
Applying Scientific Measurement of Disease Activity …...CME) is an approved provider of continuing...
12
The Coalition for Rheumatology Educators (CORE) ® is a multi-faceted initiative developed to provide education on rheumatic diseases for rheumatologists and allied healthcare professionals. This includes evidence-based information on safe and effective use of disease-modifying drug therapy with the goal being to reach low disease activity or remission, and ultimately improving patient function and quality of life. Co-sponsored by Albert Einstein College of Medicine and North American Center for Continuing Medical Education, LLC © 2011. North American Center for Continuing Medical Education, LLC Applying Scientific Measurement of Disease Activity in Clinical Rheumatology Based on a program chaired by Max I. Hamburger, MD, FACP, FACR T he Coalition of Rheumatology Educators (CORE) ® Routine Assessment in Practice Seminar Series (RAPSS) live, hands-on workshops were designed to introduce and reinforce clinical measurement of rheumatic dis- ease patients into routine practice, by emphasizing the use of simple, quick, and effective patient questionnaires. The 2-day workshops were hosted by local rheumatology practices across the country, where faculty mentors met with the host practice and observed office procedures, presented programming on the rationale and strategies for the use of patient question- naires in usual clinical care, and completed hands-on instruc- tion on the implementation of the questionnaires. Fifteen clin- ical sites were identified and enrolled in RAPSS. This activity is based on the CORE CME/CNE/AANP- accredited program entitled, Routine Assessment in Practice Seminar Series. This monograph contributes to the blended learning of the overall initiative by providing a case-based review and integration of the key learnings captured during the individ- ual live workshops and complimentary sessions assisting partici- pants in integrating the Routine Assessment of Patient Index Data 5 (RAPID5) program into rheumatology routine care. The use of quantitative measures in rheumatology practice has been demonstrated to be superior to the more common gestalt approach of a general assessment and impression. 1 Clinical assessment of disease activity, which historically has included laboratory tests, has been plagued by frequent false- positive and false-negative results. Quantitative radiographic scoring is seldom performed outside research environments due to complexity and time requirements for calculations. In addition, data show that many clinicians underestimate patient pain severity and functional disability. 2,3 Therefore, it is critical to educate rheumatologists and their healthcare team on effec- tive clinical measurement strategies to prevent damage by Vol. 5, No. 1 CME Newsletter Series June 2011 Practice Case Study Demographics: This index practice is an example of one of the sites participating in the RAPSS educational program. The rheumatology practice consists of 4 rheumatolo- gists, each with a dedicat- ed nurse, and an addition- al 2 infusion nurses. The practice also employs 5 medical assistants, 3 x-ray technicians, 2 lab technicians, 6 front office staff, 1 office manager, 1 practice manager, 1 executive assis- tant, and a 4-person billing department. CLICK HERE TO TAKE POST-TEST ONLINE
Transcript of Applying Scientific Measurement of Disease Activity …...CME) is an approved provider of continuing...

The Coalition for Rheumatology Educators (CORE)® is a multi-faceted initiative developed to provide education onrheumatic diseases for rheumatologists and allied healthcare professionals. This includes evidence-based informationon safe and effective use of disease-modifying drug therapy with the goal being to reach low disease activity orremission, and ultimately improving patient function and quality of life.
Co-sponsored by Albert Einstein College of Medicine and North American Center for Continuing Medical Education, LLC
© 2
011.
Nor
th A
mer
ican
Cen
ter
for
Con
tinui
ng M
edic
al E
duca
tion,
LLC
Applying Scientific Measurement of Disease Activity in Clinical Rheumatology
Based on a program chaired by Max I. Hamburger, MD, FACP, FACR
The Coalition of Rheumatology Educators (CORE)®
Routine Assessment in Practice Seminar Series(RAPSS) live, hands-on workshops were designed to
introduce and reinforce clinical measurement of rheumatic dis-ease patients into routine practice, by emphasizing the use ofsimple, quick, and effective patient questionnaires. The 2-dayworkshops were hosted by local rheumatology practices acrossthe country, where faculty mentors met with the host practiceand observed office procedures, presented programming onthe rationale and strategies for the use of patient question-naires in usual clinical care, and completed hands-on instruc-tion on the implementation of the questionnaires. Fifteen clin-ical sites were identified and enrolled in RAPSS.
This activity is based on the CORE CME/CNE/AANP-accredited program entitled, Routine Assessment in PracticeSeminar Series. This monograph contributes to the blendedlearning of the overall initiative by providing a case-based reviewand integration of the key learnings captured during the individ-ual live workshops and complimentary sessions assisting partici-pants in integrating the Routine Assessment of Patient IndexData 5 (RAPID5) program into rheumatology routine care.
The use of quantitative measures in rheumatology practicehas been demonstrated to be superior to the more commongestalt approach of a general assessment and impression.1
Clinical assessment of disease activity, which historically has
included laboratory tests, has been plagued by frequent false-positive and false-negative results. Quantitative radiographicscoring is seldom performed outside research environmentsdue to complexity and time requirements for calculations. Inaddition, data show that many clinicians underestimate patientpain severity and functional disability.2,3 Therefore, it is criticalto educate rheumatologists and their healthcare team on effec-tive clinical measurement strategies to prevent damage by
Vol. 5, No. 1 CME Newsletter Series June 2011
Practice Case StudyDemographics:This index practice is anexample of one of the sitesparticipating in the RAPSSeducational program. Therheumatology practiceconsists of 4 rheumatolo-gists, each with a dedicat-ed nurse, and an addition-al 2 infusion nurses. Thepractice also employs 5 medical assistants, 3 x-raytechnicians, 2 lab technicians, 6 front office staff, 1office manager, 1 practice manager, 1 executive assis-tant, and a 4-person billing department.
CLICK HERE TO TAKE POST-TEST ONLINE

Release date: June 30, 2011Expiration date: June 30, 2012Estimated time to complete: 1 hour
Intended Learners
This activity is designed for physicians, nurses, and nurse practitioners whotreat patients with rheumatoid arthritis.
Learning Objectives
After completing this activity, participants should be able to:
• Self-assess practice behavior for determination of pain severity and function-al disability with evidence-based measures of pain severity and functional dis-ability
• Integrate the use of clinical measurement tools into daily clinical practice todiagnose RA and assess disease activity
• Utilize patient self-report tools for improved RA control
• Evaluate practice behavior of self-report tool utilization with evidence basedcriteria
There is no fee associated with this activity.This publication is available in print and online.Participants who have successfully completed the live version of this activity arenot eligible to receive credit for this enduring material.For questions regarding this activity, please call 609-371-1137.
CME Accreditation
Albert Einstein College of Medicine is accredited by the Accreditation Councilfor Continuing Medical Education to provide continuing medical educationfor physicians.Albert Einstein College of Medicine designates this enduring material for amaximum of 1 AMA PRA Category 1 Credit™. Physicians should claim only thecredit commensurate with the extent of their participation in the activity.
CNE Accreditation
North American Center for Continuing Medical Education, LLC (NAC-CME) is an approved provider of continuing nursing education by thePennsylvania State Nurses Association, an accredited approver by theAmerican Nurses Credentialing Center’s Commission on Accreditation.This continuing nursing education activity was approved for 1.0 contact hours.Provider approved by the California Board of Registered Nursing, Provider#13255 for 1.0 contact hours.
AANP Accreditation
This program is approved for 1.0 contact hour of continuing education by theAmerican Academy of Nurse Practitioners. Program ID 1106193.This program was planned in accordance with AANP CE Standards andPolicies and AANP Commercial Support Standards.
Medical writer Bonny McClain contributed to the writing and editing of themonograph article.
Planning Committee
The planning committee comprises Peter Barland, MD, Alan Brown, MD,Alan Epstein, MD, John A. Goldman, MD, Max I. Hamburger, MD, FACP,FACR, Arthur Mandelin, MD, PhD, Allan Morton, DO, Victoria Ruffing,RN, CCRP, and Michael Schweitz, MD; Steven Feld, Albert Einstein Collegeof Medicine; Stephen Chavez, Emilie McCardell, Bonny McClain, RandyRobbin, Alicia Rybovic, and John Savage, North American Center forContinuing Medical Education, LLC (NACCME).
Financial Disclosure and Conflicts of Interest
According to the disclosure policy of Albert Einstein College of Medicine andNACCME, faculty, editors, managers, and other individuals who are in a posi-tion to control content are required to disclose any relevant financial relation-
ships with relevant commercial companies related to this activity. All relevantconflicts of interest that are identified are reviewed for potential conflicts ofinterest. If a conflict is identified, it is the responsibility of Albert EinsteinCollege of Medicine and NACCME to initiate a mechanism to resolve theconflict(s). The existence of these interests or relationships is not viewed asimplying bias or decreasing the value of the presentation.All educational materials are reviewed for fair balance, scientific objectivity ofstudies reported, and levels of evidence.The faculty has reported the following:Dr. Barland has disclosed no relevant financial relationships with any com-mercial interests.Dr. Brown: Speakers Bureau: Abbott Laboratories, Takeda PharmaceuticalCo Ltd, UCB Inc, Genentech Inc.Dr. Epstein: Speakers Bureau: Abbott Laboratories, Bristol-Myers SquibbCo, Centocor Ortho Biotech Inc., Genentech Inc.Dr. Goldman: Speakers Bureau: Amgen Inc., Pfizer Inc., UCB Inc;Grant/Research: Atlanta Center Clinical ResearchDr. Hamburger: Grant/Research Support: Abbott Laboratories, Amgen Inc.,Bristol-Myers Squibb Co, Centocor Ortho Biotech Inc., Genentech Inc.,UCB Inc.; Speakers Bureau: Abbott Laboratories, Amgen Inc., Bristol-MyersSquibb Co, Genentech Inc., UCB Inc.Dr. Mandelin: Speaker’s Bureau: Abbott Laboratories, UCB PharmaDr. Morton: Speakers Bureau: Abbott Laboratories, Amgen Inc., Bristol-Myers Squibb Co, Genentech Inc., Pfizer Inc., sanofi-aventis, TakedaPharmaceutical Co Ltd, UCB Inc, URL Pharma, Warner Lambert;Consultant: Amgen Inc., Genentech Inc., Pfizer Inc., UCB Inc, URL PharmaMs. Ruffing has disclosed no relevant financial relationships with any com-mercial interests.Dr. Schweitz: Consultant: Genentech, Inc., Amgen Inc.; Speakers Bureau:Genentech, Inc., Amgen Inc., Novartis Corp.Mr. Stephen Chavez, Mr. Randy Robbin, Ms. Emilie McCardell, Ms. BonnyMcClain, and Mr. John Savage (NACCME Staff) have disclosed no relevantfinancial relationships with any commercial interest.Mr. Steven Feld (CCME Staff), or a member of his household own securitiesin-Bioheart, Inc., Chelsea Therapeutics, Inc. and Pharmacopeia, Inc.Ms. Rybovic (NACCME Staff): Stock Shareholder—Novo Nordisk, AmgenInc.Einstein and NACCME require faculty to inform participants wheneveroff-label/unapproved uses of drugs and/or devices are discussed in their presentations.The faculty has disclosed that no off-label/unapproved use(s) of drugs and/ordevices will be discussed.
Grant Support
Supported by educational grants from Abbott Laboratories, Centocor OrthoBiotech Inc, and Genentech, Inc.
Privacy Policy
Einstein and NACCME protect the privacy of personal and other informationregarding participants, educational partners, and joint sponsors. Einstein andNACCME and our joint sponsors will not release personally identifiable infor-mation to a third party without the individual’s consent, except such informa-tion as is required for reporting purposes to the appropriate reporting agency.Einstein and NACCME maintain physical, electronic, and procedural safe-guards that comply with federal regulations to guard your nonpublic personalinformation.
Hardware/Software Requirements
All educational activities are accessible via a computer with 650 MHz PC, 128MB RAM, Windows or Mac operating system, Internet Explorer, Netscape, orSafari browsers. Windows Media Player, sound card, and speakers are requiredfor streamed audio. Flash Player, sound card, and speakers are required forvideo programs. A PDF reader is required for print publications. Please directtechnical questions to [email protected].
To be eligible for documentation of credit, participants must read all monograph content, complete the 10-question onlinepost-test with a score of 70% or better, and complete the evaluation form. After successful completion of the post-test andevaluation form online at www.naccme.com, participants may immediately print their documentation of credit. Instructions for accessing documentation of credit are included on the back cover of this publication.
VOL. 5, NO. 12

3
encouraging early diagnosis, ongoing assessment of RA status,and tight disease control.4,5
The goals of optimal therapy for patients with RA includecomplete disease remission and prevention of disability. Historicclassifications of disease activity by practicing rheumatologistshave included a “gestalt”-like analysis that includes observationsof clinical status in the absence of standardized assessment toolssuch as those described in the published literature.1 Patientsymptoms, physical examination, laboratory tests, and imagingstudies are recognized as validated indices to report diseaseactivity in patients with RA. These measures are essential toevaluate progression to a treatment goal such as remission or lowdisease activity in patients with RA.6
The majority of disease activity measurements (DiseaseActivity Score [DAS], American College of Rheumatology[ACR Score]) are designed for use in clinical studies and maynot be practical and/or useful in the clinical setting.1,7-10 Patient-reported disease activity measures have demonstrated predic-tive value.11 Sokka et al determined that the Health AssessmentQuestionnaire (HAQ) predicts mortality in patients with RA (n= 1095) and community controls (n = 1490). Subjects with
Course ChairMax I. Hamburger, MD, FACP, FACR
Managing Partner, Rheumatology Associates of Long IslandPresident, New York State Rheumatology Society and the American Society of Clinical Rheumatologists
Assistant Professor of Clinical Medicine, SUNY Stony BrookMelville, New York
Advisory Board
Alan Brown, MDClinical Associate Professor of Medicine
Medical University of South CarolinaPrivate Practice
Charleston, South Carolina
Alan Epstein, MDClinical Associate Professor of Medicine
University of Pennsylvania School of MedicineAttending Physician and Rheumatologist
Pennsylvania HospitalPrivate Practice
Philadelphia, Pennsylvania
John A. Goldman, MDPrivate Practice
Chief of Rheumatology, St. Joseph’s HospitalPresident, Medical Quarters
Atlanta, Georgia
Arthur Mandelin, MD, PhDInstructor, Department of Medicine
Division of RheumatologyNorthwestern University Feinberg School of Medicine
Chicago, Illinois
Allan Morton, DODirector, Michigan Osteoporosis Testing Center
Clinical Professor of Internal Medicine and Rheumatology, MichiganState University College of Osteopathic Medicine
Private PracticeDetroit, Michigan
Michael Schweitz, MDArthritis & Rheumatology Associates
Good Samaritan Medical CenterPalm Beach Gardens Medical Center
West Palm Beach, Florida
CME ReviewerPeter Barland, MD, Professor Emeritus, Department of Medicine (Rheumatology), Professor Emeritus,Department of Pathology, Albert Einstein College of
Medicine, Bronx, New York
Nurse ReviewerVictoria Ruffing, RN, CCRP, Program Director, Johns Hopkins Arthritis Center, Johns Hopkins University, Baltimore, Maryland
Applying Scientific Measurement of Disease Activity in Clinical Rheumatology Based on a program chaired by Max I. Hamburger, MD, FACP, FACR
Faculty
APPLYING SCIENTIFIC MEASUREMENT OF DISEASE ACTIVITY IN CLINICAL RHEUMATOLOGY
Figure 1. Estimates of the probability of death over 2years according to the HAQ score at baseline(HAQ >1) indicates at least some difficultiesin most activities of daily living.9
1095 patients with RA and 1490 community controls
100%
95%
90%
85%
Controls HAQ<1
Controls HAQ≥1
0 6 12 18 24
RA, HAQ<1
RA, HAQ≥1
Surv
ival
(%
)
Time (months)
JUNE 2011

higher HAQ scores of >1 had the worst prognosis in both ofthe groups (Figure 1).11
The Routine Assessment of Patient Index Data 3 (RAPID3)questionnaire provides information regarding physical func-tion, pain and global estimate, without formal joint counts.RAPID3 was developed to facilitate more widespread quantita-tive measurement in standard rheumatology clinical care, as anindex that can be collected easily to assess and monitor patientstatus. The RAPID3 is correlated with DAS in clinical trials12-14
and clinical settings3 and has capacity to distinguish active from
control treatments in clinical trials, suggesting that RAPID3has the ability to provide usable quantitative data to help directpatient care. RAPID4 and RAPID5 were developed to provideadditional data beyond patient reported outcomes that includesdata from a patient-reported joint count and/or visual analogscale (VAS) charted physician global estimate.
Rheumatologists in the featured CORE RAPSS workshopdid not currently utilize patient self-report routinely for assess-ing functional status (Figure 2) or for evaluating pain inpatients with RA.
4
Table 1. Treating RA to Target: Recommendations15
Overarching Principles a. The treatment of RA must be based on a shared decision between patient and rheumatologist.
b. The primary goal of treating the patient with RA is to maximize long-term health-related quality of life through control of symptoms, prevention ofstructural damage, normalization of function and social participation.
c. Abrogation of inflammation is the most important way to achieve these goals.
d. Treatment to target by measuring disease activity and adjusting therapy accordingly optimizes outcomes in rheumatoid arthritis.
10 Recommendations on Treating RA to Target Based in Both Evidence and Expert Opinion 1. The primary target for treatment of RA should be a state of clinical remission.
2. Clinical remission is defined as the absence of signs and symptoms of significant inflammatory disease activity.
3. While remission should be a clear target, based on available evidence low disease activity may be an acceptable alternative therapeutic goal, partic-ularly in established long-standing disease.
4. Until the desired treatment target is reached, drug therapy should be adjusted at least every 3 months.
5. Measures of disease activity must be obtained and documented regularly, as frequently as monthly for patients with high/moderate disease activityor less frequently (such as every 3-6 months) for patients in sustained low disease activity or remission.
6. The use of validated composite measures of disease activity, which include joint assessments, is needed in routine clinical practice to guide treat-ment decisions.
7. Structural changes and functional impairment should be considered when making clinical decisions, in addition to assessing composite measuresof disease activity.
8. The desired treatment target should be initiated throughout the remaining course of the disease.
9. The choice of the (composite) measure of disease activity and the level of the target value may be influenced by consideration of co-morbidities,patient factors, and drug-related risks.
10. The patient has to be appropriately informed about the treatment target and the strategy planned to reach this target under the supervision of therheumatologist.
Figure 2. Use of Self-Reports with RA Patients
For patients with RA under your care (not including when required for clinical trials or to provide a therapy to an individual patient) how often do you utilize a patient self-report questionnaire to assess functional status?
Always
75-99% of visits
50-74% of visits
25-49% of visits
1-24% of visits
Never
0 1 2 3 4 5
VOL. 5, NO. 1

The index practice reports the practice behavior of 4 rheuma-tologists representing between 12 and 30 years of clinical prac-tice. All the rheumatologists see at least 41 to 50 RA patients permonth with one participant reporting more than 51 RA patientvisits per month, correlating the ability to influence the rheuma-tology care of between 123 to over 200 patients per month.Currently, 1 physician reported using patient self-report toassess pain in 1% to 24% of RA patient visits.
Pincus and colleagues have led the drive to change thinkingfrom ad hoc clinical impressions to scientific measurement.Rheumatologists are a data-hungry specialty. Recent recommen-dations reported by Smolen and colleagues identified the needto treat to an identified target of disease activity (ie, clinicalremission or low disease activity).15 In the absence of achievingthese targets, therapy should be adjusted accordingly until targetis achieved throughout the course of disease. The use of validat-ed composite or pooled indices of disease activity was recom-mended to guide treatment decisions and management.15 Theintroduction of treat to target recommendations developed byan international task force of rheumatologists will likely impacthow many rheumatologists currently practice.
Recommendations for treating to target in patients with RAalso reported the highest number of votes and levels of agree-ment for the use of composite disease activity measures, whichinclude joint counts, in managing patients with RA.15 Thesespecific recommendations reflect the common goal of RAcare—remission and low disease activity (Table 1).
Quantitative assessment of RA lacks a single “Gold standard”disease activity measure, which can be used to assess all patients.“Gold” standard measures such as blood pressure, total choles-terol, and glucose HbA1C can make a diagnosis or implement orchange current treatment. ESR and CRP can be informative buttypically will not cause a physician to change treatment goalsbased on fluctuations or absence of significant findings.
Formal Joint CountsMost patient visits to rheumatologists include a careful
examination of joints; however, most visits do not include for-mal joint counts.1 Joint counts are the most specific clinicalmeasures for evaluating patients with RA and historically havebeen the most important measures in clinical trials of RA. Thestandard 28-joint count includes joints that are typicallyinvolved in RA (eg, PIP joints of the fingers, MCP joints, andthe wrists, elbows, shoulders, and knees) and is as useful inevaluating groups of patients as are more extensive joint
counts. Some patients with RA may have affected joints thatare not evaluated in the 28-joint count (eg, hip, ankle) andthese values are included in the RAPID4. While formal jointcounts can be of value in assessing disease severity in a patientwith RA and for guiding treatment, there are also some disad-vantages. Formal joint counts are time consuming and tediousfor the clinician, and reproducibility is poor.
Laboratory Testing in the Management of Patientswith RA
A lower-than-normal hemoglobin level and an elevatedplatelet count may be used as indicators of inflammation inpatients with RA. The most widely used laboratory tests inpatients with RA include the ESR and determination of CRPlevels. ESR and CRP are particularly useful in RA if they areelevated, but normal levels do not rule out RA. Patients withRA and normal CRP and ESR levels may be less likely todevelop damage to their joints than their counterparts withelevated levels of these markers.
Of patients with RA, 70% to 90% test positive for the pres-ence of RF. Although RF antibody titers do not strictly corre-late with disease activity, patients with a high RF titer are morelikely to have erosive joint disease, extra-articular manifesta-tions, and greater functional disability than patients who havea low RF titer. Patients who have RA and who are seronegativefor RF may have a milder course of disease. Anti-CCP anti-bodies may be more specific than RF for diagnosing rheuma-toid arthritis and may better predict erosive disease (Table 2).16
APPLYING SCIENTIFIC MEASUREMENT OF DISEASE ACTIVITY IN CLINICAL RHEUMATOLOGY
5
Case Study—Key Findings Prior to WorkshopParticipation:
• The index site of 4 rheumatologists reported that1 of the practicing rheumatologists always per-formed formal tender and swollen joint counts onpatients with rheumatoid arthritis (RA). Onerheumatologist reported performing this activityin 25% to 49% of visits. The remaining 2 indicat-ed that they never perform this activity.
• A total of 3 rheumatologists order an erythrocytesedimentation rate (ESR) and/or c-reactive protein(CRP) for their patients with RA 75% to 99% of thetime while the remaining doctor always ordersESRs and/or CRPs.
• A total of 3 rheumatologists never utilize a patientself-report questionnaire to assess pain while 1physician indicates the use 1% to 24% of the time
• None of the physicians currently utilize a patientself-report questionnaire to assess functional status
JUNE 2011
Table 2. Meta-analysis: Anti-CCP Antibody and RF
Anti-CCP RF
Number of studies 37 50
Positive likelihood ratio 12.5 4.9
Odds ratio for RA 16.1-39.0 1.2-8.7
These antibodies are often detected in the early stages of RA(onset < 1 year) and may help identify patients with rheumatoidarthritis and better predict radiographic progression.16
The ESR test is a non-specific measure of inflammation andis routinely used in the assessment of rheumatic disorders.17
This is partly due to the fact that the ESR is a simple and inex-pensive test that can be performed in almost any clinic oroffice. Beyond its importance in the classification of rheumat-ic diseases, the ESR serves as one measure of disease activityfor drug trials in RA, where values ≥ 28 mm/h are oftenrequired for entry into a study.17
Laboratory testing in RA has important limitations, particu-larly compared with laboratory tests in other diseases whichdemonstrate greater specificity, such as for serum cholesterol,creatinine, glucose, and hemoglobin A1c. Currently there isnot a rheumatology blood test that is 100% positive in anyrheumatic disease and 100% negative in all normal individuals.For example, ESR and CRP are normal in about 40% ofpatients with RA.17,18 Another disadvantage of laboratory teststo guide treatment decisions is the lack of immediate resultsthat may delay treatment.
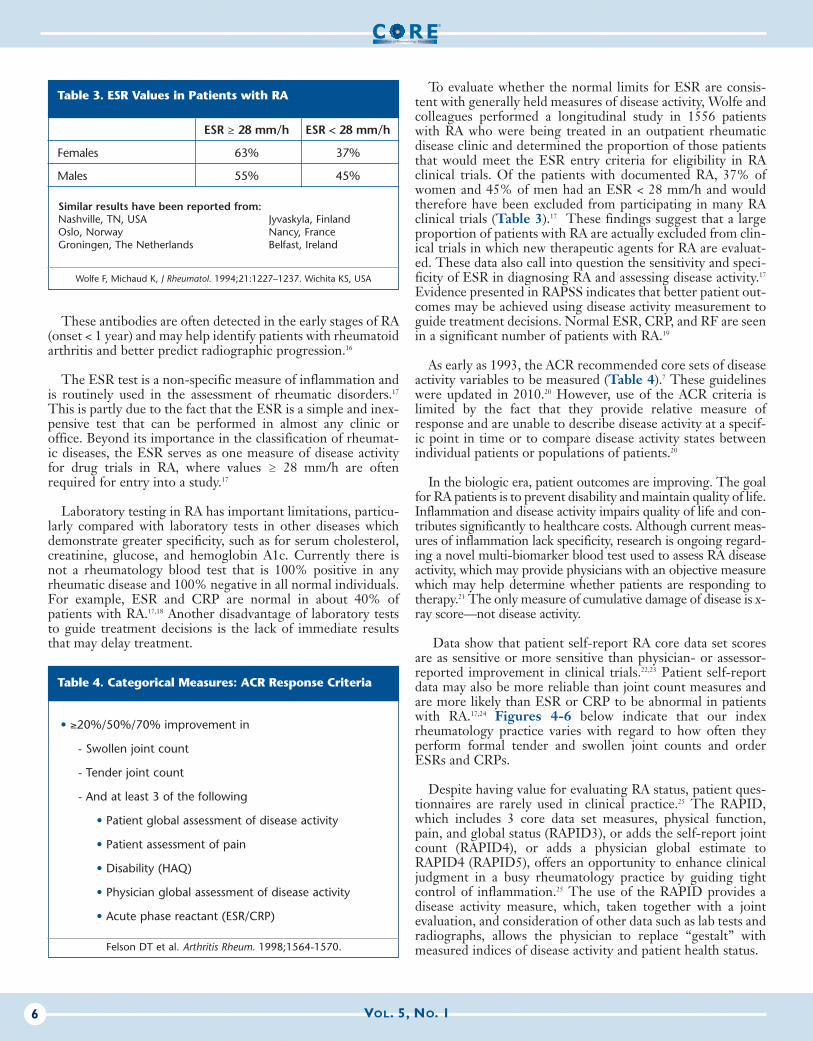
To evaluate whether the normal limits for ESR are consis-tent with generally held measures of disease activity, Wolfe andcolleagues performed a longitudinal study in 1556 patientswith RA who were being treated in an outpatient rheumaticdisease clinic and determined the proportion of those patientsthat would meet the ESR entry criteria for eligibility in RAclinical trials. Of the patients with documented RA, 37% ofwomen and 45% of men had an ESR < 28 mm/h and wouldtherefore have been excluded from participating in many RAclinical trials (Table 3).17 These findings suggest that a largeproportion of patients with RA are actually excluded from clin-ical trials in which new therapeutic agents for RA are evaluat-ed. These data also call into question the sensitivity and speci-ficity of ESR in diagnosing RA and assessing disease activity.17
Evidence presented in RAPSS indicates that better patient out-comes may be achieved using disease activity measurement toguide treatment decisions. Normal ESR, CRP, and RF are seenin a significant number of patients with RA.19
As early as 1993, the ACR recommended core sets of diseaseactivity variables to be measured (Table 4).7 These guidelineswere updated in 2010.20 However, use of the ACR criteria islimited by the fact that they provide relative measure ofresponse and are unable to describe disease activity at a specif-ic point in time or to compare disease activity states betweenindividual patients or populations of patients.20
In the biologic era, patient outcomes are improving. The goalfor RA patients is to prevent disability and maintain quality of life.Inflammation and disease activity impairs quality of life and con-tributes significantly to healthcare costs. Although current meas-ures of inflammation lack specificity, research is ongoing regard-ing a novel multi-biomarker blood test used to assess RA diseaseactivity, which may provide physicians with an objective measurewhich may help determine whether patients are responding totherapy.21 The only measure of cumulative damage of disease is x-ray score—not disease activity.
Data show that patient self-report RA core data set scoresare as sensitive or more sensitive than physician- or assessor-reported improvement in clinical trials.22,23 Patient self-reportdata may also be more reliable than joint count measures andare more likely than ESR or CRP to be abnormal in patientswith RA.17,24 Figures 4-6 below indicate that our indexrheumatology practice varies with regard to how often theyperform formal tender and swollen joint counts and orderESRs and CRPs.
Despite having value for evaluating RA status, patient ques-tionnaires are rarely used in clinical practice.25 The RAPID,which includes 3 core data set measures, physical function,pain, and global status (RAPID3), or adds the self-report jointcount (RAPID4), or adds a physician global estimate toRAPID4 (RAPID5), offers an opportunity to enhance clinicaljudgment in a busy rheumatology practice by guiding tightcontrol of inflammation.25 The use of the RAPID provides adisease activity measure, which, taken together with a jointevaluation, and consideration of other data such as lab tests andradiographs, allows the physician to replace “gestalt” withmeasured indices of disease activity and patient health status.
VOL. 5, NO. 16
Table 4. Categorical Measures: ACR Response Criteria
• ≥20%/50%/70% improvement in
- Swollen joint count
- Tender joint count
- And at least 3 of the following
• Patient global assessment of disease activity
• Patient assessment of pain
• Disability (HAQ)
• Physician global assessment of disease activity
• Acute phase reactant (ESR/CRP)
Felson DT et al. Arthritis Rheum. 1998;1564-1570.
Table 3. ESR Values in Patients with RA
ESR ≥ 28 mm/h ESR < 28 mm/h
Females 63% 37%
Males 55% 45%
Similar results have been reported from:Nashville, TN, USA Jyvaskyla, FinlandOslo, Norway Nancy, FranceGroningen, The Netherlands Belfast, Ireland
Wolfe F, Michaud K, J Rheumatol. 1994;21:1227–1237. Wichita KS, USA

Bossert et al evaluated the validity of the self-report ques-tionnaires for measuring the activity of RA in everyday prac-tice, compared with the DAS28, Clinical Disease ActivityIndex (CDAI), and Simplified Disease Activity Index (SDAI)26
to determine cutoffs for flare detection based on patients' andphysicians' opinions.
A total of 200 consecutive patients with RA completed thequestionnaires (RAPID3) and RA Disease Activity Index-5
(RADAI5). The RAPID3 and RADAI5 scores correlated sig-nificantly with the 3 composite activity indices, with P valuesranging from 0.64 to 0.74. The flare rate was 35% accordingto the patients and 22% according to the physicians, with mod-erate agreement between patients and physicians. Theseresults support the use of the RAPID3 and RADAI5 self-reportquestionnaires and should encourage their widespread use ineveryday practice in patients with RA. The self-report ques-tionnaire scores correlate with the composite activity index val-
APPLYING SCIENTIFIC MEASUREMENT OF DISEASE ACTIVITY IN CLINICAL RHEUMATOLOGY
7
Figures 4-6. Index Practice Behavior for Assessment to Evaluate Disease Activity and/or Guide Treatment
Figure 4: For patients with RA under your care how often do you order a CRP test?*
*Not including when required for clinical trials or to provide a therapy to an individual patient.
Always
75-99% of visits
50-74% of visits
25-49% of visits
1-24% of visits
Never
0 0.5 1 1.5 2 2.5 3 3.5
Figure 5: For patients with RA under your care how often do you order an ESR?*
*Not including when required for clinical trials or to provide a therapy to an individual patient.
Always
75-99% of visits
50-74% of visits
25-49% of visits
1-24% of visits
Never
0 0.5 1 1.5 2 2.5 3 3.5
Figure 6: For patients with RA under your care how often do you perform a formal tender and swollen joint count?*
*Not including when required for clinical trials or to provide a therapy to an individual patient.
Always
75-99% of visits
50-74% of visits
25-49% of visits
1-24% of visits
Never
0 0.5 1 1.5 2 2.5
JUNE 2011

ues and allow the detection of activity peaks or flares.26
The RAPID is a simple patient-generated index that has asimilar sensitivity to change. It has a clear advantage over other
assessment tools that require more time and cost.27 Providingpatients with the questionnaire upon check in, prior to seeingthe physician, is a step toward improving quantitative guidanceof clinical decisions and documentation of patient status, out-comes, and improvement.13 To accomplish such results theentire healthcare team should be educated on the value ofpatient questionnaires affecting patient care by illustratingtreatment efficacy and disease status.5,28,29
The Tight Control of Rheumatoid Arthritis (TICORA)study30 was a single-blind randomized controlled trial (n= 111)to compare tight controlled treatment and routine treatment inpatients with disease duration of up to 5 years. The evaluationand strategy of treatment algorithms were based on an objec-tive disease activity score in the individual treated, tight controlgroup and evaluated in the routine group by the subjective“gestalt” of the clinician. The outcomes of the TICORA studyincluded mean decrease in disease activity score, the number ofpatients with good response (defined as a DAS28<2.4 after 2years and a fall in this score from baseline of more than 1.2),and the percentage of patients in remission.30 The results ofTICORA demonstrated that a decrease in the disease activityscore was higher in the tight control group than in the routinegroup (−3.5 vs −1.9, P<0.0001). Compared with routine care,patients in the tight control group had a significant response(82% vs 44%, P<0.0001) or remission (DAS28<1.6) (65% vs16%, P<0.0001). Radiographic disease progression, physicalfunction and quality of life in the tight control group were alsomore favorable than in the routine care group, at no addition-al financial costs.30 The literature demonstrates that defining atarget and defining the measurement to achieve that targetprovides benefit (Figure 7).30-33
The RAPID score obtained in Barbara’s case describes mod-erate-to-severe activity. It is obtained by adding the tabulatedboxes. Utilizing quantitative measurement allows treatment tobe modified. For example a RAPID3 score of 9.7 as indicatedin the RAPID3 section of the RAPID5 survey indicates mod-erate disease activity and should encourage consideration of atreatment change.13
Changes in RAPID measures may also indi-cate the need to consider additional therapies.
Three months later, Barbara returned withRAPID scores of <3, indicating “near remission”status. Barbara’s stability can now be monitoredfor continued disease monitoring and functionalstatus.13
The educational presentation concludedwith the determination that the RAPID (addi-tional measure of joint count and MD global)reports similar separation as active arm versusplacebo as demonstrated in the DAS. Theadoption of RAPID3 measures serves as a focusto the rheumatology visit. The self-report toolalso helps patients to realize that they may notbe reporting all the issues that may be relevantto their care.
VOL. 5, NO. 18
Let’s look at a patient case presentation utiliz-ing quantitative measures.
Patient CasePresentation:Barbara is a 44-year-oldwoman who presents to theclinic saying that she has“pain in her hands that stopsher from being able to workin her garden.” • Her primary care physician
had suggested that shetake ibuprofen when shevisited his office 6 weeks ago.
• Initially her symptoms improved but then shedeveloped more pain, morning stiffness lasting atleast 1 hour, and swelling of her hands as well asher knees.
• Rheumatoid factor (RF) and cyclic citrullinated pep-tide (CCP) antibody are negative; CRP is 15(NR≤10)
• She has smoked 1 pack of cigarettes daily for 10years but denies alcohol or any drug use.
• Yearly tuberculosis skin tests, required as a result ofher occupation as a healthcare worker, have beennegative.
• Family history and the remainder of the review ofsystems are unremarkable except for occasionaldyspepsia, relieved by chewable antacids, since sheused naproxen 2 years ago for dysmenorrhea.
Figure 7. Intensive Treatment Resulted in Better Disease Response
Grigor C, et al. Lancet. 2004;364:263-269.
Month
Dis
ease
Act
ivity
Sco
re
6
5
4
3
2
1
00 3 6 9 12 15 18
Routine group (n=50)
Intensive group (n=53)

APPLYING SCIENTIFIC MEASUREMENT OF DISEASE ACTIVITY IN CLINICAL RHEUMATOLOGY
9
Patient Case Presentation:
Barbara visits your office and completes the fol-lowing RAPID5 evaluation indicating moderateto severe disease activity.34,35
Barbara describes a 5-year history of tolerable,intermittent low back pain and reportsincreased pain for the past 6 months with littlerelief from her discomfort.
Physical exam is positive for 15 tender and 12swollen joints; x-ray results are positive for sev-eral mild erosions and negative for joint spacenarrowing. She also reports pain on compres-sion of her metacarpophalangeal (MCP) andmetatarsophalangeal joints. Ocular, cardiac,respiratory and dermatologic exams all withinnormal limits.
Pertinent laboratory results are: • Hemoglobin: 11.2 g/dL (N values 12.0-
16.0)• Hematocrit: 31% (N values 35% - 45%)• Platelets: 459,000/mm3 (Normal range:
150,000 to 400,000/mm3)• White blood cell count: 12.8 x 103/L (N val-
ues 4.5-11 x 103/L• Serum creatinine: 0.9 mg/dL• Glucose 145 mg/dL (N values 70-115
mg/dL)• ESR: 45 mm/hour (N=< 15)• CRP: 1.9 pg/mL (vary)• Antinuclear antibodies: <1:4 (Normal)• RF: positive
JUNE 2011
ConclusionsThe primary objective of this educational activity is to edu-
cate rheumatologists about the RAPID score. RAPID3 is ade-quate to document status and monitor effectiveness of thera-pies in patients with RA, and is easily obtained in standard clin-ical care. RAPID3 does not require a formal joint count yetprovides results in clinical trials similar to DAS28. The RAPIDmethodology is designed to improve the ability of rheumatol-ogists to assess, monitor and document patient status quantita-tively in busy clinical settings. RAPID4 and RAPID5 weredeveloped to provide additional data beyond patient reportedoutcomes that includes physician derived data from a jointcount and/or global estimate. The adoption of the use of quan-titative measures in standard rheumatology practice couldimprove care, validate documentation and lead to better out-comes for patients with rheumatoid arthritis.
Case Study—Key Findings Post WorkshopParticipation:• All participants agree or strongly agree that the informa-
tion learned during this activity will help to improve theirskills or judgment within the next 6 months
• Compared with pre-workshop practices of never utilizing apatient self-report questionnaire to assess functional status,1 participant plans to utilize at least 50% to 74% of visits,2 participants plan to utilize 75% to 99% of the time, withanother planning to always implement the behavior.
• Compared with only 1 participant utilizing a patient self-report questionnaire 1% to 24% of visits pre-workshop,post-workshop all participants intend to utilize self-reportat least 50% to 74% of the time, with 1 participant intend-ing to always implement the behavior.
CLICK HERE TO TAKE POST-TEST ONLINE

1. Hamburger MI, Hamburger FH, Bergman JM, Epstein A, Brown A.Influence of an educational seminar on use of disease activity measure-ments by rheumatologists in treatment of rheumatoid arthritis. JRheumatol. 2009;36(3):532-538.
2. Nicolau G, Yogui MM, Vallochi TL, Gianini RJ, Laurindo IM, NovaesGS. Sources of discrepancy in patient and physician global assessmentsof rheumatoid arthritis disease activity. J Rheumatol. 2004;31(7):1293-1296.
3. Wolfe F, Michaud K, Pincus T, Furst D, Keystone El. The disease activ-ity score is not suitable as the sole criterion for initiation and evaluationof anti-tumor necrosis factor therapy in the clinic: discordance betweenassessment measures and limitations in questionnaire use for regulatorypurposes. Arthritis Rheum. 2005;52(12):3873-3879.
4. Castro-Rueda H, Kavanaugh A. Biologic therapy for early rheumatoidarthritis: the latest evidence. Curr Opin Rheumatol. 2008;20(3):314-319.
5. van der Kooij SM, Allaart CF, Dijkmans BA, Breedveld FC. Innovativetreatment strategies for patients with rheumatoid arthritis. Curr OpinRheumatol. 2008;20(3):287-294.
6. Pincus T, Yazici Y, Sokka T. Complexities in assessment of rheumatoidarthritis: absence of a single gold standard measure. Rheum Dis ClinNorth Am. 2009;35(4):687-697.
7. Felson DT, Smolen JS, Well G, et al. American College ofRheumatology/European League Against Rheumatism provisional def-inition of remission in rheumatoid arthritis for clinical trials. ArthritisRheum. 2011;63(3):573-586.
8. van der Heijde DM, van ‘t Hof M, van Riel PL, van de Putte LB.Development of a disease activity score based on judgment in clinicalpractice by rheumatologists. J Rheumatol. 1993;20(3):579-581.
9. Sharp JT, Bluhm GB, Brook A, et al. Reproducibility of multiple-observer scoring of radiologic abnormalities in the hands and wrists ofpatients with rheumatoid arthritis. Arthritis Rheum. 1985;28(1):16-24.
10. Genant HK, Jiang Y, Peterfy C, Lu Y, Redel J, Countryman PJ.Assessment of rheumatoid arthritis using a modified scoring method ondigitized and original radiographs. Arthritis Rheum. 1998;41(9):1583-1590.
11. Sokka T, Häkkinen A, Krishnan E, Hannonen P. Similar prediction ofmortality by the health assessment questionnaire in patients withrheumatoid arthritis and the general population. Ann Rheum Dis.2004;63(5):494-497.
12. Pincus T. The DAS is the most specific measure, but a patient question-naire is the most informative measure to assess rheumatoid arthritis. JRheumatol. 2006;33(5):834-837.
13. Pincus T. Can RAPID3, an index without formal joint counts or labo-ratory tests, serve to guide rheumatologists in tight control of rheuma-toid arthritis in usual clinical care? Bull NYU Hosp Jt Dis.2009;67(3):254-266.
14. Pincus T. Is a self-report RAPID3 score a reasonable alternative to aDAS28 in usual clinical care? J Clin Rheumatol. 2009;15(5):215-217.
15. Smolen JS, Aletaha D, Bijlsma JW, et al. Treating rheumatoid arthritisto target: recommendations of an international task force. Ann RheumDis. 2010;69(4):631-637.
16. Nishimura K, et al. Meta-analysis: diagnostic accuracy of anti-cyclic cit-rullinated peptide antibody and rheumatoid factor for rheumatoidarthritis. Ann Intern Med. 2007;146(11):797-808.
17. Wolfe F, Michaud K. The clinical and research significance of the ery-throcyte sedimentation rate. J Rheumatol. 1994;21(7):1227-1237.
18. Pincus T, et al. Quantitative measurement of patient status in the regu-lar care of patients with rheumatic diseases over 25 years as a continu-ous quality improvement activity, rather than traditional research. ClinExp Rheumatol. 2007;25(6 Suppl 47):69-81.
19. Sokka T, Pincus T. Erythrocyte sedimentation rate, C-reactive protein,or rheumatoid factor are normal at presentation in 35%-45% of
patients with rheumatoid arthritis seen between 1980 and 2004: analy-ses from Finland and the United States. J Rheumatol. 2009;36(7):1387-1390.
20. Aletaha D, et al. 2010 Rheumatoid arthritis classification criteria: anAmerican College of Rheumatology/European League AgainstRheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569-81.
21. Weinblatt ME, Manning W, Coblyn JS, et al. Use of a Multi-Biomarker Score for Rheumatoid Arthritis Disease Activity (Vectra™DA) to Assess Response to Therapy. In EULAR Congress. 2011.
22. Cohen SB, Strand V, Aguilar D, Ofman JJ. Patient-versus physician-reported outcomes in rheumatoid arthritis patients treated with recom-binant interleukin-1 receptor antagonist (anakinra) therapy.Rheumatology (Oxford). 2004;43(6):704-711.
23. Scott DL, Strand V. The effects of disease-modifying anti-rheumaticdrugs on the Health Assessment Questionnaire score. Lessons from theleflunomide clinical trials database. Rheumatology (Oxford).2002;41(8):899-909.
24. Kvien TK, Mowinckel P, Heiberg T, et al. Performance of health statusmeasures with a pen based personal digital assistant. Ann Rheum Dis.2005;64(10):1480-1484.
25. Pincus T. Pain, function, and RAPID scores: vital signs in chronic dis-eases, analogous to pulse and temperature in acute diseases and bloodpressure and cholesterol in long-term health. Bull NYU Hosp Jt Dis.2008;66(2):155-165.
26. Bossert M, Prati C, Vidal C, Bongain S, Toussirot E, Wendling D.Evaluation of self-report questionnaires for assessing rheumatoid arthri-tis activity: A cross-sectional study of RAPID3 and RADAI5 and flaredetection in 200 patients. Joint Bone Spine [published online ahead ofprint May 5, 2011].
27. Uhlig T. "KISS"--embracing routine patient assessment. J Rheumatol.2009;36(6):1096-1098.
28. Kavanaugh A, Klareskog L, van der Heijde D, Li J, Freundlich B,Hooper M. Improvements in clinical response between 12 and 24 weeksin patients with rheumatoid arthritis on etanercept therapy with orwithout methotrexate. Ann Rheum Dis. 2008;67(10):1444-1447.
29. Pincus T, Sokka T. Quantitative measures to assess patients with rheu-matic diseases: 2006 update. Rheum Dis Clin North Am. 2006;32(Suppl1):29-36.
30. Grigor C, Capell H, Stirling A, et al. Effect of a treatment strategy oftight control for rheumatoid arthritis (the TICORA study): a single-blind randomised controlled trial. Lancet. 2004;364(9430):263-269.
31. Puolakka K, Kautiainen H, Möttönen T, et al. Early suppression of dis-ease activity is essential for maintenance of work capacity in patientswith recent-onset rheumatoid arthritis: five-year experience from theFIN-RACo trial. Arthritis Rheum. 2005;52(1):36-41.
32. Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF, et al.Clinical and radiographic outcomes of four different treatment strate-gies in patients with early rheumatoid arthritis (the BeSt study): A ran-domized, controlled trial. Arthritis Rheum. 2008;58(2 Suppl):S126-S35.
33. Verstappen SM, Jacobs JW, van der Veen MJ, et al. Intensive treatment withmethotrexate in early rheumatoid arthritis: aiming for remission. ComputerAssisted Management in Early Rheumatoid Arthritis (CAMERA, an open-label strategy trial). Ann Rheum Dis. 2007;66(11):1443-1449.
34. Pincus T, Swearingen CJ, Bergman M, Yazici Y. RAPID3 (RoutineAssessment of Patient Index Data 3), a rheumatoid arthritis index with-out formal joint counts for routine care: proposed severity categoriescompared to disease activity score and clinical disease activity index cat-egories. J Rheumatol. 2008;35(11):2136-2147.
35. Yazici Y, Bergman M, Pincus T. Time to score quantitative rheumatoidarthritis measures: 28-Joint Count, Disease Activity Score, HealthAssessment Questionnaire (HAQ), Multidimensional HAQ(MDHAQ), and Routine Assessment of Patient Index Data (RAPID)scores. J Rheumatol. 2008;35(4):603-609.
VOL. 5, NO. 110
References

CORE®….Where Rheumatologists Live to Learn
Coming Soon
Look for the new CORE Web Resource Center atwww.NACCME.com—coming soon!
Your TRUSTED resource for CME/CE programming is now your ONLY source for medical education
and information, with an updated Coalition of Rheumatology Educators (CORE)®
Resource Center
As a registered user, you can:
o Register for and participate in the same high-quality live CME/CE eventsand on-demand activities that you have come to expect at NACCME, including new CORE programming, such as:
• Live symposia
• Regional dinner meetings
• Conference recaps
o Remain up-to-date on the latest medical news and information
o Discuss current medical issues with your peers via targeted NACCME learning groups
o Make www.NACCME.com your home for all CME/CE activities via expanded “my account” features
APPLYING SCIENTIFIC MEASUREMENT OF DISEASE ACTIVITY IN CLINICAL RHEUMATOLOGY
11JUNE 2011

300 Rike Drive, Suite AEnglishtown, NJ 07726-8544
NORTH AMERICAN CENTER FOR CONTINUING MEDICAL EDUCATION
Get your documentation of credit NOW
Completing a post-test at www.naccme.com is as easy as 1-2-3…
1. Visit http://www.naccme.com/program/2011-419-2/ and navigate to “Post-Test.”
2. Successfully complete the post-test and evaluation form and gain access to your doc-umentation of credit.
Live step-by-step assistance is available Monday-Friday 8:30 am-4:30 pm ET at 609-371-1137 or e-mail [email protected].
Copyright © 2011 by Albert Einstein College of Medicine and North American Center for Continuing Medical Education, LLC. All rights reserved. No partof this accredited continuing medical education activity may be reproduced or transmitted in any form or by any means, electronic or mechanical, with-out first obtaining permission from Albert Einstein College of Medicine and North American Center for Continuing Medical Education.
Privacy PolicyEinstein and NACCME protect the privacy of personal and other information regarding participants, educational partners, and joint sponsors. Einstein andNACCME and our joint sponsors will not release personally identifiable information to a third party without the individual’s consent, except such informa-tion as is required for reporting purposes to the appropriate reporting agency.
Einstein and NACCME maintain physical, electronic, and procedural safeguards that comply with federal regulations to guard your nonpublic personalinformation.
www.naccme.com
2011-419-2


















