
Collective Behaviour & Social Movements Precipitating Conditions.
Upload
jade-whiteheadCategory
view
232download
1
Hepatic DecompensationsHepatic Decompensations

AgendaAgenda
Hepatic decompensationsHepatic decompensations
Hepatic encephalopathyHepatic encephalopathy– Treatment/precipitating factorsTreatment/precipitating factors
SBPSBP– Differentiate from secondary peritonitisDifferentiate from secondary peritonitis
Variceal bleeding (portal HTN bleeding)Variceal bleeding (portal HTN bleeding)– Treatment and prophylaxis Treatment and prophylaxis

Hepatic EncephalopathyHepatic Encephalopathy
Neuropsychiatric abnormalities occurring Neuropsychiatric abnormalities occurring in patients with liver dysfunctionin patients with liver dysfunction– Type A acute liver failureType A acute liver failure– Type B portosystemic bypass/shunt without Type B portosystemic bypass/shunt without
cirrhosiscirrhosis– Type C chronic liver disease/cirrhoisisType C chronic liver disease/cirrhoisis

Hepatic EncephalopathyHepatic Encephalopathy
Minimal HE abnormal psychometric testing Minimal HE abnormal psychometric testing but normal routine neurologic exambut normal routine neurologic exam
Overt HE:Overt HE:– Stage I personality change, sleep impairedStage I personality change, sleep impaired– Stage II asterexis, short attention spanStage II asterexis, short attention span– Stage III somnolent but arousableStage III somnolent but arousable– Stage IV coma Stage IV coma
Blei AT, Córdoba J. Hepatic Encephalopathy. Am J Gastroenterol. Jul 2001;96(7):1968-76.

Management-Identify and Management-Identify and precipitating factorsprecipitating factors
GI bleedingGI bleeding
SepsisSepsis
Medication non-Medication non-compliance compliance
ConstipationConstipation
Protein overloadProtein overload
s/p TIPSs/p TIPS
CNS active drugCNS active drug
Development of HCCDevelopment of HCC
New liver injury (Hep New liver injury (Hep D infection in chronic D infection in chronic Hep B)Hep B)
UremiaUremia
Hypokalemia, Hypokalemia, alkalosisalkalosis
Therapy-LactuloseTherapy-Lactulose
Synthetic disaccharide-Lactulose start at Synthetic disaccharide-Lactulose start at 30 ml daily/ twice daily (PO/NGT)30 ml daily/ twice daily (PO/NGT)
Reduces colonic pH to 5.0 favors the Reduces colonic pH to 5.0 favors the formation of NH4 from NH3 (decreased formation of NH4 from NH3 (decreased plasma concentration of NH3)plasma concentration of NH3)
Titrate to 2-3 BM’s dailyTitrate to 2-3 BM’s daily
Side effects include cramp, diarrhea, Side effects include cramp, diarrhea, flatulenceflatulence

Enema-LactuloseEnema-Lactulose
Use of 1-3 liters of 20% Lactulose is more Use of 1-3 liters of 20% Lactulose is more effective than tap water enemaeffective than tap water enema
Oral therapy preferred by most Oral therapy preferred by most

Therapy- antibioticsTherapy- antibiotics
Bass NM, Mullen KD, Sanyal A, Poordad F, Neff G, Leevy CB, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071-1081.
Rifaximin 550 mg PO BID approval from Rifaximin 550 mg PO BID approval from FDA March 2010 for reduction of FDA March 2010 for reduction of recurrence of Hepatic encephalopathy)recurrence of Hepatic encephalopathy)
Bass et al- 299 patients received either Bass et al- 299 patients received either rifaximin 550 mg or placebo BID with rifaximin 550 mg or placebo BID with lactulose in >90%lactulose in >90%

RifaximinRifaximin
58% reduction in the rifaximin group in 58% reduction in the rifaximin group in recurrent HE compared with the placebo recurrent HE compared with the placebo group (group (PP <0.0001). <0.0001).
Secondary endpoint -- risk of experiencing Secondary endpoint -- risk of experiencing HE-related hospitalization reduced by 50% HE-related hospitalization reduced by 50% with rifaximin (with rifaximin (PP = 0.0129). = 0.0129).
Bass NM, Mullen KD, Sanyal A, Poordad F, Neff G, Leevy CB, et al. Rifaximin treatment in hepatic encephalopathy. N Engl J Med. 2010;362(12):1071-1081.

Therapy- antibioticsTherapy- antibiotics
Metronidazole 250 mg PO QID (short Metronidazole 250 mg PO QID (short term use-risk of neurotoxicity/antibuse term use-risk of neurotoxicity/antibuse effect)effect)
Vancomycin 250 mg PO QIDVancomycin 250 mg PO QID
Neomycin 500 mg PO QID (risk of Neomycin 500 mg PO QID (risk of ototoxicity and nephrotoxicity—in general ototoxicity and nephrotoxicity—in general avoid aminoglycosides/NSAIDS in liver avoid aminoglycosides/NSAIDS in liver patients)patients)

Alternative therapyAlternative therapy
Vegetable-based protein-consider in those Vegetable-based protein-consider in those who worsen with high protein loadswho worsen with high protein loads
Flumazenil- short term for iatrogenic or Flumazenil- short term for iatrogenic or endogenous benzo suspected to have endogenous benzo suspected to have precipitated HEprecipitated HE
Zinc 600 mg daily (especially if deficient). Zinc 600 mg daily (especially if deficient). Mixed resultsMixed results
Marchesini G, Fabbri A, Bianchi G, et al. Zinc supplementation and amino acid-nitrogen metabolism in patients with advanced cirrhosis. Hepatology. May 1996;23(5):1084-92. Bresci G, Parisi G, Banti S. Management of hepatic encephalopathy with oral zinc supplementation: a long-term treatment. Eur J Med. Aug-Sep 1993;2(7):414-6

Non-rx therapy Non-rx therapy
Closure of TIPSClosure of TIPS
Reduction of shunt diameterReduction of shunt diameter
OLT per AASLD recommend refer for OLT OLT per AASLD recommend refer for OLT at MELD of 10 or for hepatic at MELD of 10 or for hepatic decompensationdecompensation
Survival benefit once patient MELD >15Survival benefit once patient MELD >15

Spontaneous Bacterial PeritonitisSpontaneous Bacterial Peritonitis
Positive ascitic fluid culture Positive ascitic fluid culture
Nearly always a single organismNearly always a single organism
If polymicrobial consider bowel perforationIf polymicrobial consider bowel perforation
PMN count of >250 cells/mm3PMN count of >250 cells/mm3
High risk if h/o SBP, GI bleed, total High risk if h/o SBP, GI bleed, total protein<1 gram/dlprotein<1 gram/dl

TreatmentTreatment
Empirically treat prior to culture results for Empirically treat prior to culture results for PMN count > 250 cells/mm3PMN count > 250 cells/mm3
E. Coli (43%), Streptococcus species E. Coli (43%), Streptococcus species (23%) and Klebsiella pneumoniae (11%)(23%) and Klebsiella pneumoniae (11%)
Anerobes rare causes of SBPAnerobes rare causes of SBP
Fungi= SBP only in severe Fungi= SBP only in severe immunodeficiencyimmunodeficiency

TreatmentTreatment
Cefotaxime 2 grams IV q 8 hrs (x 5 days)Cefotaxime 2 grams IV q 8 hrs (x 5 days)
Ceftriaxone 1 gram daily (x 5 days)Ceftriaxone 1 gram daily (x 5 days)
Most cultures of ascitic fluid become Most cultures of ascitic fluid become negative after a single dosenegative after a single dose
5 Day duration= equivalent efficacy rates 5 Day duration= equivalent efficacy rates of cure and relapse to 10 day duration of cure and relapse to 10 day duration
Volume expansion with albumin 1.5 Volume expansion with albumin 1.5 grams/kg day 1 and 1 gram/kg on day 3 grams/kg day 1 and 1 gram/kg on day 3

ProphylaxisProphylaxis
Those with prior SBP-indefinitely or until Those with prior SBP-indefinitely or until ascities disappearsascities disappears
Cirrhotics with GI bleeding-7 daysCirrhotics with GI bleeding-7 days
Ascitic fluid TP <1 gram/dl during Ascitic fluid TP <1 gram/dl during hospitalization (controversy)hospitalization (controversy)

ProphylaxisProphylaxis
Norfloxacin 400 mg daily (poorly absorbed Norfloxacin 400 mg daily (poorly absorbed fluoroqunolone-effective for gram negative fluoroqunolone-effective for gram negative enterics)enterics)
60% reduction in ascitic fluid infection60% reduction in ascitic fluid infection
Bactrim one double strength tablet orally Bactrim one double strength tablet orally dailydaily

Portal HTN bleedingPortal HTN bleeding
Esophageal, gastric, ectopic varicesEsophageal, gastric, ectopic varices
Portal HTN gastropathy/enteropathyPortal HTN gastropathy/enteropathy
Secondary to distortion of liver architectureSecondary to distortion of liver architecture
Increased flow of splanchnic circulationIncreased flow of splanchnic circulation

Esophageal VaricesEsophageal Varices
Result of portal Result of portal hypertensionhypertension
Form when HVPG is Form when HVPG is >10 mm/hg>10 mm/hg
Bleed with HVPG is Bleed with HVPG is >12 mm/hg>12 mm/hg
Consider non-Consider non-selective b-blockers in selective b-blockers in those with large those with large varicesvarices

Conditions associated with Conditions associated with cirrhositcirrhosit
– Name the conditionsName the conditions

Isolated Gastric VaricesIsolated Gastric Varices
Consider:Consider:– Splenic vein Splenic vein
thrombosis with thrombosis with chronic pancreatitischronic pancreatitis
– TraumaTrauma– MalignancyMalignancy
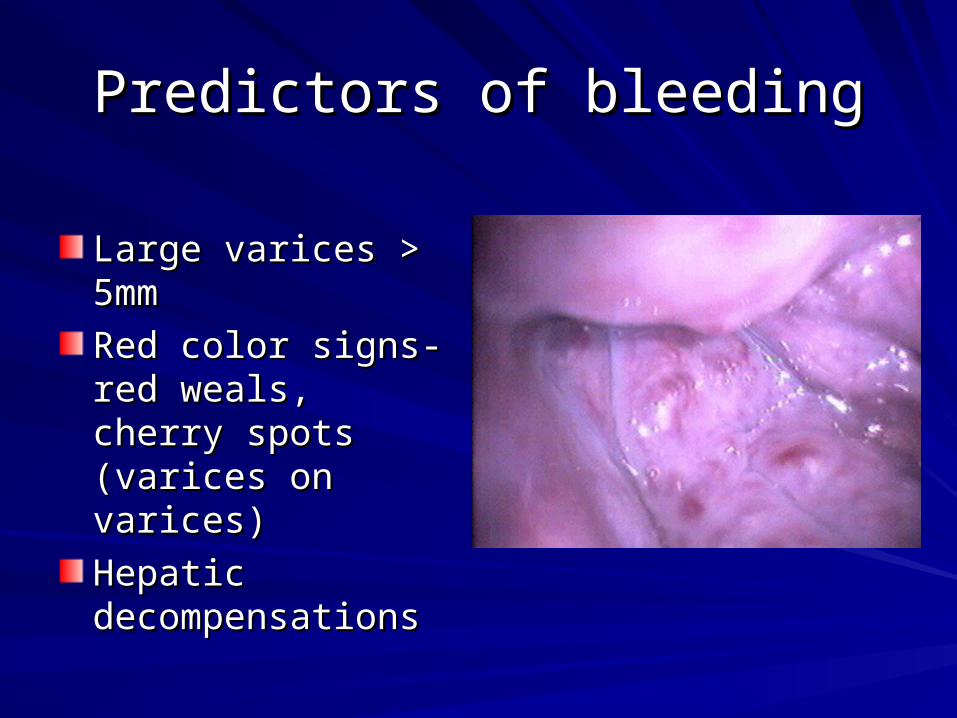
Predictors of bleedingPredictors of bleeding
Large varices > 5mmLarge varices > 5mm
Red color signs-red Red color signs-red weals, cherry spots weals, cherry spots (varices on varices)(varices on varices)
Hepatic Hepatic decompensationsdecompensations
Variceal prophylaxisVariceal prophylaxis
B-blockers including propanolol, nadololB-blockers including propanolol, nadolol
Caution with RAD/COPDCaution with RAD/COPD
Caution with hypoglycemic unawarenessCaution with hypoglycemic unawareness
Goal to reduce HR by 25% HR not less Goal to reduce HR by 25% HR not less than 55/min Systolic >90 mm/hgthan 55/min Systolic >90 mm/hg

Variceal prophylaxis Variceal prophylaxis
EVBL similar success EVBL similar success in preventing first in preventing first variceal hemorrhagevariceal hemorrhage
Sclerotherapy for Sclerotherapy for primary prophylaxisprimary prophylaxis
TIPS not indicated for TIPS not indicated for primary prophylaxisprimary prophylaxis

Acute variceal bleedingAcute variceal bleeding
ResusitationResusitation
NG tube or Ewald tubeNG tube or Ewald tube
Treat coagulopathy with FFPTreat coagulopathy with FFP
Transfuse to H/H of 8/24Transfuse to H/H of 8/24
Intubate for massive bleeds or if Intubate for massive bleeds or if compromised mental statuscompromised mental status
ABX x 7 daysABX x 7 days

Variceal BleedingVariceal Bleeding
Both EVBL and sclerotherapy can achieve Both EVBL and sclerotherapy can achieve hemostasis in 80-90% of caseshemostasis in 80-90% of cases
Sclerotherapy may be achieved with Sclerotherapy may be achieved with ethanolamine, tetradecyl sulfateethanolamine, tetradecyl sulfate– Mucosal ulceration->bleedMucosal ulceration->bleed– Esophageal perforationEsophageal perforation– MediastinitisMediastinitis– Stricture (dysphagia)Stricture (dysphagia)

Varices-TherapyVarices-Therapy
Vasopressin controls bleeding Vasopressin controls bleeding
50% risk of myocardial or mesenteric 50% risk of myocardial or mesenteric ischemia (consider addition of ischemia (consider addition of nitroglycerin)nitroglycerin)
Octreotide bolus 50-100 mcg with Octreotide bolus 50-100 mcg with additional 50 mcg/hr (typically 3-5 days)additional 50 mcg/hr (typically 3-5 days)
Combination of EVBL with octreotide Combination of EVBL with octreotide more effective than either alonemore effective than either alone

Varices-TherapyVarices-Therapy
Balloon tamponade- consider in failure of Balloon tamponade- consider in failure of endoscopic therapy/pharmacologic endoscopic therapy/pharmacologic therapytherapyMay inflate only the gastric balloon-do not May inflate only the gastric balloon-do not keep esophageal balloon inflated greater keep esophageal balloon inflated greater than 24 hrsthan 24 hrsTIPS as rescue therapy in 10-20% who fail TIPS as rescue therapy in 10-20% who fail medical therapy (less mortality than medical therapy (less mortality than surgical shunts) surgical shunts)

Material coveredMaterial covered
Hepatic decompensationsHepatic decompensations
Hepatic encephalopathyHepatic encephalopathy– Treatment/precipitating factorsTreatment/precipitating factors
SBPSBP– Differentiate from secondary peritonitisDifferentiate from secondary peritonitis
Variceal bleeding (portal HTN bleeding)Variceal bleeding (portal HTN bleeding)– Treatment and prophylaxis Treatment and prophylaxis

QuestionsQuestionsMCM 30 Oct 2011MCM 30 Oct 2011


















