
Real Cases: Bad Outcomes - 15th Annual 2017 Advanced ... · Real Cases: Bad Outcomes Fredrick M....
14
1 Real Cases: Bad Outcomes Fredrick M. Abrahamian, D.O., FACEP, FIDSA Clinical Professor of Medicine UCLA School of Medicine Director of Education Department of Emergency Medicine Olive View-UCLA Medical Center Sylmar, California Case # 1: History 17 y/o male Chief complaint: Throat pain for 4 days In addition, complains of: Difficulty swallowing Weakness Abdominal pain Intermittent fevers No vomiting, CP, or SOB
-
Upload
phunghuong -
Category
Documents
-
view
214 -
download
0
Transcript of Real Cases: Bad Outcomes - 15th Annual 2017 Advanced ... · Real Cases: Bad Outcomes Fredrick M....

1
Real Cases: Bad Outcomes
Fredrick M. Abrahamian, D.O., FACEP, FIDSA
Clinical Professor of Medicine
UCLA School of Medicine
Director of Education
Department of Emergency Medicine
Olive View-UCLA Medical Center
Sylmar, California
Case # 1: History
17 y/o male
Chief complaint: Throat pain for 4 days
In addition, complains of:
Difficulty swallowing
Weakness
Abdominal pain
Intermittent fevers
No vomiting, CP, or SOB

2
Case # 1: History
PMHx: None
Meds: None
Allergies: None
Denies smoking, alcohol or drug use
ROS: Unremarkable
Case # 1: Physical Examination
Vitals on arrival:
BP 145/85 P 125 R 22 T 38.5 ºC (101.3 ºF)
General: In no acute resp. distress but looks ill
Neck: Supple but complains of severe pain;
Very large lymph nodes
Throat: Large exudates over tonsils; no PTA
Resp: CTA; non-labored
Heart: Tachycardic but no murmurs
GI: Diffusely tender but no rebound or guarding

3
Case # 1: ED Course
Orders:
IVF 1 liter NS
Tylenol 650 mg PO
Labs: Rapid strep test negative
Diagnosis:
Viral pharyngitis
Plan: D/C home; F/U with PMD as needed
Nursing D/C notes: Patient looks really tired
Vitals on discharge:
BP 132/82 P 115 R 22 T 37.8 ºC (100.0 ºF)
Case # 1: Follow up
2 weeks later collapses while playing football
Pale, diaphoretic
Complains of severe abdominal pain
Taken by ambulance to hospital
Dx: Splenomegaly & splenic laceration
Underwent splenectomy
EBV serology consistent with acute infection

4
Case # 1: Litigation Claims
Claims:
Failure to consider mononucleosis in DDx
Failure to send diagnostic tests
Failure to provide proper D/C instructions
Defense:
Diagnostic testing may not have been
helpful
Splenic rupture would have occurred
Infectious Mononucleosis
Ball AP, et al. Infectious Diseases.1993.

5
Infectious Mononucleosis
Ball AP. Infectious Diseases 1993. Forbes CD. Color Atlas Medicine. 1993.
Infectious Mononucleosis
Highest incidence in 15-24 years of age
Posterior cervical lymphadenopathy, fatigue
Lymphocytosis with atypical lymphocytes
Monospot test:
1st week of illness with high false-neg rate
Most splenic ruptures occur in 1st 3 wks of illness
Instruct to avoid contact sports for 3-4 weeks
N Engl J Med. 2010;362:1993-2000 [Infectious mononucleosis].

6
Case # 2: History
48 y/o male c/o headache x 2 weeks
Arrives with wife by ambulance
Gradual onset of pain, severe & constant
Multiple episodes of non-bloody vomiting
Reports chills & subjective fever
Complains of photophobia
No CP, SOB, or abdominal pain
Case # 2: History
PMHx: HIV, hypertension
Unknown if has AIDS-defining illness
Unknown last CD4 count
Meds: Multiple meds (unaware of names)
Allergies: None
Denies smoking, alcohol or drug use
ROS: Unremarkable

7
Case # 2: Physical Examination
Vitals on arrival:
BP 198/118 P 98 R 24 T 37.6 ºC (99.7 ºF)
General: In severe distress from headache
HEENT: PERRLA; erythematous oropharynx
Neck: Supple; no lymphadenopathy
Resp: CTA; no wheezing
Heart: Normal rate & rhythm, no murmurs
Abdomen: Normal bowel sounds; non-tender
Neuro: A&O x4; non-focal neuro exam
Case # 2: ED Course
Orders:
IVF 1 liter NS
BMP, CBC, UA
Blood cultures
Head CT
Rocephin 1 gram IV
Vicodin 1 PO
Refused LP
risks….inability to Dx
infection or bleed…..
136
3.1 19
105
0.9
18108
11.56.8
36.4289
Non-contrast head CT:No mass or bleed
Lymphocyte: 10%

8
Case # 2: Hospital Course
Admitted to non-monitored floor
Dx: 1) Severe headache; 2) HIV
Complains of visual changes
Became confused & lethargic ….. apneic
Unable to resuscitate
Autopsy: Cerebral edema, herniation
Final Dx: Cryptococcal meningitis
Case # 2: Litigation Claims
Claims:
Inadequate physical examination
Failure to consider cryptococcal meningitis
Failure to properly warn of all risks
Defense:
Patient refused diagnostic procedure
Outcome would not have changed

9
AIDS & Cryptococcal Meningitis
Majority with no meningismus or fever
Often normal head CT scan & CSF findings
A critical clue is elevated CSF pressure
Antifungal drugs & relief of elevated ICP are
mainstays of therapy
Pressure may be relieved with serial LPs,
ventricular or lumbar drains, CSF shunts
Clin Infect Dis. 2010;50:291-322 [IDSA Practice guidelines].
Case # 3: History
62 y/o female c/o left flank & back pain
Gradual onset of pain 2 weeks ago
Pain described as severe & constant
Admits to chills, subjective fevers,
Complains of dysuria & urinary hesitancy
Pain radiates to abdomen & chest
Multiple episodes of non-bloody vomiting

10
Case # 3: History
PMHx: DM, hypertension, bipolar disease
Hx. of multiple prior UTIs
Meds: Metformin, Glipizide, Benazepril
Allergies: None
Admits to smoking; occasional alcohol use
Denies drug use
ROS: Unremarkable
Case # 3: Physical Examination
Vitals on arrival:
BP 98/50 P 130 R 22 T 38.9 ºC (102 ºF)
General: In severe distress from pain
HEENT: PERRLA; EOMI; normal TMs
Neck: Supple; no lymphadenopathy
Resp: CTA; no wheezing
Heart: Tachycardia, no murmurs
Abdomen: Mild tenderness over LLQ, left CVAT
Neuro: Moves all extremities; normal sensation

11
Case # 3: ED Course
IVF 2 liters NS
Ceftriaxone 1 gram IV
Labs:
CMP, CBC, Lipase
Blood cultures x 2
UA & culture
138
4.0
95
1.8
32425
12.222.3
36.4109
PMNs 89%Bands 15%Toxic vacuolization
16
Nitrite: PositiveLeukocyte esterase: PositiveWBC: 158; RBC: NoneBacteria: Many
Case # 3: ED Course
ED: IVF; insulin drip
Dx: DKA; UTI; possible urosepsis
Admitted to ICU
In ED, complains of increasing pain
Reassessment note:
...... not sure if she is truly in pain ….
part of it may be due to underlying
psychiatric disorder …..
12
Case # 3: Hospital Course
Complains of more back pain & dizziness
Progressively becomes more hypotensive
Requires intubation…arrests….
Unable to resuscitate
Autopsy: Emphysematous pyelonephritis
Case # 3: Litigation Claims
Claims:
Failure to consider emphysematous pyelo
Failure to initiate proper antibiotics
Failure to initiate timely interventions
Defense:
Rare condition
Presentation consistent with urosepsis
Outcome would not have changed
13
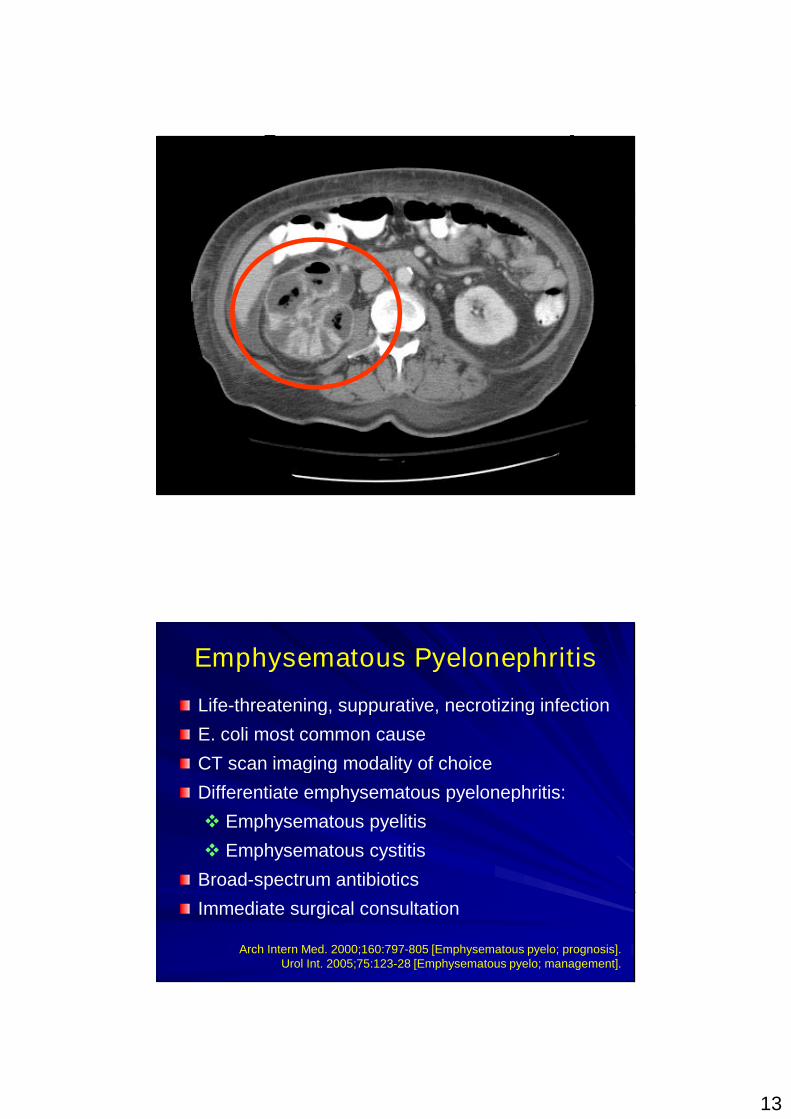
Emphysematous Pyelonephritis
Life-threatening, suppurative, necrotizing infection
E. coli most common cause
CT scan imaging modality of choice
Differentiate emphysematous pyelonephritis:
Emphysematous pyelitis
Emphysematous cystitis
Broad-spectrum antibiotics
Immediate surgical consultation
Arch Intern Med. 2000;160:797-805 [Emphysematous pyelo; prognosis].Urol Int. 2005;75:123-28 [Emphysematous pyelo; management].

14
Medical Take Home Points
Mononucleosis
Monospot test: 1st week with high false-neg rate
Avoid contact sports for 3-4 weeks
Cryptococcal meningitis
Normal CSF values
Critical clue is increased CSF pressure
Emphysematous pyelonephritis
CT scan imaging modality of choice
Immediate surgical consultation
Legal Take Home Points
Documentation:
It is the quality (“key words”), not the quantity
Re-evaluation: Improved, unchanged, worsened
Repeat vitals
Address abnormal labs; know limitations; avoid bias
Beware of the non-fit
Diagnosis doesn’t match S/Sxs & tests
Document refusal of care with all the risks
Avoid attributing physical findings to psychiatric
illness

















![Breaking Bad News PPT[1] - geneticcounselingtoolkit.comgeneticcounselingtoolkit.com/cases/testing_options/Breaking Bad... · Learning Objectives Students will be able to Define bad](https://static.fdocuments.net/doc/165x107/5a7083067f8b9ab1538c09a3/breaking-bad-news-ppt1-geneticcounselingtoolkitcomgeneticcounselingtoolkitcomcasestestingoptionsbreaking.jpg)
