ASMA GRAVE (DE DIFICIL CONTROL) La opción de la...
31
ASMA GRAVE (DE DIFICIL CONTROL) La opción de la fisiopatología L. Prieto Asociación Valenciana de Investigaciones Clínicas Valencia 1 L Prieto Alergonorte, Mayo-2009
Transcript of ASMA GRAVE (DE DIFICIL CONTROL) La opción de la...

ASMA GRAVE (DE DIFICIL CONTROL)
La opción de la fisiopatología
L. Prieto
Asociación Valenciana de Investigaciones Clínicas
Valencia
1
L Prieto Alergonorte, Mayo-2009

ASMA DE DIFICIL CONTROL
PROBABLES ESCENARIOS
ASMA DE DIFICIL CONTROL
(precisa tratamiento de alta intensidad)
Buen control solo
con tratamiento
de alta intensidad
Mal control a pesar
de tratamiento de
alta intensidad
Taylor DR, et al. Eur Respir J. 32: 545. 2008
2
L Prieto Alergonorte, Mayo-2009

Incorrecto diagnóstico
COPD
Insuficiencia cardiaca izquierda
Obstrucción localizada
Fibrosis quística
Disfunción c vocales
Mal cumplimiento terapéutico
Factores psicológicos
Asma inestable
Nocturna
Premenstrual
Labil
Asma cortico-resistente
Asma cortico-dependiente
ASMA DE DIFICIL CONTROL
PROBABLES FACTORES CAUSALESFactores no identificados
Alergenos no identificados
Exposición ocupacional
Afectación vía aérea superior
Rinitis
Sinusitis
Apnea de sueño obstruciva
Reflujo gastro-esofágico
Enfermedades sistémicas
Hipertiroidismo
S carcinoide
Churg-Strauss
Fármacos
-bloqueantes, AINES, inh ACE
Infecciones crónicas
Clamidofilia y micoplasma
Barnes PJ, et al. ERJ. 12: 1209. 1998; ten Brinke et al. ERJ. 26: 812. 2005
Strek ME. Proc Am Thorac Soc. 3: 116. 2006 3
L Prieto Alergonorte, Mayo-2009

Boulet LP. Eur Respir J. 33: 897. 2009
ASMA DE DIFICIL CONTROL
COMORBILIDADES
Que factores condicionan la dificultad
para el control del asma?
1. Diferentes fenotipos inflamatorios?
2. Diferentes fenotipos funcionales?
4
L Prieto Alergonorte, Mayo-2009
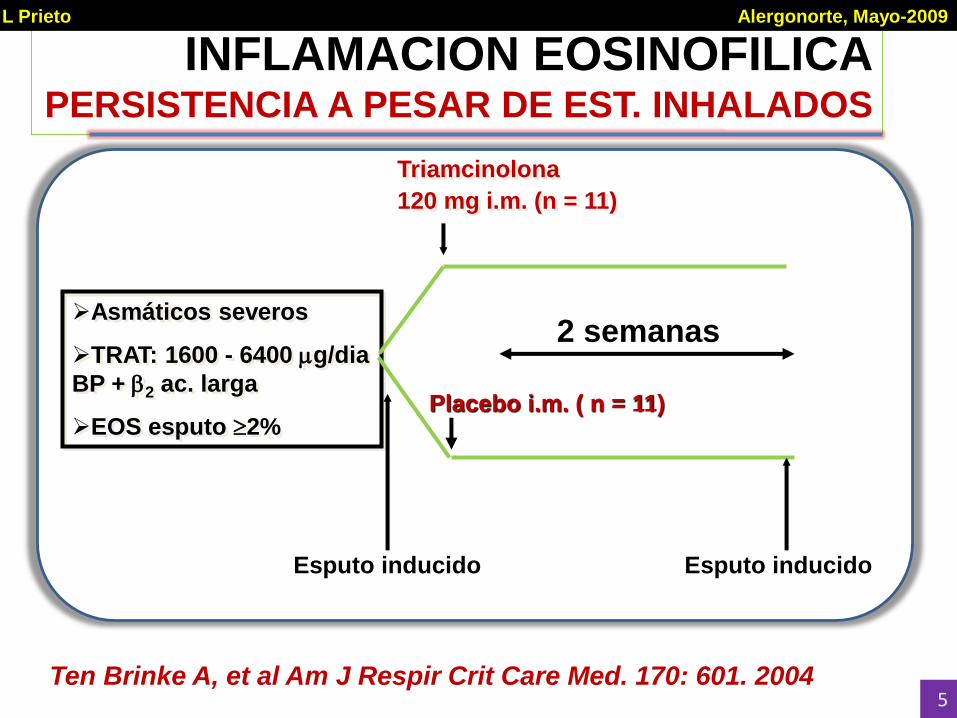
INFLAMACION EOSINOFILICAPERSISTENCIA A PESAR DE EST. INHALADOS
Asmáticos severos
TRAT: 1600 - 6400 g/dia
BP + 2 ac. larga
EOS esputo 2%
Triamcinolona
120 mg i.m. (n = 11)
Placebo i.m. ( n = 11)
2 semanas
Esputo inducido
Ten Brinke A, et al Am J Respir Crit Care Med. 170: 601. 2004
Esputo inducido
5
L Prieto Alergonorte, Mayo-2009

INFLAMACION EOSINOFILICAPERSISTENCIA A PESAR DE EST. INHALADOS
0
25
50
75
PRE POST PRE POST
PLACEBO TRIAMCINOLONA
EO
SIN
OF
ILO
S (
%)
P = 0.49 P <0.001
P <0.001
Ten Brinke A, et al Am J Respir Crit Care Med. 170: 601. 20046
L Prieto Alergonorte, Mayo-2009

0
20
40
60
80
100
ASMA DIFICIL
CONTROL
ASMA NO DIFIC
CONTROL
0
20
40
60
80
100
Eo
sin
ófi
los e
n e
sp
uto
(%
)
Neu
tró
filo
s (
%)
Boulet LP, et al. Respir Med. 97: 739. 2003
NS
P = 0.019
ASMA DE DIFICIL CONTROL IMPORTANCIA DE INFLAMACION NEUTROFILICA
7
L Prieto Alergonorte, Mayo-2009
ASMA DIFICIL
CONTROL
ASMA NO DIFIC
CONTROL

DETERIORO FUNCIONAL EN ASMA
RELACION CON ENO BASAL
FEV1 =>80% teórico FEV1 <80% teórico
P = 0.003
P = NS
Van Veen IH, et al. Eur Respir J. 32: 344. 2008 8
L Prieto Alergonorte, Mayo-2009

OXIDO NITRICO EXHALADO
ASMA DC vs ASMA NO DC
0
25
50
75
100
125
150
ASMA DC
(n=22)
EN
O (
pp
b)
Asma DC, no DC y COPD vs sanos, P <0.05
Asma DC vs no DC vs COPD, P = NS
ASMA NO DC
(n=10)
COPD (n=11) SANOS
(n=13)
9
L Prieto Alergonorte, Mayo-2009

pH del EBC
ASMA DC vs ASMA NO DC
3
4
5
6
7
8
pH
CO
ND
EN
SA
DO
P <0.05
ASMA DC
(n=12)
ASMA NO DC
(n=16)
COPD
(n=15)
SANOS
(n=12)
P <0.05
10
L Prieto Alergonorte, Mayo-2009
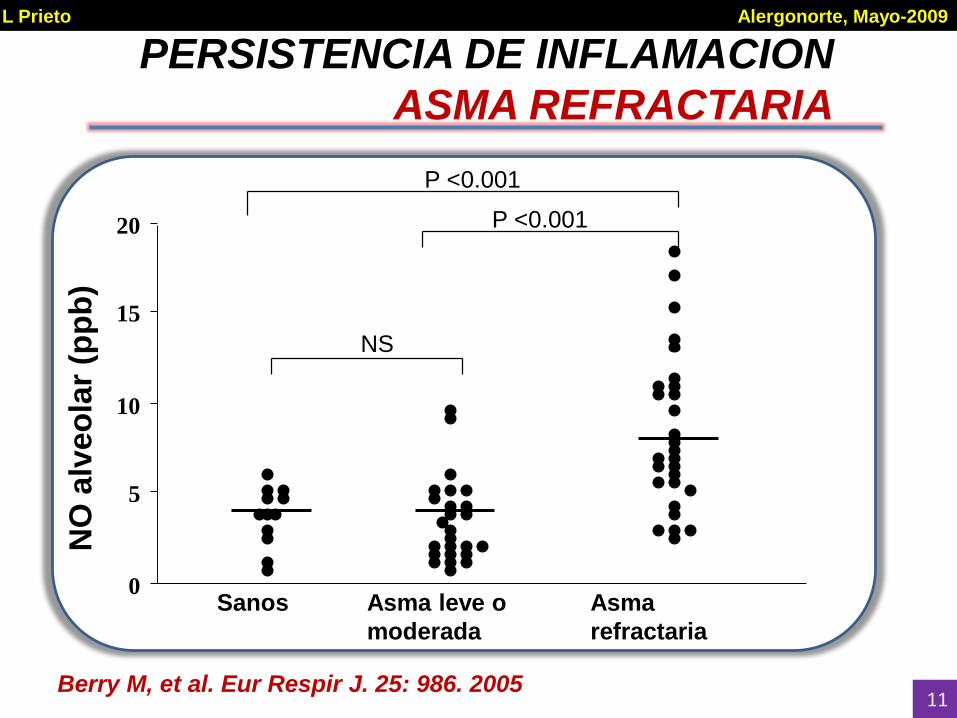
PERSISTENCIA DE INFLAMACION
ASMA REFRACTARIA
Berry M, et al. Eur Respir J. 25: 986. 2005
Sanos
NO
alv
eo
lar
(pp
b)
NS
0
5
10
15
20
Asma leve o
moderada
Asma
refractaria
P <0.001
P <0.001
11
L Prieto Alergonorte, Mayo-2009

Shin, H.-W. et al. J Appl Physiol 96: 65-75 2004
Schematic of 2-compartment model used to describe NO exchange dynamics
12
L Prieto Alergonorte, Mayo-2009
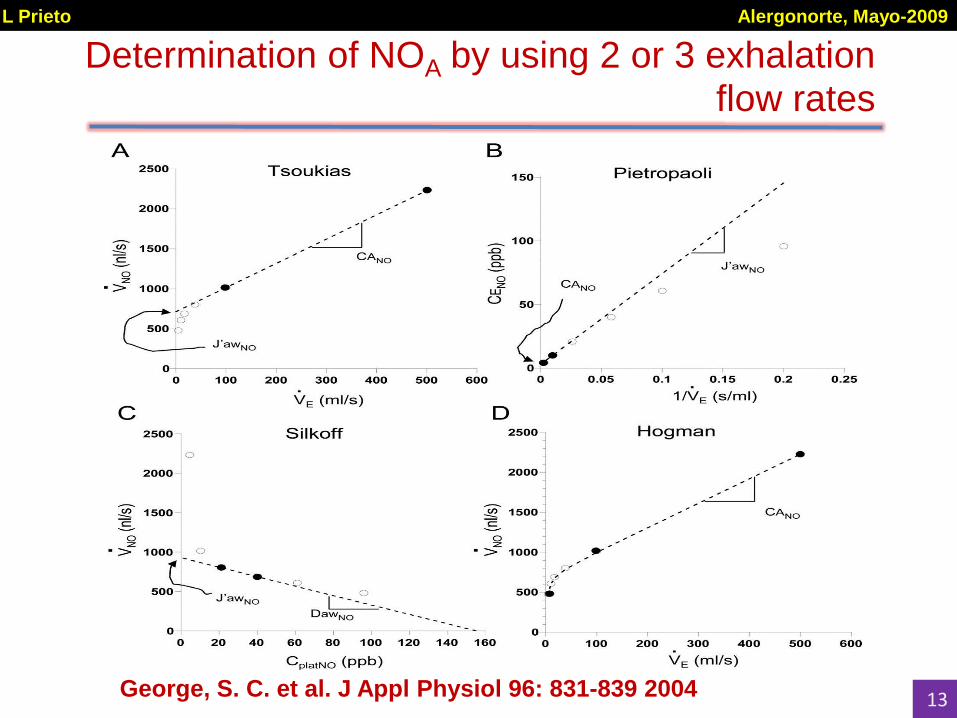
George, S. C. et al. J Appl Physiol 96: 831-839 2004
Determination of NOA by using 2 or 3 exhalation flow rates
13
L Prieto Alergonorte, Mayo-2009

14
Healthy Allergic
rhinitis
DC
Asthma
No DC
Asthma
100
1000
10000
100000
P <0.01
P <0.01
P <0.001
Bro
nch
ial N
O f
lux (
pl/
s)
ASMA DC vs ASMA NO DC
OXIDO NITRICO BRONQUIAL
14
L Prieto Alergonorte, Mayo-2009

15
Healthy Allergic
rhinitis
DC
Asthma
no DC
Asthma
1
10
100P <0.05
Alv
eo
lar
NO
co
ncen
trati
on
(p
pb
)
ASMA DC vs ASMA NO DC
OXIDO NITRICO ALVEOLAR
15
Que factores condicionan la dificultad
para el control del asma?
1. Diferentes fenotipos inflamatorios?
2. Diferentes fenotipos funcionales?
L Prieto Alergonorte, Mayo-2009
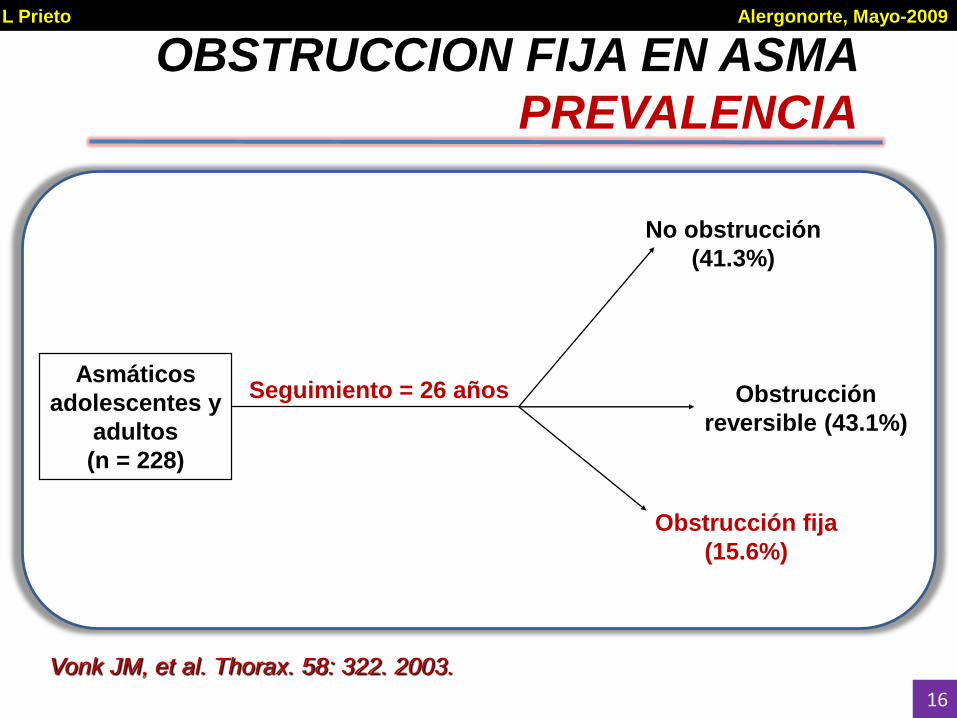
OBSTRUCCION FIJA EN ASMA
PREVALENCIA
Asmáticos
adolescentes y
adultos
(n = 228)
Seguimiento = 26 años
Obstrucción fija
(15.6%)
Obstrucción
reversible (43.1%)
Vonk JM, et al. Thorax. 58: 322. 2003.
No obstrucción
(41.3%)
16
L Prieto Alergonorte, Mayo-2009

OBSTRUCCION FIJA EN ASMA
PREVALENCIA Y FACTORES DE RIESGO
Asmáticos no
fumadores
(n = 92)
Seguimiento = 10 años
Obstrucción fija
(23%)
Obstrucción reversible
(77%)
CARACTERISTICAS BASALES
Obstr. Fija Obstr. Reversible
Edad (años) 3212 3812
FEV1 con 2 (%) 17.23.1 12.83.8*
FEV1 basal (% teórico) 77.619.7 89.118.0
* = P < 0.003
Ulrik and Backer. Eur Respir J. 14: 892. 1999.17
L Prieto Alergonorte, Mayo-2009
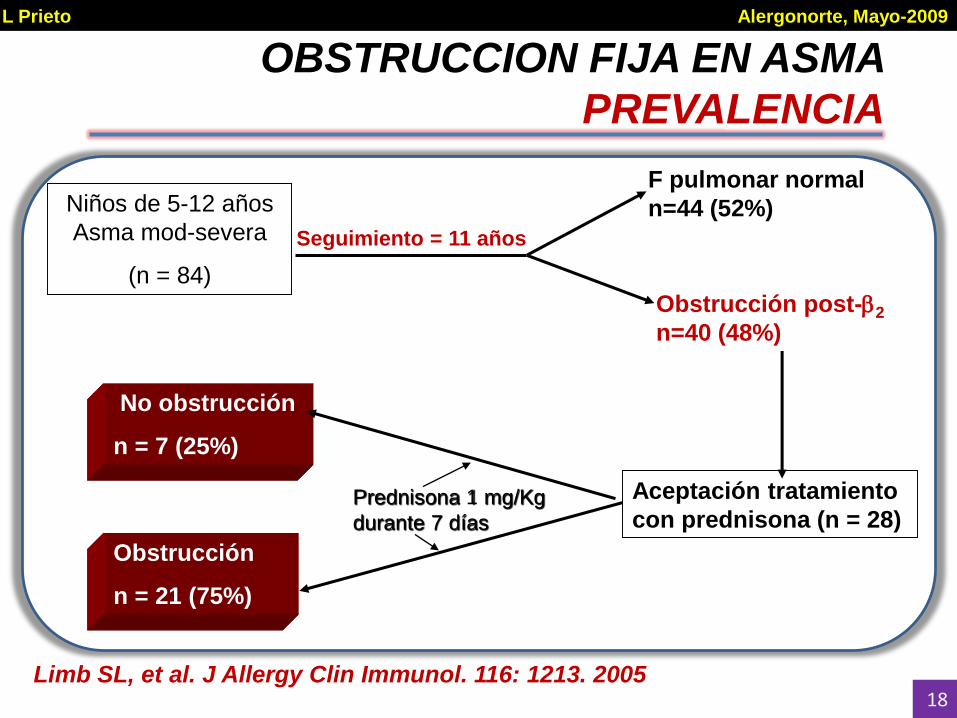
OBSTRUCCION FIJA EN ASMA
PREVALENCIA
Niños de 5-12 años
Asma mod-severa
(n = 84)
F pulmonar normal
n=44 (52%)
Obstrucción post-2
n=40 (48%)
Aceptación tratamiento
con prednisona (n = 28)
Obstrucción
n = 21 (75%)
No obstrucción
n = 7 (25%)
Seguimiento = 11 años
Prednisona 1 mg/Kg
durante 7 días
Limb SL, et al. J Allergy Clin Immunol. 116: 1213. 200518
L Prieto Alergonorte, Mayo-2009

19
L Prieto Alergonorte, Mayo-2009

DETERIORO FUNCIONAL EN ASMA
OBESIDAD COMO FACTOR DE RIESGO
Asmáticos
adultos
(n=638)
Seguimiento = 4 años
Obstrucción basal
(FEV1/FVC <70%)
No obstrucción basal
(FEV1/FVC =>70%)
DETRIORO DEL FEV1
Marcon A, et al. J Allergy Clin Immunol. 123: 1069. 200920
L Prieto Alergonorte, Mayo-2009

DETERIORO FUNCIONAL EN ASMA
OBESIDAD COMO FACTOR DE RIESGO
Marcon A, et al. J Allergy Clin Immunol. 123: 1069. 2009
BMI at baselineNo obstruction at baseline
Men and women with an intermediate BMI had the greatest FEV1 decline
21
L Prieto Alergonorte, Mayo-2009

DETERIORO FUNCIONAL EN ASMA
OBESIDAD COMO FACTOR DE RIESGO
No obstruction at baseline
P <0.001 P <0.001
FEV1 decline in men: 61.8 ml/y greater for every BMI unit (1 Kg/m2) gained
FEV1 decline in women: 20.2 “ “ “ “ “ “
Marcon A, et al. J Allergy Clin Immunol. 123: 1069. 200922
L Prieto Alergonorte, Mayo-2009

23
L Prieto Alergonorte, Mayo-2009
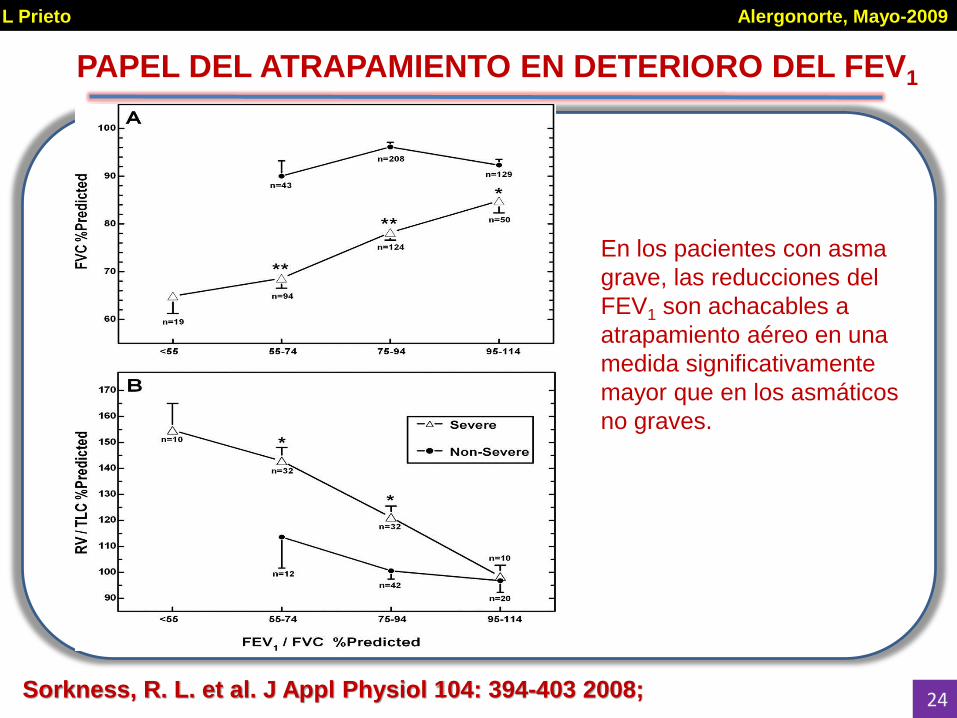
Sorkness, R. L. et al. J Appl Physiol 104: 394-403 2008;
PAPEL DEL ATRAPAMIENTO EN DETERIORO DEL FEV1
En los pacientes con asma
grave, las reducciones del
FEV1 son achacables a
atrapamiento aéreo en una
medida significativamente
mayor que en los asmáticos
no graves.
2424
L Prieto Alergonorte, Mayo-2009

AIRWAY CLOSURECONTRIBUTING MECHANISMS
Healthy
Asthma
25
L Prieto Alergonorte, Mayo-2009

Boulet, L.-P. et al. Chest 2006;129:661-668
ASTHMATIC SUBJECTSATENUATION AREAS
Healthy
nonsmoker
Asthmatic
nonsmoker
26
L Prieto Alergonorte, Mayo-2009

CT-derived three-dimension display of the lungs, airways, and regions of air trapping
Busacker A. et.al. Chest 2009;135:48-56 27
L Prieto Alergonorte, Mayo-2009

FENOTIPOS DE RESPUESTA OBSTRUCTIVA
0
25
50
75
100
125
TL
C (
% t
eó
rico
)
RV
ERV
VT
IRV
VC
RV
ERV
VT
IRV
VC
FRC
FRC
NORMAL OBS + ATRAP
RV
ERV
VT
IRV
VC
FRC
OBSTRUCCION
28
L Prieto Alergonorte, Mayo-2009

IDENTIFICACION DE ATRAPAMIENTO
PENDIENTE E INTERCEPCION
Corsico A, et al. Eur Respir J. 2000; 15: 687.29
L Prieto Alergonorte, Mayo-2009

0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
1,8
Methacholine AMP
Slo
pe F
VC
P = 0.57
ATRAPAMIENTO AEREO
METACOLINA vs AMP
Prieto L, et al. Ann Allergy Asthma Immunol. 102: 239. 2009.30
L Prieto Alergonorte, Mayo-2009

ATRAPAMIENTO AEREO: METACOLINA vs AMP
P = 0.03
a)
Moderate
asthma
Mild
asthma
0.00.20.40.60.81.01.21.41.61.82.0
Meth
acholin
e s
FV
C
b)P = 0.29
0.00.20.40.60.81.01.21.41.61.82.0
AM
P s
FV
C
Moderate
asthmaMild
asthma
31Prieto L, et al. Ann Allergy Asthma Immunol. 102: 239. 2009.
L Prieto Alergonorte, Mayo-2009