the confluence have been described byCouinaud (2) (Figure 2) . T hey are importan t for precise diagnosis of the sectors or segments involved, but a lso for management. These variations are more difficult to recognize when the ducts are enlarged above the confluence.
Bifurcation tumours are extreme ly difficult to manage surgically. Extensive resect ion to cure the disease is certa in ly the best treatment when possible (3), as is liver transplantat ion, which can on ly be proposed for carefully selected young patients with invasive carcinoma of the bifurcatio n wi thout ex rra hepa ti c sprea<l .
MICHEL C REMER, JACQUES D EVI ERE
Figure 1) Types of hilar strictures (bismuth)
Palliative surgery, which is the usual outcome of laparotomy ( 4) and which is not easy no r comple tely successful, has a mortality rate between lO an<l 15%. Moreover, when the pat ient survives after operation, the mean survival rime is very short: between six and 16 months (5,6).
Finally, o n ly a small minority of
Hopital Erasme - Universire Libre de Bruxelles, Brussels, Belgium Con·espondence and reprints: Dr M Cremer, Hofiital Erasme - Universite Libre de Bruxelles ,
Brussels , Belgium
patients having a tumo ur of the confluence are can<lidates for surgery because of associa ted diseases often related to ageing, hut also to extension of the tumour and the presence of lymph nodes.
The percutaneous-transhepat ic approach to bifurcation tumours carries a high rate of severe complicat ions, cg, peritoneal bile leakage, hemobil ia anJ cholangitis, and fa ilure to <lrain these leaves the patient even worse (7 ,8 ).
A lthough endoscopic scenting has
576 CAN J GASTROENTEROL VOL 4 NO 9 D ECEMBER 1990

RIGHT LOBE (RU
AL RL
AL RL
RL
figure 2) Anatomical i1ariat1ons of the confluence of bile ducts (reference 2)
TABLE 1 Cholangitis, 30 day mortality, median survival rate and rate of death from sepsis according to type of stricture and kind of treatment
n Early 30day Survival rate Late death from cholangitis (% ) mortality (%) (months) se~sis (%)
Type I 1 stent 20 10% 0%
Type 11 and Ill 50 30% 22%
I stent 24 38% 29%
2stents 24 17%
n Number of patients
become the method of choice for incurable malignant obstruction of the biliary tree, little enthusiasm has been elicited since the first endoscopic series. The high rate of cholangitis was related to incomplete drainage of both lobes of the liver fortype 11 and Ill tumours, and
8%
5.1 20% 5.9 38% 5.3 46% 6.5 13%
most fatalities were caused by further septic shock (9).
In consideration of these poor results, the aulhors decided afler 1984 to attempt aggressive management, ie, to drain both lobes immediately in patients with type II and III strictures,
CAN J GASTROENTEROL VOL 4 No 9 DECEMBER 1990
Bifurcation tumours
no longer wamng tM chnlangiti~ to
occur in the undrained lobe. The most frequencly used stenr for
the hdar tumours in the authors' serae~ is still the black 'sigmoid C shaped' polyamide endoprosthcsis (GuerbetBiocrol, Paris, France) wirh an internal diameter of2.6 mm, an effective length of 11 cm, and a proximal bend adapted to the an~11omy of the intrahepatiL ducts. Unlike the straight Amsterdam slent which docs not conform to the anatomical angulation of lhe left heratic duct al the confluence, the hilar Biotrol scent has an angulation at the proximal end designed specifically for use in hilar strictures, prcvcnung dislocation from the left hepatic duct. The distal C shaped end prevents duodenal perforntion, reported in rare instances with the straight Stent. The lefr hepatic duct must be stenred first for patients with type II or lll strictures as access to the right is nearly always easier for anatomical reasons.
In one patient of four w1rh type 11 and Ill strictures 1t 1s necessary to follow the percutaneous route LO lhread a guidewire through a stricture that cannot be reached by a trampapillary approach. An externa l-internal Ring catheter is left in place beside the first endoscopic scent. Two days lacer, a second stenc is irn,encd using the 'rendezvous' trnnspapillary technique, alongside the percutaneous guidewire. Th is approach has reduced sepsis and 30 day mortality, resulting in longer survival rates (Table I).
Furthermore, the authors observed that the lowest rate of late dealh from sepsis or jaundice occurred in the group of patients with the most invasive tumours ( type ll and Ill) chat were completely treated. The rate of late death was paradoxically lower than in the group with rype I strictures. l I igher rates were seen in patients with incomplete drainage (Table 2).
Late complications of endoscopic internal biliary drainage for the 59 patients who survived more than one month were mostly related to clogging of the scent (27<l{i), with a mean slent survival time of 4.8 months. Dislocation (8%) and breakage of the scenr (2%) were observed initially with
577

CREMER AND DFVIERE
straight AmsterJam srents hue nor with
the benJ-type Stent, which hetter fits the left hepatic Jucr. C holecystitis was observed in 34 pauents.
The results using this type of active
management of hilar tumours are as good as those ohtaineJ for palliative treatment of pancreatic cancer (Tahle 3).
The present anJ the future are con
cemeJ with the self-expanJing metallic scents (18, 24 and 30 French), for which
little endoscopic experience has heen obtained s in ce the work of the European Multiccntric S tudy Group in May 1989 (104 pauencs). Technical problems for type II and III hilar stric, cures remain, for which scents must be inserteJ simultaneous ly on hoth sides of the confluence.
Percurnncous transhepauc. manage, ment with these 'wallstents' has shown
secondary involvement of the scent by the tumour, but up to now few patients have been createJ with two wallsrents, and only by the preventative per
cutaneous approach.
CONCLUSION Endoscopic and combineJ per
cutaneous-endoscopic transpapi llary srenting with multiple large endoproscheses has a high technical success race (97%), and is a palliative method of
REFERENCES 1. Klatskin G. A<lenocarcinoma of the
hepatic duct at its bifurcation within the porta hepat1s: An unusual tumour with Jescruccive clm1cal anJ patholog1cal femures. Am J MeJ 1965; 38:241-56.
2. Coumau<l C. Le Foic. Etu<les Anatom14ucs er Chirnrgicales. Pr1ris: Masson, 1957:464-79
3. Launois B, Campion JP, Brissot P. Carcmoma of the hepatic hdus. Surgical management an<l the ca~e for rescrnon. Am Surg 1979;190: 151-3.
4. Bismuth M, Dunham F, Oub1s A, er al. Complications tarJivcs Jc l'cnJo~copie
578
TABLE 2 Cholangitis, 30 day mortality and median survival rate according to kind of treatment
Type II and Ill n Early 30day Survival rate Late death 2 stents cholang!tis (%) mortality (%) (months) from sepsis (%)
Endoscopic 18 11 11 74 11 route only
Endoscopic and 6 34 0 3.7 17 percutaneous
TABLE 3 Results of endoscopic internal biliary drainage in patients with malignant strictures of the bile ducts
Success rate (%) Cholangitis (%) 30day Survival rate
Pancreas 95 Hilar type I 92 Hilar type II and Ill 89
treatment for hilar tumours for which results are poor but strictly comparable
to surgical palliation. As long as endoscopic retrograde
cholangiopancreatography (ERCP) is mandatory for every patient with
obstructive jaundice and suspicion of hilar tumour, immediate dramage must be performed to avoid iatrogenic cholang1cis. Biliary dramage 1s 111 fact 'preoperative' fo r only a minority of patients for whom curative resection or
liver transplamacion could he con
siJcred.
Jiagnostique et opcrawirc des vo1cs bilio-pancrcm1ques. Acrn Gastroenterol Belg 1981 ;44:396-403.
5. Perissat J, D1ar<l F, Gouffrant JM, Bnhois JP, Doutre LP. Cancer de (;i vmc hiliaire princ1palc. lntcrct de la cholangiographic cranspanctohepatique ptc-opcratoire. Apropos de 31 ens. Ann Chir I 975;29:281-8.
6. Huguet C, Nordlinger R, Ibanez L, H.ilcam1 F, Pare R, Loyguc J. Tr,uremcnt palli,1tif de, cancers du cnnfluem hiliaire supcricur. Choix emrc derivation mcrahcpat1quc ct intuh,1tion transtumorale. Nouv Rev
mortality (%) (months)
10 2 8 12 3 7 17 8 6
Percutaneous drainage of type II and Ill tumours has a higher mortality rnrc (30%) and a lowe r mean length of survival (two co four mnnths).
The main rule to be followeJ 1s drainage of horh lobes of the liver im
mediately following ERCP, using the rendezvous technique only after failure to threaJ a gu1dewire through one of the strictures.
Additional therapy such as radio
therapy anJ chemotherapy have not proveJ as uscf ul following internal
biliary drainage.
Med 1982; 11 :1467-70. 7. Ferrucci JT, Mueller PR, Harhm WP.
Percutaneous transhcpauc biliary Jrnmagc: Technique, rcsule, anJ application~. R,1Jiology 1980; 135: 1-1 l
8. Hatfield ARW, Tohras R, Tcislauchc J, et al. Prcoperanve extern.ii biliary Jramage m 11hsrruct1ve 1aun<l1cc: A prospective controlled 1ri,1I. Lmcec I 982;i i:896-8.
9. Dev1ercJ, Baize M, de Tocuf J, Cremer M. Long term follow-up of p.it1ents with hilar malignant stricture treated hy cn<lnscnric mtcrnal biliary Jramagc. G;.istromte~t Endosc 1988; 34:95- 10 I.
CAN J GASTROENTFROL VOL 4 NO 9 DECEMRER 1990

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com











![ISSB Water Tank Consruction Manual 120908 FINAL[1]](https://static.fdocuments.net/doc/165x107/543d24b8afaf9fa00a8b4569/issb-water-tank-consruction-manual-120908-final1.jpg)