Back Pain in Pregnancy: Etiology and Treatment Strategies By: Fredrick P. Wilson, D.O.
32
Back Pain in Back Pain in Pregnancy: Etiology Pregnancy: Etiology and Treatment and Treatment Strategies Strategies By: By: Fredrick P. Wilson, D.O. Fredrick P. Wilson, D.O.
-
Upload
eleanore-newton -
Category
Documents
-
view
215 -
download
0
Transcript of Back Pain in Pregnancy: Etiology and Treatment Strategies By: Fredrick P. Wilson, D.O.

Back Pain in Pregnancy: Back Pain in Pregnancy: Etiology and Treatment Etiology and Treatment
StrategiesStrategies
By:By:
Fredrick P. Wilson, D.O.Fredrick P. Wilson, D.O.

StatisticsStatistics Low back pain occurs in 1/3 to 2/3 of Low back pain occurs in 1/3 to 2/3 of
pregnant womenpregnant women Previous back pain before pregnancy Previous back pain before pregnancy
doubles the risk doubles the risk ~85% of pregnant women will have low ~85% of pregnant women will have low
back/pelvic pain if they had pain with back/pelvic pain if they had pain with their previous pregnancy. 2/3 of these their previous pregnancy. 2/3 of these patients require sick leave during patients require sick leave during pregnancy.pregnancy.
Higher maternal age increases risk of LBPHigher maternal age increases risk of LBP

Causes of Back Pain in Causes of Back Pain in PregnancyPregnancy
Combination of biomechanical factors Combination of biomechanical factors that yield abnormal loading on muscles that yield abnormal loading on muscles and joints and behavioral factors related and joints and behavioral factors related to inadequate patient coping strategiesto inadequate patient coping strategies
Increased ligamental laxity is caused by Increased ligamental laxity is caused by increase in hormones estrogen and increase in hormones estrogen and relaxin. One study showed women most relaxin. One study showed women most incapacitated with low back pain had incapacitated with low back pain had the highest amounts of relaxin.the highest amounts of relaxin.
Herniated discs are rare-1 in 10,000Herniated discs are rare-1 in 10,000

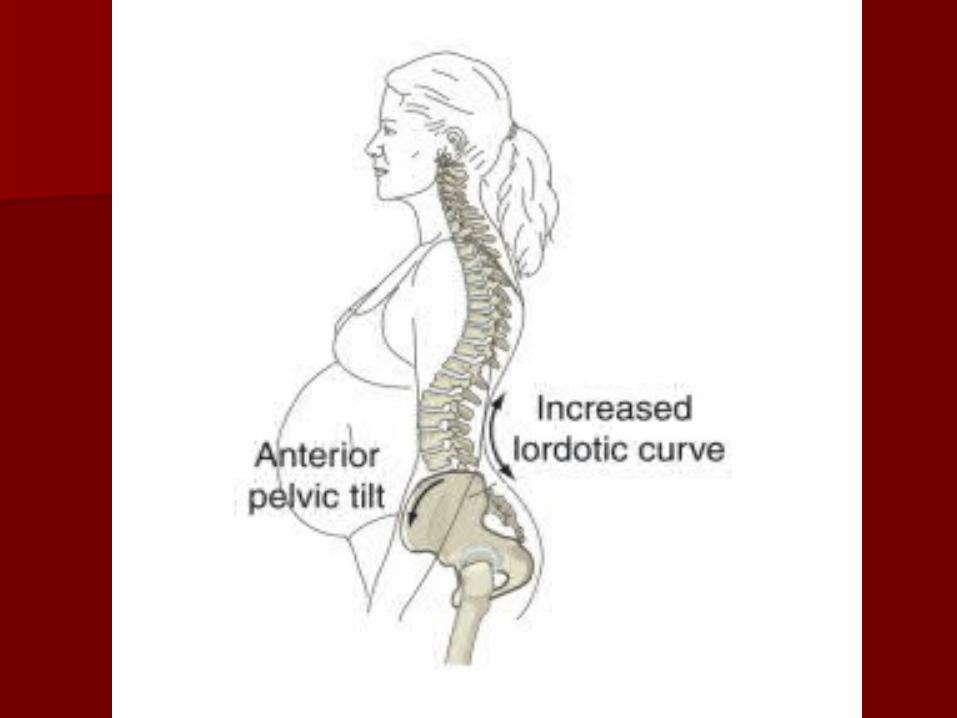
Mechanical Changes in Mechanical Changes in PregnancyPregnancy
Hyperlordosis occurs as the gravid Hyperlordosis occurs as the gravid uterus induces accentuation of the uterus induces accentuation of the anterior pelvic tilt. The sacroiliac joints anterior pelvic tilt. The sacroiliac joints resist this rotation. As pregnancy resist this rotation. As pregnancy progresses, both forward rotation and progresses, both forward rotation and hyperlordosis continue as the sacroiliac hyperlordosis continue as the sacroiliac ligaments become lax. This contributes ligaments become lax. This contributes to increasing mechanical strain on the to increasing mechanical strain on the low back, sacroiliac joints and pelvis.low back, sacroiliac joints and pelvis.


History of Low Back Pain in History of Low Back Pain in PregnancyPregnancy
Low back pain or posterior pelvic Low back pain or posterior pelvic pain aggravated by activity, relieved pain aggravated by activity, relieved by sitting or lying downby sitting or lying down
Most often in third trimesterMost often in third trimester Occasionally into posterior thighs but Occasionally into posterior thighs but
usually not distal to kneesusually not distal to knees Usually persistent but not severeUsually persistent but not severe

Physical ExamPhysical Exam
Standard neuromuscular exam Standard neuromuscular exam including ROM, DTR`s, leg strength including ROM, DTR`s, leg strength and sensationand sensation
Assess leg length standing and supineAssess leg length standing and supine Check standing and seated flexion Check standing and seated flexion
teststests Assess pelvis and sacrum prone if Assess pelvis and sacrum prone if
early enough in the pregnancyearly enough in the pregnancy

Seated Flexion TestSeated Flexion Test


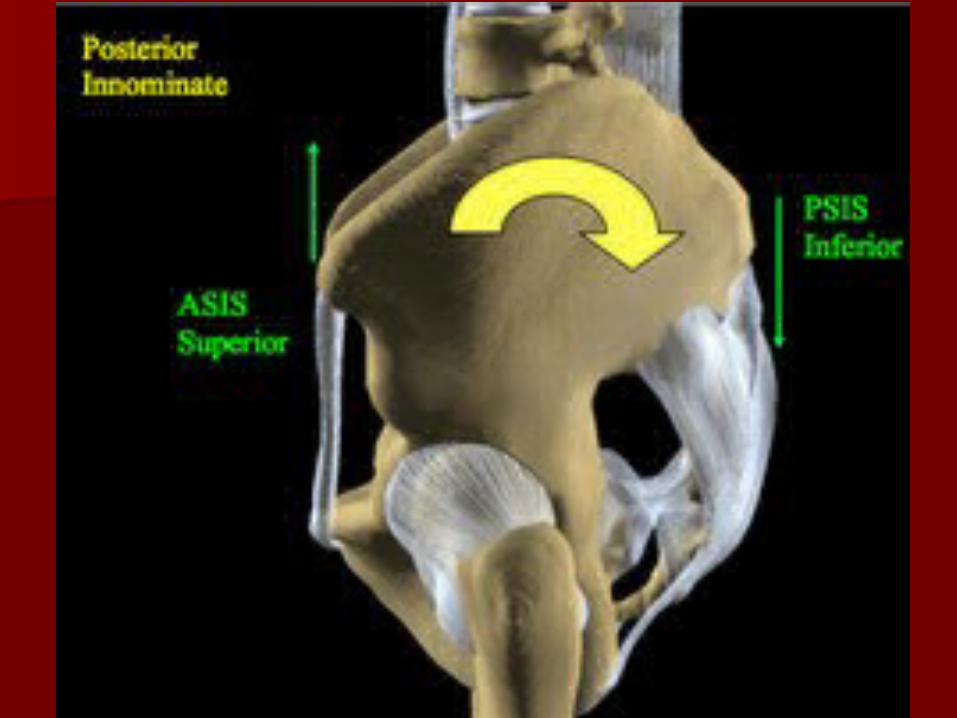

Pelvic RotationPelvic Rotation
Imaging of Pregnant Imaging of Pregnant PatientsPatients
Imaging should be done after the first Imaging should be done after the first trimester trimester onlyonly if symptoms very severe or if symptoms very severe or unusualunusual
Although no recognized biological effects Although no recognized biological effects of MRI`s on the developing fetus have of MRI`s on the developing fetus have been reported, long term effects have not been reported, long term effects have not been conclusively evaluated. MRI should been conclusively evaluated. MRI should be done only if cauda equina symptoms or be done only if cauda equina symptoms or substantial loss of lower extremity substantial loss of lower extremity strengthstrength

Treatment of Back Pain in Treatment of Back Pain in Pregnant PatientsPregnant Patients
PT – Aquatic therapyPT – Aquatic therapy Tylenol for painTylenol for pain NSAID`s can cause premature closure NSAID`s can cause premature closure
of the ductus arteriosus in the fetusof the ductus arteriosus in the fetus Other class B drugs in pregnancy Other class B drugs in pregnancy
include cyclobenzaprine, oxycodone include cyclobenzaprine, oxycodone and prednisoneand prednisone
Care should be coordinated with the Care should be coordinated with the obstetricianobstetrician

Other TreatmentsOther Treatments
Lidocaine patchesLidocaine patches One study used acupuncture which One study used acupuncture which
reduced pain in 72% of pregnant reduced pain in 72% of pregnant womenwomen
Therapeutic US is contraindicated in Therapeutic US is contraindicated in any area that may reach the fetusany area that may reach the fetus
Electric stimulation should not be used Electric stimulation should not be used on low back or abdomen although on low back or abdomen although TEN`s has been used during labor and TEN`s has been used during labor and deliverydelivery

Epidurals/SurgeryEpidurals/Surgery
Epidurals have been done without Epidurals have been done without fluoroscopic guidancefluoroscopic guidance
Surgery has been done for Surgery has been done for progressive neurologic deficit or progressive neurologic deficit or cauda equina syndromecauda equina syndrome

Recent TrialsRecent Trials
Chiropractic joint mobilization, home Chiropractic joint mobilization, home stabilization exercises, education and stabilization exercises, education and reassurance 24-33 weeks gestation. reassurance 24-33 weeks gestation. Significant reduction of pain vs. Significant reduction of pain vs. controlcontrol
Osteopathic manipulation during Osteopathic manipulation during prenatal period: reduced probability prenatal period: reduced probability of meconium-stained amniotic fluid of meconium-stained amniotic fluid and preterm deliveryand preterm delivery

Osteopathic ManipulationOsteopathic Manipulation
Avoid HVLA to low back or pelvisAvoid HVLA to low back or pelvis Use gentle techniques like Use gentle techniques like
strain/counterstrain, Still or muscle strain/counterstrain, Still or muscle energyenergy

Myofascial Release to Myofascial Release to SacrumSacrum

Muscle Energy to Anterior Muscle Energy to Anterior PelvisPelvis

Anterior Pelvis ExerciseAnterior Pelvis Exercise

Muscle Energy to Posterior Muscle Energy to Posterior PelvisPelvis

Posterior Pelvis ExercisePosterior Pelvis Exercise

Still to Anterior PelvisStill to Anterior Pelvis

Still to Anterior PelvisStill to Anterior Pelvis

Still to Anterior PelvisStill to Anterior Pelvis
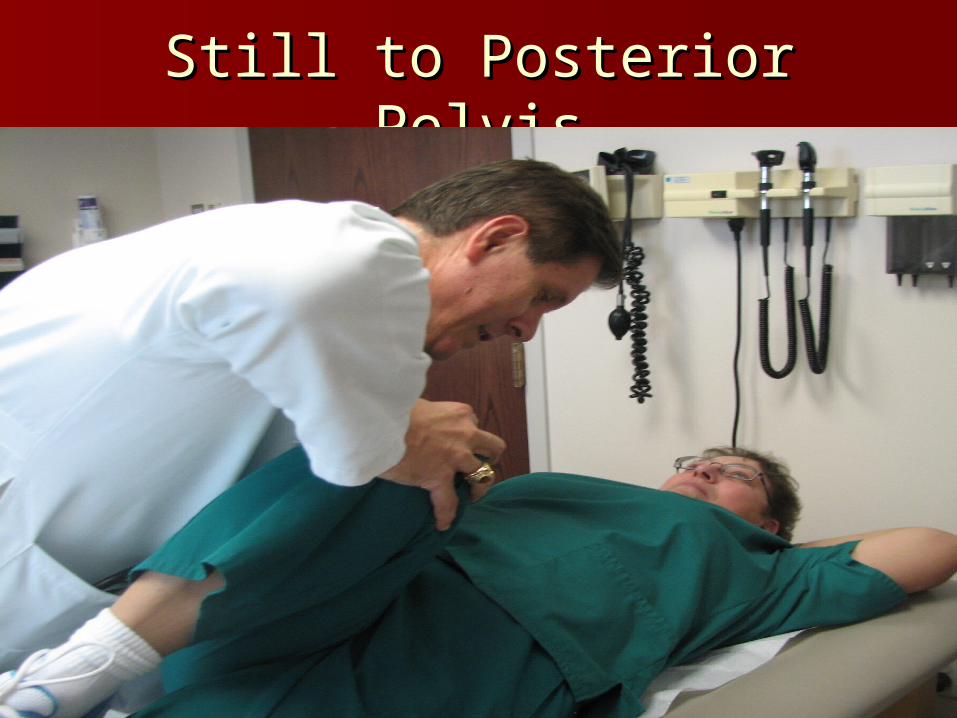
Still to Posterior PelvisStill to Posterior Pelvis



Muscle Energy for Separated Muscle Energy for Separated Pubic SymphysisPubic Symphysis

Thank You!Thank You!