Differentiating malignant and benign necrotic lung lesions ...

of 16
Upload
dudi-uchihaCategory
view
219download
07/28/2019 Benign Lung Tumor
1/16
BENIGN LUNG TUMOR
I. INTRODUCTION
Tumors are neoplasms in which an abnormal growth of new tissue. This situation is
caused by abnormal growth and differentiation genes that control the damage or apoptosis of
cells. In medical term, a tumor known as neoplasia. Neo means new, plasia means growth /
division, so neoplasia refers to the growth of new cells, which differs from surrounding cells
those are normally grow. There are two main functions of our cells, namely implementing its
functional activity and multiply by dividing. However, in tumor cells that occur, most of the
cell's energy is used exclusively for proliferation. This proliferation function regulated by the
nucleus of the cell (nucleus), resulting in tumor cells found that the cell nucleus is enlarged
because of increased work demands. Lung is an elastic organ and is located inside the cone-
shaped chest cavity (cavum thoracis). Lung tumors are one type of tumor is difficult to cure.
These tumors are caused by cells that divide and grow uncontrollably in the pulmonary organs.
Lung tumors can be classified to two of the primary lung tumors and secondary lung tumors.
Primary lung tumors can be divided into benign and malignant tumors. From the above
definitions of tumors, the tumors were divided form the two major categories of benign tumors
(benign) and malignant tumors (malignant) or popularly called as cancer. There are significant
differences in the nature of them. Rare benign lung tumor usually found incidentally on routineexamination because benign tumors are rarely giving a complaint and grow very slowly. Benign
lung tumors that are often encountered is Hamartoma. Other types of benign tumor that is the
fibroma, lipoma and others very rarely found. Solitary pulmonary nodules found on the level of
1-2 per 1000 chest radiography. Approximately 30% of the nodules proved to be malignant.
From the remaining nodules, benign lung tumors makes about 2-5% of primary lung tumors.
Benign lung tumors are a heterogeneous group of neoplastic lesions from lung structures. These
tumors include bronchial adenomas, hamartomas, and unusual group of neoplasms (eg,
chondromas, fibromas, lipomas, leiomyomas, hemangiomas, teratomas, pseudolymphomas,
endometriosis, and bronchial glomus tumors).1,2,3,4
7/28/2019 Benign Lung Tumor
2/16
Many of malignant lung tumors, are also found as carcinoma bronchogen because most
of primary malignant tumor originating from the lower respiratory system are derived from
epithelial and mucosal bronchial branching. Secondary lung tumors are more common than
primary lung tumors. Travel or metastasis from elsewhere to the lung usually haematogenous,
limfogen or directly. Usually tumors that metastasize to the lungs was already very advanced or
in high stage. Malignant tumors of other organs that often metastasize to the lungs, among others
osteosarkoma, breast carcinoma, breast carcinoma, carcinoma of the skin and womb.1,2,3,4
II. INCIDENCE
Benign lung tumors are rarely encountered that is only about 2-5% of all primary lung
tumors. In America malignant lung tumors in the reported cause of death as many as 136 000
people a year (1987). Most of cases are occur with patient over 35 years old. The highest
incidence occurred at the age of 55-65 years and men are more than women with a ratio of 4:1.
Although benign lung tumors do not cause significant health problems, complications can result
from obstructive lesions that can affect the patient's pneumonia, atelectasis, and hemoptysis.
Exact incidence is unknown because these tumors are often asymptomatic and detected only
during autopsy.1,2,3,4
III. DIVISION
Benign epithelial tumours Benign tumours arising from the submucosal glands
Sclerosing pneumocytoma
Alveolar adenoma
Squamous papilomaBenign mesenchymal tumours Hamartoma
Lipoma
Leiomyoma
Granular cell tumors
7/28/2019 Benign Lung Tumor
3/16
Benign tumors arising from submucosal glands
Most tumours of the submucosal glands are of low grade malignancy and form a small
subgroup of bronchopulmunary carcinoma. Benign tumours of the submucosal glands are even
rarer than their malignant counterparts. They include mucous cell adenoma, pleomorphic
adenoma and oncocytoma. All these tumours tend to affect young adults and even children and
are unrelated to smoking. They often grow as an intrabronchial polyp.
Pleomorphic adenoma shows a mixed pattern of differentiation with both connective
tissue and epithelial components the former probably representing metaplasia of their
myoeepithelial elements. Oncocytoma is an adenoma of unusual appearance due to cytoplasm
being packed with large number of mitochondria which are apparently inactive. This is taken to
represent a degenerative change. Similar large eosinophilic cells are sometimes found in the
ducts of otherwise normal submucosal glands. In spite of their name, these tumours are quite
benign.8
Sclerosing pneumocytoma
These benign tumours are found in the periphery of the lung. They are more common in
women than in men and affect populations in the far East more than elsewhere. There is marked
vascular and less evident epithelial component. Although originally believed to be angiomatous
in nature or even mesothelial it is probable that these tumours arise from epithelial alveolar
lining cells and the term sclerosing pneumocytoma is therefore preferred to the older one of
sclerosing haemangioma.8
Alveolar adenoma
These will-circumscribed tumours arise in the periphery of the lung of elderly patient.
They resemble lymphangiomas microscopically but the flattened cells that line their narrow
spaces are epithelial rather than endothelial and they are possibly related to the sclerosing
pneumocytoma described above. Their nature is generally only recognised once they are excised,
following which they do not recur.8
7/28/2019 Benign Lung Tumor
4/16
Squamous papillomas
Squamous papillomas may be solitary or multiple, the latter forming the condition known
as juvenile papillomatosis. This condition most commonly affects the larynx but may extend into
the trachea or large bronchi and very rarely into the distal lung. The onset is generally before the
age of 11 years and most examples regress before puberty. However repeated laser therapy may
first be required, because the lesions are prone or recur. Multiple laryngeal, tracheal and
bronchial papillomas cause hoarseness, stridor, and respiratory obstruction, while the rare
pulmonary lesions appear on chest radiographs as solid or cystic rounded nodules. The human
papilloma virus is an aetiological factor and types 6 and 11 have been identified in the lesions.
Solitary papillomas are generally found in elderly smokers with human papilloma virus
again involved, although here the virus is of types 16 and 18 rather than 6 and 11. The epithelial
covering can show the whole range of changes described in the development of squamous cell
carcinoma in flat bronchial epithelium: squamous metaplasia, dysplasia, carcinoma in-situ and
invasive tumours. In general, older patients are more likely to have premalignant lesions.
Figure 1
Figure 1 : shows multiple cysts of varying sizes in the right upper and mid-zone with ill
defined opacities in the right lower zone silhouetting the raised right dome of diaphragm8
7/28/2019 Benign Lung Tumor
5/16
Hamartoma
Hamartoma is the most common benign neoplasm of the lung, accounting for up to 8% of
all primary tumours. In dorland`s hamartoma means a benign tumours-likes nodule composed of
an over-growth of mature cells and tissue normally present in the affected part but with
disorganization and often with one elements predominating. Its pathogenesis is currently
believed to involve clonal proliferations of mesenchymal elements. Tumours are typically
composed of cartilage, fibromyxoid stroma, and adipose tissue along with incorporated
bronchiolar epithelium and less common diverse elements such as bone or hair. Incidence of
Hamartomas occurs more frequently in men, and the mean age at presentation is the six decade,
with only rare cases described before the third decade of life. Many cases of Hamartomas
unrecognized and are found only at autopsy.9
Hamartoma typically present as a solitary pulmonary nodule, usually discovered
incidentally on chest films or during the course of a surgical procedure for another indication.
Most patient are completely asymptomatic. An exception is the endobronchial hamartoma, which
represents fewer than 20% of cases. Patient with endobronchial hamartoma often complain of
cough, dyspnea, wheezing, and occasionally hemoptysis.9
Radiographically, hamartoma are usually solitarybut multiple nodules have been reported
in up to 3% of cases. The nodules are typically smooth, lobulated, peripheral lesions,
approximately 0.5 to 3 cm in diameter. These tumours grow very slowly. Classically, hamartoma
have an eccentric `popcorn` calcification pattern on plain chest radiographs. Calcification can be
seen more frequently and to better advantage by CT-Scan. These scan may also reveal central fat
within the lesion, a distinctive and characteristic finding in hamartoma. If a diagnostic workup is
pursued, then transthoracic needle aspiration should be performed, as it has proven diagnostic
yield of greater than 85%. Biopsy-proven hamartomas can be safely observed with out specific
therapy. Excision is warranted when patients have symptoms or when lesions demonstratesignificant growth. Lung-sparing surgical resection is the treatment of choice because
hamartomas rarely recur. No additional adjuvant therapy is required for the typical case.9
7/28/2019 Benign Lung Tumor
6/16
Figure 2 : `popcorn` calcification pattern on plain chest radiographs
Figure 3 : computed tomography scan after intravenous contrast demonstrate the presense of
calsification and fat within the hamartoma
7/28/2019 Benign Lung Tumor
7/16
Lipoma
Lipomas are the most frequent tumors of the body, 'pulmonary' lipomas are very rare.
Endobronchial lipomas have an incidence of 0.1 to 0.5% of all lung tumors. Lipomas, as benign
pulmonary tumors, can be found endobronchially, intrapulmonary, and mediastinal. Lipomas
may arise within a bronchus or the periphery of the lung. They are probably one-sided
developments of the mixed mesenchymoma referred to hamartomas. They have no premalignant
connotation. Computer tomography can suggest this diagnosis because the tumours have the
radiolucency of fat. Cough as the most frequent complaint. The other symptoms include:
increased sputum, hemoptysis, fever, and dyspnea. Eighty percent of patients have abnormalities
on chest radiograph (e.g., atelectasis, consolidation, or mass). Management of lipoma are
resection by bronchoscopy is the first choice of treatment.8
Figure 4 : showed a hilar mass on the right side, with the density of fat (-100 HU),
identified as a hilar lipoma. There was also a large cystic structure in the right upper lobe,
adjacent to the right hilus.
Leiomyoma
As with smooth muscle tumour elsewhere in the body the histological differentiation of
benign leiomyoma from low-grade leiomyosarcoma is difficult. However, in the lung most
smooth muscle are benign. They may be found in the trachea, bronchi, or in association with
peripheral bronchioles. In all cases the possibility of metastasis from another site, such as a low
grade leiomyosarcoma of the uterus should be considered. Pulmonary leiomyoma seem to to
occur with about equel frequency in the proximal bronchi and parenchyme.8
7/28/2019 Benign Lung Tumor
8/16
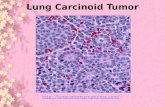
Granular cell tumour
Granular cell tumors (GCT) are uncommon, usually benign neoplasms, most frequently
originating from tongue, skin, and breast. Granular cell tumour were originally believed to be
derived from smooth muscle but it is now accepted that they are benign lesions derived from
schwann cells. As seen with nerve shealth tumours, they express the S100 neural marker but are
composed of polygonal rather than spindle cells and have abundant eosinophilic cytoplasm . The
lesions are usually small but may occasionally measure several centimetres in diameter. They
occurs in the major airway present with obstructive symptoms. Histologically the outstanding
feature is numerous fine, acidophilic, cytoplasmic granules, which appear similar to lysosomes
under electron microscopy.8
Figure 5 : Chest radiograph showing a mass lesion (arrow) intimately associated with a
segmental bronchus of the left lower lobe. Although Chest computed tomogram showing
localized expansion of mass, which measured 2.8 2.0 cm in size.
IV. ETIOLOGY
The cause of benign lung tumors till now is not understood certainty. While pulmonary
malignant tumors according to the ACS (the American Cancer Society) for more than eight out
of 10 cases of lung cancer caused by smoking. And not only the cigarette as the cause but alsothe cigar and pipe smokers have a higher risk for lung cancer. The number of smokers each year,
the number of smokers every day and how long the person inhaled smoke are at risk for
developing lung cancer. The development of lung cancer through passive smoking also increases
the exposed through the air when someone else smokes.1,4,5,7
7/28/2019 Benign Lung Tumor
9/16
A carcinogen is found in air is 3.4 benzpiren pollution. In certain circumstances
bronchogenic carcinoma is a disease caused by work. From various industrial materials, one of
the most dangerous is asbestos. The risk of cancer due to asbestos 10 times greater. There is also
an increased risk among those who work with uranium, chromate, arsenic, iron and iron oxide.
Lung cancer risk either due to contact with asbestos and uranium is greater if the person is
smoking.1,4,5,7
Other factors may also play a role in increasing the risk of lung cancer is diet and
environment especially family. Some research shows that smokers of low vitamin A diets
increase the risk of lung cancer. The loss of chromosomes (partial 11p, 13q, 17p, and 3p) tumor
gene mutations suppressor (p53, Hap-1, ErbAb etc.) and others that implicate familial factors in
the formation of lung cancer. The factors that have been in explaining this clearly states that
although smoking plays a central role in increasing the incidence of lung cancer but also many
guidelines that state that smoking is not the only factor. Chronic infection, caused by air
marshals in motor vehicles and industrial work that led to contact with carcinogenic substances,
dietary factors, family factors and perhaps other factors are not learned and is a predisposing the
occurrence of lung cancer.6
V. ANATOMY AND PHYSIOLOGY
The lungs are the essential organs of respiration; they are two in number, placed one on
either side within the thorax, and separated from each other by the heart and other contents of the
mediastinum. The substance of the lung is of a light, porous, spongy texture; it floats in water,
and crepitates when handled, owing to the presence of air in the alveoli; it is also highly elastic;
hence the retracted state of these organs when they are removed from the closed cavity of the
thorax. The surface is smooth, shining, and marked out into numerous polyhedral areas,
indicating the lobules of the organ: each of these areas is crossed by numerous lighter lines. 10
7/28/2019 Benign Lung Tumor
10/16
Figure 6 : Front view of the lungs
Each lung is conical in shape, and presents for examination an apex, a base, three
borders, and two surfaces. The apex (apex pulmonis) is rounded, and extends into the root of
the neck, reaching from 2.5 to 4 cm. above the level of the sternal end of the first rib. A sulcus
produced by the subclavian artery as it curves in front of the pleura runs upward and lateral ward
immediately below the apex. The base (basis pulmonis) is broad, concave, and rests upon the
convex surface of the diaphragm, which separates the right lung from the right lobe of the liver,
and the left lung from the left lobe of the liver, the stomach, and the spleen. Since the diaphragm
extends higher on the right than on the left side, the concavity on the base of the right lung is
deeper than that on the left. Laterally and behind, the base is bounded by a thin, sharp margin
which projects for some distance into the phrenicocostal sinus of the pleura, between the lower
ribs and the costal attachment of the diaphragm. The base of the lung descends during inspiration
and ascends during expiration.10
7/28/2019 Benign Lung Tumor
11/16
Figure 7 : Anatomy of lungs
Both lungs are filling most of the thorax cavity of each is wrapped by two membrane
called the pleura. Larger right lung and has three lobes while the left lung has two lobes. Each
lobe is further towards bronkhopulmuner segments each have segment bronchus. Tracheal
branching will end up with two main branches of lung bronchi of the right bronchus and left
bronchi. In the lungs there are branching bronchi again to form secondary and tertiary bronchi.
Furthermore, a small bronkhiolus and ends with bronkhiolus terminalis. The final part of
bronkhiolus terminalis called alveoli. Alveoli sacs in the form of thematic clusters of alveoli at
the end of the bronchial terminalis. Each lung consists of 300 million alveoli with a surface area
of 40-80m2. The alveoli are lined by a delicate layer of simple squamous epithelium, the cells of
which are united at their edges by cement substance. Between the squames are here and there
smaller, polygonal, nucleated cells. Outside the epithelial lining is a little delicate connective
tissue containing numerous elastic fibers and a close net-work of blood capillaries, and forming a
common wall to adjacent alveoli. Inoxygenate of blood in the heart are taken into the lungs
through the arteries to the bronchi will pulmunalis and bronkhiolus. Oxygenate blood of thesystem will pass through the capillary-venule venule pulmuner who will unite to form veana
pulmunalis. Lymph channels in the lungs is a closed channel which is located between alveolar
cells and on arterial pulmunalis endhothelium. Lymphatic fluid carry proteins, lipids, dead cells
and foreign particles away from the lungs intersisiel space which plays an important role in lung
defense system from disease.10
7/28/2019 Benign Lung Tumor
12/16
Contraction and relaxation of muscles in the chest and diaphragm occur if done
inspiration and expiration. As inspiration, the diaphragm and intercostal muscles will contract. In
expiration, the diaphragm and intercostal muscles relax. Respiration center located at the brain
stem controls breathing. Oxygen is obtained from the process of inspiration, through the alveoli
into the blood vessels,then will then be taken to the left side of the heart through pulmonary
veins to be pumped to the entire body. Deoxygenated blood from the body will flow to the right
side of heart to be pumped back into the lungs through the pulmonary artery. Carbon dioxide
from the capillaries will enter into the alveoli and then flow into the alveolar space and will be
released through the expiration process.10
VI. PATHOPHYSIOLOGY
Pathogenesis of primary lung tumors either benign or malignant is less understandable.
Nomenclature of benign and malignant lung tumors based on histological. Neoplastic lesions is a
proliferative lesion of autonomous cells without the normal control mechanisms of their growth.
Neoplastic lesion characterized by the proliferation of autonomous cells with no response to
normal control mechanisms that regulate their growth. An additional characteristic of benign
tumors is an extension without an invasive local tissue or spread to other sites.3
7/28/2019 Benign Lung Tumor
13/16
For secondary lung tumors, there are two prominent mechanisms of cancer spread to the
lungs those are direct extension and true metastatic. Usually a direct extension of primary tumors
involving other organs (such as thyroid, esophagus, and thymus) or derived from the tumor
metastases to other intrathoracal structure (eg mediastinal lymph glands), which generally causes
obstructive abnormalities in the trachea or bronchus. Direct extension can also occur through
blood flow, like the spread of cancer cells from the kidney or testis as thrombus that is carried
within vascular into the lungs via the inferior vena cava and the right heart. True metastatic
occurs through the pulmonary artery, bronchial arteries or lymphatic system or the lungs, pleural
cavity or through the airway passage.3
VII. CLINICAL SYMPTOMS
Most of primary lung tumors are already found in an advanced stage. In the advanced
stage there is no lung cancer patients who do not have any complaints and clinical symptoms.
Conversely in the early stages of this disease is sometimes a long time does not cause significant
complaints or clinical symptoms. Complaints and symptoms of lung cancer originating from
airway disorders, the emphasis into the surrounding organs and metastases. Disturbances in the
respiratory tract causing symptoms such as cough and haemoptysis. Tumors in the central region
generally give symptoms of cough because intrabronchial irritation. Shortness of breath may
caused by bronchial obstruction. Pressure and infiltration of surrounding organs can lead to
dysphagia, pain, dyspnoea so that it can happen intrabronkial tumor capillary rupture. Metastasis
via the bloodstream can attack and organ systems as far as the other lymph glands and liver most
frequently in children and kidney, brain, bone and kidney rarest.7,8,9
VIII. DIAGNOSIS
Diagnosis of lung tumors can be decided through the anamnesis of the major complaintsand other complaint that was followed at the same time of chief complaint. Also asked about
smoking habits, how stem spent each day, how long these habits and when to stop. Also related
to air pollution in the workplace or home environment.10
7/28/2019 Benign Lung Tumor
14/16
On physical examination noted a general state of patients according to Karnofsky scale,
deformities and thoracic movement, voice change, enlargement of lymph glands, especially in
the area of supraclavicular. Investigations including routine laboratory examinations of blood,
sputum cytology, liver function, kidney function, and others. Thoracic radiology examination is
an absolute must to determine the exact location of the tumor. Bonchoscopy inspection is also
important to be done. Transthoracal biopsy or transthoracic needle aspiration biopsy is useful to
determine the histological or cytological diagnosis, by taking material directly from the tumor. In
addition to lung cancer TNM classificationthere is also UICC & AICC 1987 staging.7
T Primary tumor
TX
T0
Tis
T1
T2
T3
T4
Primary tumor can not be assessed
The tumor did not appear
Carcinoma in situ
Tumor 3 cm
Tumors> 3 cm invasion into the pleural visceralis followed by atelectasis or obstructive
pneumonitis
Tumors of various sizes which infiltrated the thoracic wall, diaphragm, mediastinal pleura,
parietal pericardium
Tumors of various sizes which infiltrated the mediastinum, heart, great vessels, trachea,
esophagus, spinal
7/28/2019 Benign Lung Tumor
15/16
N Regional lymph nodes
NX
N0
N1
N2
N3
Regional lymph nodes can not be assessed
There was no metastasis to regional lymph nodes
Metastases in the lymph glands on the same side or same side of the hilum
Mediastinal metastases the same side and / or glandular subkarina
Contralateral mediastinal metastases, contralateral hilum lymph nodes
M Distant metastases
MX
M0
M1
Can not be in the assessed of distant metastases
No distant metastasis
There are distant metastases
IX. MANAGEMENT
Benign lung tumors were best treated by surgical resection of the tumor. The extent of
surgery may be simple endoscopic resection, thoracotomy with bronchotomy/local excision,
segmental resection, lobectomy, sleeve resection, or pneumonectomy. The extent is usually
determined at surgery and is as conservative as possible. Endoscopic resection using the rigid
bronchoscope is readily used to resect endobronchial benign lung tumors except for bronchial
adenomas. Recently, bronchoscopic resection offers an alternative to surgical resection. At 1 and
10 years, respectively, 100% and 94% of completely resected carcinoids were free of disease.
Commonly, surgical resection is recommended for bronchial adenomas because of the potentialfor malignancy. The surgical approach should include complete resection, sparing of as much
lung as possible, and lymph node dissection. Endoscopic resection with neodymium: yttrium-
aluminum-garnet (Nd:YAG) laser can be used for adenoma in high-risk or elderly patients.7,9,10
7/28/2019 Benign Lung Tumor
16/16
Treatment of malignant lung tumors or lung cancer based on histopathological type,
degree (stage, stage) and appearance (performance status) patients. In general, this treatment is a
combination of surgery, radiation or chemotherapy and consumption of cytostatic Lung
carcinoma surgery called as curative treatment if the tumor was carried out and the perfect gland
dissection accompanied by pathological examination found no metastasis to the gland that was
lifted. Patients with extensive-stage disease was handled with only chemotherapy. Several
combination chemotherapy regimens were often used consisted of cyclophosphamide and
doxorubicin.7,9,10
X. PROGNOSIS
Prognosis of benign lung tumors such as bronchial adenoma which has been operated is
good. Reported 5 years survival rates after resection reached 95% and will decrease to 70% if
regional lymph nodes are affected. Overall prognosis for patients with carcinoma bronkogenik is
bad. If there are any symptoms or signs of disease were 75% was not able to recover again. For
patients who had made the diagnosis, one-year survival reached 20%, 5 years survival rates less
than 10% and only slightly increased in recent years.4