
Ark Magazine: Vol 3
12
The Voice of Healthcare ARK VOL.3 POWERED BY In this issue TAKING OVER THE WORLD HAVE RUCKSACK, WILL TRAVEL! YOU ARE NOT ALONE... THE DEVIL’S IN THE DOSAGE A THOUSAND DAYS OF LIFE NUTRITION, A BALANCING ACT Caring for people is at the heart of everything we do
-
Upload
cme-medical -
Category
Documents
-
view
219 -
download
0
description
In this issue: + TAKING OVER THE WORLD + HAVE RUCKSACK, WILL TRAVEL! + YOU ARE NOT ALONE... + THE DEVIL’S IN THE DOSAGE + A THOUSAND DAYS OF LIFE + NUTRITION, A BALANCING ACT
Transcript of Ark Magazine: Vol 3
The Voice of Healthcare
ARK VOL.3
POWERED BY
In this issueTAKING OVER THE WORLD
HAVE RUCKSACK, WILL TRAVEL!
YOU ARE NOT ALONE...
THE DEVIL’S IN THE DOSAGE
A THOUSAND DAYS OF LIFE
NUTRITION, A BALANCING ACT
Caring for people is at the heart ofeverything we do

It’s so easy to take our every day lives forgranted. In the 1940’s, Americanpsychologist, Abraham Maslowdeveloped a theory which became knownas Maslow’s ‘hierarchy of needs’.
As the theory denotes, humanphysiological needs (air, water and food)are the fundamental requirement forhuman survival. However, for somepeople, nutrition is a complex issue thatcan easily disrupt their very existence. Asyou’ll read in the pages that follow,Carolyn Wheatley (Chair of PINNT)describes her recent trip to the States andhow it had to be strategically plannedwith the precision of a military operation.
Also as part of this issue, I had a veryenlightening chat with the UK’s leadingexpert in nutrition, Professor Alan Jacksonwho talks about the significance of goodnutrition in infancy, as well as the role ofdiet in managing chronic illness.
I’m continually humbled by the manybrave people we encounter through ourwork, the clinicians who strive to offer thevery best care and attention, and thepatients who, no matter what pain ordiscomfort they might be in, remainpositive and keep fighting.
Nutrition has always been of particularinterest to me because it evokes suchwide-ranging emotions whilst playing akey role within a variety of social,economic, political, environmental andcultural issues. I’m a true believer in eachof us being able to make a difference,however small, and with that in mind if wehave the luxury of food choices, we shouldchoose wisely so as to positively impactour lives, our families and the planet.
Rachel McClelland, Editor.
2
TAKING OVER THE WORLD
Tracy Earley, nurse consultant for theIntegrated Nutrition and CommunicationTeams based in Preston, describes what ittakes to make a rapid access seven-day aweek clinic a success.
Tracy Earley sets her sights high. And whileworld domination might not be her actualgoal in life, you clearly get the messagethat she has the drive to change things forthe better.
When it comes to establishing a seven-daysa week service for patients reliant onartificial feeding, that kind of commitmenthas helped Tracy and her colleagues breakthe mould of ‘no weekend’ cover.
‘You have to want to take over the worldand have a bit of passion,’ says Tracy, apaediatric nurse by background who spenta decade or so in paediatric intensive careunits, spells in Leicester and Nottinghamand some US training, before heading toPreston in Lancashire.
‘If you are passionate about what you wantto do, then you can normally find a way ofgetting people on board with you.
‘Believe in what you are doing and why youare doing it.’
It was this mentality which helped Tracy, whowon the Nursing Times Nurse of the Yearaward in 2011, and her team to convince thepowers-that-be at the Royal Preston Hospitalthat extending clinic access made goodclinical and financial sense.
She says: ‘Aim high and listen to yourpatients.
‘You cannot deliver a service based on whatlooks right on paper because it will never fityour patients’ needs, or the organisation.
‘When you know what patients need, usetheir stories to go and speak to your execteams to change the world, because that iswhat we have done.’
One story in particular stands out.
It was a patient who had a PEG(percutaneous endoscopic gastrostomy)tube fitted which fell out over the weekend.
He went to A&E at another hospital butstaff there were unable to help and theweekday clinic was obviously closed.
‘So the patient called me at home,’ says Tracy.
‘I came in and we sorted his tube out over the weekend. If we hadn’t done this,he would have been in hospital for a fewdays until we managed to get himtransferred over.
‘By then the gastrostomy site would havehealed over and he would have had to gothrough the whole process again.
‘I took this story to our managementexecutives when we were looking atopening seven days a week.
‘It meant they could see the problem fromthe patient’s perspective.
Passion, belief... and a desireto take over the world.
If you’d like to share your story, [email protected]
By Pat Hagan
If you are passionateabout what you wantto do, then you cannormally find a way ofgetting people onboard with you
‘There was an increased chance of illnessbecause patients were not getting theirfeed or medicines.
‘And they could see there was a significantimpact on the NHS, including a stay inhospital and an expensive procedure that ispreformed when it doesn’t necessarily needto be.
‘It was these kinds of stories that reallyhelped make the change.’
So what exactly is the Integrated Nutritionand Communication Team and how does itwork?
It’s made up of nutrition nurses, speech andlanguage therapists, dieticians and acentral venous access team.
They work together with the patients,avoiding where possible artificial feeding.
But when patients do need to be artificiallyfed, the team ensures they get the bestdevice and the best fit for them andprovides a port of call for when things gowrong.
Seven days a week provision meanspatients can be seen by an expert group ofnurses who can help replace their feedingdevice, without having to be admitted intohospital.
But there are still challenges.
‘My idea of quickly doesn’t necessarilymatch other people’s ideas,’ Tracy says.
‘If you have a patient whose feeding devicehas fallen out, this is time critical.
‘So getting them into clinic quickly isimportant and can also be a challenge.
‘This is something we are working on andthe increase from a five day clinic to aseven day clinic has helped.’
Difficulties can also arise checking theposition of a device to make sure that thepatient is safely feeding and safelyreceiving their medicines.
‘Nasogastric tubes pose a particularproblem when it comes to testing of theposition by withdrawing gastric aspirate upthe tube’, says Tracy.
But plans are afoot to improve things.
‘We are working on a technology withNGPod Global Ltd that will revolutionisethe way we look after patients withnasogastric tubes,’ says Tracy.
‘It’s really exciting. It will provide a quickand reliable response on whether it is safefor patients to feed or not, which is betterfor them and will keep them in betterhealth.’
But restricted opening is not the only thingthat needs to change, she believes.
Another area that needs tackling urgently isthe divide between hospital andcommunity services.
Tracy says: ‘At the moment these operateseparately.
‘I would like to see them integrate better,as it will provide a more seamless transitionfor patients
‘Once a patient is discharged from us, theyare looked after in the community by adifferent set of nurses and dieticians.
‘I want the same staff to work in and out ofhospital, so the patients don’t have anykind of difference in the approach.’
This is a crucial issue, she believes, becausepatients can become very expert at theirown care very quickly.
So they are inclined to notice the differenceif anyone does things ever so slightlydifferently. ‘So I want our nurses to be ableto go in and out of the community andhospital to ease the passage for patients.
‘It would give them confidence in theircare, no matter where they are having thatcare delivered.’
This issue of patient choice is clearly onethat is high on Tracy’s agenda. And thereason is simple. A happy, well-cared forpatient is less likely to end up in hospital.
She adds: ‘We have to ensure that what weare doing is right for them.
‘We try really hard to work within theirlifestyles.
‘It’s important to put the right device infor the patient because if you get it rightthey are happy and will stay out of hospitala lot longer.
‘We try to have good relationships with our patients in order to get the best fit for them.’
I felt so organised - yet so unprepared - formy journey to New York.
Organised in terms of meticulous planning;flight, connecting flight, hotels, medicalsupplies (fluids and ancillaries),communicating with my homecare companyand nutrition team, medical letters, excessbaggage arrangements - the list was endless.
But unprepared in terms of packing personalluggage. Come on, a girl needs good co-ordination and a selection of shoes. You haveto be prepared for all eventualities!
Why New York? Well, I was fortunate to beattending a patient conference in SaratogaSprings, New York state. I am not a first timeattendee. This is actually my third trip to the‘Big Apple’ and I am in fact a seasonedconference traveller in the USA. It’s where Isaw my first ambulatory parenteral infusionpump many years ago. I had ‘pump envy’, orshould I say ‘freedom and lifestyle choiceenvy’.
It’s a long story but thanks to visiting thissame conference many years ago I, alongwith a dear friend Dawn, returned to the UKand started to campaign for freedom andlifestyle choices by encouraging theintroduction of ambulatory pumps into theUK.
But as I settled into my seat prior to take offthe usual discussion took place with theairhostess about not being able to keep myrucksack with me during take-off. Afterexplaining that I was connected to it (on long
flights I always keep hydrated by infusingsaline) she agreed it was okay to keep it withme. Presumably because she realised Icouldn’t be safely stowed in the overheadlocker along with the rucksack! Of course, Ihad made pre-flight arrangements. But asmany people in my position will know, thesearen’t always filtered down to the crew.
I’m fed via a central venous catheter everynight with a three litre bag of parenteralnutrition. I may be gutless and in need ofartificial nutrition but I do try and make themost of the investment so many people havemade in me in terms of giving me back my life.
That said, taking your own ‘food’ on holidayisn’t everyone’s idea of fun. But for me it’sessential. I’m not a fussy eater, simply unableto eat sufficient to sustain my life. I’m notcomplaining – no menus to drool over, nocalorie counting; that’s been done for me, atwelve hour infusion of parenteral nutritionevery night keeps me going. The menu, ifyou like, is pre-set.
It’s a bit of a nuisance at times and I have toadmit it would be so easy to skip a night. Yetthe consequences wouldn’t upset anyonebut me. Why would I risk making myself ill forthe sake of a ten minute set up process?Home parenteral nutrition equals life for meand that’s motivation enough on those nightswhen I could easily cut corners.
The first part of my trip this time was to asmall town outside New York to representPINNT at a conference. And if I’m honest, Iwas feeling rather proud. Travelling with HPN
for eight days is no mean feat. Lots of excessbaggage and lots of bag counting to ensureall are present and correct, especially whencatching a connecting flight. It’s anything butrelaxing. There are lots of ‘what ifs’, the mainone being what if something gets lost orbroken in transit. That’s why it’s so importantto have a ‘what if’ list and be prepared forproblems. There are factors you can controlbut there are many that are alsounforeseeable. The crucial thing is to have aback-up plan for how the disappearance ofthis very special baggage could be resolvedin a timely and appropriate fashion. Oh anddid I mention I was travelling with acolleague who has enteral tube feeding? Soin essence it was potentially double trouble ifsomething went wrong.
We finally arrived at the conference hoteland with little rest it was straight into theconference the next day. First on the list wasa workshop by the Oley FoundationAmbassadors, a USA organisation thatrepresents those needing home intravenousand tube feeding. As the UK Ambassadorit’s a great opportunity to be updated withOley business, then brainstorm with fellowambassadors on how to fulfil our roles. As Iam based in the UK my role is different butit’s wonderful when I can help someonewhen they worry about travelling to the UK.There are always laughs along the way as weall network to support patients.
The next two days were a mixture of plenarysessions and workshops. Again, great to findout what’s new, different or how to showcaseUK processes and procedures. Mingling with
4
HAVE RUCKSACK,WILL TRAVEL!Carolyn Wheatley, from the charity PINNT(supporting people at home on parenteraland enteral nutrition), charts the ups anddowns of long-haul travel when youdepend on home artificial feeding.
By Carolyn Wheatley

fellow home artificial nutrition people alwaysraises the question of travel, given thatwe’ve come all the way from the UK. Wemet a friend there from Czech Republic whohad travelled with her parenteral nutritiontoo so we were all quizzed as to how we didit. It’s always a healthy debate and highlightsthe differences in cold chain transportation,multi-chamber bags and stability data forpackaging, along with appropriate storagewhen in a hotel or holiday accommodation.
I should be able to accept the problems weface when storing supplies on the move. ButI can’t. Most of the HPN patients I meet arehappy to use ice from the ice machines atthe hotel to keep their PN cold. I still can’tget my head round that because, here in theUK, we are taught very differently.
After a fabulously interactive educationalconference we had time to stop off in NewYork City itself. Leaving the tranquilsurroundings of Saratoga Springs andarriving in Times Square was part two of oureducational trip. Similar routine; lots ofbaggage which was slightly depleted due tousage but still more than your averagetraveller, sorting out fridges and working outhow much and when to fit in essential feeds!
But there was no time to worry as we set outinto the evening to absorb the electrifyingatmosphere. Bright lights and crowdedpavements. Enticing restaurants and bars atevery turn, not so attractive when you arelimited to what you can take in orally. Still,absorbing the atmosphere was goodenough for us. Being in town on 4th Julywas also a great buzz with a splendidfirework display.
Leaving aside all the excitement there is aserious side to travelling with artificialnutrition. I’ve often wondered whether,when a traveller dependent on artificialfeeding asks for medical consent to travel,does the person in charge understands theconsequence of their response? I firmlybelieve anyone electing to travel withartificial nutrition needs to assumeresponsibility for their decision.
For all those asking ‘Can I go on holiday?’ itmight be better to start with where andwhen? It’s not just about being fit to fly. It’s
also about being responsible for thepreparation and planning.
PINNT often receive calls from people whosay they didn’t appreciate all that wasinvolved in travelling. I advocate choice;choice in being able to make decisionsabout your own life, or that of your child’s.But it needs to be an informed decision.PINNT produce Holiday Guidelines andTalking Points Information sheets thatcertainly aid the process of travel.
Reflecting on my trip to New York, I amalways grateful that I managed to enjoyanother wonderful experience. I’m not sureabout you but while away I always say‘where next?’
Well, for me, where next is Australia.
That will be another great adventure, so themeticulous planning has already started. Theairline isn’t being as accommodating as I’dlike in terms of excess baggage and that’san obstacle to overcome. And as this tripinvolves a wider team of people on bothsides of the world, communication is key.
But as long as I have the ability to travel andI can obtain appropriate travel insurance Iwill keep asking that question - ‘wherenext?’
For those asking‘Can I go on
holiday?’ it mightbe better to startwith where and
when?

YOU ARE NOT ALONE…
6
By Rosemary Martin
If you’d like to share your story, email [email protected]
43 years ago I became ill. My symptomswere sickness, diarrhoea, cramps, achingjoints, dry skin, hair loss and always feelingcold. I was anaemic, generally depressedand could not lead a ‘normal’ life. The fearof having a personal accident meant thatsocial activities and holidays were out ofthe question, so I soon became a prisonerin my own home. I was put on variousdrugs and treated for Irritable BowelSyndrome (IBS). Eventually after a secondopinion at a different hospital, Crohn’sdisease was diagnosed. There followedfrequent admissions to hospital fornutritional disturbances requiring Ironinfusions, until it was decided I would havean irreversible ileostomy.
After this, things looked up for a while.Then the Crohn’s flared up again. At myrequest, I was transferred to HopeHospital, now known as Salford Royal, tobe treated by an eminent surgeon in aspecial unit called the Intestinal FailureUnit. A laparoscopy was performed firstand an abscess drained. At only 5 stone, Iwas put on HPN to build me up for furthersurgery. Following surgery, I was left withonly 20 inches of small bowel - which wasnot enough to sustain me and that is why Iwas put on HPN. I’ve been on it for 7nights a week for over 33 years now. I knowthat without the treatment and the carefrom the doctors and nurses on the unit, Iwould not be here.
I have tried to lead as near ‘normal’ life as Ican. I have been determined to rule myown life and not let the condition ortreatment rule it. My family and I havebeen on many holidays both in the UK andabroad. I have continued to visit the gym,swim, cycle, walk, do my gardening andhelp to bring up two grandchildren. Mostimportantly I also returned to work.
Over the years I have been only too willingto help other patients by talking to them.They have had various worries, the mostfrequent ones are understandable. Theyworry about what they are putting thefamily through; they find many activities areno longer appealing to them, so the familydon’t continue to enjoy them either. As apatient, you need family and friends themost to support you emotionally,particularly to help with the transition fromhospital life to home life again. After a longstay in hospital, people can becomeinstitutionalised because the safety thatthey felt from the doctors and nurses issuddenly taken away. They can feel isolatedand alone and many patients want to knowwhat is ahead of them, some don’t. Somewant to take one day at a time and takewhat comes. Others want to try and plantheir future.
Young people worry about formingrelationships, dating and being able tohave a family. Are they going to be ableto cope with looking after a family,especially if they become ill and have tobe admitted to hospital? Are they evergoing to meet a partner? Might theygrow old on their own? They fearfriendships will collapse becausesometimes they can’t or don’t want togo out to dinner or partake in certainsocial activities. If they do have a family,are they going to pass on any illnesses,are they hereditary?
My advice is, remember that you are notalone with your problems and you need totalk and share them. One way is to joinPINNT, a support group for Patients onIntravenous and Nasogastric NutritionalTherapy. This group was formed over 25years ago and a magazine is sent to youthree to four times a year, where you will
find similar problems to your own and howthey are dealt with. In addition, there aresome really interesting articles and currentresearch in there too.
There is no blueprint for coping with life atthe best of times, even with good healthon your side. But you need people tounderstand that you are still reliable,responsible, hardworking, caringindividuals and that you are capable ofgiving and receiving love.
My name is Rosemary Martin. I am 70 years old and have been onHome Parenteral Nutrition (HPN) for over 33 years.
Tweet us yourthoughts@arkmagazine
IT’S ALL ABOUT THE GUT…
To what extent do you think nutrition hasan impact on disease prevention?Hugely - we work with people all over theworld who have had issues with thyroidhealth, diabetes, IBD etc. It’s amazing reallyto look at disease in fine detail as it canalways be linked back to a deficiency.Recently I have been looking into the gutand microbiology’s effect on human health,and there is a pretty strong correlationbetween problems with the gut and disease.
To what degree do you think food affectsmental health?Ok so this is a fun one… Nutrition has a largeimpact on our emotional, hormonal, mentalstates, the way we feel and I guess you cansay the way we view ourselves. It’s amazingto hear about people who start to eat rightthat the first things they feel is mental clarityand improved energy.
With deeper mental issues, I believe it’svery important to look further down therabbit hole. There is a huge correlationbetween the gut and mental health.
What are you views on current trends likegluten free foods? Gluten free produce certainly has a placefor people with certain intolerances.However, given the current trend for glutenfree products, e.g. gluten free cakes andgluten free brownies it’s important toremember that they’re not necessarilyhealthy.
What do you think the greatestchallenges are for global nutrition?In my opinion the biggest challenge is inthe education of nutrition. Speaking topeople around the world, you realise thatthey don’t know what the right foods are,what it is that they should be eating andthe impact of a bad diet. If we were able to
address the issue from a younger age, wecould have a really positive impactthroughout the world.
What advice do you give to people whenworking with them on their diet?Humans are habitual, so you have to look attheir current habits and start rebuilding. Ifyou approach things habitually with say adifferent focus each week, such as; gettingyour optimal water intake, changing yourbreakfast, eating more vegetables – thenslowly but steadily you can start building ahealthier lifestyle.
What does the average person needwhen it comes to diet? It’s all about balance and eatingnutritionally dense foods, but you have tobe able to go out and enjoy yourself andnot become a social recluse!
There has been a lot in thepress recently about sugaryfoods, what’s your take? We are always looking forsomething to blame. A goodtip with anything is toremember that the devil is inthe dosage; we can demonisefat, we can demonise sugar.It’s when we eat too muchthat the issues occur.
Is there actually anynutritional value in fast food? Fast food pretty much has allthe nourishment, enzymes etc.taken out of it and it gets filledwith preservatives. Have youever seen the pictures on theinternet of the fast foodburgers that have been left onpeople desks for years and theystill look the same two years onfrom the day they were bought?
Is it worth buying organic food? It’s all about preference and financially whatcan be afforded. Organic food is definitelyworth considering. There is a great articlecalled the ‘Dirty Dozen’ about the 12 foodsthat are most treated with pesticides.Organic food arguably has more nutrients,it’s grown in better soil, it’s looked after andyou are not consuming as many chemicals.
Can the amount of fluoride in tap waterbe dangerous and in an ideal world wouldyou advocate bottled water? Bottled water does tend to have a muchhigher mineral count in it so I would alwaysbuy decent bottled water for that reason. Fluoride is in the water yes and has beenshown to have issues, with this again Iguess it falls back to “the devil is in thedosage.”
THE DEVIL’S IN THE DOSAGENutrition expert and personal training consultant, Simon Hall, has ten years’experience in the health and fitness sector, specialising in health and bodytransformation via a unique multi-disciplinary approach. Prior to setting up globalconsultancy, Body Composition, Simon travelled the world researching andworking with some of the most influential leaders in the industry. By Rachel McClelland
8
SOMEONE who survives to the age of 80notches up almost 30,000 days of lifespan.So you might think that leaves plenty oftime for the body to make up for anynutritional deficiencies it might endure inthe early stages of life.
But there is now a consensus that the first1,000 days of life – from conception to theage of two - are critical when it comes tolaying the foundations for a healthy life.Professor Jackson, whose early careerfocused on tackling malnutrition in children,says science can now show that if the humanbody does not get off to a good start, it maynever make up the difference.
‘If you grow well in childhood, your ability tocope with challenging environments is likelyto be greater,’ he says.
‘But if you grow poorly in childhood, thenyou’re more likely to be vulnerable.
‘That is why currently within the UnitedNations global system, there is this emphasison the first 1,000 days of life - from the timethat you are conceived to how you grow as ababy in the mother, how you grow as aninfant and how you grow as a child,particularly up to 2 years of age.
‘If there is a solid foundation of good growthand good health laid down in those first1,000 days, then you are well set up for therest of life.
‘If that is not set down well, then you are asit were ‘always trying to catch up’.’
Most of us, he concedes, have to do somecatching up at some point.
But for some the challenges are greater andthis makes them more vulnerable to illnessand disease when it comes along.
‘Quite clearly, growing during childhood istaking in food and depositing it as your ownbody tissue.
‘The body has needs and those needs are inpart determined by the genes that you have.
‘So the better able you can meet the needsof your body at whatever stage or time ofdevelopment you are at, then the greateryour ability to grow well and be moreresilient.’
The question is then, to what extent arenutritional ‘shortfalls’ involved in the wholedisease process? And how important isgood diet in terms of preventing illness?
For the past decade, Professor Jackson hasbeen working with the World CancerResearch Fund.
It has focused on exploring the complexrelationship between diet and cancer,highlighting the potential links betweenpoor nutrition and several types of tumour.
‘The World Cancer Research Fund hasinvested a very considerable sum of moneyand carried out the largest systematicreviews in any part of medical literature,’says Professor Jackson.
‘It’s quite clear that something of the orderof at least 25 to 30 per cent of cancers arecaused by nutritional considerations.
‘As smoking declines diet, nutrition andphysical activity will come to be thedominant determinants of cancer risk.’
So if diet can prevent, or at least reduce therisk of some potentially fatal illnesses, can it‘cure’ them once they have set in?
‘It’s a challenging question,’ he admits.
‘We don’t know the answer.
‘My suspicion is that it might well do butthat is probably the more important agendagoing forward.’
He points to what he calls ‘forever’conditions – chronic and incurable illnesses –that don’t go away but do respond well togood diet.
Cystic fibrosis is one, phenylketonuria isanother.
‘Children born with cystic fibrosis doextremely well and a part of that is ensuringthat their nutritional health is maintained.
‘So, it doesn’t cure disease in the sense ofcuring an infection or cutting out a tumour,but it cures the disease in terms of theprocess expressing itself as an inability tofunction well or normally.’
Knowing the effects of good diet is onething. Putting it into practice is proving to bean altogether bigger challenge.
Professor Jackson believes the real hurdle isgetting everyone – from food manufacturersto consumers – to commit to radical change.And one of the biggest battlegrounds oflate has been sugar.
It has emerged as public enemy number onein the healthy diet debate.
But how big a problem is it really?
Professor Jackson says: ‘When you aretalking about sugar, you are talking aboutsucrose.
‘Biologically, sugars are an integral part ofour metabolic machinery.
A THOUSAND DAYS OF LIFEScientists have identified the most crucial period ofhuman nutrition – and it’s the first one thousand daysof life. Professor Alan Jackson, professor of humannutrition within medicine at Southampton University,talks about the significance of early feeding, the roleof diet in managing chronic illness and the threatfrom public enemy No.1 when it comes to healthyeating – sugar.
By Pat Hagan
‘For example our gastrointestinal tract andrespiratory tract are protected because ofthe production of mucins.
‘Most people would call that mucus but it ismade up of mucins that form a physicalbarrier that keeps us healthy. Mucins aresugar related compounds.’
But dietary sugars are a completely differentmatter.
‘The clearest example is sweetenedcarbonated drinks which contain very largeamounts of sugar for their volume and verylittle in the way of nutrients.
‘Some young people consume very largequantities of sweetened drinks and thereforeconsume very large amounts of sugar andthat is not good for them at all.
‘Then you have a variety of foodstuffs whichcontain rather a lot of sugar and by andlarge too much sugar limits the quality ofyour diet.’
Tackling the sugar crisis is not impossible, hebelieves.
A good example of how it can be done iswith salt, sugar’s predecessor as most-hatedfood ingredient.
Salt levels in processed foods have graduallybeen reduced because public health bodiesworked closely with food manufacturers,rather than fight against them.
‘It was known that you could progressivelyreduce the amount in food gradually and thepopulation wouldn’t know. In time theywould end up consuming less salt.
‘That is exactly what has happened. Theconsumption of salt now is significantly lessthan it was 15 years ago without anybodynoticing.
‘The food industry has to a considerabledegree honoured their reasonability and theUK is amongst the best in the world in termsof having achieved its salt reduction.
‘It required considerable planning and effortin the set up to get agreement across theboard – but difficult things take a long time.’
With a background in artificial feeding,Professor Jackson is just as interested in howproper nutrition can benefit those withgastrointestinal disease.
He is passionate about the need to invest intraining for structured nutrition programmesand says it can lead to considerable savingsin reduced hospital stays.
But how and when is parenteral nutritionappropriate?
‘Well, if you take out someone’sgastrointestinal tract, then they haveintestinal failure.
‘That is absolute and they will needparenteral nutrition unless someonetransplants their gastrointestinal tract.
‘So parental nutrition is used in my book forintestinal failure, which may be acute, it maybe chronic, it may be total, it may be partial,it may be reversible or it may be irreversible.
‘Therefore how likely you are to come off itis determined by which of those factors areat play.
‘The most common form of intestinal failureis perioperatively, which is self-limiting and ashort period of support gets people intotheir usual form of eating.
‘But if someone takes out your tract you willbe on it for life unless you are transplanted.
‘Those are the extremes. The challenge forclinicians is to help you make progress and itis impressive how, with decent parenteralsupport, patients who previously would havenever been considered capable of comingoff nutrition, have.
‘I have seen patients with very substantialintestinal resections that didn’t look like theywould ever come of parenteral nutritionbeing able to because the gut has adaptedto cope better than it did previously.
‘These people aren’t cured. But their bodieshave responded to the insult andaccommodated to do the best they can.’
CAREER AT A GLANCE‘I’m basically a clinician and a paediatrician.
‘I have spent my time looking at evidencefor improved nutritional care and support ofpatients. Originally that was in children withsevere malnutrition in the Caribbean and,since I came to Southampton in 1985, interms of nutritional support of patients.
‘I worked very closely with Professor DavidBarker, understanding the nutritionaldeterminants of the early origins of adultchronic disease.
‘Along the way I’ve done some molecular,cellular level work, clinical studies andpopulation studies.
‘And for the past 10 years I have beeninvolved with the World Cancer ResearchFund looking at the evidence in and aroundnutrition, physical activity and cancer.’
10
Nutrition is not a word that makes mefeel warm and happy. Eating, I love. Foodand restaurants and lunch with the familyand suppers with my husband I love.Cooking, even. But nutrition alwaysmakes me think of a friend of mine whocan tell you the calorific value of sixbeansprouts and the fat content of threefluid ounces of semi-skimmed milk.
My friend sees food as fuel - which ofcourse, at one level, it is. She exercisesfuriously and eats a fiercely controlled dietto maintain an ideal weight. All of which isvery splendid. And quite boring.
I can see that it’s important to understandthe chemical components of food. If I weresick or had a hormone imbalance I wouldwant to know as much as possible abouthow to eat to feel better. I recently had tosee a gastroenterologist, who told me thata majority of the population has some sortof wheat intolerance, which isunquestionably interesting and usefulinformation.
Yet, while I want this knowledge, I alsowant to be able to retire it to the back ofmy brain, because the one thing I do notwant to be about food is joyless. For myexercise and diet-conscious friend, salt andfat are enemies to be seen off. She can bevery sanctimonious about anyone who eats,say, cream teas, or heavily seasons theirpasta water.
She is not a nutritionist. I’m not either, but Ido know that the general thinking is thatnot all fat is bad for us (and that opinionshave changed about this in recent years). Ialso know that a diet high in salt is bad forpeople with high blood pressure, but that astudy published in the New England
Journal of Medicine, monitoring more than100,000 people in 18 countries, found thata low sodium diet isn’t good either.
We lay people have to be careful with ourpartial knowledge, which rarely takes intoaccount the person eating or theircircumstances. Not that science is reallywhat my friend’s approach to food is reallyabout. Like a lot of dieters, she imbuescertain foods with moral values: lettucegood, butter bad. And once you do that,it’s easy to get things out of proportion. It’sjust food, I quite often want to shout. It’snot the devil. It’s not out to get you andyou are not, despite what you say, ‘beinggood’ if you don’t eat cake.
People who see food as either polluting orimproving can very quickly acquire an air ofsuperiority. If you are striving to be a betterperson through your food intake, you canquickly become judgmental about whatother people eat. When you are on apunishing regime, it’s hard to be relaxedabout other people with their fish andchips. They may believe they’re gettingaway with it, the dieter thinks – andsurprisingly often, says - but they are goingto suffer in the long run.
Nutrition is a serious subject. For somepeople, it is a matter of life and death.But it is perhaps best left tonutritionists. Modern nutritionalscience emerged with theisolation and identification ofcertain nutrients in food anddiscovery of their effects onthe incidence of certaindiseases. But therelationships can bemore complicated thanthey first appear.
Several studies show, for example, thateating large amounts of fruit andvegetables tends to protect against heartdisease and certain cancers. But the resultsaren’t replicated if people takesupplements containing those nutrients.Similarly, the famed superiority of theMediterranean diet doesn’t seem to beabout the foods that make up the diet somuch as their overall quality and balance.
In the developed world, food is plentiful, asituation for which we are almost certainlynot evolved. Our genetically-programmedgreed undoubtedly requires somedisciplining. So we do have to think aboutwhat we eat.
But we are also lucky to have access to richcultures of good eating, developed overcenturies, tried, tested, and honed to makepeople healthy and happy. Food is almostcertainly best for us when it is cooked withcare, shared with love, and eaten withpeople who cheer us up. So perhaps wealso need not to think too much. Myfavourite nutritional guidelines come fromthe American author Michael Pollan. Theyrequire no weighing or counting: ‘Eat food.Not too much. Mostly vegetables.’
NUTRITION, A BALANCING ACT
By Geraldine Bedell
Whether you are on parental nutrition or you’re just into nutritionalhealth and wellbeing, it’s all about making the right choices…
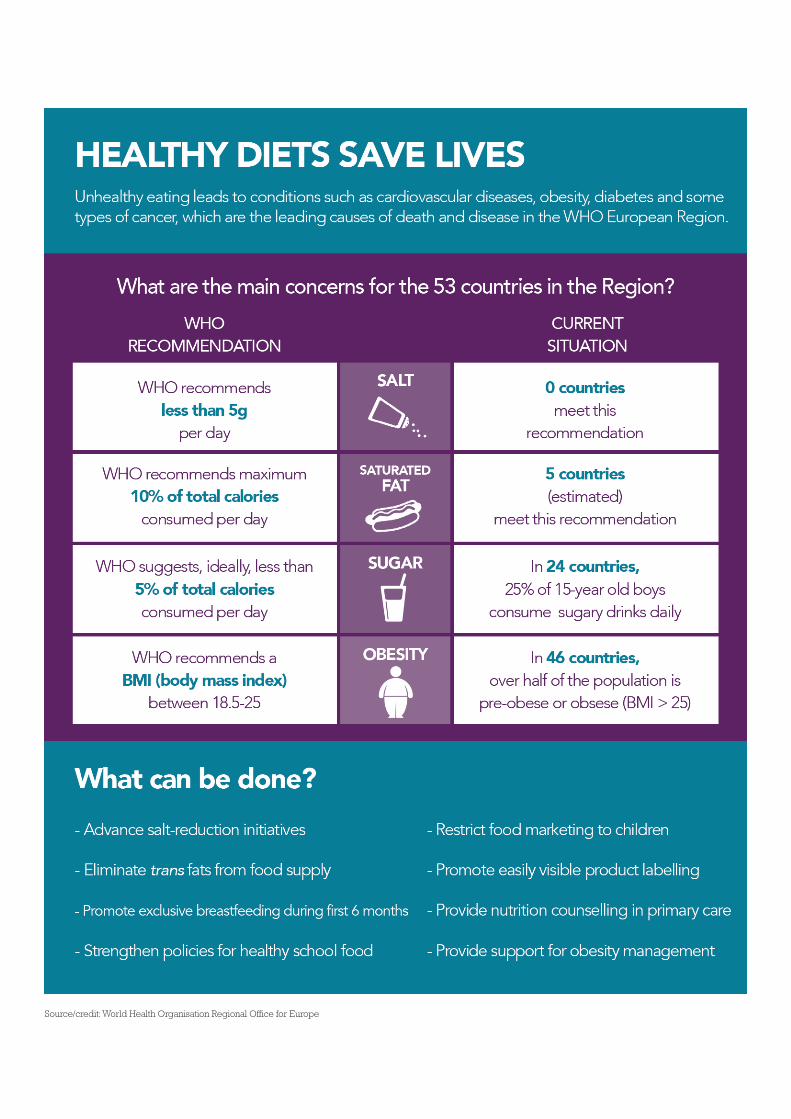
Source/credit: World Health Organisation Regional Office for Europe
POWERED BY
The Voice of Healthcare
Our next issue of Ark will focus on Integrated Care. If you would like to contribute pleaseemail Rachel at [email protected]
If you would like to request hard copies or if you would like to receive future issues of Ark please email [email protected]














![Ark Vol. 21 [GoKoTo Project].pdf](https://static.fdocuments.net/doc/165x107/5695d49a1a28ab9b02a21123/ark-vol-21-gokoto-projectpdf.jpg)